
Abstract
Purpose:
When a cancer diagnosis coincides with caring for children, it may influence the financial impacts of cancer and decisions to pursue advance care planning (ACP) or genetic testing. We examined associations between caring for children and financial hardship, ACP, and genetic testing among female adolescent and young adult (AYA) cancer survivors in North Carolina and California.
Methods:
Participants were diagnosed at ages 15–39 years with breast, melanoma, gynecologic, lymphoma, or thyroid cancer during 2004–2016. We estimated adjusted prevalence differences (aPDs) and ratios (aPRs) for each outcome by child caring status using marginal structural binomial regression models.
Results:
Among 1595 women ages 19–54 years at survey (median = 7 years since diagnosis), 819 (51.3%) reported that they were caring for children at diagnosis. Women caring for children had a higher prevalence of material financial hardship (e.g., medical debt; 30% vs. 21.9%; aPD = 9%, 95% confidence interval [CI]: 3 to 14; aPR = 1.39, 95% CI: 1.12 to 1.72) but similar levels of psychological financial hardship compared to noncaregivers. Women caring for children were more likely to complete ACPs (42.2% vs. 30.7%; aPD = 9%, 95% CI: 3 to 16; aPR = 1.30, 95% CI: 1.08 to 1.57). Among the 723 survivors of breast, endometrial, and ovarian cancer, the prevalence of genetic testing was higher among women caring for children (89%) than noncaregivers (81%); this difference was not statistically significant.
Conclusion:
Women caring for children at diagnosis may be at elevated risk for adverse financial outcomes and may benefit from additional financial navigation support. Childcare responsibilities may further complicate health decision-making for AYAs diagnosed with cancer.
Introduction
A
Approximately 50% of U.S. cancer survivors experience cancer-related financial hardship (e.g., a person's psychological response, material conditions, and coping behaviors related to the cost of medical care). 4 AYA survivors may be at greater risk for financial hardship because their health insurance coverage may be disrupted at age 26 (e.g., aging off parental insurance) or linked to employment—and AYAs may still be in school, beginning their careers, and working toward financial independence.4,5 AYAs diagnosed with cancer while also caring for children may be at greater risk for financial distress given additional financial demands related to having dependents in the home. 6
AYAs with childcare responsibilities may be more willing to engage in ACP due to the impact of health care decisions on children. ACP is a process that enables individuals to share their life goals, values, and preferences regarding future medical care with others. 7 Although ACP is typically thought of as important for individuals at the end of life it is relevant for all individuals. 7 Many healthy AYAs do not prioritize ACP; however, a diagnosis of serious illness warrants an ACP discussion. The Institute of Medicine recommends ACP for all individuals, 8 and the American Society of Clinical Oncology includes documentation of ACP by the third office visit as part of measuring quality cancer care. 9 ACP may be particularly important for AYAs with childcare responsibilities. ACP discussions can be challenging for those caring for children due to concerns about balancing parental role preservation (e.g., avoiding treatments with toxicities that may limit their ability to care for children) and the desire to extend one's life for the sake of children in the home (e.g., reluctance to engage in conversations about potential death).10,11
Having responsibilities caring for children may also impact a person's desire to perform genetic testing. Genetic testing for hereditary cancer risk is recommended for some cancers (breast, endometrial, and ovarian cancer) diagnosed at a young age and may identify hereditary cancer risk in children.12–16 The decision to undergo genetic testing for hereditary cancer risk for women with children may be complicated by challenges related to the impact of disclosure or nondisclosure of results to children. 17 In some cases, having children may increase a woman's desire for genetic testing to better understand her children's future cancer risk. 18 In other cases, having children may be a barrier to genetic testing because of fear of unfavorable genetic testing results. 18 Understanding the potential impact of childcare responsibilities on genetic testing may inform genetic counseling conversations.
Health-related decision-making is complex, and although our three outcomes of interest are distinct, each was selected for its particular relevance to AYAs with children. We examined the prevalence of financial hardship, use of ACPs, and genetic testing in relation to childcare responsibilities at diagnosis among female AYA cancer survivors in California and North Carolina.
Materials and Methods
We used data from the AYA Horizon Study, a cohort of women diagnosed with the five most common types of cancer among female AYAs (i.e., breast, thyroid, melanoma, lymphoma, or gynecologic—ovarian, cervical, or endometrial; these cancers make up 75.7% of all female AYA cancers). 1 A full description of the study methods is provided elsewhere. 19 In brief, we identified incident cancer diagnoses among women ages 15–39 years from the statewide North Carolina Central Cancer Registry (NC CCR) (2004–2015) and the regional Kaiser Permanente Northern California (KPNC) and Kaiser Permanente Southern California (KPSC) health system cancer registries (2004–2016). Additional eligibility criteria for participation included being alive and at least 18 years old at the time of contact (September 2018–November 2019) with an available mailing address, and, among women in California, current enrollment in the KPNC or KPSC health plan. The research was approved by the institutional review board at each study site.
Eligible women (n = 13,132) were invited to participate in an online survey that assessed survivorship topics related to genetic testing, information needs, health behaviors, financial concerns, caregiving roles, ACP, and fertility and reproductive outcomes. Women were invited through mailed letter to participate in the survey, and a second reminder was sent 3 weeks later. In total, 1679 (12.8%) women responded to the survey. Compared to nonresponders, a greater proportion of responders had a breast cancer diagnosis (39.9% vs. 35.2%), had regional or distant stage disease (40.9% vs. 35%), received chemotherapy (41.9% vs. 36.6%), and identified as White (83.1% vs. 73.4%). 19 Further characteristics of the invited sample compared to survey respondents are described in detail elsewhere. 19 We excluded records from 35 women with missing data on status caring for children (2% of total), leaving surveys completed by 1644 women for analysis.
Age, cancer type, and stage at diagnosis were defined from the NC CCR or the KPNC or KPSC cancer registries. Cancer types were categorized using the AYA Site Recode ICD-O-3/WHO 2008 definitions. 2 Participants self-reported their ethnicity (Hispanic/Latino) and race (12 respondents with missing values for ethnicity/race were filled with data from the cancer registries), highest level of education completed, health insurance coverage at diagnosis, marital status at diagnosis, employment/school enrollment status at diagnosis, and household income in the year before the survey.
We assessed caring for children at diagnosis through two items: (1) “A caregiver is someone who looks after a child or a sick, elderly, or disabled person. When you were diagnosed with [cancer type] in [year], were you a caregiver for children, parents, or someone else?” and (2) “When you were diagnosed with [cancer type], who were you a caregiver for?” with response options for child(ren)/daughter/son, spouse/partner/significant other, parent, grandparent, sibling/brother/sister, friend, or other (with a free text response option). Women who reported being a caregiver for “child(ren)/daughter/son” were categorized as “caring for children” (n = 819). Women were excluded from analysis if they reported a free text response of only babysitting/nannying or being a school teacher, or reported caregiving for people who were not children (n = 49). Women who responded “no” to caregiving for someone at diagnosis were categorized as “non-caregivers” (n = 776). The final analytic sample, including women caring for children and noncaregivers, was 1595.
Outcome assessment (financial hardship, ACP, genetic testing)
We assessed financial hardship related to self-reported material conditions or psychological responses. 4 Items were based on the Medical Expenditure Panel Survey Experiences with Cancer Survivorship Supplement. 20 We assessed material conditions through responses to two items: (1) “Have you or has anyone in your family had to borrow money or go into debt because of your cancer, its treatment, or the lasting effects of that treatment?” and (2) “Did you or your family ever file for bankruptcy because of your cancer, its treatment, or the lasting effects of that treatment?” Women who responded “yes” to either survey item were categorized as having material financial hardship. Psychological response was assessed through one survey item: “Have you ever worried about having to pay large medical bills related to your cancer?” (yes/no). Women who responded “yes” were categorized as having psychological financial hardship.
ACP was assessed through two items: (1) “A health care power of attorney is a legal document that allows you to name a person you trust to make health care decisions and speak for you when you are unable to speak for yourself. Do you have a health care power of attorney?” (yes/no); and (2) “A living will is a legal document in which you say what medical decisions should be made if you become too sick or injured to make those decisions yourself. Do you have a living will?” (yes/no). Women who responded “yes” to either survey item were categorized as having advance directives. Women were also asked if their “health care providers talked with them about completing a health care power of attorney or living will” at any point during their cancer diagnosis or treatment (yes/no).
Genetic testing was assessed through response to: “Have you ever had a genetic test at a doctor's office or medical center to determine if you or your family members are at greater risk for developing certain types of cancer?” (yes/no). Women who responded “yes” were categorized as using genetic testing. Genetic testing analyses were limited to women diagnosed with breast, endometrial, or ovarian cancer (n = 723) per NCCN Clinical Practice Guidelines in Oncology for genetic risk evaluation that recommends genetic testing for early age cancer onset in these populations.12,14,21
Statistical analysis
Continuous variables are reported as mean and standard deviation when normally distributed; if not normally distributed, continuous variables are reported as median and interquartile range (IQR). Prevalence differences (PDs) and prevalence ratios (PRs) with 95% confidence intervals (CIs) were estimated using marginal structural linear- and log-binomial regression models with inverse probability of exposure (i.e., caregiving for children) weighting and robust variance estimation methods. 22
The model used to derive the inverse probability weights included the following covariates: study site (NC, CA); age at diagnosis (continuous); race/ethnicity (non-Hispanic white, non-Hispanic Black, non-Hispanic Asian, Hispanic, non-Hispanic all other races); education (high school or less, some college/Associate's degree, Bachelor's degree or higher); health insurance coverage at diagnosis (yes/no); marital status at diagnosis (married/partnered, never married, other); and employment/school status at diagnosis (employed, in school, employed and in school, other). This analytic method provides a standardized measure of association by weighting exposure groups (caring for children and noncaregivers) to have comparable covariate distributions. The covariates included in the model used to derive the weights were identified as confounders a priori with the use of a directed acyclic graph. Prevalence differences provide a comparison of the absolute difference in the proportion of patients with a specific experience, while prevalence ratios provide the ratio of two proportions. The two measures are reported together to address the fact that a large ratio (e.g., ≥2) can reflect a setting where both groups have a low prevalence (e.g., 1% vs. 2%) or where conditions are more common (e.g., 40% vs. 80%). SAS version 9.4 (SAS Institute, Cary, NC) was used for analysis.
Results
Within the analytic sample (n = 1595), women were on average 40 years old at the time of the survey (SD = 6.6 years), diagnosed with cancer at a median age of 34 years (IQR = 8), and were a median of 7 years from diagnosis (IQR = 6) (Table 1). The most common cancer type was breast cancer (40%, n = 639), and the majority had localized stage disease (55%, n = 825). Treatments received included surgery only (32%, n = 507), radiation without chemotherapy (22%, n = 355), and any chemotherapy (45%, n = 714). Women were primarily non-Hispanic White (72%, n = 1149), highly educated (63% had a Bachelor's degree or higher, n = 1008), employed at diagnosis (72%, n = 1143), married or living with a partner (73%, n = 1157), and had private health insurance at diagnosis (91%, n = 1444). No substantive differences in associations for any outcome were observed by study state (NC vs. CA).
Respondent Characteristics, Overall and by Caregiver Status (n = 1595)
% of nonmissing observations.
Cell sizes <5 are suppressed to limit potential for participant identification.
Non-Hispanic other race includes Native Hawaiian and other Pacific Islanders, American Indian or Alaska Native, other race, and multiracial.
IQR, interquartile range.
Financial hardship
Overall, 26% of women (n = 416) reported material financial hardship, which included borrowing money or going into debt (25%; n = 405) or filing for bankruptcy (2.6%; n = 41) because of cancer. Approximately 13% of women (n = 201) borrowed or incurred debt of $10,000 or more, and 4.5% (n = 72) borrowed or incurred debt of $25,000 or more. Nearly half of women (45.6%; n = 772) reported psychological financial hardship (e.g., worrying about cancer related medical bills). Women caring for children versus noncaregivers reported higher material financial hardship prevalence (30% vs. 22%; aPD = 9%, 95% CI: 3 to 14; adjusted prevalence ratio [aPR] = 1.39, 95% CI: 1.12 to 1.72; Table 2). Psychological financial hardship was similar between women caring for children and noncaregivers (48% vs. 49%; adjusted prevalence difference [aPD] = −2%, 95% CI: −8 to 5; aPR = 0.97, 95% CI: 0.85 to 1.10) (Table 2 and Fig. 1).
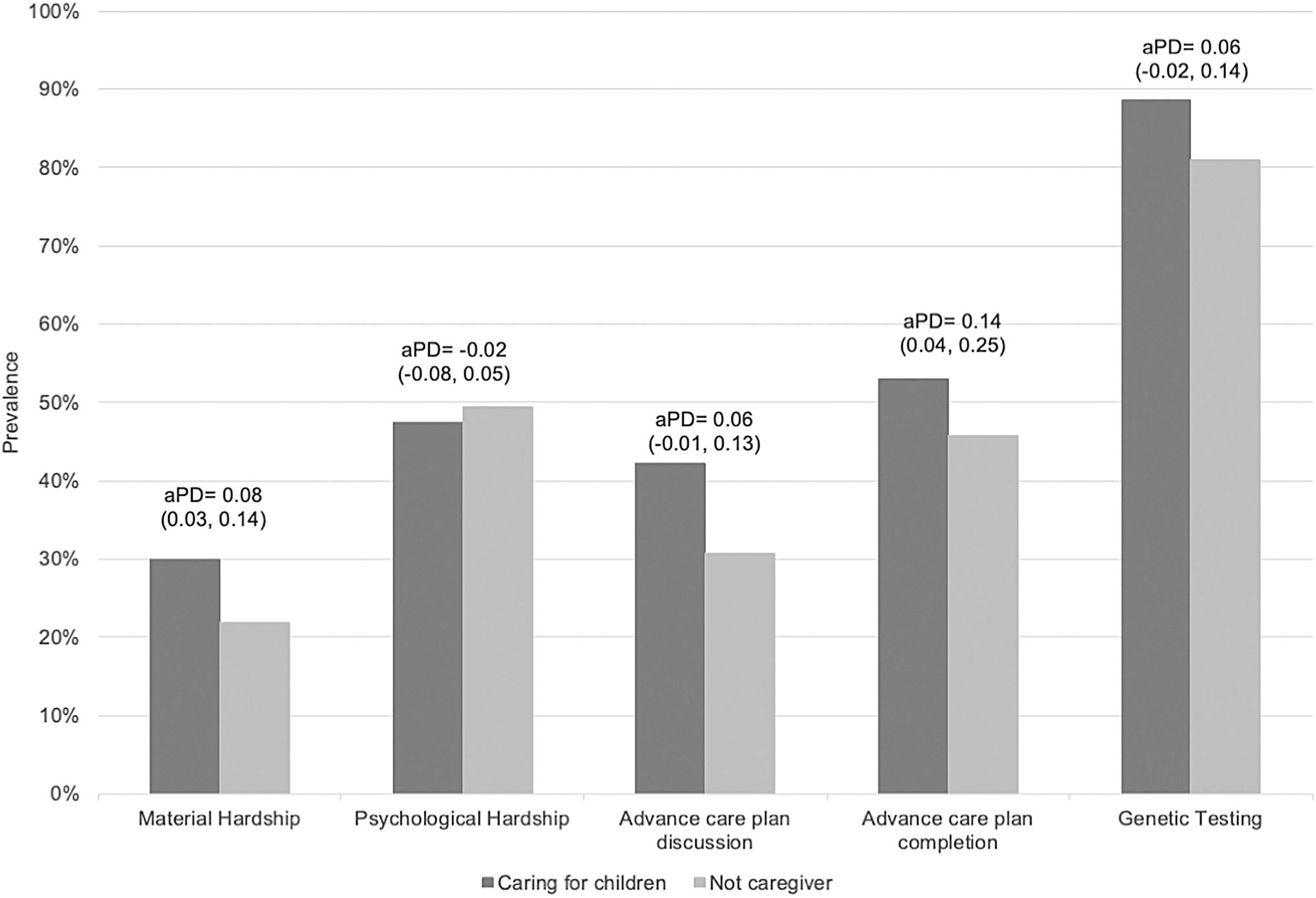
Prevalence and aPDs and 95% CIs for financial hardship, ACP, and genetic testing by caregiving status for children among AYA Horizon Study respondents (n = 819 caring for children, n = 776 not caregiver). Prevalence for advance care plan completion is limited to participants who had discussed care plans with providers (n = 346 caring for children, n = 248 not caregiver), and genetic testing is limited to participants with breast, endometrial, and ovarian cancer (n = 413 caring for children, n = 310 not caregiver). Advance care plan completion refers to having legal documents appointing a health care power of attorney or living will. ACP, advance care planning; aPD, adjusted prevalence difference; AYA, adolescent and young adult; CI, confidence interval.
Financial Hardship Due to Cancer According to Caring for Children at Diagnosis, AYA Horizon Study
Adjusted for state (NC, CA), age at diagnosis (linear), race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic Asian, Hispanic, non-Hispanic other race), education (high school or less, some college/Associate's degree, Bachelor's degree or higher), health insurance at diagnosis (yes, no), marital status at diagnosis (married/partnered, never married, other), and employment status at diagnosis (employed, in school, employed and in school, other).
Sample sizes within the monetary categories may not sum to the total number who borrowed money or went into debt due to missing data on the amount of money borrowed or debt incurred.
aPR, adjusted prevalence ratio; AYA, adolescent and young adult; PR, prevalence ratio.
Advance care planning
Of women in our sample, across both women caring for children and women who were not caregivers, 37% (n = 584) talked to a health care provider about ACP, and 34% (n = 541) completed an advance directive. Among those who discussed ACPs with a provider, 50% completed an advance directive. Women caring for children were not significantly more likely to discuss ACPs compared to noncaregivers (42% vs. 31%; aPD = 6%, 95% CI: −0.7 to 13; aPR = 1.16, 95% CI: 0.98 to 1.37). Caregiving status was not associated with ACP discussion in analyses stratified by in situ/localized (aPD = 4%, 95% CI: −0.5 to 12; aPR = 1.10, 95% CI: 0.87 to 1.39) or regional/advanced disease (aPD = 9%, 95% CI: −0.2 to 20; aPR = 1.21, 95% CI: 0.97 to 1.53). However, among women who had an ACP discussion, women caring for children were more likely to complete ACPs (53% vs. 46%; aPD = 14%, 95% CI: 4 to 25; aPR = 1.33, 95% CI: 1.07 to 1.64) (Table 3 and Fig. 1).
Prevalence of Advance Care Planning and Genetic Testing by Caregiver Status
Adjusted for state (NC, CA), age at diagnosis (linear), race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic Asian, Hispanic, non-Hispanic other race), education (high school or less, some college/Associate's degree, Bachelor's degree or higher), health insurance at diagnosis (yes, no), marital status at diagnosis (married/partnered, never married, other), and employment status at diagnosis (employed, in school, employed and in school, other).
Completion of advance directive refers to having legal documents appointing a health care power of attorney or living will.
Genetic testing includes tests performed at a doctor's office or medical center, and does not include home tests.
ACP, advance care planning.
The association between caregiving status and completion of advance directives among women who had an ACP discussion appeared to be driven by earlier stage disease, in that women with localized stage disease who were caring for children were significantly more likely to complete an ACP than women with localized stage disease who were not caregivers (localized disease aPD = 20%, 95% CI: 6 to 34; localized disease aPR = 1.49, 95% CI: 1.12 to 1.98; advanced disease aPD = 6%, 95% CI: −11 to 23; advanced disease aPR = 1.12, 95% CI: 0.81 to 1.54).
Genetic testing
Among women diagnosed with breast, endometrial, or ovarian cancers (n = 723), 85% (n = 617) reported receiving a genetic test at a medical center. Women who cared for children reported a higher prevalence of genetic testing compared to women who were not caregivers (89% vs. 81%), although the difference was not statistically significant (aPD = 6%, 95% CI: −2 to 14; aPR = 1.08, 95% CI: 0.98 to 1.19) (Table 3 and Fig. 1).
Discussion
Childcare responsibilities may contribute to financial status and health-related decision-making for AYAs with cancer. In our sample of AYA cancer survivors in California and North Carolina, women who cared for children at the time of cancer diagnosis reported a higher prevalence of material financial hardship (e.g., borrowing money or going into debt) and engagement with ACP. Women who cared for children did not report a higher psychological financial burden or higher likelihood of genetic testing for hereditary cancer risk. AYA cancer survivors are uniquely at-risk for difficulties with health-related decision-making and financial hardship due to their individual developmental age and financial vulnerability. 2 Our findings provide additional evidence that financial hardship and ACP uptake may be influenced by childcare responsibilities at diagnosis.
AYAs may be financially vulnerable after cancer diagnosis due to limited financial reserves, cancer related employment disruptions, and increased likelihood of having multiple forms of debt. 23 The effects of a cancer diagnosis on AYA's financial well-being can be further impacted by responsibilities caring for children. For example, financial obligations related to caring for children on top of their limited financial reserves may leave AYAs less likely to be able to handle the financial impact of cancer. Financial hardship can contribute to poorer quality of life, worse health, 24 and early mortality 25 among survivors. Interventions focused on improving AYAs' financial health will have minimal effects without systematic policy change. 26 Policies regarding paid sick leave and short-term welfare programs may help to reduce financial burden. Health care providers should be aware that childcare responsibilities may present a barrier to care due to competing financial and time priorities; accommodations and flexibility in timing of planned care may reduce these barriers.
Overall, women in our sample experienced levels of psychological financial hardship similar to national levels. The 48.4% who reported psychological distress in our sample is consistent with findings from a study using data from the U.S. National Health Interview Survey in which 47% of adult cancer survivors younger than age 65 years reported experiencing psychological financial hardship. 27 The high prevalence of psychological financial distress we found emphasizes the ongoing need for accessible counseling and financial navigation services throughout survivorship and policies designed to mitigate financial hardship.
ACP was originally recommended for individuals diagnosed with cancer in their last year of life. More recently, ACP has become an expected component of quality cancer care regardless of cancer stage. 9 Women in our sample had a comparable prevalence of having an ACP discussion with their health provider (37%) to the prior literature. In one study by Pennarola et al., we found that among young adult allogeneic stem cell transplant recipients, 37% had an ACP discussion. 28 In our sample, AYA survivors with childcare responsibilities were similarly likely to discuss generating an advance directive compared to noncaregivers, but women caring for children were more likely to complete ACPs following discussion. This difference may be a reflection of the perceived importance of ACP to anticipate the care of children after death or reduced capacity to provide care. 3 ACP completion may benefit individuals with cancer by increasing the likelihood of receiving treatment aligned with values and goals. However, ACP training for providers should include AYA-specific needs.
A 2021 systematic review reported that the prevalence of women with hereditary ovarian cancer who underwent genetic testing was ∼30% without intervention and 57% to 99% with intervention. 29 Our study's higher proportion of genetic testing may reflect our sample's younger age distribution, more recent recommendations expanding eligibility for genetic testing, increases in its availability,12,21 and differences in access to and coverage for genetic testing by health insurance plans.
This study has limitations. The survey included financial hardship questions regarding bankruptcy, medical debt, and borrowing of money for medical expenses but did not include less severe forms of financial hardship that may still impact AYA cancer survivors' overall financial well-being. Information on discussions about ACP or genetic testing was self-reported, introducing the potential for errors in recall by participants. However, we are reassured by previous research that demonstrates >86% accuracy in reporting genetic testing, 30 and to our knowledge no studies have shown the accuracy of self-reported ACP completion. Nonetheless, given the specificity of living wills and health care power of attorney documents in ACP discussions, we can be reasonably sure of the accuracy of responses. We also note that our sample is fairly well-educated, English-speaking, and insured and may not fully represent the experience of women without insurance, whose primary language is not English, or who have lower education. In addition, our analysis primarily reflects the experience of AYAs ages 25–39 who were caring for children at diagnosis. AYAs in the younger age range (15–24) may have parents/caregivers more involved in health decision-making. A much smaller number of AYAs ages 15–24 reported caregiving roles at diagnosis in our sample, and our findings may not be indicative of health decision-making in younger AYAs caring for children. Our findings also only reflect AYAs caring for children but not adults (e.g., spouses and parents). We chose to exclude participants who reported caregiving for people who were not children because their care responsibilities and relationships are substantially different in terms of impact on health decision-making and the subsample was too small to analyze separately (n = 49).
Finally, the response rate to the online survey was low (12.8%), 19 consistent with low response rates in AYA cancer survivor populations in clinical trials (6%) and nontherapeutic studies (17%), 31 but considerably lower than studies utilizing resource-intensive recruitment strategies among more recently-diagnosed individuals (43%). 32 Successfully reaching AYA survivors is challenging given increased residential mobility, especially if the diagnosis occurred several years in the past and updated contact information is not available. Efforts to engage AYA cancer survivors may be improved using age-appropriate recruitment methods (e.g., social media) and multimodal participation options that were not available in the current research. 33 Despite our low response rate, our findings are based on data from over 1600 female participants from a rigorous sampling frame and provide an important contribution to our understanding of the health decisions made by AYA women with cancer.
Despite these challenges, our study describes the relation of caregiving status at diagnosis to experiences with financial hardship and health-related decision-making among female AYA cancer survivors. Caring for children may exacerbate financial hardship but be associated with more ACP. Future qualitative work understanding how caring for children after a cancer diagnosis impacts health decision-making experiences may reveal opportunities for financial navigation or intervention to increase uptake of recommended ACP. Our findings highlight the need for additional qualitative work, system-level changes to reduce the financial impacts of cancer, and AYA specific training for ACP discussions.
Footnotes
Acknowledgment
The authors thank Dr. Kimberly Farris for her editing services.
Authors' Contributions
K.R.T.: Conceptualization, visualization, and writing—original draft introduction, discussion, review, and editing. C.M.: Conceptualization, methodology, formal analysis, and writing—original draft methods, results, review, and editing. C.A.: Writing—review and editing. A.D.: Data curation, writing—review and editing. S.E.: Writing—review and editing. D.G.: Writing—review and editing. E.E.K.: Supervision, writing—review and editing. A.C.K.: Writing—review and editing. M.L.K.: Writing—review and editing. S.M.: Project administration, writing—review and editing. E.M.P.: Writing—review and editing. A.S.: Writing—review and editing. C.R.C.: writing—review and editing. L.K.: writing—review and editing. H.B.N.: Conceptualization, supervision, funding acquisition, writing—review and editing.
Disclaimer
The opinions expressed are solely the responsibility of the authors and do not reflect the official views of the funding agencies.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by grants from the National Cancer Institute (H. Nichols, R01CA204258) and a developmental award from UNC Lineberger Comprehensive Cancer Center (H.Nichols, P30ES010126). Three authors were supported by training/fellowship grants from the National Cancer Institute (K.R.T., T32CA116339; E.M.P., K07CA218167; and C.M., T32CA057726, F31CA260787).