
Abstract
Purpose:
This study's aim was to determine the actual status of transitional care for patients with pediatric cancer (PPCs) in Japan by surveying obstetricians/gynecologists.
Methods:
A questionnaire survey on transitional medicine was conducted in the form of an online questionnaire at 579 major training facilities nationwide, which were registered with the Japanese Society of Obstetrics and Gynecology.
Results:
While 40% of the facilities had received referrals for PPCs, only 13% provided transitional care specifically for PPCs. The most common problems with referrals were related to “insufficient explanation.” In addition, at facilities with no experience treating PPCs, many respondents commented that they did not know how to follow the progression of the disease. Regarding the necessity of obstetrics/gynecology visits for PPCs, more than half of the respondents at facilities with experience treating PPCs answered that such visits were “necessary”; only 1% answered that they were “unnecessary.” On the other hand, 37% of the facilities that had no experience treating PPCs answered that it was “necessary,” whereas 4% answered that it was “unnecessary.”
Conclusions:
This survey of the actual status of transitional care between pediatrics and obstetrics/gynecology in Japan identified issues to be addressed for the spread of transitional care. The results suggest that, in the future, health care professionals need education to increase their knowledge, and that patient education that leads to patients' awareness of their own self-management is necessary.
Introduction
Advances in cancer treatment have led to an increase in the number of cancer survivors, and improving quality of life after overcoming cancer has become an issue. According to the 2022 Cancer Statistics published by the National Cancer Center, 1 the 10-year relative survival rate for childhood cancer in Japan is ∼70%–80%, whereas in other countries, it is reported that ∼90% of patients with pediatric cancer (PPCs) reach adulthood. 2 One major difference between PPCs and patients with adult-onset cancer is that PPCs undergo stages of both physical and mental growth from childhood to adulthood. PPCs should transition between departments as they grow physically, and the transition from pediatrics to adult departments can benefit PPCs.3,4
In Europe and the United States, web-based patient support systems and passports are being used as tools to educate PPCs about their treatment history and the need for long-term follow-up.5,6 These tools include information on the individual patient's treatment history and when the patient should return to the hospital for prevention and diagnosis of late complications by organ, which is effective for educating patients and facilitating information sharing among health care providers. Systems for transitional care are also being established in other countries.
On the other hand, it is important for obstetricians/gynecologists to be involved in the treatment of PPCs because of the risk of various late complications of childhood cancer, including effects on reproductive function. 7 However, transitional care between pediatricians and obstetricians/gynecologists and health care providers is not widely practiced in Japan, leading to a deficit in this area.
Therefore, in this study, we decided to conduct a survey on transitional care for PPCs in Japan targeting obstetricians/gynecologists.
Materials and Methods
Survey subjects
We surveyed 579 major training facilities in Japan registered with the Japanese Society of Obstetrics and Gynecology and asked representatives of obstetrics and gynecology departments at those facilities to respond. The response period was from January 2021 to March 2022. The major medical training facilities included 113 university hospitals and 466 city hospitals.
Questionnaire survey
A questionnaire on transitional care in the form of an online survey was developed and answered by the respondents. The facilities were classified according to whether they had any experience treating PPCs (Fig. 2) and they were asked to answer each question, and the results were then tabulated (Table 1). Facilities that responded that they had experience treating PPCs were asked to complete a questionnaire consisting of 11 items (Table 1).
Questionnaire Contents
HPV, human papillomavirus; AMH, anti-Müllerian hormone; AFC, antral follicle count.
The contents included “Reasons why the PPC was referred,” “Trouble with the referral of the PPC,” “Specific episodes of trouble,” “Recommendations for treating the PPC,” and “Necessity for the PPC to attend obstetrics/gynecology.” Facilities that responded that they had no experience treating PPCs were asked to complete a questionnaire consisting of nine items (Table 1), the contents of which included “Anticipated difficulties when a PPC is referred,” “Things I would recommend when treating a PPC,” and “Necessity for the PPC to attend obstetrics/gynecology.”
The following scores were used to graphically portray the current status of transitional care in each prefecture: 0 for no transitional care, 1 for having plans to open an outpatient clinic specializing in transitional care, 3 for not having an outpatient clinic specializing in transitional care, and 5 for having an outpatient clinic specializing in transitional care (Fig. 2).
Ethical considerations
This study was approved by the Institutional Review Board at St. Marianna University School of Medicine (approval No. 5387). An item asking the surveyed institutions to confirm their consent to participate was included in the questionnaire, and answers were given freely.
Results
The total response rate was 58.5% (339/579), and only one of the responding facilities did not agree to complete the questionnaire. The respondent facilities consisted of 104 university hospitals and 235 city hospitals.
First, when asked if they provide transitional care specifically for PPCs between pediatrics and obstetrics/gynecology, only 13% (44/338) responded that they do, whereas 40% (136/338) of the facilities had received referrals for PPCs. In addition, the facilities providing transitional care were concentrated in the Tokyo and Osaka metropolitan areas (Fig. 1).
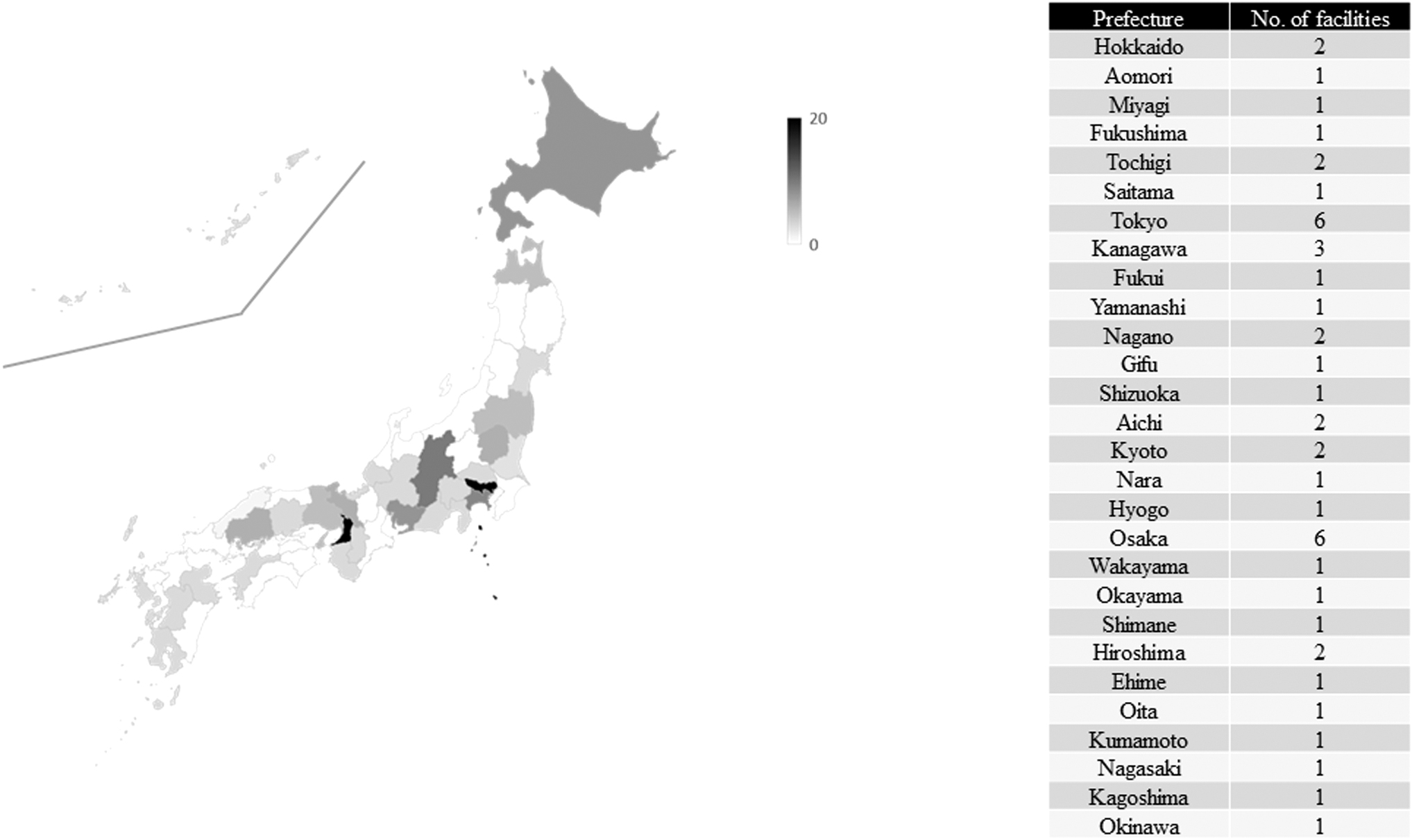
Current status of transitional care facilities in Japan. The number of facilities in Japan that treat patients with pediatric cancer in obstetrics and gynecology departments is shown. The following scores were used to graphically show the current status of transitional care in each prefecture: 0 for no transitional care, 1 for having plans to open an outpatient clinic specializing in transitional care, 3 for not having an outpatient clinic specializing in transitional care, and 5 for having an outpatient clinic specializing in transitional care.
Academic facilities
Thirty-one percent of the facilities provided transitional care, and 73% of the facilities indicated that they had experience treating PPCs (Fig. 2).
The most common reasons for referral were “irregular menstruation or irregular genital bleeding,” “suspected ovarian dysfunction after puberty,” and “request for fertility preservation therapy before cancer treatment.” Other reasons included “desire to have a baby,” “desire to confirm ovarian function and semen findings,” “dysmenorrhea,” and “transition to adulthood with ovarian dysfunction” (Fig. 3A).

Current treatment of patients with pediatric cancer.

Results of a survey on the content of referrals for patients with pediatric cancer.
The most common response regarding problems encountered on referral at facilities with experience treating PPCs was “I don't know how to follow-up” (Fig. 3B). Furthermore, many facilities with no experience treating PPCs also commented that they did not know how to follow up on such patients (Fig. 3C).
Regardless of whether or not they had experience treating PPCs, about 70% recommended the human papillomavirus (HPV) vaccine, 80% recommended cervical cancer screening, 80% recommended hormone level measurement, about half recommended anti-Müllerian hormone (AMH), 40% recommended antral follicle count (AFC), and about 60% recommended bone densitometry (Figs. 4 and 5). The respondents also indicated that they provided information on ovarian dysfunction, infertility treatment, perinatal prognosis, and hospital visits in advance, in addition to evaluating cardiac function and performing other investigations as needed.
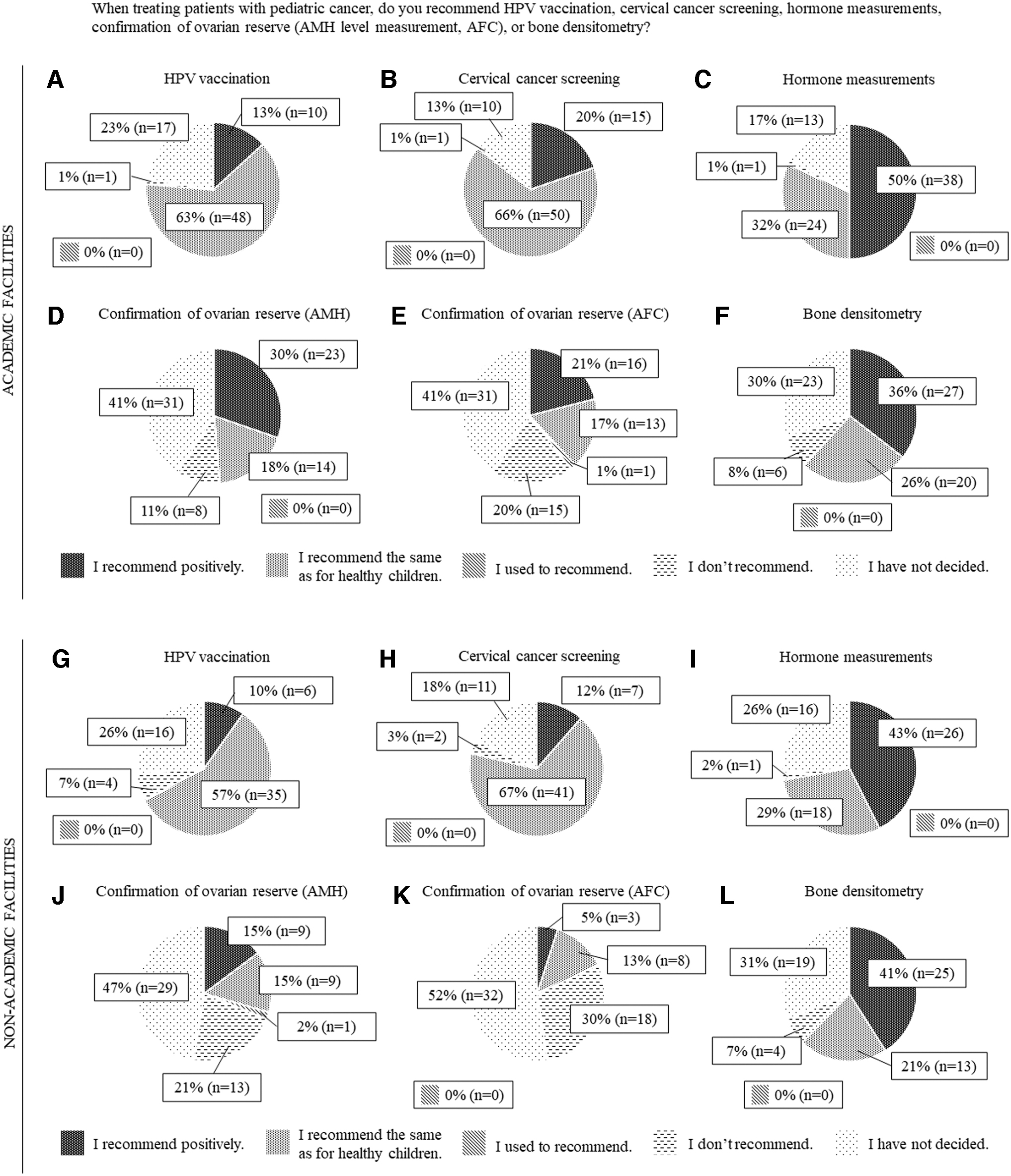
Results of a questionnaire about the treatment of patients with pediatric cancer in obstetrics/gynecology (from facilities with experience in treating patients with pediatric cancer).
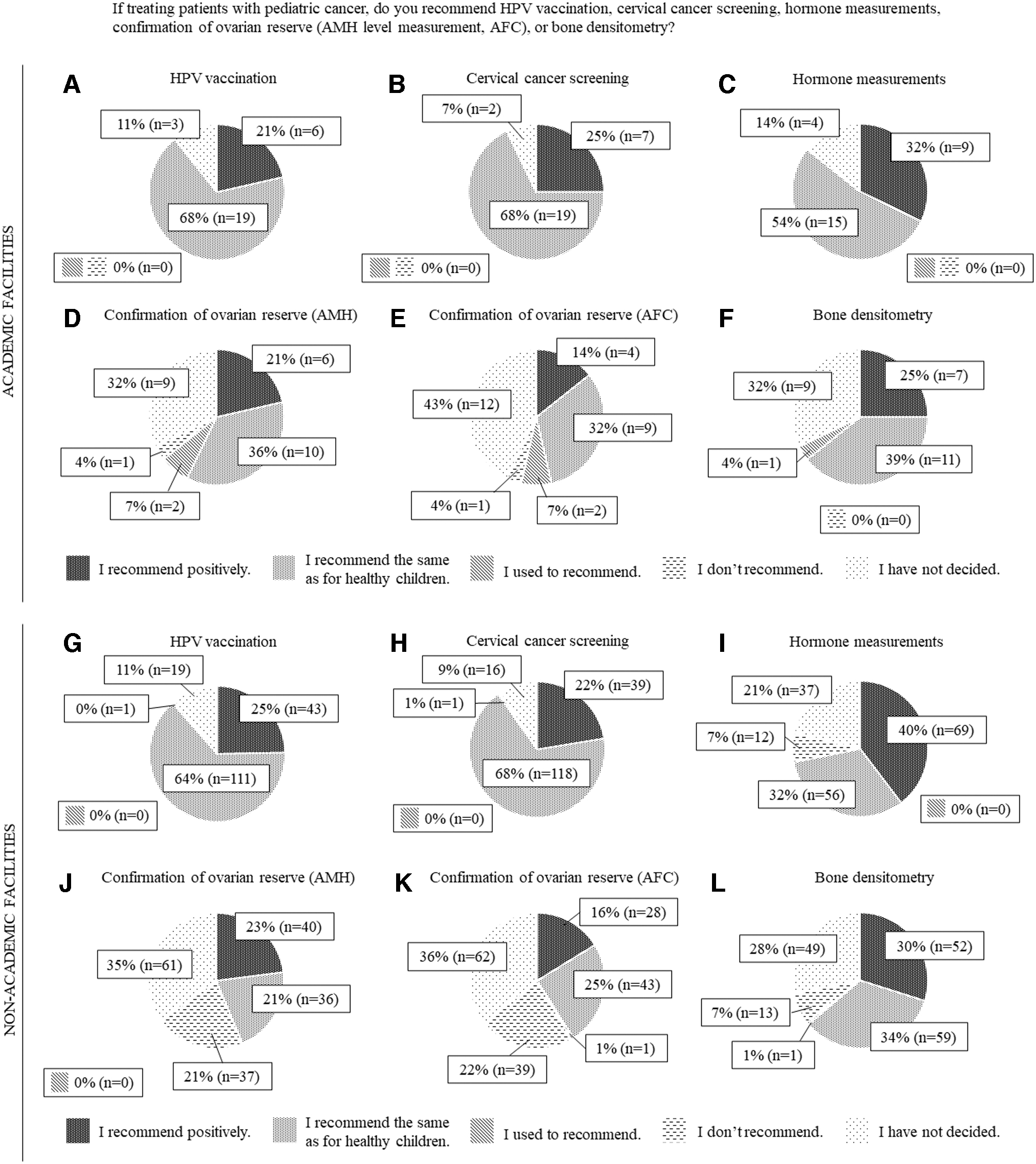
Results of a questionnaire about the treatment of patients with pediatric cancer in obstetrics/gynecology (from facilities with no experience in treating pediatric cancer patients).
Figure 6 shows the results for responses regarding the need for PPCs to visit an obstetrician/gynecologist. Regarding the need for obstetrical/gynecological care for PPCs, 62% of the facilities with experience in this area indicated that it was “necessary,” whereas 38% responded “yes and no.” The most common reason given for the “necessary” response was “Evaluation is necessary, because long-term effects on reproductive function are not known based on the individual's perception of menstrual status alone, and intervention may be necessary to avoid osteoporosis and cardiovascular events.”
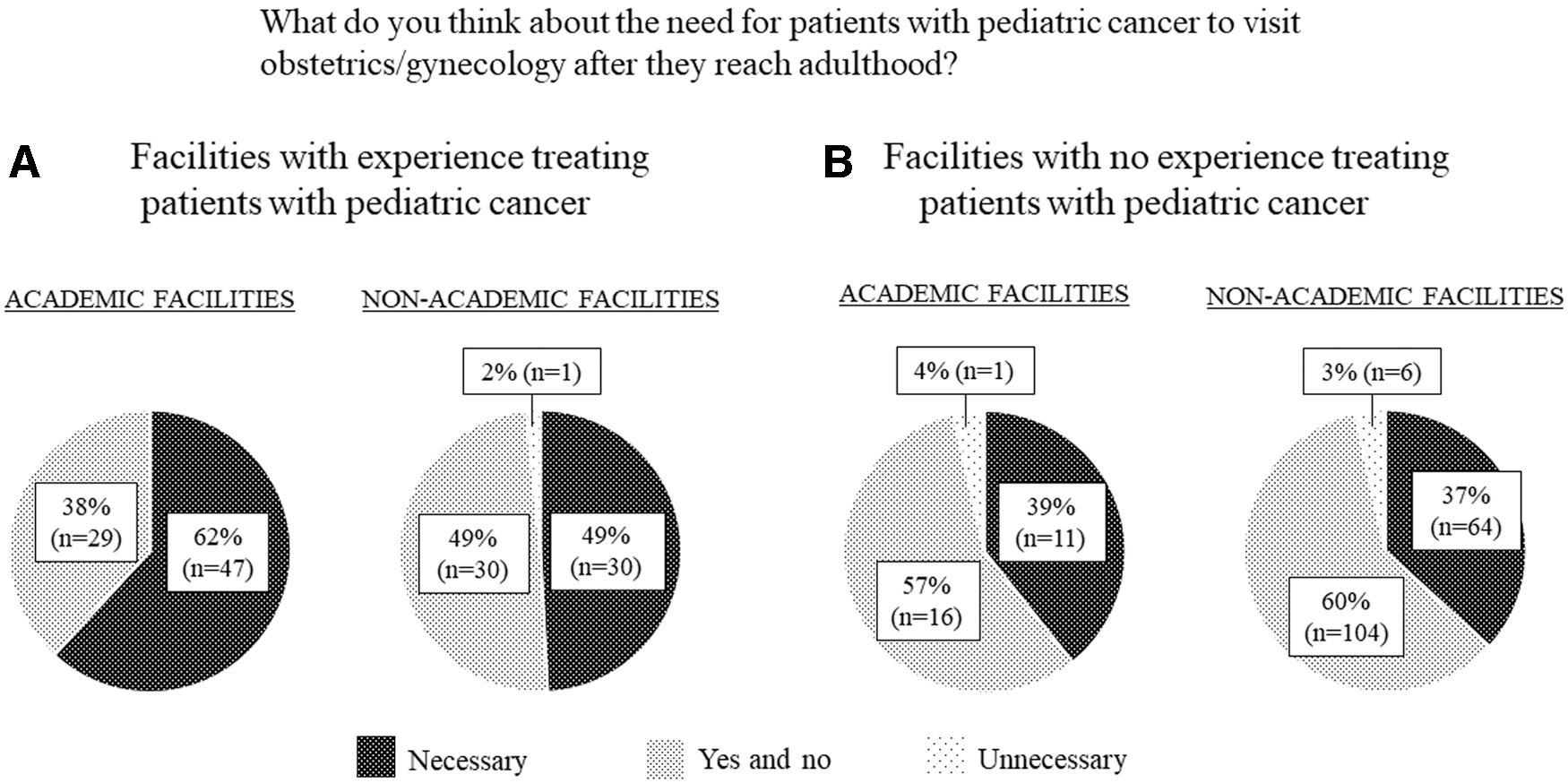
Results of a survey on the need for obstetric and gynecological care for patients with pediatric cancer.
The following responses were also given: “The activity will contribute to the improvement of survivorship for PPCs who need long-term follow-up,” “It has a therapeutic and preventive effect because gynecological diseases increase with life stage,” “Because of the possibility of premature ovarian failure,” and “Some patients may not be old enough at the time of treatment to understand the explanation, or may not have time to think about it, so another opportunity to explain is necessary.”
The most common reason given for the “yes and no” response was “It is acceptable to see a doctor after symptoms such as menstrual abnormalities appear.” The following responses were also given: “It is necessary in cases of suspected ovarian dysfunction, but not necessarily in cases of normal ovarian function”; “Because regular follow-up, such as of ovarian function, can be handled by pediatrics”; “Gynecological care does not need to be actively encouraged because it may cause patient embarrassment,” and “It depends on the patient's wishes.”
About 40% of the facilities with no experience in treating PPCs indicated that it was “necessary,” more than half responded “yes and no,” and only one facility responded that it was “unnecessary.” The reasons were similar to those of facilities with experience treating PPCs. No response was received regarding the reason for the “unnecessary” response.
Nonacademic facilities
More than 90% of the facilities did not provide transitional care, and only 5% reported providing transitional care. Only 26% (61/235) of the facilities had experience treating PPCs.
The most common reasons for referral were “irregular menstruation or irregular genital bleeding” and “suspected ovarian dysfunction after puberty,” followed by “request for surgical intervention.” Other reasons included “information about fertility before treatment” and “perinatal management” (Fig. 3A).
The most common response regarding problems encountered on referral at facilities with experience treating PPCs was “I don't know how to follow-up” (Fig. 3B). Furthermore, many facilities with no experience treating PPCs also commented that they did not know how to follow up on the patients (Fig. 3C).
At facilities with experience treating PPCs, about 70% of the respondents recommended the HPV vaccine, 80% recommended cervical cancer screening, 70% recommended hormone measurement, 30% recommended AMH, 20% recommended AFC, and 60% recommended bone densitometry (Fig. 4).
Of the facilities that had no experience treating PPCs, ∼70% recommended hormone measurements and 60% recommended bone density measurements, similar to those with experience treating PPCs. However, about 90% of the respondents said that they would recommend the HPV vaccine, 90% recommended cervical cancer screening, 40% recommended AMH, and 40% recommended AFC, and a greater proportion recommended it than for facilities with experience treating PPCs (Fig. 5). Other recommendations were similar to those of academic facilities.
Regarding the need for obstetrical/gynecological care, about half of the facilities with experience treating PPCs said it was “necessary,” whereas less than half of the facilities without experience treating PPCs said it was “necessary.” Furthermore, 3% (6/174) of facilities with no experience treating PPCs responded that it was “unnecessary.”
Nonacademic facilities differ from academic ones in that the reasons for “yes and no” responses often involved reluctance, such as “It is acceptable to see a doctor after symptoms appear,” “The follow-up can be done by internal medicine, not obstetrics/gynecology,” “I don't think there is any reason to go to obstetrics/gynecology specifically because you are a PPC,” “Unmarried, ovarian reserve confirmation may be information that is better not to know,” and “Little understanding of special care needs and their usefulness.”
The reasons for the “unnecessary” response were “I don't believe that just being a PPC requires a visit to obstetrics/gynecology” and “If there are no symptoms, the patient may as well be considered a healthy individual with no issues.”
Problems obstetricians and gynecologists face when referring PPCs
The response to the question of whether there was any current or anticipated problem with the referral was “none in particular,” but among the facilities that had experienced problems, many responded that they did not know how to follow up on the progress of the referral. Other responses included the “patient's lack of knowledge (not explained) that they have gonadal dysfunction,” “unannounced disease name to the patient,” “desire to have a baby among patients with ovarian dysfunction,” “lack of time to start treatment for the underlying disease,” and “difficulties in the timing of starting hormone replacement and difficulties in examining children” (Fig. 3).
The specific episodes of actual difficulties at the facilities could be categorized into (I) explanation, (II) system, (III) knowledge, (IV) fertility preservation and ovarian dysfunction related, (V) perinatal related, (VI) primary disease related, and (VII) unfamiliarity with pediatric care (Table 2).
Classification of Specific Episodes of Difficulty That Actually Occurred at the Facility
The most common response to the question of whether there was any problem anticipated upon referral of a PPC to a facility with no experience treating PPCs was “I don't know how to follow up” (Fig. 3). The “other” category included “cannot follow up because the facility does not treat gynecological diseases.”
Discussion
PPCs may experience a variety of irreversible effects from cancer treatments administered during childhood and adolescence. Therefore, although PPCs have a high survival rate, they often require a long follow-up period, while being exposed to various health risks. 8
As survivors of child and adolescent cancer, they transition from pediatric to adult health care. A successful transition to adult health care benefits patients because new health problems may be identified during the transition, and this may improve patient outcomes.3,4 However, the results of this study showed that only 13% of the facilities actually provided transitional care, indicating that regional differences exist in Japan, where transitional care is not widespread (Fig. 1). This was to be expected, since the current state of transitional medicine in Japan is less well developed than in other countries. The primary reason for this is the lack of implementation of a system for this purpose.
Furthermore, it was clear that transitional care was not provided at nonacademic facilities, and that there was less experience providing care at nonacademic facilities than at academic facilities. Compared to academic facilities, fewer nonacademic facilities recommend assessment of ovarian reserve by AMH or AFC (Fig. 4), and fewer nonacademic facilities recommend hormone measurement (Fig. 5). The difference between academic and nonacademic facilities in Japan lies in whether they are staffed by specialist doctors. Obstetrics/gynecology in Japan is divided into four major specialties: Oncology, perinatal medicine, reproductive medicine, and women's health medicine.
Although many academic facilities have doctors in each specialty, it is not uncommon for nonacademic facilities to have none of these specialists on staff. Therefore, the staff of a nonacademic facility may be less knowledgeable. Fewer nonacademic facilities than academic facilities considered obstetrics/gynecology care to be necessary. Transitional care for PPCs requires relatively few advanced skills, so it is preferable to obtain follow-up at facilities such as city hospitals and clinics, but the results were conflicting. The reasons for this were apparent in the presence of a perception that “patients should see a doctor only after symptoms appear,” and responses indicating reluctance such as “just follow up with someone other than the obstetrician/gynecologist.”
In addition, many respondents stated that they did not know how to follow up on the progress of their patients, which is thought to be one of the reasons why transitional care is not widely used. This lack of knowledge and awareness among obstetricians/gynecologists needs to be improved and is considered one of the challenges associated with the spread of transitional medicine. To overcome this challenge, one solution may be to develop guidelines and other materials regarding following up on the progress of PPCs, as mentioned in the responses to the results of this study. In particular, it is essential to develop guidelines for physicians in city hospitals and clinics and for medical coordination.
Key points for optimal transitional care include a clear plan and process, the use of patient navigators, the adoption of a phased and flexible approach, clear and effective communication, the promotion of educational opportunities for self-management, access to online resources such as tailor-made roadmaps and treatment overviews, and joint pediatric and adult care clinics. 8 It will be difficult to incorporate these key points immediately because it will take a certain amount of time to establish a nationwide transitional care system.
On the other hand, one thing that can be improved relatively early on is seamless communication between the pediatric and adult care departments. In addition to ensuring the transfer of patient information from the pediatrician to the adult care physician, it is believed that the pediatrician's reiteration of the patient's medical condition and other information during the transition can facilitate a smooth transition to the adult care department. 9
However, the results of this study showed that there were some cases in which pediatricians' lack of an explanation to patients led to problems when they visited obstetricians/gynecologists. In addition, episodes exist in which obstetricians/gynecologists have struggled with how to explain issues to patients, and “explaining to patients” is an important factor for smooth and successful transitional care. To overcome this problem and assist with explanations, it may be helpful for pediatric and adult departments to create leaflets and other materials that can be used when explaining diseases to PPCs.
In the United States, attempts are being made to distribute credit card-sized passports as a tool to educate PPCs about their treatment history and the need for long-term follow-up. 6 In addition to health care provider education, patient education is also necessary to promote transitional health care. For patient education, a web-based Survivorship Passport (SurPass) that summarizes the clinical histories of patients who have overcome childhood and adolescent cancer in Europe is available. 5 The SurPass provides a summary of each PPC's clinical history, detailed information about the cancer and the treatment received, and individualized follow-up and screening recommendations.
However, we consider that one of the SurPass's problems is the lack of clarity regarding who is responsible for filling out this information. In this regard, the primary pediatric oncology physician who has first contact with the patient should first have the patient register and be responsible for filling out the information.
When the patient becomes an adult and transitions to an adult care department, we consider that transitional care can proceed without disadvantage to the patient if the attending physician of the pediatric care department contacts and shares information with the adult care department to which the patient will transition and the new attending physician. Similarly, in Japan, pediatricians who are the primary physicians treating children with cancer should first educate their patients, and then, when the patients become adults and are transferred to adult care, they should provide the relevant information to their new primary physicians to ensure a smooth transition of care.
The results of this study show that the situation wherein patients are concentrated in facilities that treat acute patients should be avoided as much as possible, and it may be necessary to triage patients before considering hospital visits. For example, treated patients with a high risk of late effects should be transferred to a specialized facility, such as a university hospital, whereas low-risk patients should be transferred to a general practitioner. Risk-specific approaches have been proposed to match the risk of long-term health outcomes with the most appropriate health care setting for care delivery,10,11 and supportive self-management systems such as Oncokompass may be useful in this regard. 12 However, there is no such material available in Japan, and the development of such materials for the spread of transitional medicine is an issue to be addressed in the future.
A limitation of this study is that not all facilities in Japan responded to the questionnaire, so caution must be exercised in interpreting the results. Furthermore, since this study was conducted as a questionnaire survey in Japan, caution is needed when applying the results to global populations.
Conclusions
In this study, we surveyed the actual status of transitional care between pediatrics and obstetrics/gynecology in Japan and identified issues for the spread of transitional care. The results suggested that health care professionals need to be educated further, such as by providing knowledge to health care workers, and that patient education that leads to patients' own awareness of self-management needs to be provided as well.
Authors' Contribution
K.N.: Data curation, investigation, methodology, resources, validation, visualization, and writing–original draft. Y.T.: Investigation, methodology, and writing–review & editing. A.M.: Supervision and writing–review & editing. N.S.: Conceptualization, funding acquisition, project administration, supervision, and writing–review & editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by MHLW Research for Promotion of Cancer Control Program Grant No. JPMH20EA1004 and JPMH23EA1016.