
Abstract
Purpose:
To examine the factors associated with females attending a fertility consultation within 30 days of cancer diagnosis.
Methods:
This is a retrospective cohort study, including females, 15 to 39 years of age, diagnosed with cancer in Ontario, Canada. Administrative data were used from the Institute of Clinical and Evaluative Sciences for the period 2006 to 2019. A backward selection multivariate logistic regression was performed, with a primary outcome of fertility consultation within 30 days of diagnosis.
Results:
A total of 20,556 females were included in the study, with 7% having attended a fertility visit within 30 days of diagnosis. Factors associated with being more likely to attend included: not currently having children (odds ratio [OR] = 4.3; confidence interval [95% CI 3.6–5.1]), later years of diagnosis (OR = 3.2; 95% CI [2.8–3.8]), having undergone chemotherapy (OR = 3.6; 95% CI [3.0–4.3]) or radiation therapy (OR = 1.9; 95% CI [1.6–2.2]), and less marginalization within dependency quintiles (OR 1.4; 95% CI [1.1–1.7]). Having a cancer with lower risk to fertility (OR = 0.3; 95% CI [0.2–0.3]), death within a year of diagnosis (OR = 0.4; 95% CI [0.3–0.6]), and residing in a northern region of Ontario (OR = 0.3; 95% CI [0.2–0.4]) were associated with being less likely to attend. For sociodemographic factors, lower levels of income (OR = 0.5; 95% CI [0.4–0.6]) and marginalization with residential instability (OR = 0.6; 95% CI [0.5–0.8]) were associated with being less likely to attend a fertility consultation.
Conclusions:
Rates for attendance of female fertility consultations after a cancer diagnosis remain low, with disparities by both clinical and demographic factors.
Introduction
Adolescents and young adults (AYAs, 15 to 39 years of age) with cancer are recognized to have unique challenges.1,2 Fertility is one of the most important issues for young females diagnosed with cancer that can impact both quality of life and psychosocial well-being.3–9 Females with cancer have reported to be frustrated regarding both a lack of information about fertility risks and an inability to undertake fertility preservation before treatment. 5 Providing patients with information regarding fertility before treatment is important considering the results of a recent study that showed that female cancer survivors had a 30% greater overall risk of an infertility diagnosis than a matched cohort of females who had never had cancer. 10
Research has also shown that fertility consultations before treatment can reduce regret related to decisions around fertility preservation. 6 Better understanding of factors affecting uptake of fertility consultations in this population is important to help improve oncofertility care in females with cancer.
There are many factors related to cancer and its treatment that may lead to lower fertility rates in female survivors, with the risk to fertility highly dependent upon both the specific treatment and the particular disease. 11 There are several potential options for females to preserve fertility after a cancer diagnosis, including fertility-sparing procedures and embryo or oocyte cryopreservation. However, the availability of these varies according to age at diagnosis, cancer type, and access to specialized fertility clinics.
Discussion regarding fertility preservation before cancer treatment is recommended for all young cancer patients, to discuss these options and help patients better understand fertility risks before undergoing therapy.12–14 Pretreatment fertility consultations have been found to lead to greater uptake of fertility preservation in females diagnosed with cancer. 7
Some study has been done examining factors associated with referral of cancer patients for fertility consultation. Investigators in the Netherlands that, like Canada, has a publicly funded health care system conducted a study of female cancer patients, finding that 9.8% were referred for fertility preservation counseling. A diagnosis of either breast cancer or lymphoma and being aged 20–29 years at diagnosis were important factors associated with acceptance of fertility counseling. 15 In Ontario, Canada, two studies have examined fertility consultation referrals, finding low rates for female AYAs with breast cancer 16 and lymphoma. 17 However, these studies did not include all females with cancer.
To ensure effective planning, it is important to understand the state of fertility referrals that occur within the optimal window before commencement of treatment. The objective of this study was to determine factors associated with attending a fertility consultation within the first 30 days of a cancer diagnosis for AYA females in Ontario. Thirty days after diagnosis was chosen as a proxy for the start of treatment, based on results from the development of an indicator to monitor oncofertility care. 18
Materials and Methods
A retrospective cohort study was performed on data obtained from the Institute of Clinical Evaluative Sciences (ICES) in Toronto, Ontario. ICES is an independent nonprofit research institute whose legal status under Ontario's health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. All analyses were completed in iDAVE, a remote access server, using SAS® 9.4 (SAS Institute, 2013, Cary NC).
Population
We included all females, 15 to 39 years of age, diagnosed with cancer in Ontario between January 1, 2006, and September 30, 2019. Exclusion criteria included secondary cancer diagnosis; fertility consultation preceding a cancer diagnosis by >30 days; non-Ontario resident status; and prior sterilization procedure (hysterectomy, oophorectomy, and tubal ligation) identified using diagnostics codes in the Ontario Health Insurance Plan (OHIP)—Supplementary Appendix Table SA1.
Data
Data were extracted between December 1, 2005, and November 30, 2020, with data for past diagnoses reviewed starting April 1, 1998, from the following administrative databases housed at ICES: Ontario Cancer Registry, OHIP Claims Database, Registered Persons Database (RPDB), MOMBABY, and Cancer Activity Level Reporting (ALR). These data sets were linked using unique encoded identifiers and analyzed at ICES.
A service visit for a female fertility consultation was identified using the diagnostic billing code ICD-9 628 in OHIP. The male infertility ICD-9 606 billing code was also included because misclassification by gender has been identified for this code. 18 Treatment information for chemotherapy and radiation was obtained from ALR. Reproductive related cancer surgeries (excluding biopsies) were identified from OHIP using billing codes previously identified by ICES 19 (Supplementary Appendix Table SA1).
Factors included in analyses were informed by those identified previously by Korkidakis et al. 16 and Coleman et al. 17 Data for patient characteristics were obtained from RPDB, including rurality, and quintiles for residential instability, material deprivation, economic dependency, and ethnic concentration. Quintiles are interpreted as marginalization on an ordinal scale from one (least) to five (most). A summated score of marginalization was also calculated, as described by Matheson and van Ingen. 20 Neighborhood income quintiles were also considered and represented on an ordinal scale from one (poorest) to five (wealthiest).
Clinical factors, including age at diagnosis, year of diagnosis (2006–2010, 2011–2015, and 2016–2019), cancer diagnosis, type of treatment (chemotherapy, radiation, and reproductive related cancer surgery), death within 1 year of diagnosis, and geographical region of oncology care, were also examined. Years of diagnoses were grouped into 5-year intervals, with only 4 years available after the start of fertility funding (2006–2010, oncofertility field newly formed; 2011–2015, increasing oncofertility awareness; oocyte cryopreservation available; and 2016–2019, start of government funding for fertility preservation in Ontario).
Cancer diagnoses were defined according to Barr et al. 21 and grouped based on future risk to infertility as follows: low (melanoma, thyroid cancer, and other), moderate (brain tumors, bone and soft tissue sarcomas, breast cancer, and colorectal cancer), and high risk (gynecological cancers, Hodgkin and non-Hodgkin lymphoma, and leukemias). Parity of cases was obtained from MOMBABY.
Analysis
Descriptive statistics were calculated for all demographic and clinical variables. Univariate analyses were completed using one factor logistic regression models with intercepts to assess the relationship of each factor to the outcome event of attending a fertility consultation within 30 days of diagnosis. Correlations between continuous variables were assessed; if variables had a correlation coefficient >0.70, one variable was excluded from multivariate modeling. Significant factors from the univariate analyses were entered into a logistic model using a backward approach, with a two-way cutoff p < 0.05 for inclusion in the model.
Odds ratios (ORs) and confidence intervals (95% CIs) were calculated for the final model. Model fit was assessed using the Hosmer and Lemeshow Goodness of Fit test, 22 Akaike information criterion, and the concordance statistic. Cases with missing data were excluded.
Ethical approval
This study was approved by the Hamilton Integrated Research Ethics Board (HiREB No. 5958).
Results
There were 20,556 AYA females diagnosed with cancer included in the analyses. A considerable (84%) majority of cases did not attend a fertility consultation within 30 days of diagnosis. Most cases had a cancer considered to be of a low risk to fertility (46%), with 29% and 25% having a cancer of moderate or high risk to fertility, respectively (Table 1). Fertility consultation increased over time from 4% in 2006 to 13% in 2019 (Fig. 1).
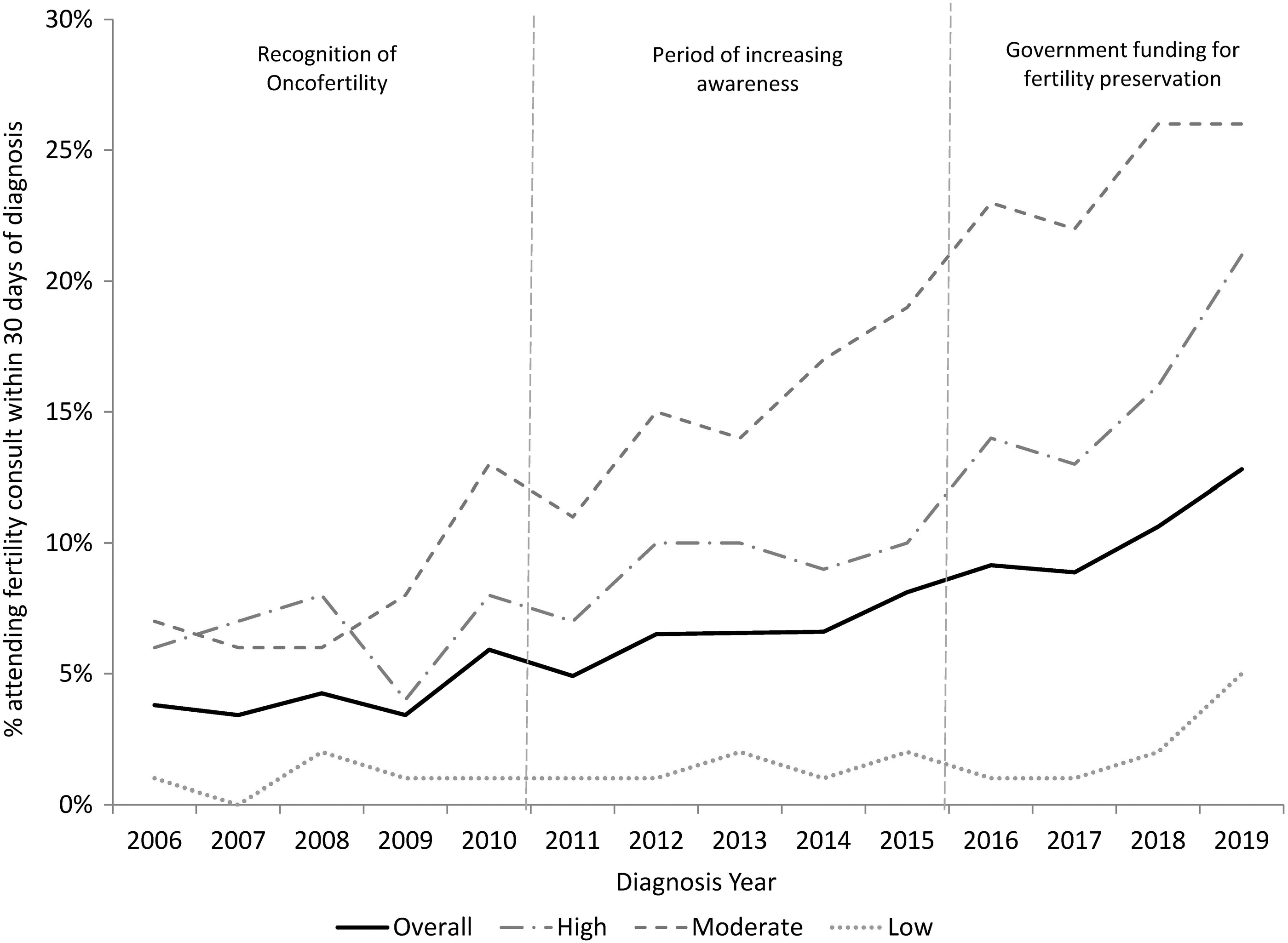
Percentage of AYA females with cancer attending a fertility consultation within 30 days of diagnosis, by year of diagnosis.
Clinical and Demographic Statistics, Females Aged 15–39 Years Diagnosed with Cancer in Ontario, Canada (N = 20,556)
Residential instability represents number of people in a neighborhood living alone, and with a higher proportion of rented dwellings and apartment buildings; ethnic concentration represents number of people in a neighborhood who are recent immigrants and/or people belonging to a “visible minority”; material deprivation represents number of people in a neighborhood who are not able to access and attain basic material needs calculated based on income, quality of housing, education level, and family structure; dependency quintile represents number of people in a neighborhood who are in uncompensated work or receiving a disability pension.
Univariate results
All factors were significantly associated with attending a fertility consultation (p ≤ 0.006), with a concordance statistic >0.50. The material deprivation and income quintile were correlated (r = 0.73; p < 0.0001), therefore, the material deprivation quintile was dropped from modeling and the income quintile was retained because of a lower percentage of missing data. Also, because the Ontario Marginalization Summary Score is an index of the ethnicity concentration, economic dependency, residential instability, and material deprivation quintiles, it was dropped from further modeling as it had the lowest concordance value of the associated variables and small cell sizes (Supplementary Appendix Table SA2).
Multivariate results
A total of 19,729 of 20,556 cases were included in multivariate analyses, 827 cases were excluded due to missing data. The backward elimination was completed in three steps, with the Ontario rurality index (step 1 p = 0.72), reproductive related surgery (step 2 p = 0.39), and ethnic concentration quintile (p = 0.13) removed from the final model. The Hosmer and Lemeshow Goodness of Fit test indicated that the final model fit the data well (p = 0.979). Point estimates for ORs and 95% CIs for final model parameters (Supplementary Appendix Table SA3) are shown in Figure 2.
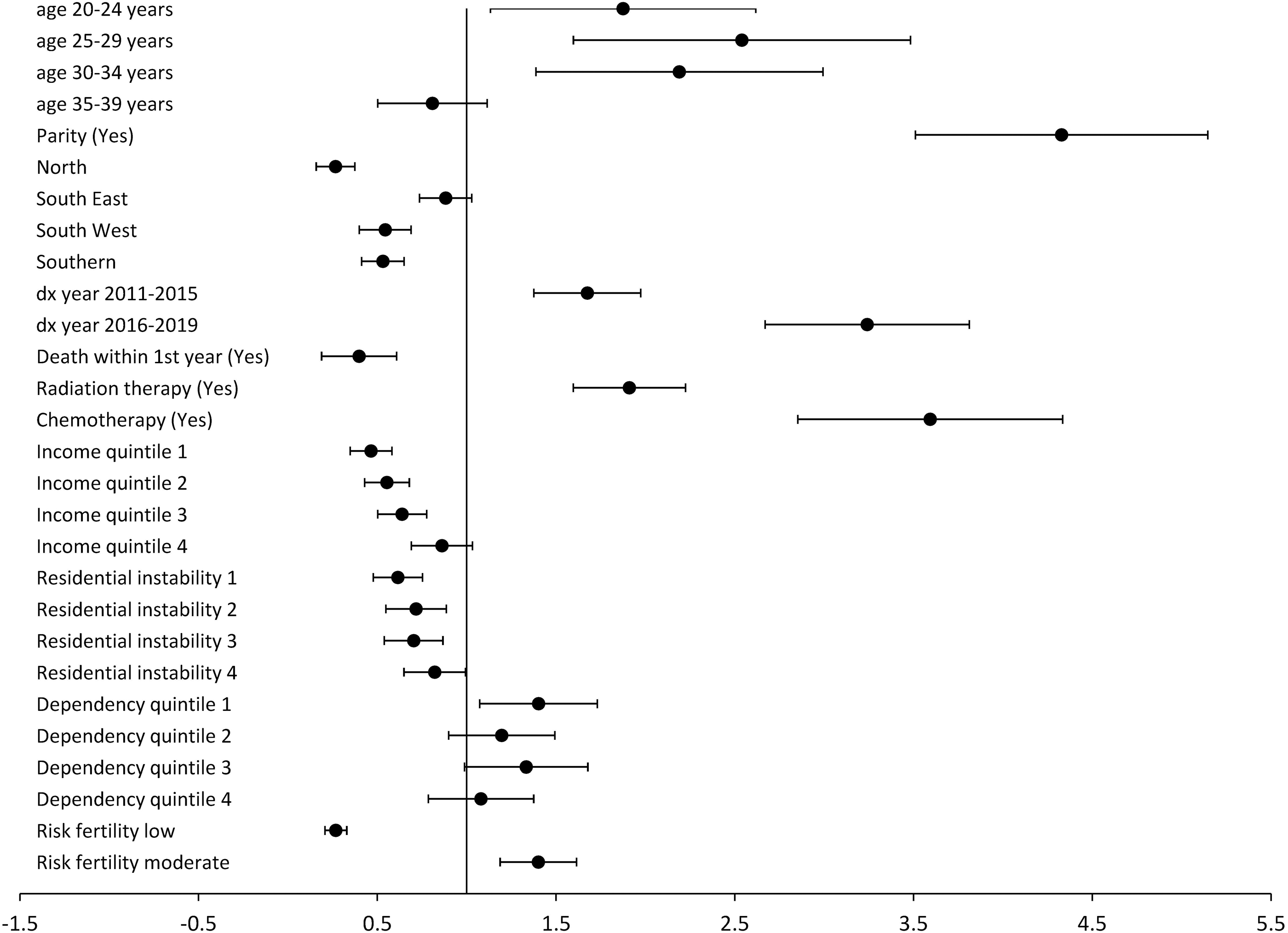
Adjusted odds ratios and 95% confidence intervals for multivariate logistic regression with factors regressed on attending a fertility consultation within 30 days of diagnosis for females 15–39 years of age at diagnosis. Note: Reference categories: age at dx 15–19 years; region central; dx year 2006–2010; income quintile 5 wealthiest; residential instability 5 most marginalized; dependency quintile 5 most marginalized; risk to fertility high. dx, diagnosis.
Effect sizes with increased odds of attending a fertility consultation within 30 days of diagnosis were greatest for not currently having children (OR = 4.3; 95% CI [3.6–5.1]), later years of diagnosis (OR = 3.2; 95% CI [2.8–3.8]), and having undergone chemotherapy (OR = 3.6; 95% CI [3.0–4.3]) or radiation therapy (OR = 1.9; 95% CI [1.6–2.2]). Having a cancer with lower risk to fertility (OR = 0.3; 95% CI [0.2–0.3]), death within a year of diagnosis (OR = 0.4; 95% CI [0.3–0.6]), and residing in a northern region of Ontario (OR = 0.3; 95% CI [0.2–0.4]) were associated with being less likely to attend a fertility consultation.
Lower income (OR = 0.5; 95% CI [0.4–0.6]) and marginalization in residential instability (OR = 0.6; 95% CI [0.5–0.8]) were also associated with being less likely to attend a fertility consultation. Being less marginalized within the dependency quintiles (OR 1.4; 95% CI [1.1–1.7]) was associated with an increased likelihood of attending a fertility consultation.
Discussion
The results of this study identified factors associated with attendance at a fertility consultation within 30 days of diagnosis by female AYAs (females 15–39 years of age) with cancer. The findings were consistent with previous study in females with breast cancer and lymphoma.16,17 Overall, the proportion of females attending fertility consultations was 7% (10.2% in the most recent period, 2016–2019), similar to previously reported rates for breast cancer (8.0%) 16 and lymphoma (10.7%). 17 Increasing attendance at consultations over time was also consistent with previous reports.16,17
Despite improvements over time, rates remain low with important disparities related to clinical and sociodemographic factors. Parity and marginalization in sociodemographic factors were associated with a lower likelihood of attending a fertility consultation. Other important factors, including year of diagnosis, cancer diagnosis risk to fertility, treatment modalities, and geographic region are discussed hereunder.
Year of diagnosis was an important factor associated with fertility consultations, with proportion of females attending consults increasing steadily over time. The oncofertility term was first defined in 2006 by Woodruff, suggesting little awareness in our earliest time period examined. 23 During the time period of 2011–2015, many events occurred to help raise oncofertility awareness with patients and healthcare providers. In 2010 and 2012, the Canadian Task Force on AYAs with cancer held international stakeholder workshops.12,13
The first workshop resulted in the publishing of principles and recommendations for care of AYAs with cancer, as well as a supplement in cancer addressing the important topics discussed at the workshop including oncofertility.12,24 Also, in 2014 a dedicated AYA oncology program at the Princess Margaret Cancer Center was established. 25 Funding for fertility preservation was implemented in Ontario in December 2015, greatly reducing financial barriers. However, increases in uptake of consultations after funding were not as substantial as reported in males with cancer. 26 This may reflect differences in uncovered costs.
The Ontario Fertility Program provides funding for one cycle of fertility preservation and in vitro fertilization (IVF). However, drug and storage costs are not covered. Drugs for females can cost upward of $5000 per cycle and storage costs are $250–$500 per year of eggs/embryos.27,28 Another factor likely associated with improving rates may be the approval of oocyte cryopreservation for nonexperimental use in 2013. 29 Since this method does not require a contemporaneous sperm donor, this option may reduce barriers for younger patients who are not yet in long-term relationships. 29 Advocacy and research targeted at females with cancer in Ontario may have also played an important role in the steady upward trend observed in this study.30,31
Risk to fertility based on cancer diagnosis was also an important factor. It has been suggested that detailed treatment information should be used to determine fertility risk. 32 However, this approach was infeasible for this study because administrative data in Ontario are not detailed enough to allow this classification. This lack of detail is a barrier to more in-depth exploration of treatment risks to fertility. However, despite the broad nature of the classification, “risk to fertility” was still an important factor.
Females with cancers having moderate risk to fertility were more likely to attend fertility consultations (13.1%) than those with cancers having a higher risk to fertility (9.2%). This unexpected difference may be attributable to a focus on fertility in females with breast cancer who comprised 70% of the moderate risk cases in this study. Much research has focused on this subgroup of patients in relation to fertility, including the development of breast cancer-specific decision aids for fertility preservation.31,33,34 Srikanthan et al. 30 also found that a dedicated program for breast cancer patients helped improve fertility referrals, suggesting that cancer-specific approaches may be effective methods for improving uptake of fertility consultations.
The institutions where these decision aids were developed and dedicated breast cancer fertility program was implemented are both located in Toronto, Ontario.30,31 These institutions treat a large proportion of AYA-aged breast cancer patients in Ontario, likely having substantial influence on the results of our Ontario-based study. Therefore, disease-related finding may not be generalizable to other provinces or countries.
Surprisingly, females who underwent reproductive related surgeries were not more likely to attend a fertility consultation, and this was not a significant factor in the final model. Surgery to reproductive organs and radiation to either the pelvic area or the hypothalamic–pituitary–gonadal axis can lower fertility rates in female cancer survivors.11,35 It would, therefore, be expected that this group would have some of the highest rates of referral for fertility consultation given the nature of their cancer. 36 In a recent review of the literature, examining quality of life and fertility preservation counseling for females with gynecological cancers, it was noted that fertility preservation has an impact on both quality of life and psychological well-being in survivors. 9
It is important to better understand the lower consultation rates in females undergoing reproductive related cancer surgeries (7.7%) compared with the other treatment modalities, chemotherapy (11.7%) and radiation therapy (11.6%). Females diagnosed with gynecological cancers were also found to have a lower fertility consultation rate (9.9%) than other cancers, such as breast cancer (25.1%), suggesting that females with gynecological cancers are less likely to attend a consultation regardless of treatment received. 18 One possible explanation for this difference may be females with gynecological cancers tend to receive care from gynecology–oncology specialists.
This type of specialist would likely be more knowledgeable about fertility preservation than some other types of oncologists potentially negating the need to see a fertility specialist for consult. Using other metrics such as the uptake in fertility preservation procedures might show a greater use of fertility services in patients with gynecological cancers and warrants further exploration.
Another important factor in attending a fertility consultation was geographical region of care. Females with cancer in northern Ontario were 70% less likely to attend a consultation than females being treated in central and southern Ontario. Fertility preservation for females requires specialized IVF clinics, none of which is located in northern Ontario. 37 Results in this study were consistent with those found in females with breast cancer, with <1% of females attending fertility consultations who were treated in northern regions of the province. 16
Rashedi et al. 38 examined fertility preservation options for patients with cancer globally, noting that lack of providers was a specific barrier to fertility preservation in Canada. Given the large geographic area of the province of Ontario, travel distance and costs may present a major challenge for females living in northern regions to access fertility preservation before the start of treatment.
Although this study had many strengths and represented a large population of AYA aged females with cancer, it does have some limitations. Sociodemographic information was not available at the individual case level but was representative of the neighborhood in which the individual resided. Demographic data at the individual level could provide more accurate results as well as further insight into differences in fertility consultation rates by race, gender, and educational attainment. Information was also not available on cancer staging or risk that may impact the timing of treatment that may be an important factor in a patient's decision to seek fertility consultation.
Another potentially important factor in uptake of fertility consultations that could not be examined is the type of oncologist or nature of the institution a patient was treated at. Knowledge may vary by specialty negating the need for a consult, and institutional resources vary. For example, pediatric cancer centers or teaching hospitals may have greater supports or programs in place to help patients make decisions regarding fertility preservation that could influence uptake of fertility consultations. We were unable to examine hospital type due to the amount of missing data for this variable. 18
Also, this study only examined consultations for fertility that does not account for those females who are referred for fertility preservation or who go on to receive fertility preservation. Capturing further information about fertility services in administrative databases could greatly inform the field of oncofertility in Ontario, as well as ensure equitable distribution of services. This study was conducted in a single province in Canada that is representative of ∼38% of the population. Owing to geography and specific policies around funding for fertility preservation unique to this province, results may not be generalizable to other provinces within Canada or countries, and further investigation is warranted to explore factors associated with attending fertility consultations both nationally and internationally.
Conclusions
Although improvements are being made in oncofertility care for females shown by increasing uptake of fertility consultations over time, rates remain low. This study also highlighted disparities in clinical and demographic factors influencing the attendance at fertility consultations within 30 days of diagnosis. The factors identified in this study can be used to inform implementation of various strategies, such as targeted decision aids, specialized programs, and oncofertility models of care, to help improve consultation rates for fertility preservation before treatment in females with cancer.
Footnotes
Authors' Contributions
C.R. contributed to conceptualization, methodology, formal analysis, writing—original draft, and visualization. R.D.B. was involved in supervision and writing—review and editing. H.S. carried out supervision and writing—review and editing. A.C. was in charge of supervision and writing—review and editing.
Disclaimer
The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources including Ontario Ministry of Health (MOH), Ministry of Long-Term Care (MLTC), Ontario Health (OH), and Canadian Institute for Health Information (CIHI); no endorsement is intended or should be inferred.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant of the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by Ontario Ministry of Health (MOH), Ontario Health (OH), and Canadian Institute for Health Information (CIHI). This study is part of Charlene Rae's doctoral thesis “Metrics for Evaluating System Level Change in Adolescent and Young Adult (AYA) Cancer Care in Canada” completed at McMaster University 2021 (![]() ).
).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.