
Abstract
More than 1000 Australian adolescents and young adults (AYAs) are diagnosed with cancer annually. Many report unmet social well-being needs, which impact their mental health. Australian AYA cancer care providers lack guidance to address these needs well. We aimed to develop guidelines for caring for the social well-being of AYAs with cancer in Australia. Following the Australian National Health and Medical Research Council guidance, we formed a multidisciplinary working group (n = 4 psychosocial researchers, n = 4 psychologists, n = 4 AYA cancer survivors, n = 2 oncologists, n = 2 nurses, and n = 2 social workers), defined the scope of the guidelines, gathered evidence via a systematic review, graded the evidence, and surveyed AYA cancer care providers about the feasibility and acceptability of the guidelines. The guidelines recommend which AYAs should have their social well-being assessed, who should lead that assessment, when assessment should occur with which tools/measures, and how clinicians can address AYAs' social well-being concerns. A key clinician, who is knowledgeable about AYAs' developmental needs, should lead the assessment of social well-being during and after cancer treatment. The AYA Psycho-Oncology Screening Tool is recommended to screen for social well-being needs. The HEADSSS Assessment (Home, Education/Employment, Eating/Exercise, Activities/Peer Relationships, Drug use, Sexuality, Suicidality/Depression, Safety/Spirituality Assessment) can be used for in-depth assessment of social well-being, while the Social Phobia Inventory can be used to assess social anxiety. AYA cancer care providers rated the guidelines as highly acceptable, but discussed many feasibility barriers. These guidelines provide an optimal care pathway for the social well-being of AYAs with cancer. Future research addressing implementation is critical to meet AYAs' social well-being needs.
Introduction
More than 1000
These ongoing social and emotional challenges have an immense cost on young people's well-being, and also on the Australian society as a whole, with the estimated lifetime cost of reduced workforce participation among AYA cancer survivors totaling $290.1 million. 5
The Youth Cancer Services (YCS) have been developed to provide support to address AYAs' social and emotional needs during and after cancer treatment, through use of the Psychosocial Care Manual pathway. 6 However, data evaluating the implementation of this framework have found that psychosocial staffing shortages, 7 coupled with Australian oncology health care providers underestimating the range and depth of AYAs' psychosocial concerns, 8 have left Australian AYAs with cancer continue to report unmet social needs, such as challenges navigating engagement with education or work, as well as poor mental health, long after their treatment has concluded.
Internationally, guidelines have been key first steps in addressing unmet needs and upskilling health care professionals, on the path toward improving the psychosocial care of young people with cancer.9–14 While there is international consensus that AYA cancer care should include a multidisciplinary team of medical and psychosocial health care professionals and that AYAs should be provided accessibly and equitable care for their psychosocial needs from diagnosis through survivorship, 15 there is no evidence to support the applicability or efficacy of existing international guidelines within the Australian health care system.
This is problematic because Australia's model of care for AYAs with cancer is quite different from those across the United States, Canada, and the United Kingdom, and the age ranges to which AYA cancer care and resources cater are different. 15 Through the YCS, Australian AYAs with cancer have access to an AYA-specialized multidisciplinary team of cancer care experts through major hospitals across the country, but they must be treated within the pediatric or adult wards. Australia also has a unique geographic distribution, with the major proportion of the population concentrated around coastlines of the country, and vast amounts of rural area occurring in between, requiring many AYAs to travel significant distances to access cancer care.16,17 While the United Kingdom has a similar national youth cancer service, they have the added advantage of dedicated teenage and young adult cancer wards available at hospitals across the country.
The United Kingdom is also much smaller than Australia and does not pose as many geographic challenges to accessing AYA cancer care.15,18 Lastly, in the United States and Canada, there have been guidelines and frameworks established to guide youth cancer care, but there is no singular, national youth cancer service to promote adherence to those guidelines and frameworks, as in the United Kingdom or Australia.11,12,19 To build on an international body of work6,11,18,20–23 and address both young people's unmet care needs and health care professionals' skill/knowledge needs, we aimed to develop specific guidelines for caring for the social well-being of AYAs with cancer in Australia.
Methods
As there is no consensus on how the social impacts of a cancer diagnosis on AYAs should be defined and measured, 22 for the purpose of these guidelines, we use the term social well-being, drawing from the model proposed by Ferrell et al., in which social well-being encompasses the following domains: family distress, roles and relationships (peers, romantic partners, and family), affection/sexual function, appearance, employment/education, and finances. 24
Developing the guidelines
We followed the steps recommended by the Australian National Health and Medical Research Council (NHMRC) guidance on developing clinical guidelines (Fig. 1).
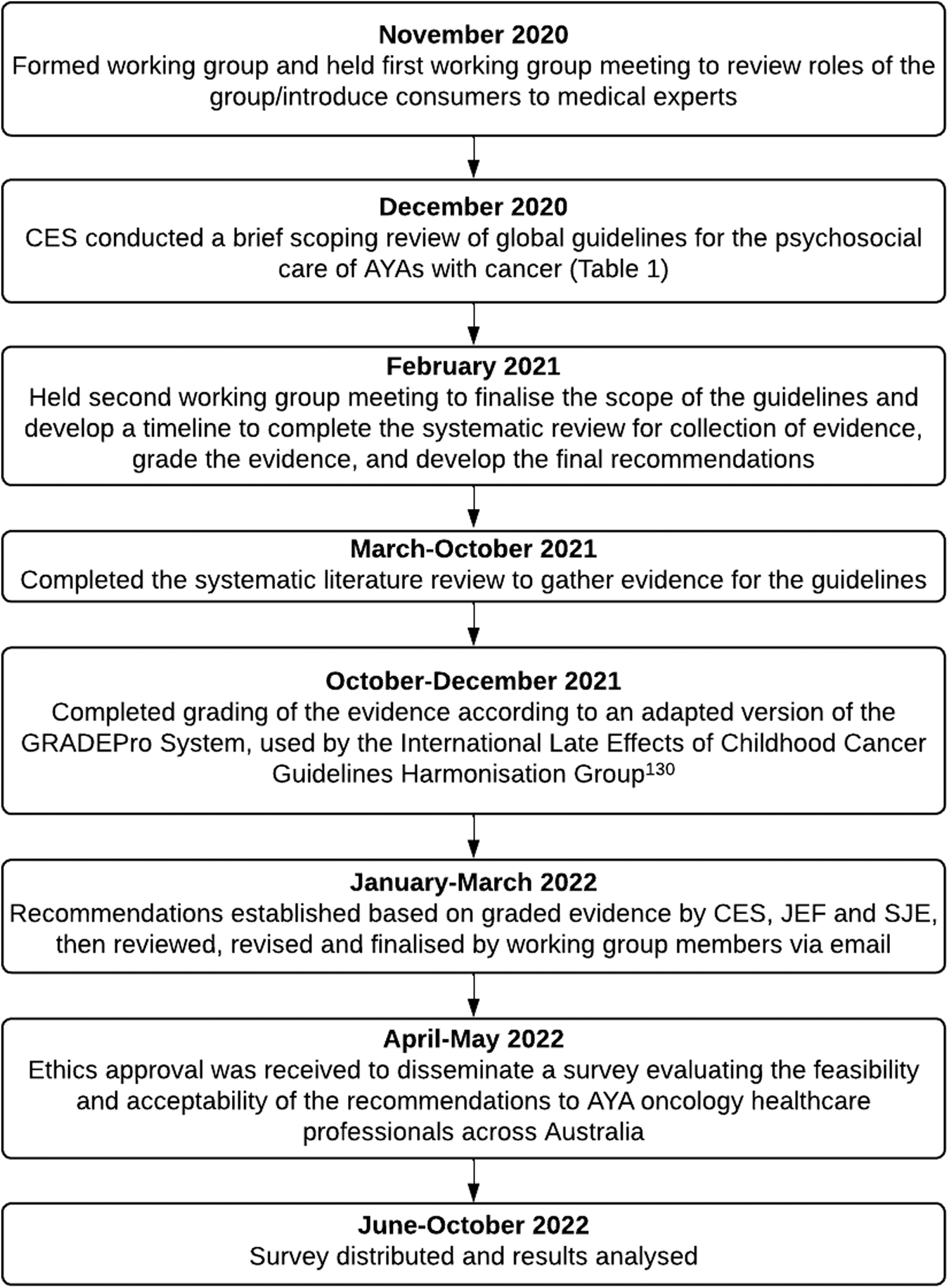
Developing the guidelines.
In November 2020, 18 individuals joined the working group: 4 psychosocial researchers, 4 psychologists, 4 AYA cancer survivors, 2 oncologists, 2 nurses, and 2 social workers. Two working group meetings were held via Microsoft teams in November 2020 and February 2021, to agree on the plans for and scope of the guidelines, with the remainder of the finalization of the guidelines occurring via email to accommodate members' varying schedules.
The scope of the guidelines was determined by identifying key gaps across existing international guidelines for the psychosocial care of AYAs with cancer (reviewed in Table 1). We focused on outlining for what country the guidelines/standards of care were developed, when they were developed, and what the guidelines/standards of care suggested specific to assessing and addressing the social well-being AYAs with cancer. With the exception of the UK's Teenage Cancer Trust Blueprint for Care 18 and the Canteen Australia Psychosocial Care Manual, 6 most guidelines did not explicitly address social well-being in the context of AYA cancer care. Rather, most guidelines grouped social well-being under psychosocial well-being (as a combination of social and emotional well-being).10–12,17,21
Overview of International Guidance on Caring for the Social Well-Being of Adolescent and Young Adult Cancer Patients and Survivors
AYAs, adolescents and young adults; HEADSSS Assessment, Home, Education/Employment, Eating/Exercise, Activities/Peer Relationships, Drug use, Sexuality, Suicidality/Depression, Safety/Spirituality Assessment.
Few existing guidelines provided recommendations on time points when assessment of social well-being should occur, and where such recommendations were made, they differed across guidelines. In addition, only two sets of guidelines from the United States and Australia discussed risk factors that might indicate which AYAs are most likely to experience poor social well-being and should therefore have their social well-being particularly closely monitored.6,11,12 Only two guidelines from the United Kingdom and Australia recommended measures or questions to assess social well-being,6,18 of which the qualitative Home, Education/Employment, Eating/Exercise, Activities/Peer Relationships, Drug use, Sexuality, Suicidality/Depression, Safety/Spirituality (HEADSSS) Assessment interview was the only similar recommended measure across both guidelines. No recommendations exist for more brief quantitative screening tools.
Lastly, there were also inconsistencies in terms of whether, and how, existing guidelines provided care pathway recommendations based on evidence versus expert opinion. We therefore aimed to address these gaps by developing evidence-based guidelines that provide clear recommendations on the following:
Aim 1: When should assessment of social well-being occur for AYAs diagnosed with cancer?
Aim 2: What risk factors (clinical, demographic, and social) should be used to identify AYAs with cancer in need of surveillance of social well-being?
Aim 3: Which validated measures should be used to assess social well-being among AYAs with cancer?
Aim 4: Which models of care/care pathways/interventions are effective to address social well-being concerns or deficits among AYAs with cancer?
Systematic review
Following finalization of the scope of the guidelines, we conducted a systematic literature review to gather evidence for the guidelines (Fig. 2).
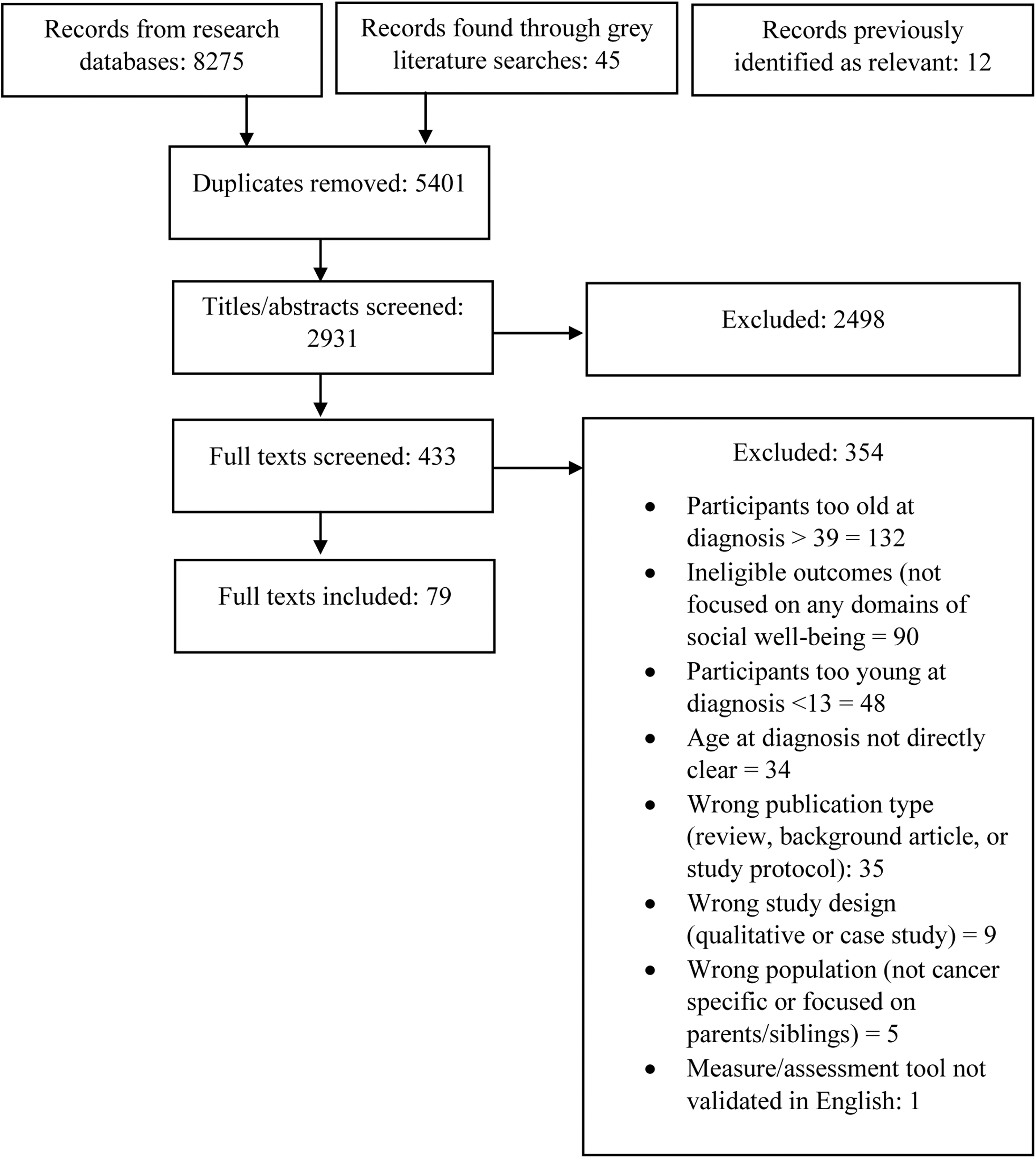
PRISMA diagram 30 of review outcomes. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Literature search
C.E.S. registered the protocol for this systematic review with PROSPERO in February 2021 (CRD42021227407). We developed the search strategy collaboratively, in consultation with a medical research librarian (Table 2). Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses framework, 25 C.E.S. searched MEDLINE, PsycINFO, PsycTESTS, EMBASE, CINAHL, and Google on January 7, 2021, for publications dated 2000–2021. We opted to include studies from as early as 2000 because the international shift toward recognizing the specific psychosocial needs of this age group and the importance of providing them age-appropriate care began in the early 2000s, particularly in the United Kingdom, and we did not want to miss any relevant publications from that early time period.26,27
Search Terms
C.E.S. conducted an updated search on October 8, 2021, to identify any relevant articles published since January. Reference lists of included publications were also hand searched for any additional publications not identified through electronic searches.
Inclusion and exclusion criteria
Included studies were those that focused on any aspects of social well-being of young people with cancer falling under our definition, were peer-reviewed published in English, and those that use either quantitative or mixed-methods research designs. The mean age at diagnosis must be 13–40 years old. While this is broader than the range of 15–25 used in Australia for youth cancer care, it was used to capture literature published in Canada, the United States and the United Kingdom where the age ranges extend between 13 and 40. 28 Studies involving both AYAs receiving and completed treatment were included, given social well-being may be disrupted at any stage of treatment or survivorship. Gray literature was also included, such as AYA cancer care manuals, standards, recommendations, and position statements, and other guidelines were also included.
Exclusion criteria included systematic reviews and meta-analyses, purely qualitative studies (considering the system we use to grade the quality of evidence collected ranks qualitative studies as very low-quality evidence in comparison with quantitative studies),29,30 studies including participants without a history of cancer, and studies that were individual case studies or small case series (i.e., <10 participants) excluded.
Data extraction
All abstracts and full-text articles were double screened by C.E.S. and one of the collaborators (S.J.E.) independently, using RAYYAN systematic review software. Discrepancies were discussed until an agreement was reached (k = 0.98), C.E.S. extracted data from full texts in Excel.
Recommendation development
Quality assessment and evidence grading
We conducted quality assessment using an adapted version of the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system published by the International Late Effects from Childhood Cancer Guideline Harmonization Group.29,31,32 We used the GRADE Profiler online tool 30 to generate tables summarizing these findings. C.E.S., S.J.E., and J.E.F. conducted the evidence grading collaboratively, through discussion of each potential guideline item and its related evidence, across each research question. Given the high degree of variability in ways in which publications reported on similar outcomes, we generated a narrative summary of findings tables. In keeping with the International Late Effects of Childhood Cancer Guidelines Harmonization Group version of the GRADE system, both clinical and scientific quality and impact of evidence were considered when determining the level and strength of evidence across each factor/guideline item.
Typically, the GRADE system accounts for the difference between an intervention or factor's desirable and undesirable effects (the larger the difference the stronger the recommendation), the overall quality of the evidence (with higher quality warranting stronger recommendation), and resources required to implement the factor/intervention (the more resources required, the weaker the recommendation). 29 However, given the heterogeneity of evidence we gathered, we generated a narrative summary of findings tables, and therefore focused on assigning the strength of a recommendation based on the overall quality of evidence, experience-based clinical relevance, and the resources required. Levels of evidence were assigned as follows: Level A—greater than three studies providing evidence and high clinical relevance of the factor/item based on expert opinion, Level B—less than three studies but high clinical relevance, or Level C—evidence solely stemming from existing guidelines or standards, or from only one study. 31
For items with higher evidence quality (Level A), few resources required for implementation, and for which benefits greatly outweighed risks or burdens, we gave a strong recommendation. For items with moderate-quality evidence (Level B), we gave a strong, moderate, or weak recommendation depending on resources required for implementation and/or the extent to which benefits outweighed risks/burdens. For items with low-quality evidence (Level C evidence), recommendations were either moderate or weak depending on expert opinion. Weak recommendations based on Level C items were excluded from the final list of recommendations.
Evaluating the feasibility and acceptability of the guidelines
After finalization of the guidelines in March 2022 (Fig. 1), we obtained ethics approval for evaluation of the feasibility and acceptability of the recommendations in April 2022 (UNSW Human Research Ethics Committee approval number HC220401). We developed an online evaluation survey using Qualtrics survey software 33 and Slido for PowerPoint. 34 The survey was anonymous and did not collect any demographic or identifying information from participants. For open-ended questions, conventional content analysis was used to identify frequently occurring responses and tabulate the frequency of common responses (those provided by more than one individual).35,36
We distributed a copy of the guidelines along with the evaluation survey via collaboration with Canteen, the national Australian youth cancer nongovernment organization, and the YCS, the national AYA oncology health care service for 15- to 25-year olds. First, Canteen shared the guidelines and evaluation survey via their newsletter to their subscribers. We also shared the guidelines and survey via presentation at a national Youth Cancer Service professional development webinar, as well as at a local level, via presentation to the clinicians of the Kids Cancer Centre, Sydney Children's Hospital.
Results
The literature search identified 2931 unique records, of which 79 full-texts remained included following screening (Fig. 1). We generated a narrative summary of findings table for each research question. Of the 79 full-texts included, types of texts included cross-sectional studies (N = 34),3,37–68 prospective longitudinal studies (N = 8),69–77 scale development and psychometric validation publications (N = 15),78–90 guidelines/standards of care/recommendations (N = 10),10–12,21,91–96 care manuals (N = 2),6,18 frameworks (N = 4),17,19,97,98 an online news article (N = 1), 99 a position statement (N = 3),95,100,101 a program report (N = 1), 102 and a guide for patients (N = 2)13,103 remained included following screening. Publications came primarily from the United States (N = 36),11–13,37,43,44,50,51,53–55,62,68,70,71,74,76,78,83–86,88,90,92,94,95,98–100,102–106 Australia (N = 14),6,10,17,23,38,47,52,56,58,79,89,91,97,101 and the United Kingdom (N = 6).18,39,48,75,81,107
Recommendations
Aim 1: when should assessment of social well-being occur for AYAs diagnosed with cancer?
Evidence for time points at which social well-being should be assessed came from three sets of guidelines/standards of care and three research studies.6,10–12,69,72,74 The guidelines/standards highlighted the importance of assessing psychosocial well-being overall at diagnosis and at major transition points (such as completion of treatment).10–12 The Canteen Australia Psychosocial Care Manual recommended further assessment time points of 2 weeks postdiagnosis, 6–8 weeks postdiagnosis, 1 year post-treatment, and 5 years post-treatment. 6 Three prospective longitudinal studies provided evidence that AYAs' social well-being is compromised between 6 and 12 months postdiagnosis, suggesting the importance of monitoring social well-being during this time frame.69,72,74 Two of these studies also found that social well-being remained compromised around 24 months postdiagnosis, with AYA cancer survivors reporting significantly poorer social well-being than population norms at this stage.72,74
Recommendation 1
It is strongly recommended that screening for social well-being concerns be conducted regularly following diagnosis, including at diagnosis, 6–12 months postdiagnosis, and at major transition points. It is also moderately recommended that screening for social well-being concerns be conducted 24 months postdiagnosis, 1-year post-treatment, and 5 years post-treatment (Table 3).
Time Points for Assessment of Social Well-Being
Aim 2: what risk factors (clinical, demographic, and social) should be used to identify AYAs with cancer in need of surveillance of social well-being?
We identified nine studies and no guidelines/standards of care that provided evidence of demographic risk factors for poor social well-being.37,40,42,46,59,63,64,71,77 Five cross-sectional studies and one prospective longitudinal study reported a significant association between female sex and poor social well-being, or reported significant odds ratios that females were more likely than males to report poor social well-being.40,42,46,59,64,77 Four cross-sectional studies reported discordant associations between age at diagnosis and poor social well-being,37,46,63,71 with two studies reporting associations between younger age at diagnosis and poor social well-being46,71 and two other studies reporting associations between older age at diagnosis and poor social well-being.37,63 Considering these discordant results, our expert working group suggested that age as a risk factor should focus on younger AYA ages 12–14 or older ages 26–39, which are developmentally still within adolescence and young adulthood but are outside of the age range covered by the Australian YCS (15–25).
Two sets of guidelines/standards of care6,11,12 and 10 studies49,50,54,55,61,65,72,74,77,104 reported on clinical risk factors for poor social well-being. Three cross-sectional studies54,55,104 and one prospective longitudinal study 72 reported a significant association between poor physical functioning and poor social well-being. Three cross-sectional studies49,55,104 and one prospective longitudinal study 77 reported significant association between fatigue and poor social well-being. One cross-sectional study 50 reported increased odds of experiencing poor social well-being if AYAs experience cognitive impairment from their cancer treatment, and two sets of guidelines/standards of care6,11,12 reported cognitive impairment as a risk factor for poor social well-being. Clinical complications, such as graft-versus-host disease, were found to be associated with poor social well-being in one cross-sectional study, 104 while two cross-sectional studies identified an association between physically disfiguring diagnoses or treatments (e.g., limb amputation for sarcoma) and poor social well-being.61,65
One set of guidelines/standards of care 6 and six studies41,55,60,72,76,104 reported psychosocial risk factors for poor social well-being. One cross-sectional study 104 and one prospective longitudinal study 76 reported a significant association between increased psychological distress and poor social well-being, while one prospective longitudinal study found increased odds of poor social well-being among AYAs experiencing psychological distress compared with AYAs not experiencing that distress. 72 Past or present mental health concerns were found to be associated with poor social well-being in two cross-sectional studies.40,55 The Canteen Australia Psychosocial Care Manual also identified past or present mental health concerns as a risk factor for poor social well-being, in addition to past or present alcohol or substance abuse. 6
Table 4 presents the summary of findings for risk factors for poor social well-being among AYAs with cancer.
Risk Factors for Poor Social Well-Being
Recommendation 2
It is strongly recommended that, at minimum, AYAs presenting with risk factors for poor social well-being are screened for social concerns on a frequent and regular basis. Key risk factors for poor social well-being include female sex, poor physical functioning, and symptoms of fatigue, cognitive impairment, psychological distress, or past/present mental health condition (e.g., depression). Additional risk factors moderately recommended for frequent and regular screening of social well-being include ages 12–14 or 26–39, those developing physical complications (such as graft-versus-host disease), those with a past/present alcohol/substance abuse problems, and those with diagnoses including sarcoma, head and neck cancer, breast cancer, and acute lymphoblastic leukemia screened for social well-being concerns frequently and regularly.
Aim 3: what validated measures should be used to assess social well-being among AYAs with cancer?
We identified 3 sets of guidelines/standards of care6,10,18 and 36 research studies3,24,51,52,55,57,60,61,79,83–88,90,105,108–124 providing evidence for the use of both brief screening tools and comprehensive assessments to assess social well-being for AYAs with cancer. These tools and assessments have been validated in both AYAs, are publicly available, and are free for clinical use. The AYA Psycho-Oncology Screening Tool (AYA-POST) is the only brief measure of general social well-being (includes less than 10 items assessing social well-being) that has been codesigned by AYAs undergoing cancer treatment, AYA survivors who had completed cancer treatment and AYA oncology health care providers, and has been validated, particularly within Australia.6,79,108
The HEADSSS Assessment is the only comprehensive interview/assessment of AYAs' social well-being we identified. Two sets of guidelines/standards of care recommended its use for AYAs with cancer6,18 and it has been used extensively in the Australian health care context to assess psychosocial well-being in other AYA illness groups (Table 5).123–125
Measures to Assess Social Well-Being in Adolescents and Young Adults with Cancer
Number of items specifically assessing social well-being.
AYA-POST, AYA Psycho-Oncology Screening Tool; FACT-G, Functional Assessment of Cancer Therapy-General; Mini-SPIN, Mini Social Phobia Inventory; MMQL, Minneapolis-Manchester Quality of Life Instrument; N/A, not applicable; PedsQL, Pediatric Quality of Life Inventory; PROMIS, Patient Reported Outcomes Measurement System; QoL-CS, Quality of Life-Cancer Survivors; SF-36, Short Form Health Survey-36; SPIN, Social Phobia Inventory.
Recommendation 3
It is strongly recommended that, in the context of clinical care, the AYA Psycho-Oncology Screening Tool (AYA-POST) be used for brief screening of problems with social well-being, and the Social Phobia Inventory (SPIN) or Mini Social Phobia Inventory (Mini-SPIN) be used for brief screening for social anxiety symptoms (Table 5). For young people reporting clinically significant concerns on either of these measures, the HEADSSS Assessment interview is strongly recommended to gain a more in-depth understanding of young people's concerns. A modified version of the HEADSSS Assessment can be found in the AYA Psychosocial Care Manual and is part of the manual's recommended care pathway.
There are also more comprehensive research measures available to assess young people's social well-being in the context of research studies. Research measures that are strongly recommended include the Pediatric Quality of Life Inventory (PedsQL), the Quality of Life-Cancer Survivors (QoL-CS), the Short Form Health Survey-36 (SF-36), the Patient Reported Outcomes Measurement System (PROMIS), and the Minneapolis-Manchester Quality of Life Instrument (MMQL) (Table 5).
Aim 4: what models of care/care pathways/interventions are effective to address social well-being concerns or deficits among AYAs with cancer?
There are key aspects of clinical care, interventions, and resources that can be followed to both prevent and address social well-being concerns in young people. At a service level, three existing guidelines/standards of care and three research studies provide evidence to suggest that having a multidisciplinary team that is educated on the developmental needs and preferences of AYAs is necessary to appropriately manage AYAs' social well-being.6,11,15,45,66,100 In addition, three sets of guidelines/standards of care and one research study highlight that it is advantageous for this team to meet regularly and for each AYA to be assigned a key clinician who is responsible for coordinating care for their social well-being.6,10,15,17
At an individual level, eight guidelines/standards of care suggested that AYAs diagnosed with cancer should be provided information and support regarding connection to social life outside of hospital and treatment, opportunities for social interaction within hospital, guidance for engaging with education/work, and early referral to a psychologist coupled with regular psychological follow-up throughout treatment and survivorship (Table 6).6,10–13,17,18,96,99,103
Models of Care/Care Pathways/Interventions for Addressing Social Well-Being Concerns
Recommendation 4
To prevent social well-being concerns and promote positive social well-being, it is strongly recommended that quality age-appropriate clinical care, at both the individual and service levels (as detailed in Table 6), is provided. High-quality, age-appropriate clinical care components will differ across settings and according to health system structural differences and resourcing constraints; Table 6 summarizes key components drawn from specific models of care, care pathways, or interventions at both the service and individual levels internationally, with the strength of available evidence connected with each.
A summary of these recommendations is outlined in Figure 3.
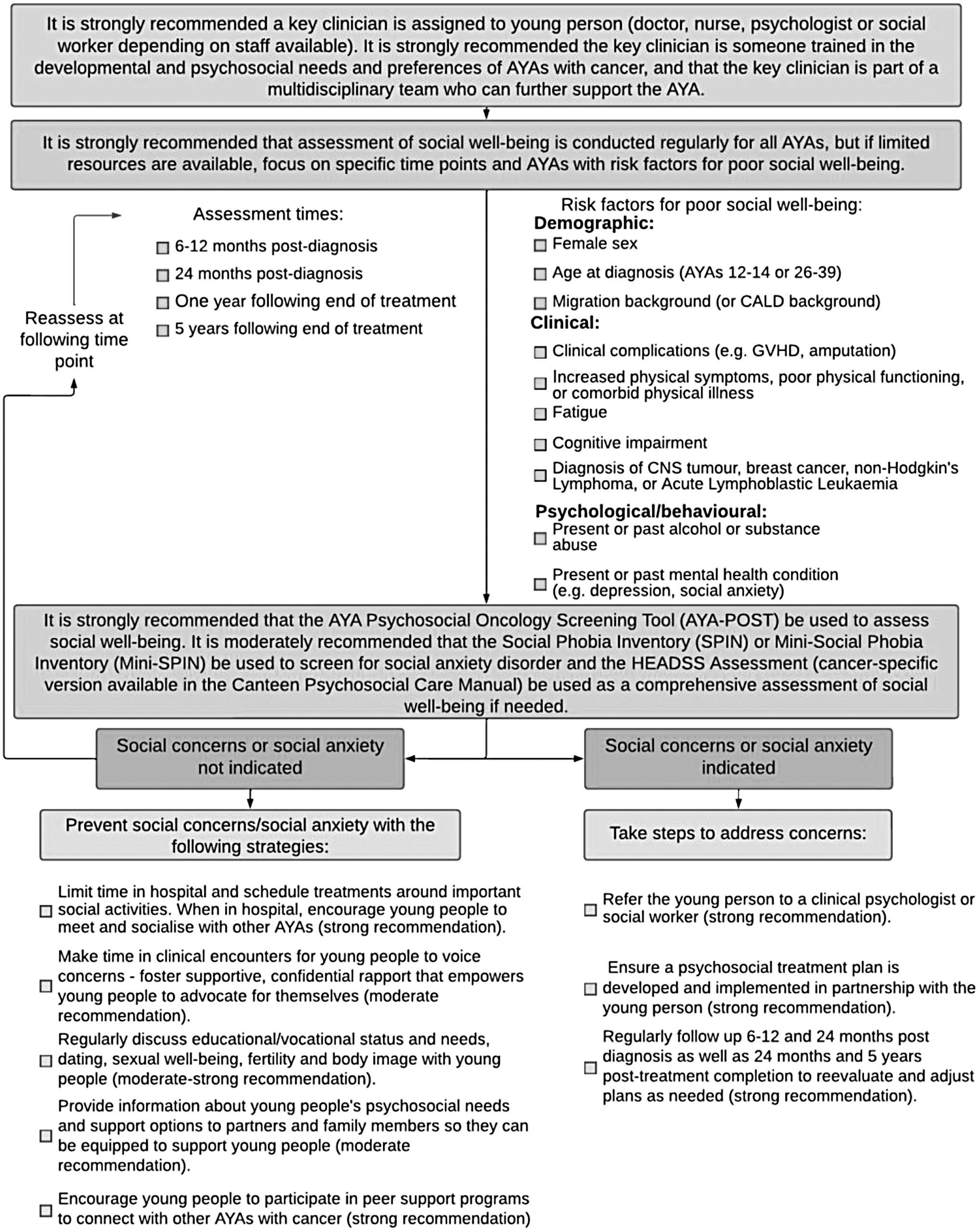
Guidelines for caring for the social well-being of AYAs with cancer in Australia. *AYAs, adolescents and young adults; CALD, culturally and linguistically diverse; CNS, central nervous system; GVHD, graft-versus-host disease; HEADSSS, Home, Education/Employment, Eating/Exercise, Activities/Peer Relationships, Drug use, Sexuality, Suicidality/Depression, Safety/Spirituality Assessment.
Evaluation of the guidelines
A total of 23 AYA oncology health care professionals completed the evaluation survey. The guidelines were rated highly acceptable, with 65% of health care professionals reporting they were somewhat or very likely to implement the guidelines in their own work/clinical practice. However, several barriers and concerns related to the feasibility of this implementation were described, including limited time and private spaces to conduct in-depth assessments (Table 7).
Feasibility of Implementation: Barriers and Concerns
Participants were able to endorse multiple response options per question, therefore percentages of responses to each question can total more than 100%.
Discussion
We provide evidence-based and expert-based recommendations for caring for the social well-being of young with cancer in Australia, aged 13–40 years. These guidelines were developed following the Australian NHMRC Guidelines, involving an expert working group, systematic literature review, and gold standard evidence grading using an adapted version of the GRADEPro system.29–31,126 These guidelines aim to build on the existing psychosocial support services provided through the Australian Youth Cancer Framework and in accordance with the Australian AYA Oncology Psychosocial Care Manual. 20
To date, social well-being remains a significant area of unmet need for young people with cancer in Australia, and young Australians prioritize improvements in care for their social well-being.6,22,23,127–129 Although the Youth Cancer Framework has enabled significant strides in the psychosocial care provided to young people with cancer across Australia, there continue to be gaps experienced by young people who are not able to access quality age-appropriate care for their social well-being due to the geographic location, limited psychosocial services available at certain hospitals, and/or being treated in pediatric or adult environments where some health care professionals may not be aware of the specific psychosocial needs of this age group.8,15,52,108
To optimize resources available and overcome any limitations imposed by lack of access to AYA-specialized cancer care professionals, the goal of these guidelines is to empower all members of the oncology health care teams, as well as community general practitioners, to participate in caring for young people's social well-being.
Evaluation of these guidelines indicates that while the recommendations are acceptable, barriers to their feasibility that we identified are consistent with findings from studies on international implementation of patient-reported outcome measures in the oncology care setting. International studies on implementation of patient-reported outcome measures have identified feasibility limitations including the time required to conduct the screening and follow-up care, clinicians' limited knowledge about how and when to conduct social well-being screening, and the need for any screening time points, tools, and follow-up procedures to be integrated into the electronic medical records. 130 Further research trialing implementation of these guidelines may be useful to identify ways to overcome barriers to their feasibility and subsequently improve the uptake of the guidelines' recommendations by health care professionals.
Limitations
These guidelines are limited by the reliance on existing guidelines and standards as well as poorer quality cross-sectional studies, resulting in the predominance of Level B evidence and moderate recommendations based on expert opinion. In addition, although there have been significant advances in the understanding of the psychosocial impact of cancer treatment on AYAs, there were very few interventions available specifically focused on social well-being. In addition, many existing studies and guidelines/standards do not specify optimal methods for caring for young people's social well-being, with many broadly discussing “psychosocial well-being,” but focusing more on distress and emotional well-being.
Lastly, the sample size involved in the evaluation of these guidelines was small and we did not collect demographic or identifying details from participants, and therefore, it is not possible to know whether participants are representative of Australian AYA cancer health care providers. We were also unable to determine the response rate for the evaluation survey as the recruitment for the survey involved both word of mouth and email distribution, so we cannot be certain of the number of professionals who received and were eligible to complete the survey. Despite these limitations, these guidelines provide the first set of evidence-based recommendations for caring for the social well-being of AYAs with cancer in Australia.
Clinical implications
It is widely acknowledged that clinical guidelines alone are insufficient for creating true clinical practice change.131,132 These guidelines provide a critical first step toward change by clearly outlining what optimal care for the social well-being of young people with cancer should comprise, regardless of the young person's cancer diagnosis, treatment type, or treatment center.
Effective guidelines are those that improve both the care process and outcomes of patients receiving care.131,132 Implementation of patient-reported outcome measures, such as screening for social well-being concerns, may facilitate increased clinician awareness of changes in a patient's psychosocial status, shared decision-making, and doctor–patient communication.133,134 There is also some evidence to suggest that exposure to and uptake of psychosocial supportive care and resources can contribute to improved self-efficacy, quality of life, and psychosocial well-being.135,136 However, methods of delivering psychosocial supportive care may impact whether or not that care contributes to positive patient outcomes. There is currently a lack of consensus around optimal methods for delivering psychosocial care pathways such as that recommended in the guidelines, with discordance across results from technology and face-to-face delivered care/interventions.137,138
Therefore, future implementation studies of these guidelines should also identify how Australian AYAs prefer for this care pathway to be delivered, particularly in regard to technology-based versus face-to-face delivery methods.
Conclusions
Therefore, the future success of these guidelines for caring for the social well-being of AYAs with cancer in Australia will require working closely with AYA oncology health care professionals and cancer centers to ensure that appropriate training can be provided to all members of the care team. The recommended care pathway outlined in the guidelines will also need to be adapted to overcome site-specific feasibility barriers, such as staffing, time, space, and skill-related needs, and to ensure that assessment of social well-being facilitates positive change to patient care. If successful implementation of these guidelines can be achieved, they may facilitate protection and promotion of optimal long-term social well-being for young Australians with cancer.
Footnotes
Acknowledgment
This work was included in the dissertation of C.E.S., submitted to the University of New South Wales, in fulfillment of the degree of Doctor of Philosophy, awarded February 23, 2023.
Authors' Contributions
C.E.S.: conceptualization, investigation, formal analysis, project administration, and writing: original draft and editing; U.M.S.-D., J.E.F., T.N.T., and A.C.A.: supervision, investigation, and writing: review; S.J.E., Az.A., T.L., F.M., C.E.W., S.L., E.B., K.L., A.R., Ad.A., T.K., N.H., S.T., P.P., and F.M.D.: conceptualization, investigation, supervision, and writing: review.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
C.E.S. is supported by a Research Training Program Scholarship from the Australian Government, a PhD Top-Up Scholarship from the Kids Cancer Alliance, and a PhD Top-Up Scholarship from the Kids to Adults (K2A) Clinical Academic Group, which is part of Maridulu Budyari Gumal, The Sydney Partnership for Health, Education, Research & Enterprise. J.E.F. is supported by the Kids Cancer Project. C.E.W. is supported by the NHMRC (APP2008300). U.M.S.-D. is supported by the Cancer Institute of NSW (ID: 2020/ECF1163) and the NHMRC (APP1111800).