
Abstract
Adolescent and young adults (AYAs) require support from their parents and caregivers. While there are formal programs available for patients with complex medical problems, <20% of pediatric practices are performing transition readiness processes in patients aged 12–17 years to effective transition. Although cancer is the most common cause of disease-related death in AYAs in high-income countries, AYA oncology patients have not attained the same clinical improvements as pediatric patients, and their outcomes remain poorer. While there are published data on an expected degree of lag time for patients presenting with solid tumors, due to the underlying biology and slow growth of the cancer, we have recently witnessed extreme delays in the presentation to medical care. In this article, we share the cases of two young adults.
Introduction
Although some formal health transition exists from pediatrics to adult care, gaps remain in health care transition, and adolescent and young adult (AYA) patients often still require support and guidance from their parents and adult caregivers. 1 Adolescent patients with complex medical issues are frequently involved in a dedicated program to ensure a smooth transition as they move to adult medicine providers.2–4 There have been several studies that have looked at patients with chronic conditions, such as sickle disease, and documented the importance of smooth transition of care from pediatric to adult medicine. 5 However, for healthy pediatric patients, the transition to adulthood is often left to the patient and family to navigate. Despite published guidelines, the most recent parentally completed National Survey of Children's Health (2019–2020) found that only 17.6% of pediatric practices are performing transition readiness processes in patients aged 12–17 years to effective transition. 6
Cancer is the most common cause of disease-related death in AYAs in high-income countries. 7 According to the National Cancer Institute, AYA patients comprise all patients between the ages of 15 and 39 years. AYA oncology patients have not attained the same clinical improvements as pediatric patients, and their outcomes remain poorer.8,9 Although previously believed to be due to the underlying biology of the cancer subtypes, this observation probably reflects a combination of biology and contributing psychosocial factors.
The Children's Hospital at Montefiore is the only tertiary care pediatrics hospital in the Bronx. We care for a wide array of patients and their families, mainly from low socioeconomic status. We have observed several AYA patients who are either expected to take over their medical care as they enter college or do not ask their parents for help because they do not see themselves as children. This has resulted in extreme presentations of solid tumor cancer. While there are published data on an expected degree of lag time for patients presenting with solid tumors such as Ewing sarcoma, due to the underlying biology and slow growth of the cancer, we have recently witnessed extreme delays in the presentation to medical care. 10 In this article, we share the cases of two young adults.
Cases
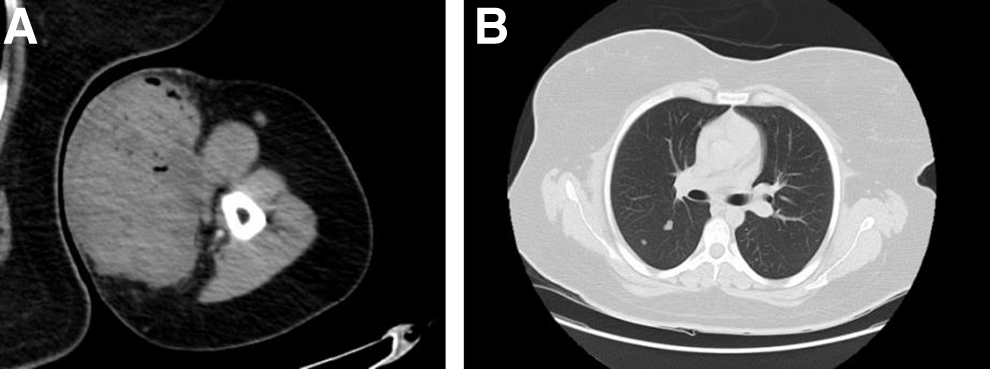
A 22-year-old previously healthy young woman presented with a left arm mass, which was initially 2–3 cm in diameter 5 months before presentation, but subsequently grew to 10.5 × 7.4 × 2.2 cm (Fig. 1A). She presented to an outside hospital after the lesion burst open and frank blood with associated yellow pus began to drain from it. She was admitted and started on intravenous antibiotics. She underwent a computed tomography (CT)-guided biopsy without sufficient tissue for diagnosis, and she was discharged on a course of oral antibiotics. She was seen by a sarcoma specialist who recommended admission for further imaging and open biopsy. A CT of her chest was performed, which demonstrated numerous lung nodules, suspicious for pulmonary metastasis (Fig. 1B). An open biopsy was then performed, which confirmed the diagnosis of high-grade undifferentiated small round cell sarcoma.
She underwent ovarian cryopreservation and began therapy as per the Children's Oncology Group (COG) protocol AEWS0031 with vincristine, doxorubicin, and cyclophosphamide alternating with ifosfamide and etoposide in an interval compressed manner, with radiation to her primary site as local control and whole lung radiation for her metastatic pulmonary disease. At the time of diagnosis, the patient was completing her final year of college with a double major and was living away from home. She graduated with honors with plans to pursue a master's degree. Before her time away in college, she lived at home with her parents and two younger siblings. She endorsed having a close relationship with both her immediate and extended families, which was evident by the constant rotation of extended family members while our patient was hospitalized. Her family history was notable for colon cancer in her paternal grandmother. She had a primary care provider (PCP) who she was able to identify. The patient shared that she did not plan to seek medical care but was forced to when her arm “burst open.” She was in remission at the end of therapy and remains free of disease 4 years later.
A 16-year-old previously healthy young man presented with a large fungating right upper arm mass. He was sent to an outside hospital after he visited his school health clinic. He noticed the mass several weeks prior but was hiding it from his mother. However, after he hit it against a wall, it began to bleed, and he therefore sought care. Magnetic resonance imaging of the lesion was notable for a 5 × 7 cm heterogeneous solid mass that was abutting and displacing the extensor tendons and muscles of the dorsum of the distal forearm but did not surround or invade them (Fig. 2). He was admitted to the hospital for an open biopsy, which revealed a spindle cell sarcoma. His CT chest and positron emission tomography scan did not demonstrate evidence of metastasis. He was treated as per the COG trial ARST0332, Arm D, with ifosfamide and doxorubicin and concurrent preoperative radiation followed by surgical resection.

MRI forearm notable for 5 × 7 cm heterogeneous solid mass, which abuts and displaces the extensor tendons and muscles of the dorsum of the distal forearm but does not invade them (arrow).
He completed neoadjuvant chemoradiation, underwent tumor resection with negative margins, and completed adjuvant chemotherapy. Our patient lives at home with his mother who is disabled. At the time of his initial diagnosis, he reconnected with his father, from whom he was previously estranged. He spent time at his father and stepmother's home while receiving treatment, as his mother was unable to adequately care for him. His family history was notable for renal cancer in his maternal uncle and prostate cancer in both his maternal and paternal grandfathers. He could not identify a PCP and sought care from his school health clinic. His social determinants of health screen were notable for two medium-risk categories in economic stability and social connections, and one high-risk category in transportation. He was in remission at the end of therapy.
Discussion
The gap in formal transition of care from pediatric to adult medicine often results in a delay in obtaining an adult primary care physician. While this is not ideal for a healthy adolescent, this is especially problematic when a health-related issue arises. Our 22-year-old young woman had not appreciated the extent of her tumor, and it was only when she returned home that her parents immediately encouraged her to seek medical attention. In contrast, our 16-year-old young man realized that there was a sizeable mass on his arm, but he did not want to burden his family and instead was determined to manage his symptoms alone.
Both our patients sought care through the emergency room despite having had symptoms for a prolonged period and no emergent event that precipitated an emergency room visit. AYA patients have an increased utilization of acute care visits compared with their adult counterparts. 11 Access to care is challenging for them, and AYA patients face the additional burden of navigating the financial aspects of health care. Furthermore, when teenagers go away to college, this is often their first time away from home and caring for themselves. Proactive education is needed, and perhaps, collaboration with high school and college health care clinics could benefit this population and make transition from pediatric to adult care more broadly a smooth process.
While there has been significant attention focused on reducing the interval between symptom onset and cancer diagnosis in adults, addressing this phenomenon, termed lag time, has not been as successful in the AYA population.10,12 There are many strategies to promote early detection of adult cancers such as breast, cervix, and colon. The same is not true for pediatric and AYA cancers, as we do not yet have standardized and validated processes for cancer screening other than for those patients with cancer predisposition syndromes. In addition, AYAs are typically at a health care transition when these tumors develop and navigating insurance and financial burdens has been hypothesized as a barrier in access to care. It has been demonstrated that the poorer prognosis seen in AYA patients with rhabdomyosarcoma compared with children is due not only to the disease biology but also to poorer access to care, differing treatment paradigms, and delayed clinical presentation.13–16 Integration of AYA patients into pediatric protocols has shifted the paradigm slightly in rhabdomyosarcoma, and formation of AYA-specific subcommittees has further improved overall outcomes. 17
While we have witnessed delayed presentation to care in our solid tumor oncology patients, the teenage years are a time when many complex diagnoses present such as eating disorders, diabetes, and other rheumatologic conditions. While most solid tumors are slow growing and allow for time to presentation, there is a window before further complications such as damage to adjacent organs, metastasis, and/or extrusion through the skin develop. Collaboration with our primary care colleagues on signs and symptoms of solid tumors is imperative to impart to patients and their families as our teenage patients transition to adult medicine.
Footnotes
Authors' Contributions
R.O.: Conceptualization and lead writing. S.N.: Writing—review and editing. D.M.L.: Review and editing. A.L.: Conceptualization.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.