
Abstract
Adolescent and young adult (AYA) cancer patients and survivors are a growing population due to more frequent diagnoses and improved survival. Fatigue is a common symptom experienced by cancer patients and it is often missed by health care professionals. Patient reported outcome measures (PROMs) can assist in evaluating patient reported fatigue. This systematic review aims to determine if AYA cancer patients report more fatigue than AYAs who have not been diagnosed with cancer. We used a subset of articles from a larger review that searched PubMed, EMBASE, CINAHL, and PsycINFO to determine which PROMs and domains are currently being used to evaluate AYA cancer. This study identified 175 articles related to PROMs in the AYA cancer population. Articles with PROMs reporting on fatigue/vitality were used in this review. From the original 175 articles, we identified 8 fatigue/vitality articles for this review. All eight articles found an increase in fatigue/decrease in vitality in the AYA cancer population compared to healthy controls. A meta-analysis was performed on four articles that used the same PROM tool (EORTC QLQ-C30). This found a statistically significant and clinically meaningful increase in mean fatigue of 12.5 95% confidence interval: 3.3–21.8 points (scale 0–100, higher number indicates more fatigue) in the AYA cancer group compared to healthy noncancer controls. Fatigue in the AYA cancer population is a significant issue, it is often undetected and underreported, and early interventions are needed to prevent the negative subsequent sequelae.
Introduction
The number of adolescent and young adults (AYAs) diagnosed with cancer has been steadily increasing over the last few decades.1–5 Mortality rates among this group are declining, leading to an increase in the number of AYA cancer patients and survivors.1,2,4–6 This population, defined as individuals diagnosed with cancer for the first time between the ages of 15–39 years, faces a unique set of challenges, both during and after cancer treatment.1,2 AYAs are already dealing with physical, emotional, cognitive, and social transitions during this age period.2,3,6 A cancer diagnosis during this phase of life can threaten the natural development of one's identity, autonomy, independence, education, career, relationships, and family.2–4 The AYA cancer group requires support both during treatment and into the survivorship period that differs from others diagnosed with cancer at different ages.1,6 There is a need to better understand the challenges faced by this population to offer appropriate support, at all stages of cancer diagnosis and treatment. 2
Patient reported outcome measures (PROMs) are tools that measure a patients' view of their health status.7,8 When used, these tools improve survival, symptom identification and management, and overall quality of life.8–12 Despite these benefits, PROM tools are not widely utilized in practice. 13 Health care providers tend to underestimate symptoms and the severity of these symptoms when PROM tools are not utilized. 14 Laugsand et al. found that fatigue had one of the highest rates of underestimation by health care providers compared to other symptoms like pain, vomiting, and diarrhea. 14 The utilization of PROM tools for the AYA cancer population can help bridge that gap to improve patient-centered care and the quality of care they receive.7,15
Given that fatigue, specifically among the AYA cancer population, is often underestimated by health care professionals, it is imperative to measure its effect to provide appropriate clinical care.2,4,14,16 Fatigue is one of the most distressing symptoms reported by cancer patients of all ages. 3 It can negatively affect psychosocial distress, symptom severity, functional status, and quality of life.3–5,16,17 Fatigue can also negatively impact a person's ability to exercise, increasing the risk of obesity, depression, and increased pain.2,17 Therefore, our systematic review aims to determine if AYA cancer patients and survivors report more fatigue than AYAs who have not been diagnosed with cancer.
Methods
Search strategies
This systematic review used a subset of the articles from a larger review which aimed to broadly identify all PROM tools used and clinical domains measured in the AYA cancer population. 18 Full details of that review, including the detailed search strategy, are available elsewhere. Briefly, the search strategy utilized four electronic databases (PubMed, EMBASE, CINAHL, PsycINFO) and examined articles published from January 1, 2011 to June 16, 2021. The search aimed to identify articles that included: (1) AYAs (15–39 years); (2) malignant neoplasms; and (3) PROMs. With the help of a professional librarian, MeSH terms and additional search strategies were utilized. After title, abstract, and full text screening, 175 articles were identified as relevant and included in that study. All assessments for inclusion and data extraction were performed by at least two independent researchers.
PROMs are tools that measure a patients' view of their health status.7,8 The PROM tools measuring fatigue in this review were composed of the European Organization for Research and Treatment of Cancer—Quality of Life Questionnaire (EORTC-QLQ-C30) and the Pediatric Quality of Life Inventory (PedsQL). The PROM tools measuring vitality or “zest for life” were the 36-Item Short Form Survey (SF-36), the 12-Item Short Form Survey (SF-12), and the Questions on Life Satisfaction (FLZM). All of these tools are self-reported questionnaires with small differences in domains/subsets of data collected.
The EORTC-QLQ-C30 is one of the most widely used tools in cancer research. 19 It consists of questions related to function, symptoms (i.e., fatigue), financial difficulties, and global health/quality of life. 19 The PedsQL is a questionnaire for both the patient, as well as their parent/career. It measures different domains, one of which is fatigue, to ultimately gain an understanding of the patients' overall health related quality of life. 20 The SF-36 measures various different subscales such as physical function, role, pain, general health, vitality, social function, and emotional well-being. 21 The SF-12 is a condensed version of the SF-36 designed to be a shorter self-reported questionnaire for the participant. 22 Finally, the FLZM assesses general and health related quality of life. One of the subsets of this questionnaire measures an individual's “energy or zest for life” which is consistent with the definition of vitality. 23 All of these are validated PROM tools recognized within the AYA cancer community. The decision about which tool to use may be impacted by the age of the patient or the specific domains of interest.
Study selection
Using the 175 studies included in the original search, we filtered articles containing PROMs measuring fatigue or vitality. Vitality was included as it measures an individual's energy and activity level, the opposite of fatigue. We felt this would add to the breadth of studies and allow us to use PROM tools that only measured vitality without measuring fatigue. Included articles were subject to a further full text review by a single researcher (C.F.). Studies were included if: (1) they focused on AYAs (defined as 2/3rd of study cohort aged 15–39 at diagnosis) or reported the AYA group separately; (2) patients had a malignant neoplasm; and (3) established PROMs were used to evaluate fatigue/vitality. Studies were excluded if: (1) there was no noncancer comparison group; (2) the study was not a cohort, cross-sectional, or case–control study design; and (3) the study used a custom PROM tool or qualitative interviews/focus groups for measuring fatigue/vitality. A reverse record check of all included studies was performed to ensure that there were no additional relevant studies potentially missed in the original search.
Data extraction and risk of bias assessment
Data extraction was performed in two phases. Basic publication data were used from the Engstrom et al. extraction. 18 This included: author, date, study design, and PROM tool used. Further data extraction was then performed to collect the fatigue/vitality specific data by a single reviewer (C.F.). This included: participant characteristics, time since cancer diagnosis, comparison group characteristics, and the primary outcome of interest, fatigue/vitality in AYAs with cancer compared to the noncancer controls.
The risk of bias was assessed independently by two different researchers (C.F. and S.T.) using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool. 24 Conflicts between researchers were resolved through discussion, and a consensus was reached. Each study was evaluated in seven different domains. These were: (1) bias due to confounding, (2) bias in selection of participants into the study, (3) bias in classification of interventions, (4) bias due to deviations from intended interventions, (5) bias due to missing data, (6) bias in measurement of outcomes, and (7) bias in selection of the reported results. The overall risk of bias was then based on the least favorable outcome of the seven different domains. The risk of bias in each domain was recorded as low, moderate, serious, or critical.
Data synthesis and analysis
The data from all included studies were first analyzed descriptively. Means, p-values, and standard deviations were included where appropriate.
A meta-analysis was then performed among studies that utilized the same fatigue PROM measure: the European Organization for Research and Treatment of Cancer—Quality of Life Questionnaire (EORTC-QLQ-30) PROM tool. Some studies were not included in the final meta-analysis given that some of the required information was not available in the published article and was not able to be obtained by contacting the corresponding author. The meta-analysis was carried out using the R statistical software specifically with the “R package meta” using a random effects model. 25
Results
We identified 76 articles which contained PROMs measuring fatigue or vitality in the AYA population (individuals diagnosed with cancer for the first time between the ages of 15–39 years 2 ). After applying the exclusion criteria, eight articles were included in the review (Fig. 1). A reverse record check of the included studies was performed, but no further articles matched the inclusion criteria. Characteristics of the included studies can be seen in Table 1, and the details of the studies are in Table 2.
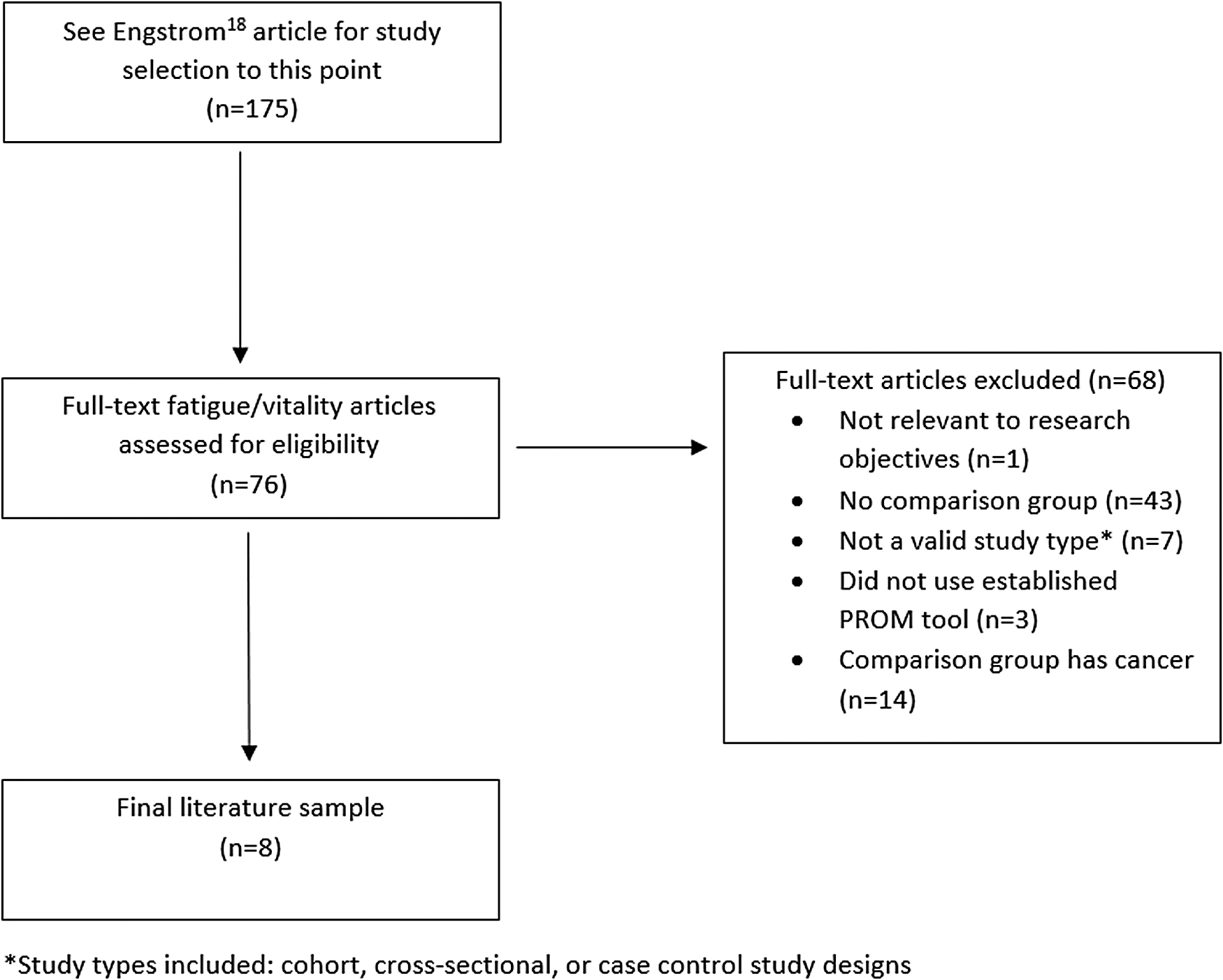
Study selection flow diagram.
Characteristics of Studies Included
PROM, patient reported outcome measure.
Details of Included Studies
Statistical significance of results.
AYA, adolescent and young adult.
The majority of the studies used a cross-sectional study design (n = 7, 87.5%), leaving just one cohort study (n = 1, 12.5%). The German population represented the largest proportion of studies (n = 3, 37.5%), followed by the Netherlands (n = 2, 25%), and then Austria, Denmark, and the United States equally (n = 1, 12.5%). A large proportion of studies had 100–500 participants (n = 3, 37.5%), followed by >500 participants (n = 2, 25.0%) and 50–100 participants (n = 2, 25.0%), leaving only 1 study with <50 participants (n = 1, 12.5%). Most of the studies focused on one specific type of cancer (n = 5, 62.5%), which included sarcomas, cervical cancer, malignant melanoma, and thyroid cancer. The remaining studies included participants with any type of cancer. Half of the studies used age- and gender-matched noncancer control groups (n = 4, 50.0%). Two studies used an age-matched noncancer control group (n = 2, 25.0%), one study used data from the German population and then performed multiple regression analysis to account for age differences (n = 1, 12.5%), and the remaining study used healthy medical students as their control (n = 1, 12.5%).
The majority of studies used the EORTC-QLQ-C30 PROM tool to measure fatigue (n = 5, 62.5%) with the remainder of the studies using the 36-Item Short Form Survey (SF-36) (n = 1, 12.5%) and the 12-Item Short Form Survey (SF-12) and the Pediatric Quality of Life Inventory (PedsQL) (n = 1, 12.5%) and the Questions on Life Satisfaction (FLZM) (n = 1, 12.5%). The risk of bias was assessed to be low in 1 (12.5%) of the studies and moderate in 7 (87.5%) of the studies. Most of these studies were given a moderate rating due to the bias in selection of participants into the study. See Table 3 for risk of bias details.
Risk of Bias
Bold text represents low risk of bias; Italics text represents moderate risk of bias; Bold and italics text represents no information.
Studies reporting fatigue
Six of the eight studies reported on fatigue (n = 6, 75.0%) (Table 2). Five of these used the European Organization for Research and Treatment of Cancer—Quality of Life Questionnaire (EORTC-QLQ-30) (n = 5, 62.5%), and one study used the Pediatric Quality of Life Inventory (PedsQL) (n = 1, 12.5%). Five of these were cross-sectional (n = 5, 62.5%), and one study had a cohort design (n = 1, 12.5%). Three of these studies used an age- and sex-matched comparison group (n = 3, 37.5%), two studies used age-matched (or similar age) comparison groups (n = 2, 25.0%), and one study used multiple regression analysis to account for the different age demographics in their control group (n = 1, 12.5%). The PROM tools were completed as a self-reported questionnaire. Five of these studies showed a statistically significant result of increased fatigue in the AYA cancer population compared to a noncancer control group (n = 5, 62.5%). These studies showed consistent results of increased fatigue in the AYA cancer population even when accounting for a variation in time since diagnosis, type of cancer, treatment received, and geographic location.
Studies reporting vitality
Three of the studies measured vitality or “zest for life” using established PROM tools (Table 2) (n = 3, 37.5%). One study used the Short Form Survey 36 (SF-36) (n = 1, 12.5%), another study used the Short Form Survey 12 (SF-12) (n = 1, 12.5%), and the remaining study used the Questions on Life Satisfaction (FLZM) (n = 1, 12.5%). All three of these studies had a cross-sectional design (n = 3, 37.5%). One study used an age- and sex-matched comparison group (n = 1, 12.5%), another study used age-matched population norms (n = 1, 12.5%), and the remaining study used healthy medical students who were not age or sex matched (n = 1, 12.5%). The PROM tools were completed as a self-reported questionnaire. Two of these studies showed a statistically significant result of lower levels of vitality or “zest for life” in the AYA cancer population compared to a healthy noncancer control group even with variations in time since diagnosis, type of cancer, treatment received, and geographic location (n = 2, 25.0%).
Meta-analysis
The meta-analysis of studies by Beutel, 26 Drabbe, 27 Geue, 28 and Mols 29 was performed using the “R package meta” 25 with a random effects model. These four studies all measured fatigue using the EORTC-QLQ-30 PROM tool. Studies have shown that an increase of >10 points for fatigue (scale of 0–100, higher scores equal more fatigue) on the EORTC-QLQ-30 is clinically meaningful. 30 The meta-analysis consisted of 1072 cancer patients and 2988 noncancer controls. The difference in mean fatigue score between the cancer population and noncancer controls was 12.5 (95% confidence interval: [3.3–21.8]), with the cancer population reporting statistically significant higher levels of fatigue (p-value <0.0077) compared to the noncancer control group. The forest plot of the meta-analysis can be found in Figure 2.

Meta-analysis forest plot.
Discussion
In this review, eight studies were included to describe a relationship between a diagnosis of cancer in the AYA population (15–39 years) and self-reported fatigue/vitality. This self-report was carried out using established PROM tool questionnaires. Our descriptive data analysis showed that AYAs diagnosed with cancer do experience more fatigue and have less vitality (“zest for life”) than their healthy counterparts. Our meta-analysis showed that the AYA cancer population had a statistically significant and more importantly a clinically meaningful increase in fatigue compared to noncancer controls.
Given that fatigue is associated with the AYA population in general, 31 it can be overlooked by the clinical teams managing AYA cancer patients. 14 With the studies included in this review, and included in the meta-analysis, there is a clear clinically meaningful increase in fatigue that should be actively managed.
The relationship between being diagnosed with cancer as an AYA and increased fatigue was consistent across all studies regardless of the PROM tool, study design, country, diagnosis, or treatment.
Adolescents with cancer are particularly vulnerable to cancer related fatigue. 32 This fatigue is more consistent throughout the cancer trajectory rather than just after treatments, such as chemotherapy. 32 Unfortunately, there is a paucity of studies focusing on cancer related fatigue in adolescent specific populations. 32 Therefore, it is important to also draw on adult and pediatric research. Cancer related fatigue in the adult population has been linked to functional impairment, a lower quality of life, and more distress. 3 It has been shown to have a negative impact on work, relationships, and mood. 33 Early identification and accurate assessment of fatigue in the AYA cancer population is needed to help prevent this sequela. Interestingly, in the adult cancer population, fatigue is not directly related to a certain cancer treatment; patients who received the same treatments may experience different levels of fatigue at different times throughout their treatment and post-treatment period. 33 In children, fatigue is associated with factors like anemia in early stage cancer and symptom distress with late stage cancer. 34
Fatigue is amenable to intervention, which may prevent these negative outcomes. A variety of different interventions have been shown to decrease fatigue in the adult cancer population. 33 Some of which include physical activity, cognitive behavioral therapy, mindfulness, yoga, and acupuncture. 33 Interventions targeted to adolescents must find a way to engage AYAs and persist with physical activity despite their fatigue. 35 Engaging family and careers may help AYAs engage and commit to interventions. 35 The use of PROM tools in the AYA cancer population can help to better recognize fatigue and, therefore, may improve the care AYA cancer patients are receiving, both during and after treatment.7,8,15
Several limitations of this review need to be considered when interpreting the results. Only studies coded as focusing on PROMs in the database search were included. This may have excluded studies that used different coding or terminology. Another limitation was that only articles written in English were included, potentially excluding valuable articles written in different languages. The focus of this review was to determine if AYAs with cancer experience more fatigue than their healthy counterparts. Our inclusion criteria required a two-thirds majority of study participants to be in the AYA age range, so the included studies may have some non-AYA participants which could impact the findings. One study included participants aged from 30 to 70+; three studies do not specify the age range of the participants but do state their mean age and SD, permitting an assessment of two-thirds of subjects that are in the AYA age range.
Most of the included studies had a cross-sectional study design, limiting the ability to evaluate fatigue over time. Although all studies had similar results, the meta-analysis only included four of the eight studies which may have influenced the magnitude of this relationship. The risk of bias was determined to be of moderate risk for seven of the eight included studies. This needs to be taken into consideration when looking at these results. More research is required to determine if fatigue is influenced by the type of cancer, treatment type and duration, sex, and the length of time this fatigue is experienced, both during and after treatment.
In summary, our review and meta-analysis show that AYAs diagnosed with cancer experience more fatigue than noncancer controls. Moving forward, the routine use of PROM tools is necessary for health professionals to accurately assess fatigue among AYA cancer patients.9,10,14 Given that fatigue has many negative long-term effects, assessment and appropriate clinical management are required.2–5,16 Appropriate interventions, tailored to the AYA population, are required to prevent those adverse effects.1,6
Footnotes
Authors' Contributions
J.D.P. conceived the work; J.D.P., T.E., and C.F. designed the work, including search strategy, inclusion and exclusion criteria; C.F. reviewed the articles; C.F. and S.T. completed risk of bias; C.F. drafted the article; C.F., J.D.P., T.E., R.W., and N.B. interpreted the results. All authors revised, edited, and approved the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.