
Abstract
Purpose:
Social anxiety disorder (SAD) remains an understudied potential link between the cancer experience and adolescent and young adult (AYA) cancer survivors' poor psychosocial outcomes. We investigated the frequency and duration of, as well as factors associated with, symptoms of SAD among AYAs with cancer.
Methods:
This longitudinal, mixed-methods study involved online surveys (including a validated screening tool for SAD) at recruitment and 6 months later, and a structured clinical interview.
Results:
Twenty-eight AYAs (aged 12–30 years, <1-year postdiagnosis, 50% male) completed the first survey (M = 6 months postdiagnosis). About 32% reported clinically significant SAD symptoms. Fourteen completed the follow-up survey (M = 12 months postdiagnosis), of which 9 (62%) reported persistent or worse symptoms of SAD significantly associated with emotional distress, physical appearance concerns, negative social cognitions, and depression.
Conclusion:
A subset of AYAs with cancer may experience clinically significant SAD symptoms that can affect their psychosocial well-being. Further work on how to best identify and support AYAs with SAD is needed.
Introduction
In Australia, >1200
Despite numerous studies highlighting the experience of social anxiety symptoms among AYAs living with chronic illness, including cancer,7–10 clinically significant symptoms of social anxiety disorder (SAD) remain an understudied potential link between the AYA cancer experience and poor social outcomes. SAD is defined by the Diagnostic and Statistical Manual, Version 5 (DSM-5) 11 as an anxiety disorder not attributable to physical health conditions, with anxiety persisting for 6 months or more that is (1) present in almost every social situation, (2) greater than warranted by the social situation, (3) resulting in avoidance of social situations or endurance of them with distress, and (4) negatively affecting young people's social functioning.11,12 Risk factors for developing SAD include common impacts of youth cancer treatment: poor physical health or negative perceived physical appearance, social isolation, and traumatic events that have social impact (i.e., bullying, peer victimization).3,13
The Clark and Wells cognitive model of social phobia (SAD) is the prevailing model for understanding SAD and proposes that SAD is developed and maintained through negative beliefs people hold about themselves in relation to their social worlds, as well as negative social cognitions (thought processes they have about how they appear to others before and after social interactions).14,15 In the general population, SAD often precedes the development of comorbid disorders, including depression.16–18
To address these gaps, we conducted a prospective, longitudinal, mixed-methods study that aimed to:
Investigate the frequency and duration of SAD symptoms among AYAs recently diagnosed with cancer. Explore whether AYAs qualitatively describe aspects of the cancer experience (experience of social isolation, hair loss, etc.) as associated with SAD symptoms. Determine clinical, demographic, and psychosocial factors that are quantitatively associated with symptoms of SAD.
For the purposes of this research, we define
Methods
Study design and recruitment
We used a longitudinal, convergent mixed-methods design. 19 Quantitative data collection was performed before qualitative data collection and integration of findings was during data analysis. 20 The study was approved by the Human Research Ethics committee (2019/ETH13377).
Eligible AYAs were within 1 year of their diagnosis, aged 12–30 years at diagnosis, and recruited via social media (from anywhere in the world) or one of five cancer centers in New South Wales, Australia. Considering this study was conducted in Australia, but recruited participants internationally, we reviewed evidence on the age of onset of SAD as well as international differences in the age ranges used for AYA cancer, to determine the optimal age range for participants in this study. Existing evidence consistently indicated that SAD most commonly occurs in the general population between the ages of 10 and 20 years, spanning the developmental periods of late childhood and early adulthood. 13
However, the broadest age range used to define AYA cancer spans the ages of 13–39 years. 21 A minimum age of 12 years would therefore facilitate capture of early adolescence, whereas a maximum age of 30 years is what aligns with recommendations that reviewed international age ranges for AYA cancer previously published by the Journal of Adolescent and Young Adult Oncology in 2011. 21
Potential participants who, in the clinical opinion of their treating team would be unsuitable for the study (e.g., their family were experiencing other serious individual or psychosocial complexities) were not approached. All participants received reimbursement for participation ($10 electronic gift card following each survey and interview, with a bonus $5 electronic gift card for completing all parts of the study).
Owing to COVID-19 pandemic restrictions in Australia persisting through the duration of this study, we were unable to conduct in-person recruitment. Instead, site investigators, who were clinicians at participating sites, conducted recruitment in person and via text messages or emails to eligible AYAs. A study flyer, including QR code links to the survey, was also displayed at all participating centers and shared on Twitter. We invited all participants to complete an electronic consent form and baseline survey at the time of recruitment, followed by an optional structured clinical interview assessing their present and past mental health. Six months later, participants were invited to complete an identical follow-up survey.
Participants who were recruited via social media were verified to be eligible participants and from their specific countries via IP address verification (IP addresses are collected automatically by Qualtrics survey software) and email confirmation through which C.E.S. emailed the participant to confirm their details (date of birth, date of diagnosis and diagnosis type entered into the survey). Participants who did not respond and correctly verify their details were not included.
Measures
Analysis
All quantitative data analyses were conducted in IBM SPSS software. 31
Aim 1: Investigate the frequency and duration of SAD symptoms among AYAs recently diagnosed with cancer
We calculated total scores on the SPIN and compared them with the published clinical cutoffs for SAD. We calculated the percentage of AYAs whose scores on the SPIN remained the same, decreased, and increased from time 1 (T1) to time 2 (T2). We used structured clinical interviews (SCID and KSADS-PL) to describe SAD symptoms experienced by AYAs. We recorded the interviews using Microsoft Teams, transcribed them verbatim, and C.E.S. conducted qualitative, deductive content analysis in NVivo.32,33 Categories for content were derived from the SCID social anxiety section, with primary nodes based on the key DSM-5 diagnostic criteria for SAD, and secondary nodes based on the extent to which symptoms have bothered/caused problems for the participant. S.N. then double coded three of the interviews (20%) for reliability purposes. Review of coding yielded a high level of agreement (k = 0.95).
Aim 2: Explore whether aspects of the cancer experience are qualitatively associated with SAD symptoms
In addition to the qualitative coding of structure clinical interviews (SCID and KSADS-PL) described for Aim 1, we also coded interviews as yes or no to whether SAD symptoms were primarily owing to another physical medical condition (such as cancer, and therefore according to DSM-5 criteria, meant AYAs did not meet diagnostic criteria for SAD).
Aim 3: Determine the clinical, demographic and psychosocial factors quantitatively associated with SAD symptoms
We conducted univariate linear regression analyses between participants' SPIN scores and their clinical, demographic, and psychosocial characteristics.
Results
Participant characteristics
A total of 81 AYAs were invited to the study between June 2020 and March 2022, of which 28 (35%) participated in the first survey. We did not collect information from participants who did not opt into the study on why they chose not to participate. Most participants (24) were recruited from Australian cancer centers, and four from international locations via social media (United States = 2, Singapore = 1, Finland = 1). Participants were an average of 19 years old, 50% male, and 6 months postdiagnosis at the time of the first survey (T1) (Table 1). Fifteen AYAs (54%) also participated in a structured clinical interview and 14 (46%) in the second survey.
Participant Demographics and Outcomes
Other cancers include bone sarcoma, neuroblastoma, squamous cell carcinoma of the lung, giant cell tumor, juvenile nasopharynx angiofibroma, and breast cancer.
AYA-POST, Adolescent and Young Adult Psycho-Oncology Screening Tool; PHQ-9, Patient Health Questionnaire-9.
Aim 1: Investigate the frequency and duration of SAD symptoms among AYAs recently diagnosed with cancer
At 6 months postdiagnosis, nine (32.10%, of N = 28) AYAs scored above the clinical cutoff for SAD, on the SPIN, indicating clinically significant symptoms of SAD. At 12 months postdiagnosis, eight AYAs scored above the clinical cutoff for SAD on the SPIN, which was a relatively higher proportion of our smaller sample at that time (57.10% of N = 14). More than half of AYAs (62%) reported higher SPIN scores between an average of 6 and 12 months postdiagnosis, indicating increased severity of SAD symptoms over time. For 12 (86%) participants reporting subclinical or clinical SAD symptoms at T1, those symptoms persisted or progressed in severity by T2 (Fig. 1).
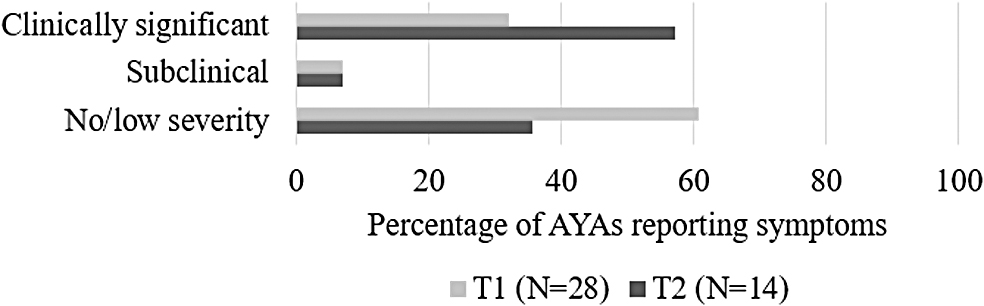
Frequency and duration of social anxiety disorder symptoms.
Of note, there was poor agreement between meeting diagnostic criteria for current SAD on the self-report SPIN compared with the structured clinical interview (k = 0.25). Of the 15 AYAs who participated in the interviews, 5 scored above the clinical cutoff for current SAD on the SPIN but only one met diagnostic criteria for current SAD on the structured clinical interview.
Aim 2: Explore whether aspects of the cancer experience may be qualitatively associated with development or progression of SAD symptoms
The criteria on the structured clinical interview that were
DSM-5 Social Anxiety Disorder Diagnostic Criteria on the Structured Clinical Interview
Aim 3: Determine the clinical, demographic, and psychosocial factors that are associated with increased severity of SAD symptoms
At 6 months postdiagnosis, increased SPIN scores (more severe SAD symptoms) were significantly associated with depression (PHQ-9), negative social cognitions (SBSA), and emotional needs (AYA-POST), general physical appearance concerns, pain, sexual functioning concerns, and nausea (Table 3).
Univariate Regressions with SPIN Scores and Demographic, Clinical, and Psychosocial Factors at T1
p<0.05; **p<0.005.
CI, confidence interval; CNS, central nervous system; PALS, Perth A-loneness Scale; RYSC-NE, Report of Youth Social Cognitions—Negative Evaluation subscale; RYSC-PI, Report of Youth Social Cognitions–Positive Impression subscale; RYSC-RS, Report of Youth Social Cognitions–Revealing Self subscale; SBSA, Self-Beliefs related to Social Anxiety scale; SPIN, Social Phobia Inventory.
Discussion
This study is the first to longitudinally assess the frequency and duration of SAD symptoms using validated measures and gold standard structured clinical interviews in a cohort of AYAs recently diagnosed with cancer. We found 32% of AYAs endorsed clinically significant symptoms of SAD, an average of 6 months postdiagnosis. This proportion was consistent with the proportion previously found in a sample of Australian AYA survivors (33%: N = 27, average of 7 years post-treatment). 34 This is more than double the prevalence of SAD (5%–13%) reported for the general AYA population.13,35,36 We also found for most (62%) of our sample of AYAs, subclinical and clinical symptoms persisted or worsened over time, consistent with evidence from the general AYA population if SAD is left untreated. 35
In structured clinical interviews, AYAs qualitatively highlighted cancer-specific factors, such as changed physical appearance and fear of disclosure of cancer history, that contributed to their social anxiety symptoms. We found that fewer AYAs in our sample met diagnostic criteria for SAD on the structured clinical interview than on the SPIN because (i) symptoms did not last long enough (<6 months) or (ii) symptoms were directly attributable to the impact of their cancer treatment. This highlights a potential limitation of the DSM-5 in that persistent medical illness, such as cancer, may invalidate an SAD diagnosis but at the same time facilitate maladaptive self-beliefs, social cognitions, and avoidant behaviors that are essentially identical to SAD.
SAD symptoms were significantly associated with emotional distress, physical appearance concerns, and depression symptoms. These findings align with the Clark and Wells' cognitive model of social phobia, and suggest that negative self-perceptions, such as negative perceived physical appearance, together with negative social cognitions (e.g., worries that others will judge them negatively because of their appearance) may lead to the development and maintenance of SAD for AYAs. 14
SAD symptoms were not significantly associated with social needs, which may indicate that AYAs continue to participate in social activities, enduring them with distress rather than avoiding them altogether. For example, one young woman undergoing treatment for Hodgkin lymphoma mentioned: “For work I think it [social anxiety] does [affect work], yeah, just because nursing is constantly meeting people. It's definitely something I have to push through in my work on a daily basis.” Previous qualitative research similarly suggests AYAs persist in trying to develop and maintain social relationships despite feelings of being different, embarrassed, excluded, or alienated.37–39
Limitations
The generalizability of these findings is limited by small sample size, primarily because of the entirety of this study being conducted during Australia's COVID-19 pandemic, during which restrictions prevented researchers from entering hospital clinics and wards, so all recruitment and study participation needed to occur virtually. However, our low opt-in and retention rates (35% and 50%) were consistent with international psycho-oncology studies documenting difficulties in recruiting and maintaining involvement of AYA cancer survivors in research.40,41 An added limitation of our sample was that most participants were from New South Wales, Australia, attending large cancer centers where specialized AYA cancer services were available. We did not assess existing support service use, or current/previous treatment of SAD symptoms, which may affect responses.
Finally, the number of variables analyzed through the univariate linear regressions increases the likelihood of type 1 error and underscores the importance of cautiously interpreting the results from this study. Without a more robust sample size and multivariate analyses, it is not possible to draw conclusions about which factors may independently predict severity of SAD symptoms versus those that may act in combination to predict symptoms.
Clinical implications
Our findings suggest that AYAs recently diagnosed with cancer may experience distressing social anxiety symptoms warranting assessment and intervention, although they may not meet diagnostic criteria for SAD owing to the symptoms being related to their cancer experience. AYAs with cancer experiencing social anxiety but not meeting diagnostic criteria for SAD would benefit from exercises to correct negative thoughts and images, especially around how their physical appearance or cancer history are perceived by others. These AYAs are likely to continue participating in social situations despite the distress they experience; therefore, assessment and treatment approaches should be cognizant that appearance of normal social function does not necessarily indicate normal social function.
Referral to a mental health professional, such as a social worker or clinical psychologist, who can provide evidence-based treatments for social anxiety, particularly in the context of their cancer diagnosis, may be worthwhile if the symptoms of social anxiety are causing impairments to day-to-day functioning and quality of life. In addition, further research and clinical consensus is needed to determine whether different diagnostic criteria may be needed for AYAs with cancer or other chronic illnesses who experience many clinically significant symptoms of SAD, but do not meet current DSM criteria because SAD symptoms are related to their illness.
Furthermore, SAD is not currently part of any recommended psychosocial screening conducted for AYAs with cancer in Australia, or internationally. Findings from this study suggest that it would be beneficial to screen these AYAs for SAD at diagnosis and that SAD symptoms may be transient in nature, so additional screening across the treatment and survivorship trajectory is needed. Validation of screening tools for SAD for use among AYAs with cancer as well is necessary.
Conclusions
These findings provide preliminary evidence that clinically significant symptoms of SAD are prevalent in a subset of AYAs recently diagnosed with cancer. Many AYAs experience increasing severity of SAD symptoms in the first months following their diagnosis, which can contribute to limited participation in or increased avoidance of age-appropriate social activities. Further research is needed to identify how and when to optimally assess and address SAD symptoms, to protect and promote AYAs' social well-being.
Footnotes
Acknowledgment
This work was included in the dissertation of C.E.S., submitted to the University of New South Wales, in fulfillment of the degree of Doctor of Philosophy, awarded February 23, 2023.
Authors' Contributions
All authors: Conceptualization, methodology, and writing—editing and review of writing. C.E.S.: Project administration, investigation, data curation, and writing—original draft. S.N.: Validation. A.A., T.L., C.O.D., F.M., and R.B.: Resources. U.M.S.-D., J.E.F., A.C.A., and T.N.T.: Supervision.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
C.E.S. was supported by a Research Training Program Scholarship from the Australian Government, a PhD Top-Up Scholarship from the Kids Cancer Alliance, and a PhD Top-Up Scholarship from Child Unlimited, part of Maridulu Budyari Gumal (SPHERE). U.M.S.-D. is supported by an Early Career Fellowship from the Cancer Institute of New South Wales (ID: 2020/ECF1163) and an Early Career Fellowship from the National Health and Medical Research Council of Australia (APP1111800). J.E.F. is a Maridulu Budyari Gumal (SPHERE) Cancer CAG Senior Research Fellow and is supported by a Cancer Institute NSW Research Capacity Building Grant (2021/CBG003).