
Abstract
Advances in medical technology are expected to increase the possibilities for pregnancy for women during and after cancer treatment. We aimed to clarify the psychological dimensions of cancer diagnosis for patients hoping for a pregnancy (their own or their spouse/partner’s) during or post-treatment and identify ways to improve support for these survivors and their families. A systematic literature review was conducted in May 2023 using six electronic databases: PubMed, Web of Science, Cochrane Library, PsycINFO, Ichushi-Web, and CINAHL. The search targeted English and Japanese studies with English abstracts published between January 1, 2001, and May 10, 2023. Search terms related to cancer, pregnancy, and psychological aspects were included. The initial search identified 1328 potentially relevant studies after removing duplicates. Subsequently, two reviewers screened article titles and abstracts to exclude studies with no data, those unrelated to pregnancy, and so on, and identified 44 potentially relevant studies. Two reviewers then reviewed the full text of each study, and 20 articles finally met the inclusion criteria. Several studies indicated that trying to conceive negatively impacts survivors’ finances, their relationships with their spouses/partners, and their mental health. Although many participants required fertility counseling, few received such opportunities. When cancer survivors try to conceive, they experience physical, psychological, and social burdens; moreover, many report a lack of access to fertility counseling or sufficient information about reproductive health care. Health care professionals should provide patients with updated and more accurate information on reproductive medicine and fertility counseling to enhance pregnancy support during the survivorship phase.
Background
Recent advances in cancer treatment and reproductive technologies have contributed to increased opportunities for pregnancy in survivors. This technological advance is especially important for Adolescent and Young Adult (AYA) patients with cancer who are trying to plan a pregnancy. Cancer survivors with reproductive concerns who have not fulfilled their pre-treatment desire to become parents have elevated risks for depression and poor mental health.1,2 Moreover, cancer survivors who are unable to conceive after treatment have been shown to have diminished physical well-being and lower quality of life than survivors who have children after cancer treatment.3,4
The Pregnancy Outcome and Safety of Interrupting Therapy for Women with Endocrine Responsive Breast Cancer (POSITIVE) trial with women desiring pregnancy during breast cancer treatment was conducted on four continents as an international collaboration. 5 Of the 497 women, 368 (74.0%) had at least one pregnancy and 317 (63.8%) had at least one live birth. Although the observation period was too short, the 3-year incidence of breast cancer events was similar in the treatment interruption and control cohorts. 6 Based on the POSITIVE trial results, increasing numbers of patients are expected to seek pregnancy after treatment or a pause in treatment. Therefore, understanding survivors’ experiences concerning conception is essential to improving service provision and accurately tailoring services to meet their psychosocial support needs.
Several systematic reviews have reported on fertility in cancer patients. For example, a systematic review of fertility and psychological distress among cancer survivors aged under 45, 7 a systematic review focused on fertility preservation counseling for women with cancer, 8 and a systematic review focused on fertility in young female patients with cancer 9 have shown beneficial findings. All these reviews focused on psychological distress and quality of life for those with fertility issues. Unlike these previous studies, this review focused on cancer survivors who tried to conceive during or after treatment.
This systematic review focused on studies examining the psychological state of survivors during or after cancer treatment as they attempt to conceive: the emotions experienced by male and female survivors as they contemplate and plan for pregnancy, their desire to have children, their concerns about infertility, and their mental health. We also searched for studies examining the needs for support and consultation or fertility counseling. The purpose of this review was to provide opportunities to learn about the psychological states of cancer survivors trying to conceive during and after treatment and to explore options for better treatment and care. The findings may be most useful for AYAs who are planning to become pregnant in the future.
Methods
Inclusion criteria and search strategy
A mixed-methods systematic review was conducted in accordance with the Preferred Items for Systematic Reviews and Meta-Analyses guidelines. The protocol for this review is registered in the International Prospective Register of Systematic Reviews (ID: CRD42022372946). This secondary data analysis was based on published aggregate data and did not require informed consent for participation and ethical approval.
In this systematic review, we considered studies reporting the psychosocial aspects related to when a survivor becomes pregnant during or after cancer treatment, or when there is some action (e.g., receiving a fertility consultation) that leads to pregnancy. Studies exploring only fertility preservation for future pregnancies were excluded, while those wherein the survivors experienced pregnancy/some action leading to pregnancy, with or without fertility preservation, were included. To accurately capture the broad range of experiences of cancer survivors, no restrictions were placed on gender, cancer diagnosis, fertility preservation, or length of time since diagnosis. We searched the literature using six electronic databases: PubMed, Web of Science, Cochrane Library, PsycINFO, Ichushi-Web, and CINAHL. The search targeted English and Japanese studies with English abstracts published between January 1, 2001, and May 10, 2023. Search terms related to cancer, pregnancy, and psychological aspects were included (Table 1). The initial search identified 1328 potentially relevant studies after duplicates were excluded. Two reviewers screened the articles’ titles and abstracts; after excluding 436 with no data, 283 with only treatment outcomes, 246 unrelated to pregnancy, 112 not during or after treatment, 116 unrelated to cancer, 76 that did not include patients, 15 without human participants, and 44 potentially relevant studies were identified.
Summary of Search Terms Used Across All Electronic Databases
The full text of each study was then reviewed by two reviewers, and disagreements were resolved through discussion and third-party input. A final total of 20 articles met the eligibility criteria (Fig. 1).
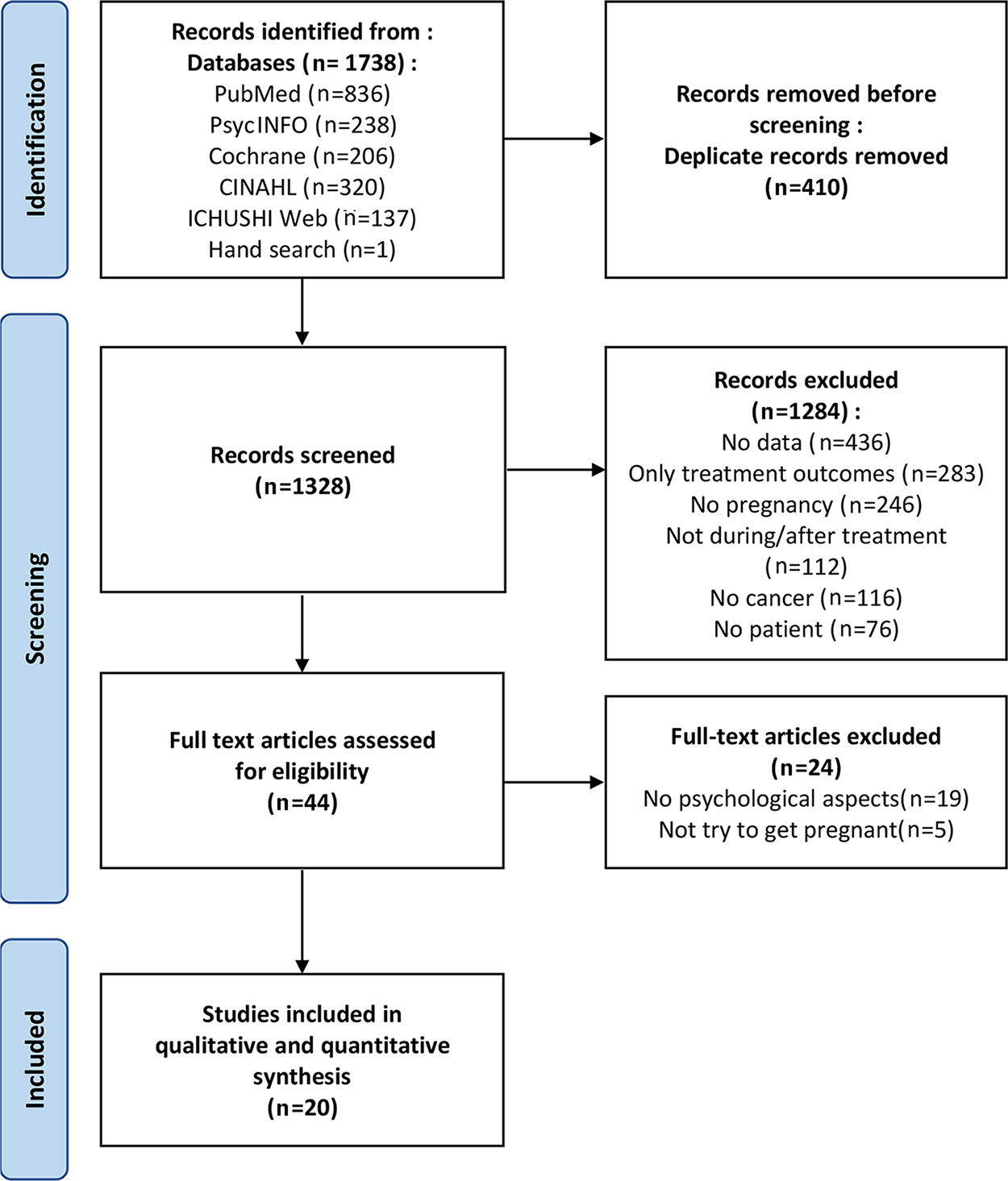
PRISMA Flow Chart of the systematic review selection process.
Quality analysis and extraction
The Mixed-Methods Appraisal Tool (MMAT) was used to assess study quality.10,11 The MMAT assesses the quality of qualitative or quantitative studies for each of the following areas: sampling, measurement, data completeness, and bias. Two reviewers analyzed the reported data and assessed the research quality, which was considered sound for the majority of the included studies (6 studies’ quality scores = 100%,12–17 11 = 80%,1,4,18–26 2 = 60%,27,28 1 = 40% 29 ). Data on patient characteristics (age of sample, sample size, gender, cancer diagnosis) and descriptions, as well as details of psychosocial aspects, were extracted from each article.
Methods and means of data analysis
Psychosocial aspects were analyzed under six themes: “emotions concerning pregnancy during and after treatment,” “desire for children,” “fertility concerns,” “mental health,” “fertility consultation or counseling,” and “support needs.” Four articles concerned “emotions concerning pregnancy during and after treatment,” seven articles “desire for children,” five articles “fertility concerns,” five articles “mental health,” nine articles “fertility consultation or counseling,” and four articles “support needs.” The systematic review was conducted to qualitatively analyze the evidence obtained from each article for each theme.
Results
Study characteristics
A total of 20 articles were reviewed, of which 16 were quantitative1,4,12,13,15,16,19–24,26–29 (including two quantitative non-randomized studies13,15) and 4 were qualitative.14,17,18,25 All 20 were retrospective studies. The studies were published over 16 years, from 2007 to 2023, and originated from nine countries (United States: 9; Germany: 2; Sweden: 2; Netherlands: 2; Japan, Taiwan, Turkey, France, and United Kingdom: 1 each). There was a large variation in sample size (minimum 10 to maximum 1106 participants), which was attributed to the study design.
The majority of articles reported on female survivors exclusively; five included a combination of men and women, and two included only male survivors. Ten studies focused on one cancer diagnosis/patient type each: studies exclusive to female survivors of childhood cancer (n = 3), patients with breast cancer only (n = 3), patients with testicular cancer only (n = 2), patients with blood cancer only (n = 1), and patients with cervical cancer only (n = 1). The remaining 10 studies included a variety of cancer diagnoses.
The quality of the 20 articles evaluated by the MMAT was as follows: 17 articles were of high quality, scoring above 80% of the MMAT’s research quality assessment criteria. There were 14 quantitative descriptive studies: of which one met 40%, two at 60%, nine at 80%, and two at 100% of the MMAT’s research quality assessment criteria. Eleven articles were assigned a “no” for the item “low risk of non-response bias,” three articles were assigned a “no” for “adequate measurement,” and two articles were assigned a “no” for “sample representative of the target population.” There were two quantitative non-randomized studies that were at 100% of the MMAT’s research quality assessment criteria. There were four qualitative studies, of which two met 80% and two met 100% of the MMAT’s research quality assessment criteria.
Emotions concerning pregnancy during and after treatment
Four studies reported on the emotions cancer survivors experienced about pregnancy during or after treatment.14,17,18,25
Four major themes were identified among male and female cancer survivors (n = 46) pursuing family-building after cancer treatment: emotional experiences of family-building after treatment, financial aspects of family-building after treatment, impact on partners, and connections/impacts on life trajectories. 18 The underlying factors in all four themes were negative emotions about infertility, family-building, and financial issues, which were perceived more strongly than positive emotions. Survivors were also concerned about the impacts of fertility and financial problems on their partners. In addition, the relationship between parenthood and broader life plans required accepting delays in the planned timing of parenthood. 18
Fifty percent (n = 9) of the breast cancer survivors were concerned that cancer-positive genes would be passed on to their children and that cancer-related treatments would affect their children’s health; 50% (n = 8) believed that pregnancy would cause physical damage such as cancer recurrence; and 31.1% (n = 5) claimed that having children was the best time of their lives and that raising children gave the family hope and happiness. Cancer and its treatment interrupt women’s pre-cancer lives. They indicated that having children after the end of cancer treatment brings new meaning to their lives and helps them achieve a balanced life. 25
The four main categories of cancer survivor (n = 10) experiences during the perinatal period were: the possibility of infertility but hope for the measures to take fertility preservation; worry and conditional joy because of the possibility of cancer recurrence and concerns about child health during pregnancy and postpartum; complaints about the lack of information about fertility treatments during and after cancer treatment and actions to ensure the best possible health care team throughout pregnancy; and allowing pregnancy to define the borderline between cancer and motherhood. Post-cancer, perinatal women reported dual emotions such as “I’m so happy, but also terrified,” uniquely influenced by their cancer history. 14
These results indicate that both men and women have negative feelings about infertility, family-building, and financial issues, and that women have complex emotions, such as wanting to have children but worrying about recurrence and their children’s health.
Desire for children
Seven studies reported the desire of cancer survivors to have children.1,4,12,15,21,22,29 In these studies, 72% (n = 172) of female cancer survivors, 29 86% (n = 953) of female childhood cancer survivors, 15 and 48.2% (n = 121) of testicular cancer survivors 21 reported wanting children. Four of these studies reported pre- and post-treatment changes in the cancer survivors’ desire to have children.1,4,12,22
Of those who had a desire for children before treatment (71 men and 81 women), those who had a desire for children 3–7 years later had fewer children in younger age groups, while those who no longer had a desire for children had children at diagnosis in older age groups. 1 Of those who did not want children before treatment (83 men and 246 women), those who did not want children 3–7 years later were older women and those who already had children at the time of diagnosis; those who wanted children were younger than the others, and a lower percentage had children at diagnosis. 1
In terms of pre- and post-testicular cancer diagnosis and treatment, the majority (n = 166, 87.4%) had no change in their desire to become parents. 22 The pre-diagnosis desire to have children did not change during or after experiencing cancer for the majority of female survivors (n = 163, 68%) in these seven studies, whereas that desire grew stronger for 15% (n = 36) of the participants and decreased for 17% (n = 40). 4 However, in a study of 131 breast cancer survivors, 12 the proportion who expressed a desire to become a parent before diagnosis (n = 63, 48%) fell to 28% (n = 36) after diagnosis.
Fertility concerns
Five studies reported infertility among cancer survivors.4,12,13,21,22 One involved both male and female hematopoietic cell transplant survivors. Fertility concerns were significantly higher among hematopoietic cell transplant survivors, with 26% reporting higher values than 7% of the controls (p < 0.001). Altogether, 24% of the survivors supported the idea that problems related to having children had at least a moderate impact on their lives, which was more than 5% of the controls (p < 0.001); 18% of survivors and 8% of controls reported that infertility affected their emotions (p = 0.02); and 14% of survivors and 7% of controls felt that fertility problems affected their relationship with their partner/spouse (p = 0.08). 13
Two studies included only testicular cancer survivors. A three-armed comparison of fertility concerns among survivors who had children both before and after treatment, those who had children after treatment, those who had children before treatment, and those who were childless showed that fertility concerns were most severe among childless survivors (p < 0.001). 21 The Reproductive Concerns Scale results showed that 35% felt unable to talk openly about fertility, 57.7% indicated that they did not have control over their reproductive future, 29.1% were not satisfied with the number of children they had, 19% were grieving owing to impaired fertility, and 9.3% reported low satisfaction with their lives because of impaired fertility. 22
Two studies included only female survivors. Higher Reproductive Concerns Scale scores in breast cancer survivors were related to more depressive symptoms (p = 0.0002), no children, nulliparity at diagnosis, not avoiding pregnancy after diagnosis, treatment-related ovarian disorders, and state of menopause (all p < 0.01). The group with high infertility concern was more likely to be childless at diagnosis, to have had a desire for children before diagnosis, to have had a desire for children after diagnosis, and to have wanted children but never married. 12 Female survivors who wanted to conceive at diagnosis but could not had a higher burden about infertility (p < 0.001) had more intrusive thoughts about infertility and tried not to remember infertility (p < 0.001). Stress was highest among childless women, moderate among women with adopted children or stepchildren, and least distressing among women with at least one biological child. 4
Mental health
Five studies reported on the mental health of cancer survivors.1,12,16,19,20 Female cancer survivors had higher psychological distress scores than their male counterparts (p < 0.025). 20 Among male and female cancer survivors who wanted to have children before treatment, those who had children after treatment (n = 49) had better mental health than those who did not (n = 98) (p = 0.024). 1 Adult survivors of childhood cancer who did not have children had more depression (p < 0.001) and anxiety symptoms (p < 0.001) than the others. 19 Female survivors of childhood cancer had a lower sense of coherence (p < 0.05), more symptoms of anxiety (p < 0.05), and no significant differences in depressive symptoms as compared to the normal group. Clinical assessment was required for 37% (n = 20) of patients with anxiety and 9% (n = 5) with depression. 16 There was no significant difference in depressive symptom scores between women who had children after breast cancer treatment and those who did not (p = 0.80). 12 Breast cancer survivors with a spouse had fewer depressive symptoms (p < 0.001) than those without. In addition, three lifestyle variables (adherence to recommended diet, higher physical activity level, lower body mass index) (p < 0.05), greater social support (p < 0.0001), and fewer major life events (p < 0.0001) were significantly related to fewer depressive symptoms. 12
Fertility consultation or counseling
Nine studies reported fertility counseling or consultations with cancer survivors.15,20,21,23,24,26–29 Among cancer survivors, 68% (n = 34) of men and 56% (n = 56) of women discussed infertility with their oncologists (p < 0.071), and 51% (n = 46) were satisfied with the discussions they had. Survivors who had not completed family planning prior to diagnosis were three times more likely to discuss it with their oncologists than those who had. In total, 33% (n = 30) of the survivors who communicated their desire to have children to their oncologists also contacted a fertility specialist; of these, 80% (n = 24) were very satisfied with the counseling and 7% (n = 2) were not satisfied. 20
One study addressing fertility counseling included only men. Among the 121 who had survived testicular cancer and wanted to have children, 81.0% were not provided with any fertility counseling opportunities. 21
Seven studies included only female survivors. In a survey of 801 female cancer survivors who were 15–39 years old at the time of cancer diagnosis, 17% reported that they had received counseling from a fertility specialist 28 ; 39.7% of 517 breast cancer survivors (18–43 years) also reported this. 24 In a survey of 150 female cancer survivors (18–42 years), 64.7% reported being referred to a fertility counselor; of these, 66.7% were highly satisfied with counseling and 20% were unsatisfied. 27 Fifty-two percent (n = 124) of female cancer survivors (18–44 years) reported having undergone fertility consultation, and those who had received fertility consultation were more likely to be in the highest income group (p = 0.04), have no biological children (p = 0.04), want children (p < 0.001), and be recently diagnosed (p = 0.02) than their counterparts. 29 Infertility severity, lower recognized barriers to fertility consultation, and higher perceived effectiveness of fertility consultation were related to fertility consultation. Those who were recommended fertility consultation by a health care provider and those who told their family and friends about fertility consultation were more likely to seek it. 29
Among young female cancer survivors (n = 204), 15% sought fertility treatments after cancer treatment, and 93% consulted fertility specialists. Those most likely to use fertility treatments after cancer treatment were those who had a history of infertility before cancer diagnosis (p = 0.03), had pursued fertility consultation prior to cancer treatment (p = 0.003), and felt less fertile than other women their age (p = 0.02). 26 Twelve percent (n = 135) of female childhood cancer survivors and 10% (n = 83) of the controls consulted a fertility specialist. The mean age at first consultation for childhood cancer survivors was 27.7 years, significantly lower than for controls (29.9 years) (p < 0.01). 15 In total, 56% (n = 31) of female childhood cancer survivors reported having at least one follow-up reproductive discussion with their health care providers after completing cancer treatment; 5% (n = 3) had a formal reproductive consultation with a fertility specialist after completing cancer treatment, and two of them considered the consultation helpful. Moreover, 54% (n = 29) of the women indicated that they would pursue reproductive consultation if the opportunity presented itself during the survival phase. 23
Support needs
Four studies reported the support needs of cancer survivors.20,22,23,25 In particular, 64.6% of male and female patients with cancer (18–45 years) who wanted to have children believed that their fertility was adversely affected by cancer and subsequent treatments. Meanwhile, 50% of those who wanted a child reported needing supportive care concerning this issue, and 18.2% reported a high need for support. Among those who indicated a high need for support, 80% were women without children. 20 Testicular cancer survivors (n = 29, 14.4%) reported that they would have wanted to counsel about fertility concerns 22 ; breast cancer survivors (n = 14, 87.5%) reported that they would have the courage to conceive if they had enough support and received information from health care providers. 25 Forty percent (n = 22) of female childhood cancer survivors (18–45 years) believed they received adequate information about reproductive health after cancer treatment, and only 5% (n = 3) had a formal reproductive consultation with a fertility specialist after completing cancer treatment, with two of the three deeming the consultation helpful. 23
Discussion
We systematically reviewed the literature on psychological aspects reported by cancer survivors who wished to conceive during and after treatment to understand the impact of pregnancy. According to the results, many showed fertility concerns and a desire for children, as well as possible negative effects on mental health, suggesting a need for psychological support.
Following treatment, survivors were more likely to perceive negative emotions related to finances, partners, and the effect on their lives. 18 During the post-cancer perinatal period, women simultaneously experience happiness and fear, 14 and support that accounts for complex emotions is necessary during the perinatal period as well as during pregnancy. Pregnancy after cancer treatment is likely to involve joy and hope brought about by the pregnancy, as well as negative feelings about the body, finances, and relationships that developed as a result of survivors’ experience with cancer, which may result in an unstable psychological condition.17,18,25 Cancer survivors need long-term and regular support. It would be helpful to form a community where parties can support each other. Participation in such a community may improve quality of life and reduce anxiety about pregnancy and childcare. In Japan, a long-term follow-up system for adolescent and young adult cancer survivors is being established and is expected to provide support at each life stage.
More than 70% of female cancer survivors15,29 and 50% of male cancer survivors 21 desire children. Fertility preservation would be helpful for younger survivors 30 because they were found to be more eager to have children after treatment as they were unlikely to have had any before. 1 However, given the low rate of fertility treatment, 31 effective ways to expand the support for pre- and post-treatment pregnancies need to be explored. Although the desire to have children did not change before and after treatment in most men and women,4,22 it decreased after diagnosis in breast cancer survivors. 12 Breast cancer differs from other cancers in that it is more likely to be associated with breastfeeding behaviors, and factors that increase anxiety, such as decreased confidence in parenting and a tendency to associate pregnancy with recurrence, may decrease the desire to have children. The factors influencing this decline in aspirations need to be investigated.
Fertility concerns are reportedly higher among childless survivors.4,12,21 Breast cancer survivors who are unmarried, childless, or wanting children at the time of breast cancer diagnosis are more concerned about fertility and have been linked to depression. 12 Among testicular cancer survivors, 57.7% stated that they did not feel in control of their reproductive future, and 19% were grieving owing to impaired fertility. 22 As breast and testicular cancers affect reproductive organs, they may be particularly prone to leading to infertility. Therefore, data must be collected for each cancer type to ensure appropriate support. Fertility concerns may also be related to mental health issues, such as depression and grief. The desire to have children and heightened reproductive concerns increase the risk of depression, leading to poorer mental health,1,2 and may require appropriate support. Additionally, as many hematopoietic cells transplant survivors felt that their fertility concerns affected their emotions, relationships with their spouse/partner, and other social relationships, 13 aspects of relationships may need to be considered.
Survivors who had children after cancer treatment had better mental health than those who did not, 1 and those who did not have children had higher depression and anxiety symptoms, 19 suggesting that the presence or absence of children after cancer treatment may affect mental health. However, there was no significant difference in depression among breast cancer survivors by the presence or absence of children. Marital status, cancer stage, estrogen receptor positive status, and lifestyle were associated with depression. 12 Young breast cancer survivors have specific concerns and psychosocial needs, including anxiety about their ability to have children, raising children as cancer survivors, premature menopause, loss of fertility, early ovarian dysfunction, associated symptoms, and the impact of pregnancy on the risk of recurrence.32–35 In a Swedish random sample study, female survivors of childhood cancer had lower Sense of Coherence Scale scores and more anxiety symptoms than women aged 30 years (n = 47). 16 Although they had better mental health than the normal group, some survivors required clinical assessment, 16 suggesting the importance of individualized assessment owing to large individual differences.
The numbers varied widely, with 11% 21 and 68% 16 of male and 12%, 15 17%, 28 40%, 24 56%,20,23 65%, 27 and 93% 26 of female survivors receiving fertility counseling, consultation, or discussion from an oncologist, fertility specialist, or health care professional, respectively. Those who received a fertility consultation had the following characteristics: “did not complete family planning before diagnosis,” 20 “had a history of infertility before cancer,” “had experience with fertility counseling,” and “perceived difficulty in conceiving.” 26 They were also associated with higher incomes, not having biological children, and being recently diagnosed. They had received recommendations for fertility consultation from a health care provider or talked with family and friends about fertility consultation. 29 Survivors who had not received a fertility consultation were those who thought it would be cumbersome and expensive, 29 those with regular menstrual cycles, and those with greater reproductive concerns. 26
Among male and female survivors who wanted to have children, 65% believed that their fertility had been adversely influenced by cancer or cancer treatment, and 50% of them (80% of women who had no children) needed supportive care. 20 Moreover, 14% of testicular cancer survivors wanted fertility counseling, 22 and breast cancer survivors reported that sufficient support, including informational support, was essential for conception. 25 By contrast, only 40% of female childhood cancer survivors thought they were well informed about their reproductive health after cancer treatment. 23
This statistic suggests that women are more likely than men to require fertility counseling. Financial support should be considered because financial strains can hinder consultations. The use of fertility counseling is also influenced by the encouragement and information given by medical professionals. 29 However, although the majority of survivors remember discussing fertility treatment with their health care providers, 36 up to half report an inadequate provision of information. 34 Health care professionals should be knowledgeable about fertility and be able to provide relevant information. The Japanese Society of Reproductive Psychology has been training psychologists specializing in cancer and reproductive medicine since 2016. Support from psychologists with knowledge of both cancer and reproduction will be increasingly needed.
Study limitations
While this review captured a variety of studies, most did not focus exclusively on psychological conditions during pregnancy. Therefore, there is a risk that important information is not captured in the reported studies owing to a lack of focus. Most of the 20 articles were of sound quality, but all were retrospective studies, and few articles mentioned the risk of non-response bias; therefore, the risk of bias was assumed in the study results. Some studies did not distinguish between cancer types or genders and included a wide range of age groups, making it difficult to compare the results. We searched for articles published in the 16-year period from 2007 to 2023 and found that the median year of publication for 20 articles was 2018, indicating that the number of studies has increased in recent years. As the number of women seeking pregnancy during and after cancer treatment is expected to further increase in the future, studies incorporating methods that reduce the risk of bias, such as prospective studies and non-randomized controlled trials, are required.
Conclusions
Cancer survivors were shown to simultaneously experience fear of recurrence or worsening of cancer owing to pregnancy, the joy of pregnancy, and hope for parenthood, and these feelings persisted during the perinatal period. They were concerned about the impact of cancer and reproduction on their finances, relationships with their spouses/partners, and other social relationships. Many cancer survivors who wanted children were found to be concerned about infertility. Some mental health conditions, such as depression and grief, may have their roots in fertility-related worries. Those who had children after cancer treatment had better mental health than those who did not, suggesting that the presence or absence of children after cancer treatment may affect mental health. Many needed fertility counseling, especially women who were childless and wanted children. However, many survivors did not have the opportunity for fertility counseling or thought they did not have sufficient information about reproductive health. Early fertility counseling and pregnancy support during the survivorship phase will result from health care professionals’ knowledge of fertility and their survivors’ access to reliable information.
Footnotes
Authors’ Contributions
All authors contributed to the conception and design of the study. K.K., Y.Y., and T.K. were involved in the conceptualization of the review, database searches, screening, data extraction, quality assessment, and analysis. The conception and drafting of the article were led by K.K., and N.S. contributed to the funding acquisition.
Data Availability
Data sharing is not applicable to this article, as no new data were created or analyzed in this study.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
This work was supported by a
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.