
Abstract
Adolescent and young adult (AYA) patients with cancer often demonstrate suboptimal engagement in cancer care due to a host of logistical, developmental, and psychological factors. This clinical case study of a young adult (YA) with cancer highlights the multiple ways in which social anxiety disorder (SAD) impacted a YA’s engagement in cancer care. The case study also details the use of an evidence-based treatment for SAD to support behavioral change. Identification and receipt of timely evidence-based psychological intervention for SAD have the potential to improve AYA well-being and enhance cancer care engagement.
Literature Review
Researchers and health care organizations increasingly focus on the benefits of treatment engagement and work to improve the degree to which patients actively participate in and utilize the health care services that are available to and appropriate for them. 1 Actively engaged patients routinely schedule and attend their medical appointments, accurately report their medical symptoms, and readily participate in shared decision making. 2 Adolescent and young adult (AYA) patients with cancer (defined by the National Cancer Institute [NCI] as ages 15–39 years) often demonstrate suboptimal engagement in cancer care due to a host of logistical, developmental, and psychological factors. 3 Mental health disorders, such as social anxiety disorder (SAD), represent an important factor that may impact how AYA access and engage with health care services. 4
SAD is defined as a persistent fear and/or avoidance of social situations in which a person may be subjected to the scrutiny of others. 5 Within the United States, SAD is estimated to be prevalent among 9% of adolescents and 12% of adults. 6 Medical settings represent a particularly challenging environment for individuals with SAD due to the numerous direct social interactions required and the sensitive and often intimate health-related discussions that occur. A recent systematic review noted that while most anxiety disorders (e.g., generalized anxiety disorder, panic disorder, etc.,) are associated with an overutilization of health care services, the relationship between SAD and health care utilization remains unclear due to a paucity of data, 7 although several articles have suggested that SAD may be associated with suboptimal health care engagement.8,9
Given that the onset of SAD frequently occurs during adolescence, special attention should be paid to AYA cancer survivors whose challenges with cancer care engagement may reflect underlying anxiety disorders such as SAD.5,10,11 Research suggests that AYA with comorbid chronic health conditions, such as cancer, tend to exhibit lower levels of treatment adherence and engagement,12,13 with one study identifying a particular prevalence of SAD among AYA cancer survivors. 11 In oncology care (i.e., a setting that is often characterized by contact with multiple staff and clinicians), SAD symptoms have the potential to lead to suboptimal engagement including missed clinic visits and limited communication with oncology providers.10,14 This clinical case study of a YA with cancer with cancer highlights how patient engagement in cancer care can be affected by SAD symptoms and describes evidence-based treatment to reduce symptoms and enhance patient engagement across both medical and psychosocial domains.
Overview of the Case
A 30-year-old non-Hispanic White woman was diagnosed with neuroblastoma in 2015 (at age 23), and the metastatic disease recurred in 2018 (at age 26). She reported symptoms of depression and anxiety to her palliative care physician and was referred to the psychosocial oncology team at an NCI-Designated Cancer Center in 2019. Psychiatric assessment conducted by a predoctoral clinical psychology student using a semi-structured clinical interview indicated that the patient met criteria for major depressive disorder, recurrent, severe with anxious distress, consistent with the patient’s care team reports. Subsequent assessment revealed that the patient also met criteria for SAD.
Distinct from her depression diagnosis, the patient reported feeling particularly concerned about how other people were judging her in various social situations including when she was at work, out with friends, and running errands. She frequently perceived herself to be stumbling over her words and sweating profusely, leading her to fear that people thought she was incompetent. She reported the onset of specific SAD symptoms occurring as early as adolescence, but she noted that after losing her hair during chemotherapy, her behaviors and cognitions associated with SAD increased significantly. She described frequently engaging in emotional and behavioral avoidance designed to manage distress within social settings (e.g., being on her phone, not engaging in small talk, and ordering groceries online to avoid in-person shopping).
The patient reported specific feared outcomes and avoidance behaviors that were impacting her adherence to medical appointments and interfering with her communication and medical care coordination. For example, she described feeling hesitant about accurately expressing the extent of her physical pain because she worried that the oncologist would negatively judge her body weight. She described challenges with health advocacy, reporting multiple instances in which she wanted more information or explanation from her providers but felt too embarrassed to ask additional questions. She also reported numerous examples of behavioral avoidance (e.g., discontinuation of psychotropic medications without medical consultation, lack of follow through with referrals) and identified various strategies she employed to minimize fear of being judged as incompetent by others. Despite limited medical engagement, this patient presented with notable strength and resiliency, as evidenced by her decision to report psychological concerns to her palliative care team, her willingness to engage in psychological treatment, and her ability to maintain long-term employment throughout cancer treatment.
At the time of referral to psychology, the patient had discontinued an immunotherapy medication due to an adverse reaction and was receiving palliative radiation and surveillance scans. Subsequently, her local oncology team recommended that she enroll in a clinical trial at a children’s hospital in a neighboring state that involved monthly airplane travel, a new oncology team, additional scans, and strong adherence to a new oral medication associated with the clinical trial. Recently, the patient transitioned off the clinical trial after achieving cancer remission and now continues to be followed by her local oncology team.
Psychotherapy treatment
Psychotherapy intervention utilized a theoretically informed and empirically supported exposure-based treatment approach15–17 detailed in Managing Social Anxiety: A Cognitive-Behavioral Therapy Approach. 18 Therapy took place at a behavioral health clinic associated with a university’s clinical psychology training program. Initial treatment sessions focused on identifying the patient’s early fears of social rejection and connecting those fears to her current fears of specific social situations and outcomes. The primary focus of the first phase of SAD therapy centered around identifying the patient’s negative automatic cognitions (e.g., likelihood and cost biases) in social situations and using cognitive restructuring to generate more accurate and balanced thought processes. These efforts included psychoeducation on different types of cognitive distortions and use of strategies to help the patient more accurately evaluate and challenge unhelpful or inaccurate cognitions. The second phase of SAD therapy focused on using exposure therapy and involved (a) working with the patient to identify specific social situations that she feared, (b) encouraging her to intentionally engage in specific feared social situations as a means of testing the accuracy of her feared predictions of negative outcomes, and (c) changing her relationship to anxiety in social situations. For example, to build confidence with symptom reporting and appointment scheduling, we designed a series of “small talk” exposures in which the patient met with confederates (i.e., clinic staff members unknown to patient) and engaged in both prescribed and unscripted small talk conversations. Over time, the patient learned to identify her automatic thoughts, challenge her negative assumptions using cognitive restructuring, and approach social situations differently within and outside of clinical sessions, including in cancer care settings.
Therapeutic progress
As indicated in Figure 1, this patient has thus far exhibited mild reductions on her reported fear and avoidance of common social situations as assessed with the Liebowitz Social Anxiety Scale (LSAS; 24 self-report items). 19 At the same time, she has demonstrated significant functional improvement in behavioral SAD indicators across several domains (Table 1). For example, at the beginning of therapy for SAD, the patient frequently expressed extreme hesitation to disclose the extent of physical pain she was experiencing to her cancer treatment team because she worried that doing so would lead to further negative evaluation of her body size. Sixteen sessions into therapy, she gained awareness of how specific cognitive distortions were contributing to her long-standing fears of negative body evaluation from others and demonstrated increased willingness to accurately report pain symptoms to her oncologist. Similarly, by session 36, the patient demonstrated notable improvements in her ability to advocate for her medical needs (e.g., requesting an additional visit with the clinical trial oncologist) and to demonstrate interpersonal effectiveness (e.g., directly addressing conflict with a close friend). Treatment has continued with a focus on targeting the underlying fears associated with social situations occurring both within and outside of medical settings.
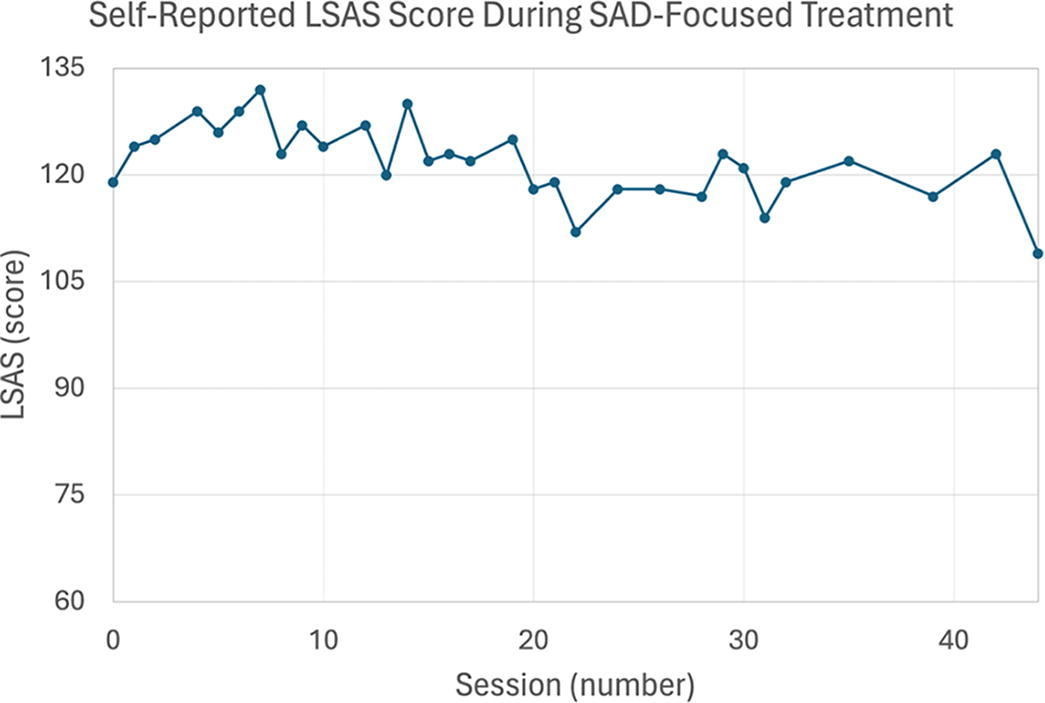
Self-reported LSAS during SAD-focused treatment. Session 0 refers to the start of SAD-focused treatment. Patient-reported LSAS scores were obtained for 33 out of 44 SAD-focused CBT sessions, spread across 82 weeks. LSAS is a 24-item patient self-report questionnaire assessing the ways in which social anxiety impacts a person’s life. The clinical cutoff for SAD on LSAS is a score of 60, 19 with greater scores indicating greater fear and avoidance in social situations. Elevations in self-reported measures are expected when starting SAD treatment, resulting from increased patient knowledge and awareness of anxiety symptoms. CBT, cognitive behavioral therapy; LSAS, Liebowitz Social Anxiety Scale; SAD, social anxiety disorder.
Behavioral and Self-Report Markers of Progress During SAD-Focused Treatment
The behavioral markers of progress occurred during the course of 44 SAD-focused CBT sessions spread across 82 weeks. The patient’s corresponding baseline behavior is provided to illustrate the degree of behavioral change exhibited during SAD-focused therapy.
CBT, cognitive behavioral therapy; SAD, social anxiety disorder.
Summary and Conclusions
Numerous psychological and logistical barriers can impede AYA engagement in and continuity of cancer care. 20 This case report illustrates that one patient-level barrier to engagement may be the degree of social anxiety that patients face while interacting with their cancer care team members. We document the multiple ways in which SAD impacted a YA’s engagement in cancer care, and we demonstrate the use of an evidence-based treatment for SAD to support meaningful behavioral improvements (e.g., advocacy in and outside of the cancer setting, engagement with life activities such as grocery shopping and interactions with friends). A standard course of treatment for SAD in a general outpatient therapy setting typically lasts between 11 and 20 sessions,21,22 but treatment length is variable based on individual factors (e.g., rate of symptom reduction, maintaining factors, life events, and crises). 17 This case report reveals that therapeutic progress may take more time in the context of cancer while still yielding important patient-level improvements. Additionally, travel, medical scans, and procedures associated with the clinical trial represented obstacles to SAD treatment adherence (i.e., delayed sessions).
SAD is a common psychiatric disorder, yet its assessment and impact are rarely considered within medical settings, particularly among AYA with cancer. At the patient level, SAD symptoms often emerge during adolescence, which may coincide with AYA cancer diagnosis and survivorship, further strengthening the rationale for greater focus on SAD among AYA. Although this case report focused on the patient as the change agent, it is also important to consider interpersonal and system-level variables that can support improved identification and treatment of SAD among AYA with cancer. For example, this psychotherapy treatment was provided outside of the cancer center. At the system level, on-site, multidisciplinary collaboration may improve treatment efficiency and provide a better understanding of how SAD-focused treatment can directly impact cancer care milestones. At the interpersonal level, greater clinician awareness of SAD symptoms may lead to more efficient identification of individuals struggling with SAD within the context of cancer care. If low patient engagement is observed, we suggest that cancer care providers utilize a brief evidence-based SAD assessment such as the LSAS or the Social Anxiety Scale for Adolescents 23 to inform subsequent referral to supportive cancer care services. If direct assessment of SAD for an AYA is not feasible within a cancer care setting, we recommend that cancer care clinicians directly refer the patient to a psychologist or embedded mental health professional at the cancer center.
Although this case study must be considered within the context of case report generalizability limitations, it offers a window into assessment of SAD among AYA patients with cancer, highlights the potential influence of SAD on patient engagement with treatment, and details the positive impact evidence-based SAD treatment can have on AYA behavior and well-being both within and outside of medical settings. Taken together, accurate identification and timely psychological intervention for SAD has the potential to improve AYA psychological well-being, engagement in medical care, and appropriate utilization of oncology-related health care services among AYA with cancer.
Footnotes
Acknowledgment
The authors would like to thank the patient who consented to participate in this case report for their time and effort.
Authors’ Contributions
E.S.V.H.: Conceptualization, resources, writing—original draft, writing—reviewing and editing, and visualization. A.M.P.: Writing—original draft, writing—reviewing and editing, visualization, and supervision. T.K.T.: Resources, writing—reviewing and editing, and visualization. J.J.: Conceptualization, resources, writing—original draft, writing—reviewing and editing, visualization, and supervision.
Author Disclosure Statement
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest.
Funding Information
No funding was received to assist with the preparation of this article.