
Abstract
Germ cell tumors (GCTs) are chemosensitive neoplasms with high cure rates; however, a small group of patients present tumors with refractory chemotherapy, with a dismal prognosis and few effective management options. Although immune checkpoint inhibitors (ICIs) are approved for use in chemotherapy refractory GCT, the evidence supporting this indication remains scarce. Original research studies were included on patients with GCTs refractory to chemotherapy treated with ICI up to December 2023. Comprehensive search strategies databases and MeSH keywords were used to locate eligible literature. Study characteristics, participant demographics, and oncological outcomes were recorded. A total of 13 studies (n = 106) were included, five single-patient case reports, one retrospective cohort, six-phase II randomized controlled trials (RCTs), and an abstract from the preliminary results of a phase II RCT. Most of the studies evaluated did not request biomarkers as inclusion criteria. Median overall response rate across studies was 3.4% (range, 0–57) and 0% (range, 0–6) in retrospective cohort and phase II studies. Progressive disease as the best response was present in most patients, with 75% (range, 0–82.9) in the overall population and 82% (range, 75 −83) in the retrospective cohort and phase II trials. Some of the most durable clinical responses documented in this systematic review corresponded to high tumor mutational burden (TMB-H) or high microsatellite instability (MSI-H)/dMMR tumors. Retrospective cohorts and clinical trials evaluating ICIs for the treatment of chemo-refractory GCTs documented limited activity of these drugs as a single intervention in patients not selected by biomarkers, with a tendency to better results described in those with TMB-H or MSI-H/dMMR tumors.
Introduction
Germ cell tumors (GCTs) are the most common solid tumors in young men; 1 these are chemosensitive neoplasms with high cure rates, even in the metastatic setting. 2 However, a small group of these patients will present tumors refractory to platinum-based and/or high-dose chemotherapy, with a dismal prognosis and very few effective and safe management options. 3 The mechanisms by which these tumors generate resistance to cisplatin are multifactorial and have not been completely elucidated. 4 Immunotherapy, particularly with programmed cell death protein-1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors, has proven to be effective in the treatment of several solid tumors and has been an attractive option to be explored in this group of patients. 5 Currently, the National Comprehensive Cancer Network guidelines estipulate as an option the use of the anti-PD-1 monoclonal antibody pembrolizumab in patients with GCTs refractory to platinum-based chemotherapy with high microsatellite instability (MSI-H/dMMR) or high tumor mutational burden (TMB-H), the above based mainly on basket studies with little or no representation of this tumor line.6–9
Immune checkpoint inhibitors (ICIs) exert their effect by blocking inhibitory signals from the immune system, mainly inhibiting the interaction between PD-1 and PD-L1 or PD-L2, leading to nonspecific reactivation of T cells and tumor-specific T cells. 10 PD-1 is a member of the T cell regulatory family that is expressed on the surface of activated T cells, B cells, and macrophages. PD-L1, the PD-1 ligand, is expressed in tumor cells, macrophages, and T cells, among others. 11 PD-1 plays a key role in regulating and maintaining the balance between T cell activation and immune tolerance. Cancer cells can use this immune checkpoint and cause T cells and NK cells to become anergic and unable to destroy the tumor cells. 12 The binding of PD-L1 or PD-L2 on tumor cells to their receptor PD-1 on T cells can also inhibit the cytotoxic T cell response.13,14
The testicle is an immunologically privileged site.15,16 It represents a tissue with naturally suppressed immune responses, which favors immune tolerance to spermatids and spermatocytes. The direct expression of PDL-1 in normal testicular tissue has not been consistently documented. 17 Lack of PD-1 expression has been documented in GCTs, along with higher levels of PD-L1 compared with normal testicular tissues. 18 These findings emphasize the importance of PD-L1 in the signaling and growth of TGCTs, which constitutes an attractive pathway to be pursued for the treatment of cancer through immunotherapy.19,20 PD-L1 expression on GCTs tumor cells and a tumor microenvironment with T cell mediated inflammation are associated with poor prognostic features, including the presence of ≥3 metastatic sites, increased serum tumor markers, and/or nonpulmonary visceral metastases.21–26
Although ICIs are approved for use in selected cases of GCTs refractory to chemotherapy, the evidence supporting this indication is limited. 17 The latest approaches to analyzing this scenario do not include the results obtained in the most recent publications and the potential usefulness of biomarkers. 27 We aimed to analyze the oncological results documented in patients with GCTs refractory to chemotherapy to better understand which patients could benefit the most from these treatments while minimizing physical and economic toxicity.
Materials and Methods
This systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and was registered in PROSPERO (CRD42023485470) 28 and approved by the Research Committee of the Faculty of Medicine of the Autonomous University of Nuevo León with code RVS23-00034.
Search strategy
An experienced librarian helped design and carry out the search strategy. We employed the Scopus, Web of Science, MEDLINE, and EMBASE electronic databases for our search strategy from the time of their creation to November 2023; gray literature was searched through Google Scholar. The design and execution of the search strategy were completed in December 2023. The initial strategy was complemented by reviewing the references of selected studies to identify any potentially relevant studies that were missed and by searching clinical trial registries as well as contacting experts in the field to identify any unpublished or in-progress eligible studies.
Selection criteria
Articles on randomized controlled trials (RCTs), quasi-RCTs, or observational studies report the use of immunotherapy in platinum-refractory GCTs. The search strategies used keywords and Boolean operators described as follows: “testicular cancer,” “germ cell tumors,” “platinum refractory testicular germ cell tumor,” “genitourinary cancer,” “immunotherapy,” “immune checkpoint inhibitors,” “PD-1, PD-L1 in testicular cancer,” “clinical trials.” We excluded reports with ambiguous or not-reported design, population, intervention and outcomes of interest, and lack of detailed information, as well as studies with language barriers for data extraction.
Data management
All search results were uploaded to EndNote X8 for deduplication in December 2023. Resulting studies were uploaded to Distiller Systematic Review software for title/abstract and full-text screening in December 2023. All search strategy results were documented per database before and after duplication.
Study selection process
The selection of studies was carried out in two phases (title/abstract and full-text selection). In each phase of the review, two reviewers worked independently and in duplicate to assess study eligibility. Randomized interrater agreement was assessed at each phase using Cohen’s kappa statistic. Prior to each screening phase, a pilot test was carried out with a random sample of studies based on the results of the search strategy to standardize the reviewers’ criteria. Disagreements were discussed, and the criteria were adapted if necessary. The pilot test was repeated until a kappa index >0.70 was reached. During this phase, the discordant decisions were passed to the full-text phase to achieve a highly sensitive selection. Eligibility was then assessed through a full-text screening. Disagreements between the reviewers during this second phase were resolved by consensus, and if this was not achieved, a third reviewer served as arbitrator (Fig. 1). Throughout the process, the number of included and excluded articles were documented, and the reasons for exclusion of each study were recorded.
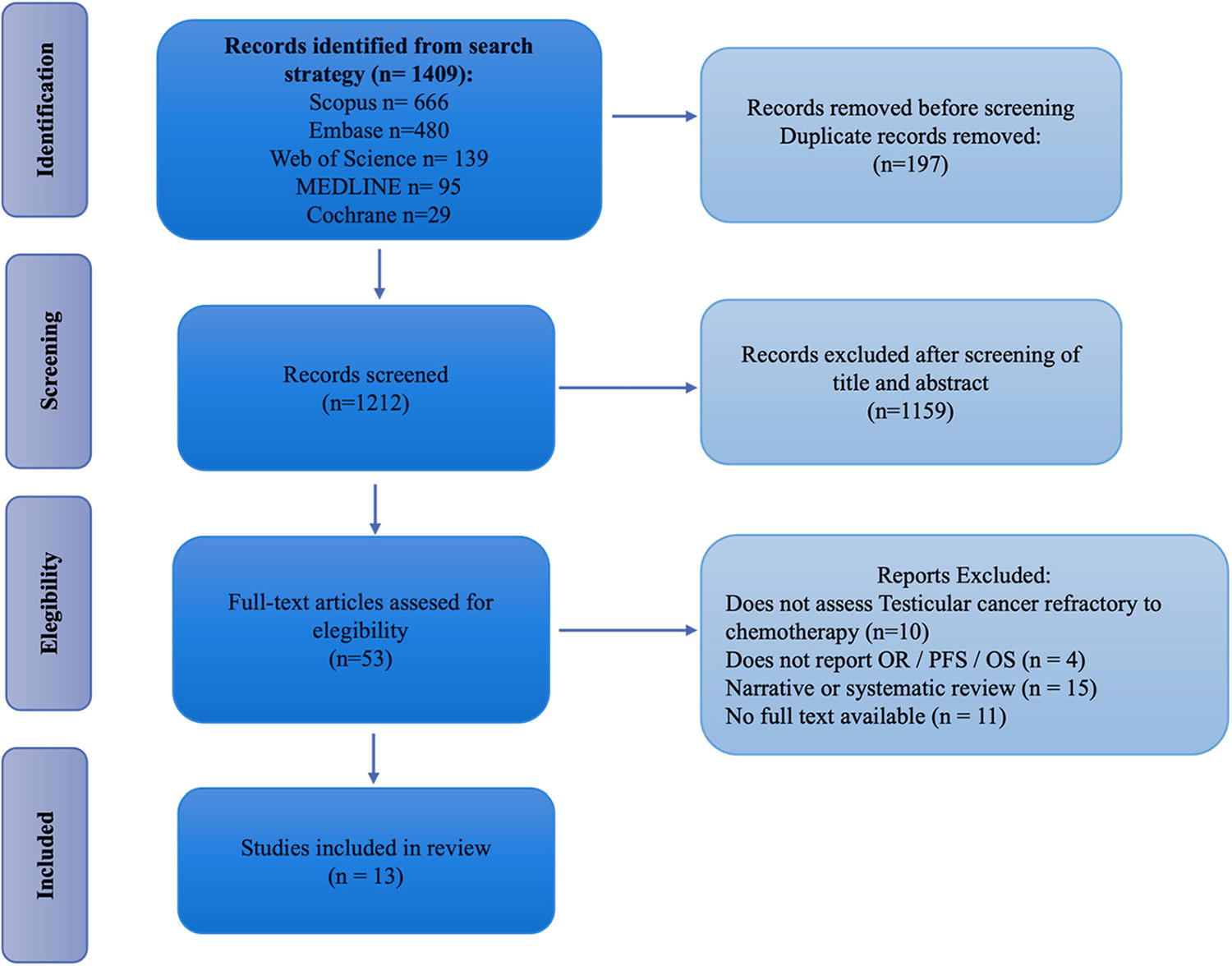
PRISMA flow diagram of literature search, eligibility, and inclusion process. OR, objective response criteria; OS, overall survival; PFS, progression-free survival; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data collection process and missing data
Two independent reviewers collected data from all eligible articles by duplicate using a web-based data extraction form. The type of study, title, author data, follow-up, year of publication, baseline characteristics of the patients, biomarkers, and oncological outcomes. Disagreements were resolved by consensus, and in case of disagreement, a third reviewer aided with the final decision. Prior to this process, the two reviewers conducted a pilot test working independently and in duplicate. Reviewers provided feedback on suggested adjustments and, where necessary, applied to the preliminary extraction form.
Data synthesis
Included studies were described as a narrative synthesis including author, year of publication, type of study, type of tumor, mechanism of drug action, PDL1 biomarkers, oncological outcomes, and response evaluation. We described the median response rates and ranges across studies that reported them and performed a sub-analysis with cohort and phase II trials only, to remove bias from case report studies (with one reported patient). Further, we perform a comprehensive discussion of all studies.
Results
Systematic review and characteristics
A total of 1,409 publications were identified through the search strategy employed, and we excluded a total of 1,212 studies due to duplication. PRISMA flow diagram is reported in Figure 1. A total of 13 studies encompassing 6 countries (n = 106) were identified for inclusion [26, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40] 5 of which corresponded to single-patient case reports (n = 5), 1 was identified as a retrospective cohort (n = 7), 6 were phase II RCTs (n = 65) and we included a recent abstract from the preliminary results of a phase II RCT (n = 29), as shown in Table 1.
Characteristics of Included Studies in the Systematic Review
EGCT, extragonadal germ cell tumor; GCT, germ cell tumor; ND, no data; RCT, randomized clinical trial.
Patient characteristics
A total of 106 patients from the 13 included studies were analyzed, with a median age range of 29 to 38 years, the majority were male (from data of available studies, n = 10). Nine studies reported results of only non-seminomatous tumor patients. Six studies included patients with primary extragonadal GCTs (with proportions of patients ranging between 8% and 57%) (Table 1). Most of the studies evaluated did not request biomarkers as inclusion criteria.
The mechanism of action of the ICIs was ant-PD1 in 9 studies, anti-PDL1 in 1, anti-PD1/anti-CTLA4 in 1, and anti-PDL1/anti-CTLA4 in 2. Seven studies reported PDL1 positivity, ranging from 13.8% to 100% across studies. RECIST was the most frequent response rate evaluation method (n = 12), followed by biochemical response (n = 7) (Table 2). In case report studies, progression-free survival (PFS) ranges from 6 to 14 months (n = 3), while overall survival (OS) ranges from 1.5 to 14 months (n = 3). In the rest of the studies, median PFS and OS ranged from 0.9 to 2.4 months (n = 4) and 2.7 to 10.6 months (n = 5), respectively.
ICI Characteristics and Patient Outcomes Across Studies
CR, complete response; ICI, immune checkpoint inhibitor; ORR, overall response rate; PD, progressive disease; PR, partial response; SD, stable disease.
Median overall response rate across studies was 3.4% (range, 0%−57%) and 0% (range 0%−6%) in retrospective cohort and phase II studies. Complete response was not reached in any patient. Progression of disease as the best response was present in the majority of patients, with 75% (range, 0%−82.9%) in the overall population and 82% (range, 75%−83%) in the retrospective cohort and phase II trials (Table 3). Some of the most durable clinical responses documented in this systematic review corresponded to TMB-H or MSI-H/dMMR tumors.
Median Response Rates Across Studies (Overall and in Retrospective Cohort/Phase II RCT Studies)
RCT, randomized clinical trial; ORR, overall response rate; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Discussion
Immunotherapy in refractory germ cell tumors, reports, and case series
There are case reports or case series that have documented a possible role for immunotherapy in the treatment of advanced GCTs refractory to chemotherapy. Shah et al. reported a case of embryonal carcinoma positive for PD-L1 by immunohistochemistry with cervical and retroperitoneal involvement treated with a single dose of the anti-PD-1 monoclonal antibody nivolumab (3 mg/kg), demonstrating a 33% reduction in tumor volume according to RECIST 1.1 criteria and a 49% reduction according to immune-related response criteria. Subsequently, the treatment was changed to bleomycin, etoposide, and cisplatin for three cycles achieving a complete radiological response. 26
In a case series, seven patients with platinum-refractory NS GCTs were treated with an anti-PD-1 (nivolumab or pembrolizumab). Four patients had rapid disease progression and died shortly after starting treatment. Three others continued receiving therapy for at least 6 months. Among them, one patient (embryonal carcinoma) achieved a partial radiological response, one had a stable disease, and one had a mixed response followed by progression. It is important to mention that the only patient who demonstrated a partial response received concomitant etoposide. There appeared to be no association between PD-L1 status and response to treatment, as some PD-L1 negative tumors showed response to immunotherapy, while other PD-L1 positive tumors showed disease progression despite anti-PD-1 treatment. 31
A case report showed the efficacy of nivolumab in metastatic choriocarcinoma. A man with choriocarcinoma metastatic to lungs, bone, brain, and lymph nodes demonstrated disease progression after multiple lines of chemotherapy, in addition to stereotactic radiosurgery and high-dose chemotherapy with tandem autologous stem cell transplantation. Subsequently, he received nivolumab for a period of 14 months, obtaining a partial radiological response and stability of tumor markers. 38 Similarly, a case of primary retroperitoneal NS GCTs refractory to multiple lines of chemotherapy was reported that achieved sustained stable disease 13 months after starting treatment with nivolumab. 30
Pembrolizumab was also evaluated as fourth-line therapy in a young man with refractory metastatic choriocarcinoma. This patient presented with metastatic choriocarcinoma at the time of diagnosis, with lung, brain, and lymph node disease. He was treated with three different lines of standard chemotherapy, including peripheral hematopoietic stem cell transplantation, which was followed by relapse. He subsequently received a cycle of pembrolizumab 200 mg, with a marked increase in serum B-HGC 3 weeks after its application, so treatment with this drug was interrupted. 39 Another case report described the benefit of pembrolizumab in a patient initially diagnosed with pure seminoma who had failed multiple lines of chemotherapy. Analysis of one of the sites of progression at the lung demonstrated a mixed germ cell tumor with positivity for PD-L1, as well as high microsatellite instability (MSI-H). After 6 months of starting treatment with pembrolizumab, the patient maintained a partial response to the target lesions. 29
When analyzing the reports and case series presented, it is important to note that some cases documenting the activity of ICIs in refractory GCTs involved the use of chemotherapy either subsequent to or concomitant with ICI treatment. Therefore, it is difficult to determine the specific role immunotherapy played in these patients.
Immunotherapy in refractory germ cell tumors, clinical trials
To date, results from prospective studies aimed at identifying the clinical efficacy of ICIs in patients with advanced GCTs have been reported. A phase II study evaluated the role of the anti-PD-1 antibody pembrolizumab at a dose of 200 mg every 3 weeks until toxicity or progression in patients with platinum-refractory advanced GCTs. This was a two-stage design, in which no clinical benefit was demonstrated for pembrolizumab in patients with metastatic GCTs who progressed after at least one line of salvage chemotherapy. This study only included 12 patients with NS GCTs, regardless of their PD-L1 status, as only two patients had PD-L1-positive tumors. Ten of the 12 patients progressed (including those with PD-L1-positive tumors) and only two achieved a mixed response, with radiological stable disease associated with biochemical AFP progression. Because there were no objective responses in the first 12 patients, the study was closed early. 32 Another study analyzed a pre-specified cohort from an open-label phase II study, which evaluated the efficacy of pembrolizumab in 12 patients (10 men and 2 women) with previously treated GCTs (median previous lines 3.5) not selected by biomarkers. Three patients had radiographical stable disease as the best response, none had an objective response. The median PFS and OS in this study were 2.4 and 10.6 months, respectively. 35
In an open-label phase II randomized clinical trial, the anti-PD-L1 durvalumab was evaluated at a dose of 1500 mg, alone or in combination with tremelimumab 75 mg (anti-CTLA-4) for four cycles administered every 28 days, followed by single-drug durvalumab until toxicity or progression. In total, 22 patients were enrolled in this study (11 in arm A with durvalumab alone and 11 in arm B with durvalumab plus tremelimumab). Due to the significant number of patients (72.7%) who presented hyperprogression of the disease with durvalumab monotherapy, arm A was closed. One patient with pure seminoma in arm B achieved a partial response in multiple lung metastases. Another patient in this arm presented stable disease with decreased serum tumor marker. All remaining patients experienced tumor progression as the best response, while hyperprogressive disease was described in four (36.4%) of them. The responses in this study occurred independently of the molecular characteristics of the tumor and the expression of PD-L1. 33 Another single-arm phase II study only available as an abstract and therefore not included in the systematic review evaluated the combination of durvalumab with tremelimumab in two different administration regimens, followed by maintenance durvalumab for up to 1 year in 29 patients diagnosed with platinum-refractory GCTs. Of the total cases analyzed, four obtained stable disease and one had a partial response, in the rest, disease progression was documented as the best response to treatment. 37
A phase II study evaluated the anti-PD-L1 avelumab at a dose of 10 mg/kg biweekly until disease progression or toxicity in patients with GCTs with multiple relapses and/or refractory to chemotherapy treatment not selected by biomarkers. The primary endpoint was PFS at 12 weeks. Eight heavily pretreated patients, predominantly with NS GCTs, were enrolled in this study. After a median follow-up of just 2.6 months, all patients experienced disease progression as the best response, therefore not meeting their primary objective. 34
A single-arm phase II trial evaluated the use of the anti-PD-1 nivolumab at a dose of 240 mg every 2 weeks until toxicity or disease progression in 17 patients with GCTs refractory to chemotherapy (median of three previous lines). One patient had a partial response, four had stable disease, and 12 had disease progression as the best response. In the patient who achieved partial response, it lasted for 90 weeks. Genomic sequencing revealed a high tumor mutational burden in the tumor of the patient who achieved a long-lasting partial response, while the expression of PD-L1 did not correlate with the response obtained with the treatment. 36
In the phase II study conducted by McGregor et al., 57 patients with genitourinary tumors of different strains were treated with nivolumab 3 mg/kg and ipilimumab 1 mg/kg every 3 weeks for 4 doses, followed by nivolumab 480 mg fixed dose every 4 weeks until toxicity or disease progression. Of the total of patients, five were classified as having platinum-refractory GCTs, only one patient in this group achieved stable disease, while the remaining four had disease progression as the best response. 40
There are also phase II basket studies that are currently evaluating the clinical activity of immunotherapy in various types of advanced tumors, in which it is planned to recruit patients with GCTs refractory to chemotherapy (NCT02834013/NCT02832167).
The results of clinical trials that evaluated the efficacy of ICIs in refractory GCTs are contradictory with previously published reports and case series. A possible explanation for this observation may be the insufficient ability of ICIs to eliminate the immune tolerance characteristic of GCTs. Testicular tumors are characterized by a physiologically suppressed immune microenvironment. A pathological vascular system in combination with an altered blood–testis barrier is associated with an increased entry of cytotoxic immune cells into tumor tissue. However, due to their exposure to inhibition through PD-L1-mediated immune escape, these cells cannot carry out their antitumor and cytotoxic activities. 17 Concomitant treatment with antiangiogenics could result in the normalization of the structure and function of the tumor vasculature and ultimately contribute to more efficient anti-PD-L1/PD-1 drug delivery. 41 Likewise, the low mutational burden and microsatellite instability described in GCTs, which translates into a low number of neoantigens, could also participate in the poor clinical activity of these agents.42,43 Although the use of ICI as a single intervention has failed to produce meaningful clinical outcomes in biomarker-unselected populations with platinum-refractory GCTs, inhibiting other immune checkpoints such as TIGIT and LAG-3 could lead to improved clinical outcomes.
To date, it has not been demonstrated that immune checkpoint inhibition as a single intervention has a relevant role in the treatment of chemotherapy refractory GCTs not selected by biomarkers outside of clinical trials. While some case reports have suggested that there is a population of patients who could potentially benefit from immune checkpoint inhibition, we currently lack valid predictors for clinical decision-making in routine practice.
High tumor expression of PD-L1, as observed in choriocarcinomas, has been considered a promising predictive biomarker; however, clinical results reviewed in clinical trials and case reports have shown disappointing results regarding the role of this biomarker as a predictor of a better response to ICIs. For patients with GCTs refractory to standard therapies, genomic testing for MSI and TMB is crucial, as the Food and Drug Administration has approved pembrolizumab for the treatment of MSI-H and TMB-H (≥10 mutations/megabase) solid tumors that have progressed after prior treatment and lack satisfactory alternative options. Microsatellite instability and/or high tumor mutational burden could potentially serve as predictors of response to ICIs, as reported in the reviewed literature29,36; however, only a small percentage of GCTs exhibit these molecular characteristics, and further high-quality research is needed to determine their clinical significance in long-term oncological outcomes. Additionally, the clinical benefit of combining immunotherapy with conventional cisplatin-based chemotherapy and/or its use in previous lines of treatment cannot be ruled out. Therefore, further clinical trials are needed to elucidate the clinical and molecular factors that can predict the response to immunotherapy with ICI in patients with platinum-refractory GCTs in a practical and reproducible manner.43,44
Conclusions
GCTs remain common in young men, with an excellent response rate to standard treatment with platinum-based chemotherapy. However, a small percentage of these tumors will progress despite multiple lines of chemotherapy, leading to a poor prognosis. Immunotherapy has emerged as an attractive treatment option for this group of patients. This analysis showed encouraging results in case reports/series, some of which used a combination of ICIs plus concomitant or subsequent chemotherapy. In contrast, data from clinical trials with ICIs as monotherapy have documented a limited activity of these drugs, with better outcomes described in tumors with high tumor mutational burden or microsatellite instability. Future prospective studies should aim to select patients using biomarkers to elucidate better the clinical and molecular factors that predict response to ICIs in this setting.
Footnotes
Authors’ Contributions
C.E.S.M. and R.V.V.-G. designed the study. C.E.S.M., R.V.V.-G., C.D.D., and E.G.-R. wrote the article. S.A.A.R., A.S.G.-G., R.Q.-H., K.A.S.-S., and N.E.A.-V. contributed to data collection. C.D.D. performed the statistical analysis. C.E.S.M., R.V.V.-G., and C.D.D. performed interpretation of the results. C.E.S.M., R.V.V.-G., O.V.G., C.D.D., and N.E.A.-V. performed critical analysis and review. All authors read and approved the final article.
Availability of Data and Materials
If you require access to the data, you can contact the corresponding author.
Ethical Approval
Research was conducted ethically in accordance with the Declaration of Helsinki. This was not a human or animal study, therefore informed consent was not required. It was approved by the Research Committee of the Faculty of Medicine and University Hospital of the Autonomous University of Nuevo León with the approval code RVS23-0034.
Author Disclosure Statement
All authors read and approved the final article and declare that there are no conflicts of interest of a financial or personal nature. The article has not been published elsewhere and is not under consideration for publication elsewhere.
Funding Information
No funding has been received for this article.