
Abstract
Purpose:
Childhood cancer survivors (CCS) represent a growing population worldwide, and lifelong follow-up care is recommended for most. Once CCS become adults, the transition to adult care is emerging. Today, there is no transition or long-term follow-up care model in the adult setting that clearly outweighs others. We therefore aimed to evaluate the transition to physicians outside the hospital.
Methods:
In this single-center, cross-sectional, questionnaire-based study, we assessed in 2022 the current follow-up care situation of CCS who already transitioned to physicians outside the hospital (family physicians, pediatricians). We asked CCS about cancer knowledge, worries, self-management skills, and expectations and physicians about their experience with CCS and their needs when caring for CCS. We included physicians where a CCS was transitioned to. We compared the results with CCS transitioned in a hospital setting and used descriptive statistics.
Results:
Twenty-three CCS responded to the questionnaire (median age at questionnaire of 22 years, median 14 years since diagnosis). Nearly two-thirds reported not being in follow-up care anymore. The cancer knowledge was good, and cancer worries were low. Twenty-eight physicians responded with 21 reporting that they care for CCS. Half of them see CCS for acute problems only. Physicians are open to care for CCS but request the necessary recommendations and would also be available for respective training.
Conclusion:
Transition to physicians might be an option for selected CCS. However, education and empowerment of CCS early on and education of physicians is urgently needed to prevent loss to follow-up, which may lead to lifelong nonengagement and incorrect perceptions about future health.
Introduction
Childhood cancer survivors (CCS) represent a growing population worldwide.1–4 In Switzerland, around 400 children and adolescents up to the age of 19 years are newly diagnosed with cancer per year. 5 With a 5-year survival of 87%, approximately 345 former CCS become long-term survivors annually. Growing evidence shows that a large proportion of CCS suffers from chronic medical conditions, so-called late effects, years to decades after the completion of treatment. 6 As a result, specific long-term follow-up (LTFU) care guidelines for CCS have been developed. There are the guidelines from the Children’s Oncology Group (COG) in the United States, from the Dutch Children’s Oncology Group (DCOG), or from the United Kingdom.7–9 In 2010, the International Guideline Harmonization Group started harmonizing the different national guidelines, based on evidence and a clear predefined methodological approach. 10
Having LTFU care guidelines is an important element, but equally important is the place of care. Follow-up care starts in the pediatric oncology setting, where LTFU care guidelines are broadly implemented. By reaching adolescence and adulthood, the former pediatric oncology patients need ongoing care and a LTFU care model that takes the social, psychological, and somatic aspects of from adolescents to adults into account. This transition phase with change in the care setting is critical. Rokitka et al. showed that the adherence to LTFU care drops with increasing time from end of treatment. 11 This trend is going in the opposite direction for the development of late effects, which increase in frequency with increasing time from diagnosis. Knowledge about the diagnosis, treatment received, and the resulting potential risk to develop late effects are important facilitators to transition and to adherence to LTFU care. 12 Different transition models have been studied previously and are implemented in daily practice. 12 The transition model used depends on the national or local LTFU care structure and on the CCS’ preferences. The following models are described: 1) transition to adult oncology or internal medicines from one visit to another; 2) transition to adult oncology or internal medicines in a stepwise approach during joint visits with pediatric oncologist and adult physicians in the hospital; 3) specialized LTFU clinics with multidisciplinary teams, consisting of pediatric and adult physicians, providing life-long LTFU care; 4) transition to primary care physicians in collaboration with a cancer center; and 5) transition to primary care physicians with adult specialist consultations if needed (e.g., cardiologist) but independent of cancer centers.
Today, there is no transition or LTFU care model in the adult setting that clearly outweighs the others. Local circumstances and availabilities of infrastructure as well as insurance aspects might have an impact on the model chosen by the different countries and hospitals. This is also true for Switzerland. In a previous publication, we could show that cancer knowledge, cancer worries, and self-management skills do not differ between Swiss CCS, that transition from one visit to another to the adult oncologists compared to those, who transition during at least two joint visits with pediatric and adult oncologists. 13 With this study, we aim to describe the current LTFU care situation of CCS that have been transitioned to a primary care physician, including family physicians and pediatricians.
Methods
This single-center, cross-sectional study is part of the Aftercare of Childhood Cancer Survivors (ACCS) study. 14 The ACCS study is a prospective, multicenter, observational study, including a cross-sectional and longitudinal part. For this study, CCS were included in the cross-sectional part and received one questionnaire. We developed a separate questionnaire for physicians. The ACCS study is registered at ClinicalTrials.gov (NCT04284189), and ethics approval was issued by the cantonal ethics committee Ethikkommission Nordwest- und Zentralschweiz (EKNZ) in February 2019 along with an amendment to include physicians in April 2022.
The CCSs’ questionnaire consisted of six parts: 1) general information and current follow-up situation, 2) diagnosis and treatment, 3) Cancer Worry Scale (CWS), 4) self-management skill scale (SMSS), 5) adapted expectation scale, and 6) working situation (Supplementary Data S1). We translated the CWS and SMSS developed by Klassen et al. into German and evaluated the applicability in a previous feasibility study.15,16 The scores in the CWS range from 0 to 100, and higher scores indicate lower cancer worries. CCS from the previous ACCS publication and transitioned in the hospital setting were used as comparators for cancer knowledge, CWS, SMSS, and the adapted expectation scale.13,14 To validate cancer knowledge in CCS, one author (MO) performed a medical chart review of all participating CCS and collected information on diagnosis, treatment exposure, and the potential risk for late effects. Organ systems at risk were defined according to the COG LTFU care guidelines V5.0. 7
The questionnaire for physicians consisted of three sections: 1) demographics, 2) caring for CCS, and 3) treatment summary, including information that should be included and preference about a shorter or longer version (Supplementary Data S2). Physicians included family physicians and pediatricians. Based on the information from the hospital records, we only included physicians, where CCS have been transitioned to.
To be included in this study, CCS had to fulfil the following criteria: 1) diagnosed at the University Children’s Hospital Zurich; 2) diagnosed from the year 2000 onward; 3) treatment with chemotherapy, including high-dose chemotherapy, radiotherapy, or surgery, resulting in a risk for late effects according to the COG LTFU guidelines V5.0; 4) aged at least 16 years on May 2022; 5) transitioned to family physician or pediatrician with a completed referral letter documented in the hospital records; and 6) transitioned after December 2014 as per ACCS inclusion criteria. CCS treated with surgery only were excluded. We used STATA for the analysis of the data. To compare CCS who transitioned to family physicians or pediatricians to those who transitioned in the hospital setting, we used Fisher’s exact test for categorical variables and the t-test for continuous variables.
Results
We identified 719 CCS diagnosed after 2000 and aged at least 16 years as of May 2022. At the end, we included 70 CCS. The most frequent reasons for exclusion were end of follow-up care before 2014 (n = 93; 13%), patients referred to the University Children’s Hospital Zurich for second opinion or part of the treatment only (e.g., surgery; n = 89; 12%), and unclear follow-up situation (n = 79; 11%). The response rate of the 70 contacted CCS was 33% (n = 23). The same proportion were nonresponder (34%), and for 17 CCS (24%), no current address was available (Supplementary Fig. S1). We contacted 63 physicians instead of 70 because seven physicians have been allocated more than one CCS. Twenty-eight physicians (44%) could be included, 23 (36%) did not respond, and the remaining (20%) were either retired, could not be reached, did not have time, or thought that they were not eligible for the survey (Supplementary Fig. S2). We received feedback from nine dyads, consisting of CCS and the respective physician (Supplementary Table S1).
Half of the CCS were female (56%) with a median age of 6 years (interquartile range [IQR] 3–9) at diagnosis, 22 years (IQR 21–24) at questionnaire, and a median time since diagnosis of 14 years (IQR 11–19) (Table 1). The median time since transition was 2.8 years (IQR 1.7–4.2; range 0.2–7.6). The median value of the current health status was eight with a range of three to ten, where ten represents CCS very happy with their current health status. Nearly two-thirds of CCS report not being in follow-up care anymore, either because their follow-up visits have been terminated (45%) or because no new follow-up appointment was scheduled (13%). The questionnaire did not further ask by whom the follow-up visits have been terminated. Of those CCS still in follow-up care, most are taken care of by the physician together with organ-specific specialists (22%) (Table 1).
Characteristics Reported by Survivors (n = 23)
Data extracted by author from medical records. IQR, interquartile range.
The cancer knowledge was high. All CCS stated the correct diagnosis except of two CCS, who did not answer the question (Table 1). One CCS did not correctly recall the treatment with chemotherapy and two CCS with surgery and radiotherapy each (Fig. 1a). For organ systems at risk for late effects, the proportion of CCS not sure about their risk ranged from 22% for hearing problems, visual impairment, and impaired memory function, up to 43% for endocrine dysfunction (Fig. 1b). Of CCS, who either confirmed or denied being at risk, CCS overestimated their risk for pulmonary and endocrine dysfunction, hearing impairment, and impaired memory, but underestimated the risk for cardiac dysfunction, impaired bone health, fertility, visual impairment, and secondary malignancies.
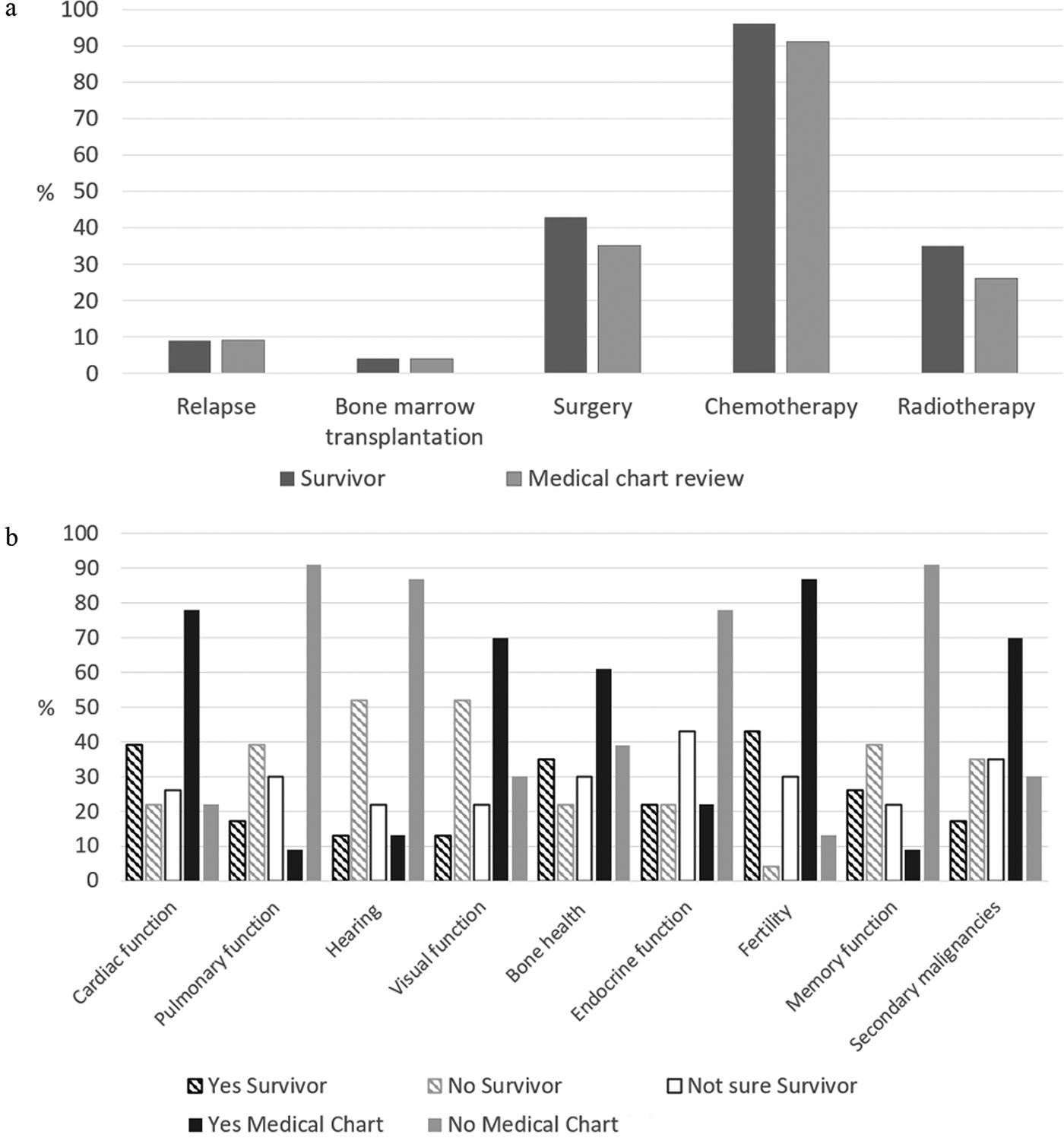
Cancer knowledge.
CCS mainly worried about having children in the future and potential late effects (Fig. 2). The median score of the CWS was 62 (IQR 51–71).

Results from the Cancer Worry Scale (n = 23).
Most of the 14 CCS, who completed the self-management skill scale, show a high degree of independence in 13 of its questions, where at least half of the CCS agreed or strongly agreed to the respective statement (Table 2). Physicians’ knowledge about the cancer history (69%), timely start of the visits (69%), to be seen by the same physician (61%), and to have the opportunity to call the physician in case of questions are aspects important for CCS and expected from the visits (Table 3). For these four aspects and additional four aspects (66%) of the SMSS, the expectations regarding follow-up care visits are fulfilled for at least half of the CCS (Table 4).
Results from the Self-Management Skills Scale
Shaded areas indicate at least 50% agreement with the respective statement (n = 14 [n = 9 with all items missing]).
Results from the Expectation Scale on What Survivors Expect from Follow-Up Care Visits
Shaded areas indicate at least 50% agreement with the respective statement (n = 13 [n = 10 with all items missing]).
Results from the Expectation Scale Regarding Whether the Expectations Are Reality During the Follow-Up Care Visits
Shaded areas indicate at least 50% agreement with the respective statement (n = 13 [n = 10 with all items missing]).
Of the included 28 physicians, slightly more were male (57%), most were aged 51 years and older (89%), with a median of 20 years of working experience. Three quarter (75%) stated that they care for CCS. Of the physicians caring for CCS, 57% see them for acute problems only (Table 5). Three quarter of physicians received some form of information and guidance about LTFU care. This ranged from information on diagnosis, examinations performed, and previous treatment only to referral letters including recommendations for LTFU care and to treatment summaries. Information physicians did not receive, or information they would be interested in, included concrete recommendations for psychosomatic LTFU care (e.g., what needs to be done; list of specialists they could refer the CCS to in case of abnormal findings), long-term prognosis, fertility, late effects, vaccinations, potential interactions in the future, and a contact person for questions. All physicians (n = 28) agreed that a treatment summary is helpful (Table 5). The number of physicians favoring the short version (n = 15) and the extensive version (n = 13) was similar. The main reason for the short version is the time aspect. Except five physicians all stated their interest in receiving some form of education and teaching on the topic of LTFU care (Table 5).
Results from the Physicians (n = 28)
listed answers could have been mentioned more than once. IQR, interquartile range; CCS, childhood cancer survivors.
Discussion
Our study, including 23 CCS and 28 physicians, has revealed two critical aspects—the low proportion of CCS, who consider themselves in follow-up care and more than half of the physicians taking care of CCS for acute problems only.
Less than half of CCS still attend follow-up care might be partially explained by the relatively high proportion of CCS not sure about their risk for late effects. They have either not been informed about their risk or they have been informed orally during the last visit before transition but do not remember the information provided after several years. It is additionally unclear how the CCS have been informed; we do not know if the CCS were addressed directly or just their parents and if the CCS were open for such a discussion at this stage. These are crucial aspects for a successful transition. 17 In the present setting, written treatment summaries were not provided to CCS at this time, and the letters were mainly sent to the physicians only. Being informed about the treatment received and the resulting risk for potential late effects is a well-described facilitator to adherence to LTFU up care, especially during the transition.12,18–20 Not only CCS need to be informed about LTFU care but also physicians. Insufficiently informed physicians in the adult setting are barriers to the attendance to LTFU care.20,21 Uncertainty or lack of knowledge about the reasons for LTFU care may lead to the notion that the consultations are not important; consequently, they are not carried out. It is also likely that the recommended tests are not carried out for the same reasons. That only 43% of physicians see their patients for LTFU care indicates their lack of knowledge about LTFU care and the risk for late effects. Their uncertainties were also expressed in the free text options of the survey (e.g., “Are regular examinations indicated by physicians, which ones?”).
The cancer knowledge and organ systems at risk for late effects were similar between the cohort transitioned to the physicians and those transitioned in the hospital setting. 13 The proportion of CCS unsure about their risk and the organ systems under- and overestimated were similar (Supplementary Fig. S3). This highlights that the education and empowerment of CCS need to be improved in both settings. Comparable results exist for the cancer worries. The degree of cancer worry reflected by the median CWS score was similar between both cohorts (score of 62 in physician cohort, score of 60 in hospital cohort) (Table 1, Supplementary Table S2, Supplementary Fig. S4). However, both psychological worries (“cancer is always at the back of my mind” and “I worry about my cancer every day”) were reported more often by CCS transitioned in the physician setting, indicating a higher psychological burden. Not only receiving information about potential late effects but also the absence of information can cause fears. Fear is a known facilitator to continue LTFU care in the adult setting in some CCS but can be associated with reluctance in others.12,20,22 The relevance of psychological aspects and mental health in CCS is increasingly recognized and led to the formulation of specific screening recommendations. 23
The participating CCS showed a high degree of independence in the self-management skill scale—a facilitator for LTFU care. Independent survivors might be receptive for LTFU care recommendations, but in our study, many seem not to be aware of their need for LTFU care. Loss to follow-up is a well-described issue in cancer survivors.11,24,25 Besides knowledge about the reasons for the visits, also socioeconomic status is an important factor and needs to be addressed during counseling CCS, as this is often linked to the insurance status. Lower socioeconomic status and health insurance issues are barriers to transition and to attend LTFU care visits.12,25–27 Loss to follow-up of CCS may lead to an incorrect perception about current and future health and the miss of potentially treatable late effects in early phases. National concepts must be developed and implemented to guarantee the continuity of care for CCS. All relevant stakeholders need to be part of this process, including pediatric oncologists, adult oncologists, internal medicine specialists or general practitioners, additional medical subspecialties if needed (e.g., cardiologists, endocrinologists, psychologists), CCS, and parents. Our results show that the participating physicians are open to care for CCS and for a respective specific education and training.
The advantage of LTFU care by physician would be the care close to home, a known facilitator for LTFU care. However, as most CCS are young, they have often not yet settled in one place and might relocate due to work or familial circumstances, where they must look for a new physician, most probably not familiar with CCS. At the time of transition, not all CCS have yet developed late effect. This would again be an argument to the transition to the physicians for screening purpose only. In this situation, however, the physician must be aware of the risk for late effects, the increasing burden over time, and what to do if abnormal findings are detected. Even a well-educated CCS can become unsettled if the physician says that screening is no longer needed. In addition, LTFU is an evolving field with updates in recommendations over time. These updates can hardly be guaranteed if only the physician provides care and the CCS are not linked to an expert in LTFU care anymore.
In the United Kingdom, a risk stratification tool was developed to categorize CCS into three levels, based on the cancer type and treatment received. 28 The tool takes three outcomes into account: secondary primary neoplasms, fatal non-neoplastic conditions, and nonfatal non-neoplastic conditions. Patients diagnosed between 1940 and 1991 were included. Nonfatal non-neoplastic conditions were assessed through the British Childhood Cancer Survivor Study and are consequently self-reported. Level 1 includes supported self-management, Level 2 shared care, and Lever 3 a consultant-led care. 28 However, this model does not take cumulative doses of chemotherapeutic agents into account (e.g., anthracyclines as risk factor for cardiotoxicity), relapses, intensive treatment modalities such as high-dose chemotherapy, or complications during treatment.
Independent of the transition model used, CCS need to be well informed, educated, and empowered. CCS loss to follow-up should be informed about the potential risk for late effects, and they all should have the opportunity to receive a specific consultation at a center with expertise in LTFU care. CCS can be reached through campaigns, e.g., by the national childhood cancer organization or survivor group, or by contacting them directly to offer the possibility for a consultation.
Strengths of this study include the comparability of our results with other Swiss cohorts, the inclusion of CCS with a relatively long follow-up with a median of 14 years, and the inclusion of physicians. Limitations include the low response rate in CCS and physicians, resulting in participation bias and results which might not be generalizable. Reasons for the low response rate might be the missing knowledge about this topic and the lengths of the questionnaire in both groups. The feeling, that cancer belongs to the past, reported by other studies, might be a reason specific for CCS. Limited time besides directed patient care could contribute to the low response rate in physicians. Contacting physicians, who received the referral letter, might have resulted in the situation that we contacted the doctor where the CCS no longer goes. The questionnaire-based design might result in recall bias.
Conclusion
Half of CCS transitioned to physicians, including family physicians and pediatricians, qualifying for LTFU care according to current guidelines, are not seen for screening purposes anymore. Education of CCS early on and of physicians is urgently needed as loss to follow-up may lead to lifelong nonengagement and incorrect perceptions about future health.
Footnotes
Acknowledgment
The authors thank all the childhood cancer survivors and physicians who participated in the survey.
Authors’ Contributions
Conceptualization and Methodology: M.O. and K.S. Data curation/analysis: M.O. Roles/Writing—original draft: M.O. Writing—review & editing: M.O., S.K., and K.S.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
Swiss Cancer Research, Grant number:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.