
Abstract
Purpose:
Young adults (YAs) with cancer are a distinct and complex population, yet few interventions exist to meet their unique needs. Sarcomas disproportionately affect YAs, confer a high symptom burden and poor prognosis, and require multidisciplinary management. We sought to improve the delivery of goal-concordant care to YAs with sarcoma; enhance communication among clinicians, patients, and families; provide education around YA-specific needs; and support one another in serving this population.
Methods:
This study was submitted to the institutional review board and determined to be exempt. We established an innovative transdisciplinary collaborative combining medical oncology, palliative care, and social work expertise. We conduct joint visits, normalizing psychosocial and palliative care support and allowing for real-time tailoring of communication. Through iterative assessments, we track symptom trajectories and fluctuations in psychosocial needs, revisiting goals of care alongside clinical transitions. Biweekly rounds facilitate a shared approach to meet patients’ needs. A retrospective chart abstraction identifies rates of contact with our YA team and advanced care planning (ACP) documentation.
Results:
Between 2020 and 2022, our team cared for 56 YAs (median age = 28 years, range = 18–42) with primarily metastatic (76%) sarcomas. Our patients averaged 6 touchpoints with a YA social worker, 8 visits with a YA palliative care provider, and 14 visits with a YA medical oncologist. ACP documentation increased drastically.
Conclusion:
With no additional hospital resources and few workflow modifications, we established a functional transdisciplinary, collaborative team in support of YAs with sarcoma. Our model is both sustainable and adaptable to other cancer types and care settings.
Introduction
Young adults (YAs) with cancer represent a unique and underserved population living in a “donut hole” of cancer care delivery: aged 18–39 at time of cancer diagnosis, 1 they no longer qualify for treatment on pediatric wards but are a stark minority of adults with cancer, comprising less than 5% of adult cancers. 2 In both research and care delivery, YAs are often grouped with their younger counterparts, jointly described as “adolescents and young adults” (AYAs). The National Comprehensive Cancer Network and others have published specific guidance for AYA cancer care, recognizing the unique needs of this population.3–5 Integral to these guidelines are recommendations for early and ongoing support from a palliative care team as well as enhanced psychosocial support to address the added layers of complexity from this transitional stage of life. Although models of care incorporating these guidelines remain in their infancy, several targeted interventions and care delivery approaches have recently emerged,6,7 with a few cancer centers now offering AYA-specific cancer programs to better meet the needs of this population.8,9
However, YAs with cancer are distinct from their adolescent counterparts. 10 YAs have unique disease and symptom features,11–13 lower rates of clinical trial enrollment,14,15 transitional life stages, 16 and insecure support systems (e.g., no longer living in the family home). YAs are often treated in settings (adult medical oncology) with less wrap-around care than in pediatrics; clinicians are less experienced with and thus less comfortable caring for YAs with serious illness. Furthermore, care and communication preferences vary between adolescents and YAs, with YAs more commonly desiring early discussion about end-of-life (EOL) topics and more comfortable discussing death. 17 Models of care for AYAs must recognize this heterogeneity within the AYA population; a one-size-fits-all approach may be insufficient to meet the needs of both adolescents and YAs. Recognizing this dichotomy, we describe the implementation of a YA cancer collaborative team at a NCI comprehensive cancer center comprising members from medical oncology, palliative care, and social work embedded within a dedicated AYA program. The goals of this transdisciplinary collaborative are to improve the quality of cancer care delivery for YAs and to support clinicians and colleagues caring for the YA population.
Methods
Cancer care at academic centers is routinely provided in disciplinary silos. However, treatment for YAs with sarcoma is multimodal and requires multidisciplinary management from providers in oncology, surgery, and radiation oncology. In addition, sarcoma disproportionately affects a younger patient population while conferring a high symptom burden and poor prognosis. To address these needs, we developed a Sarcoma Collaborative, a novel model of transdisciplinary care for YAs with sarcoma. This study was submitted to the institutional review board and determined to be exempt. Here, we describe this model of care and a retrospective chart review with preliminary process outcomes related to care delivery.
The objectives of the Sarcoma Collaborative are as follows:
To provide enhanced, individualized, whole-person cancer care with improved delivery of goal-concordant care from initial diagnosis through survivorship or end-of-life; To increase early advance care planning (ACP) discussions and documentation of goals of care (GOC); To enhance clinician awareness and communication with patients around key YA issues (e.g., fertility, sexuality, substance use, finances, independence); and To increase clinician comfort and satisfaction in caring for YAs with cancer in this important, emotive work.
Eligibility
All patients diagnosed between the ages of 18 and 39 with bone or soft tissue sarcoma at the NC Cancer Hospital and treated in medical oncology are enrolled in the Sarcoma Collaborative, regardless of stage. We elected to include patients with localized disease because (1) this normalizes palliative and psychosocial support for all, building relationships from treatment initiation; (2) treatment for YA sarcoma involves intensive chemotherapy, radiation, and potentially morbid surgeries, substantially impairing quality of life during and after treatment18,19; and (3) many YA sarcomas are highly aggressive, and recurrence is unfortunately common even in those with early-stage disease. 20
Team structure
Our team operates with a transdisciplinary model of care, emphasizing mutual respect among team members and a shared set of goals centered around the provision of holistic, patient-centered care. Our approach involves adaptation to individual patients’ evolving needs and clinical changes 21 and incorporates flexibility and backup behavior when indicated. 22 The composition of our team reflects guidelines that recommend palliative care and psychosocial support alongside medical treatment. We have two dedicated AYA social workers (one clinical, one administrative), a fellowship-trained YA specialist palliative care physician, a medical oncologist specializing in sarcoma, and two nurse navigators in oncology and palliative care. Figure 1 depicts our team structure; Table 1 defines team roles.
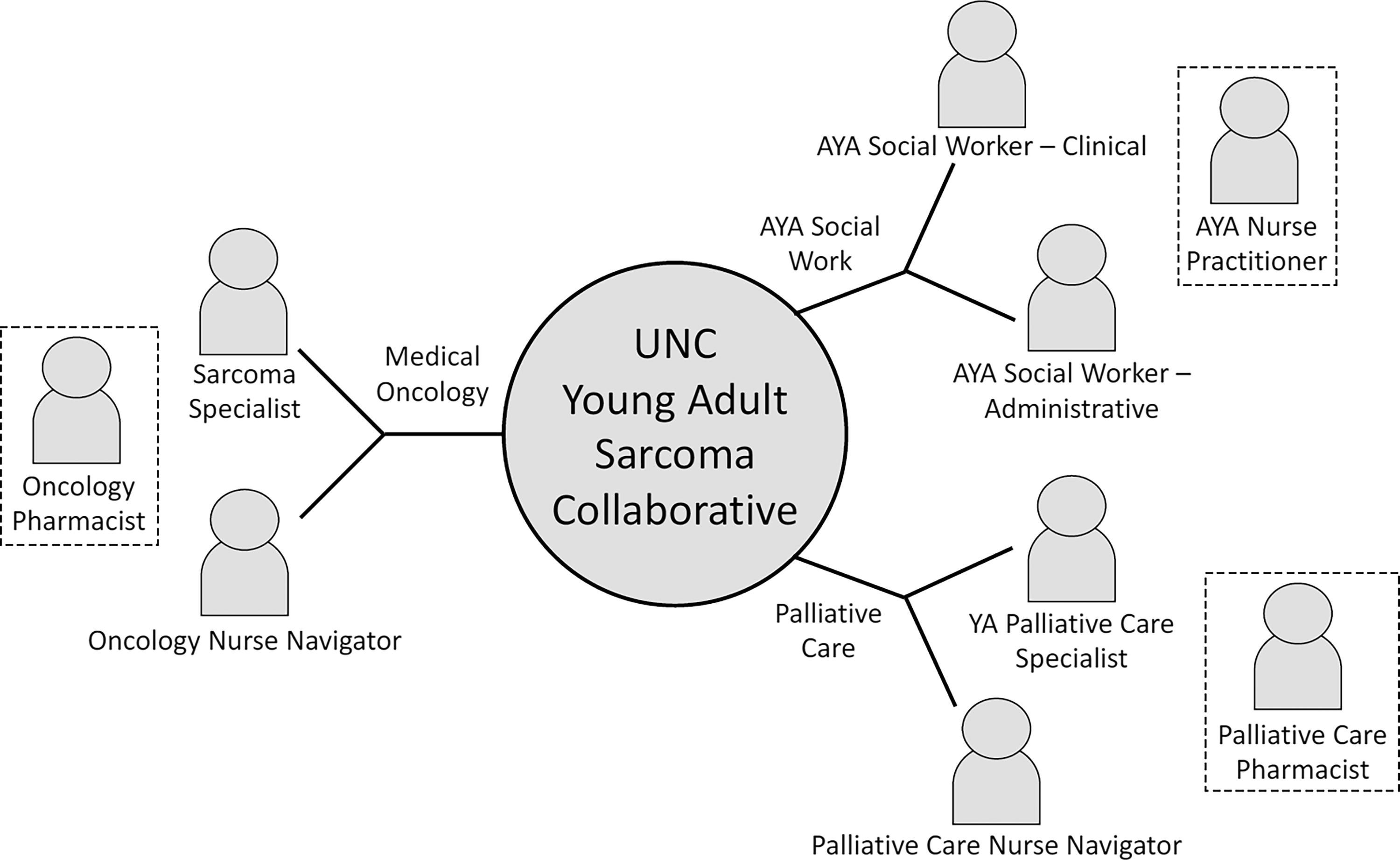
Sarcoma Collaborative team structure. It is a diagram showing the structure of the UNC Young Adult Sarcoma Collaborative, including medical oncology, AYA social work, and palliative care. The branches on the diagram connect to the various roles that comprise the team across these three areas.
Key Characteristics of Transdisciplinary Team
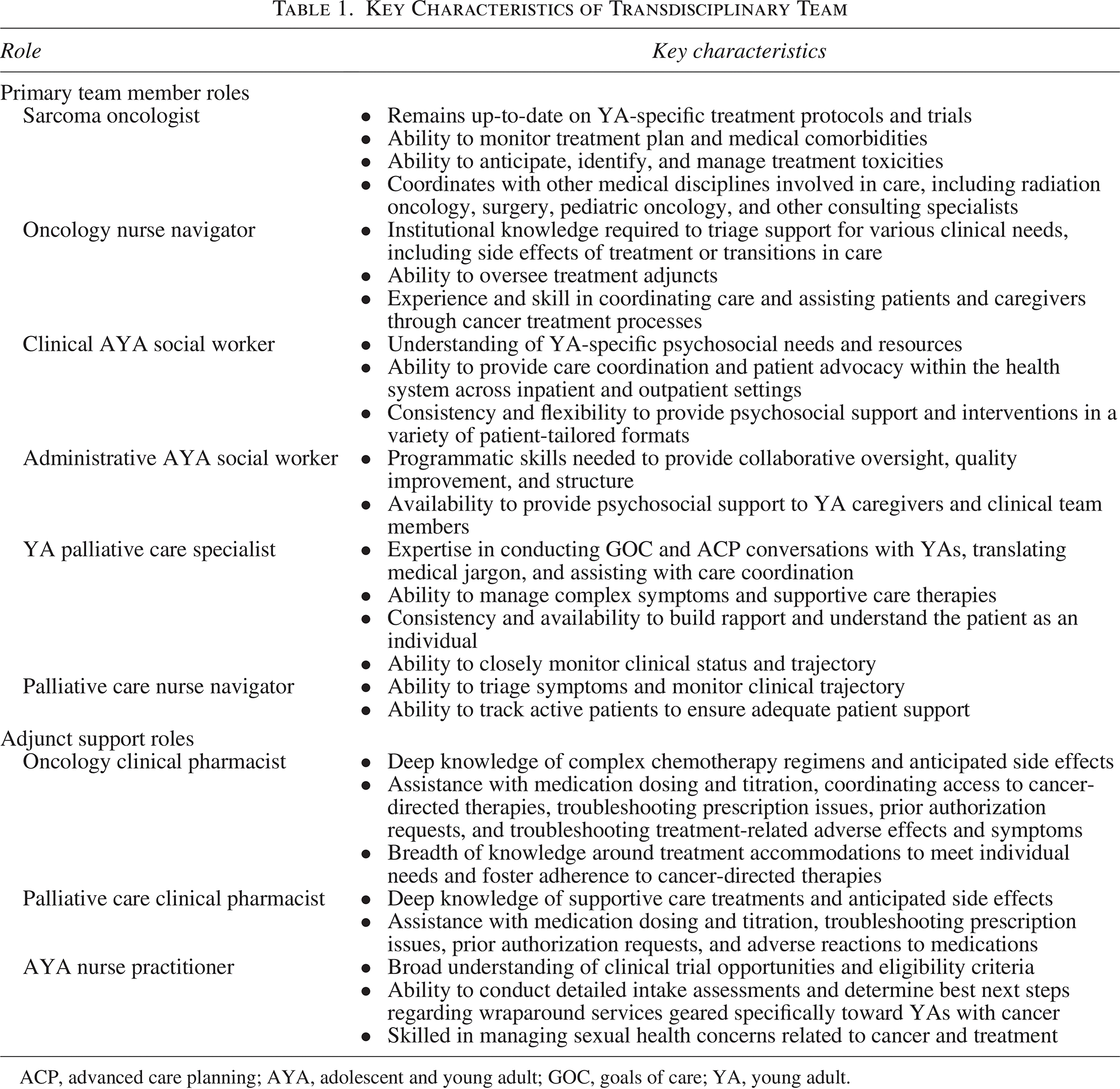
ACP, advanced care planning; AYA, adolescent and young adult; GOC, goals of care; YA, young adult.
Team function
Three key features of our program contribute to its success: joint patient visits, iterative patient assessment, and biweekly team rounds. We also emphasize role flexibility and backup behavior, which has been shown to benefit both teams and patients. 22 Although each team member fills an integral role as described in Table 1, we can shift into each other’s arenas if needed. Furthermore, by presenting the Sarcoma Collaborative as a single, unified team, we make it clear to patients and families that they are being cared for by a team, and we will address their needs by whomever is best suited to do so.
Joint patient visits
We introduce the program and the three main members of our team to new patients by their second clinic visit. We offer joint visits on a regular basis, often every 3–6 weeks, especially at times of potential transition (with new scans and/or decision points). Palliative care and social work visits tend to occur alongside oncology appointments whenever warranted. Separate video and telephone visits are conducted individually or jointly by palliative care and/or social work as needed for continuity, psychosocial support, and complex symptom management. Joint visits ease the burden on the patient to engage in a separate visit and offer more opportunities for clinicians to recognize when topics of discussion require further clarification.
These joint visits are a cornerstone of our program. They allow for a shared understanding among clinicians, YAs, and their caregivers regarding treatment options and implications at each stage of treatment, with multiple team members present to address patient and caregiver concerns holistically. Medical providers gain a deeper understanding of the nuances of YA care from multiple perspectives, advancing our goal of increasing clinicians’ comfort in caring for the YA population. Thus, joint visits enable the provision of integrated, whole-person care to all our YA patients.
Iterative patient assessment
A recurring evaluation of needs and GOC is a critical process given the frequent life changes and varying needs among Yas.
23
Through iterative assessments within each of the following categories, we have successfully addressed a wide range of individual needs and preferences.
Symptom assessment. Fluctuating symptoms related to cancer and toxicity from cancer treatment are particularly challenging for YAs given their dynamic life transitions.
24
A symptom assessment is conducted at every oncology visit and again more thoroughly with palliative care. We tailor management to varying lifestyles, and when symptoms worsen, we can quickly consider creative solutions. Psychosocial needs assessment. Given YAs evolving psychosocial needs, iterative assessment is key, even regarding basic factors such as preferred support person(s) and living situation. Our AYA team is piloting a needs assessment tool that identifies and addresses unmet patient needs
25
; we are exploring opportunities for integrating this tool into the Sarcoma Collaborative. GOC assessment. Iterative GOC assessments account for both symptom burden and changes in psychosocial needs, allowing patients to update their goals (e.g., around treatment options and supportive care services) throughout the course of their illness. Through periodic reassessment, this model shapes a more complete narrative to inform EOL choices better than documentation of a single conversation or hypothetical scenarios.
26
We normalize early and regular discussions around EOL care and decision making. The palliative care provider uses an age-appropriate EOL decision support tool at initial visits, opening the door to early EOL discussions that can evolve over time. These iterative symptom and psychosocial needs assessments can be readily incorporated into a framework for revisiting GOC around routine cancer management planning and EOL. Though true goal-concordant care is difficult to measure,
27
this structure offers a better structure to achieve it.
Biweekly rounds
The final element of our Sarcoma Collaborative is a regular transdisciplinary team meeting. We meet biweekly to discuss patients and review clinical and psychosocial updates. This enables better understanding of our patients as individuals, more nimble and responsive care delivery to evolving circumstances, and psychosocial support for one another in the challenging work of caring for seriously ill young people.
Results
Between January 2020 and December 2022, our team enrolled 56 patients with a variety of sarcoma types (Fig. 2), including desmoid fibromatosis (N = 7), the only non-malignancy. Bone sarcomas (Ewing sarcoma, n = 6 and osteosarcoma, N = 5) comprised one-third of the malignant sarcomas; rhabdomyosarcoma (N = 5) and a variety of non-rhabdomyosarcomatous soft tissue sarcomas (N = 33) made up the remainder of cancer types, most commonly small round cell tumor (N = 4), liposarcoma (N = 4), and round cell sarcoma (N = 4). Demographics are described in Table 2. Ten patients were under age 21 at the time of diagnosis, and the remainder were split relatively evenly between patients in their 20s and 30s, with an overall male predominance and one patient identifying as gender non-binary. Most patients identified as either Black/African American (N = 23) or Caucasian (N = 22), with a smaller proportion (N = 9) in the LatinX community. Many received public insurance (Medicaid, N = 25 or Medicare, N = 7); about one-third (N = 19) received employer-based insurance, with a smaller percentage supported by the military (N = 6) or uninsured (N = 7).
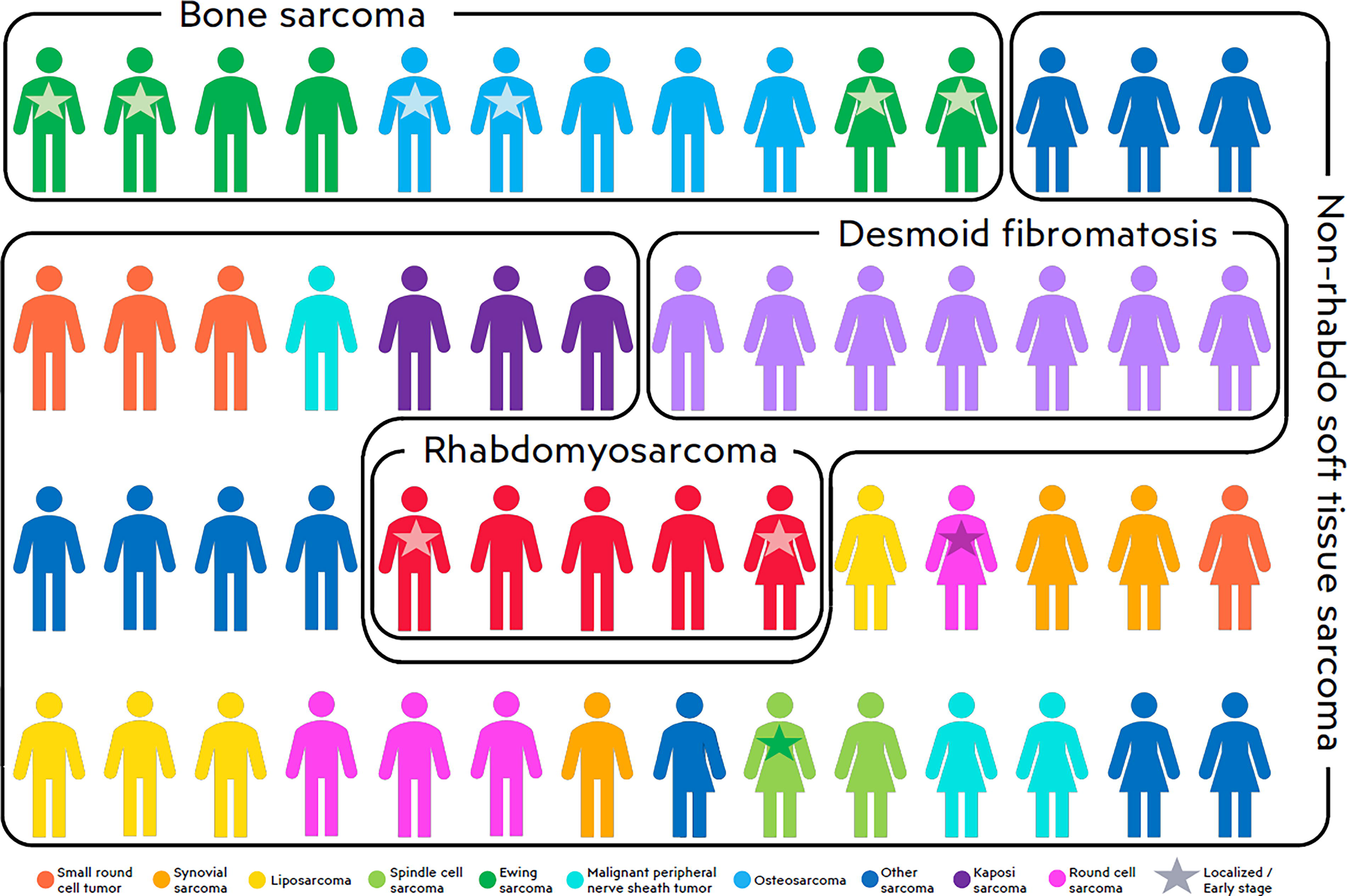
Distribution of cancer diagnoses and stage. It is a diagram showing the distribution of cancer diagnoses and stages the team enrolled between January 2020 and December 2022. The different colors on this diagram correspond with the specific cancer type in the figure legend, and a star indicates localized or early stage.
Patient Demographic Characteristics

Table 3 presents aggregated data on touchpoints with clinicians with and without dedicated YA training and/or engagement with our collaborative team. Among social work visits, 83% were conducted with a clinical social worker with a dedicated YA focus, with an average of 6.4 visits per patient. Similarly, 94% of palliative care visits included a dedicated YA-specializing palliative care physician member of our collaborative team, and we conducted an average of 7.5 palliative care visits. Patients averaged 13.6 visits with a medical oncologist. Visits with a fertility specialist were obtained by approximately a third of patients. Advanced care planning (ACP) notes were nearly non-existent prior to 2020, and by the end of 2022, there were 65 ACP notes, an average of more than 1 per patient.
Visits and Advanced Care Planning Documentation Among YA Collaborative Patients
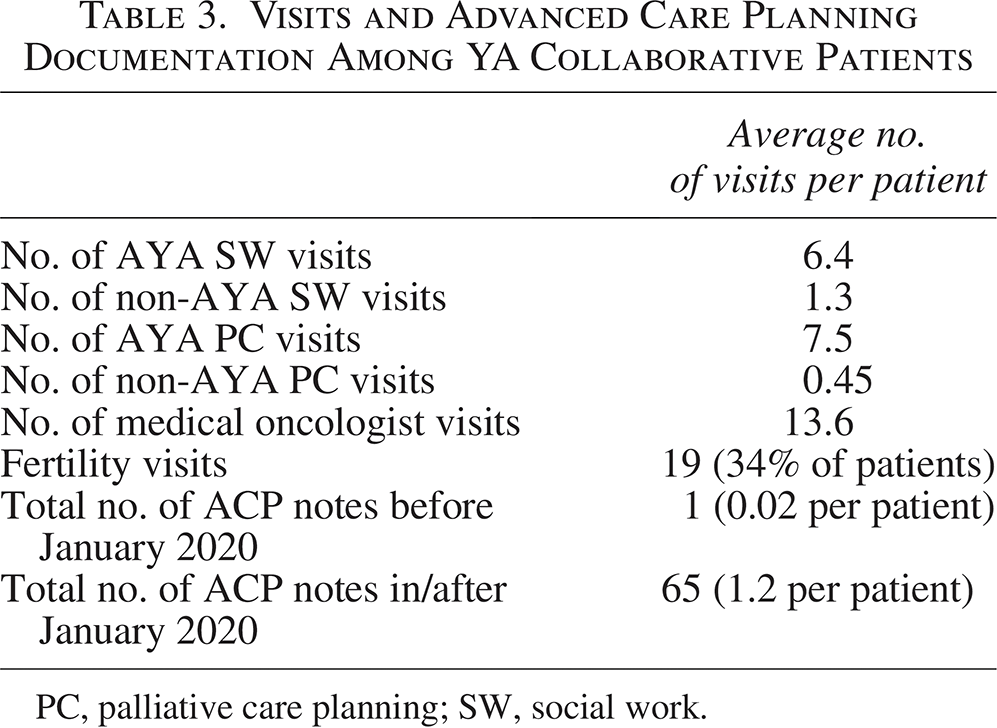
PC, palliative care planning; SW, social work.
Suggested Framework for Implementing a YA-Focused Transdisciplinary Cancer Care Team

The following clinical vignette, a fusion of multiple experiences, illustrates the benefits of our team-based approach to symptom and psychological needs assessments and addressing GOC.
A young man with refractory and metastatic sarcoma was at a treatment crossroads, having progressed through his most recent chemotherapy regimen. He had experienced debilitating early effects of cancer progression and had undergone aggressive intravenous chemotherapy for many months which was quite taxing both physically and emotionally. After a much-needed treatment holiday, we learned that part of the emotional toll was a sense that there would be no breaks in cancer therapy, that he would be on toxic treatments indefinitely until he died. Meanwhile, he had a strong desire to participate more fully in family-oriented responsibilities, which would render him less available for regular hospital visits and multi-day treatments. He was also experiencing worsening waves of intermittent pain episodes that he had difficulty characterizing; he was already taking a moderate dose of gabapentin for peripheral neuropathy, and he was hoping to avoid short-acting medications that would require frequent dosing throughout the day which would interfere with his ability to maintain focus on his family. These insights allowed us to plan for future treatment holidays and recommend a home-based oral cancer regimen as the next course of treatment, as well as a slow introduction and titration of methadone for pain, and he was able to spend more quality time with his family in the supportive role he desired with an informed understanding of potential trade-offs related to anti-cancer efficacy of his oral regimen.
Discussion
Our primary outcomes of interest relate to our team’s ability to collectively care for our patients independently, and we were successful in achieving an overwhelming majority of palliative care and social work touchpoints with dedicated AYA care providers from our team. The primary oncologist met with our patients an average of twice as often as other clinicians, which aligns with our model of ensuring joint visits while promoting regular, dedicated time between patient and oncologist.
From a data standpoint, one limitation of our study is that the time period we examined included preexisting patients as well as patients diagnosed during and throughout the study period, rather than restricting our sample to patients who were diagnosed and completed treatment within the study period. Thus, we may not have captured a complete set of visits for all our patients. Fortunately, the average number of patient visits (with oncologist, palliative care provider, and social worker) collected in this sample is well aligned with our expectations around the care we provide to the patients who enter our collaborative.
A systematic and objective assessment of patient-centered outcomes is planned for the collaborative. Measuring quality of care for YAs with cancer likely differs from both pediatrics and adult oncology, necessitating new measures and more nuanced assessments. Traditional indicators of low-quality cancer care at the EOL, such as intensive care unit stays, chemotherapy administration, and duration of hospice enrollment, may not prove to be as relevant among YAs 28 ; the definition of unnecessary suffering is much more nuanced within this population. Goal-concordant care for YAs with cancer may involve pursuing aggressive care until the final phases of illness, even with complete understanding of the terminal nature of their disease. As an example, a young parent with adequate performance status and organ function may accept high treatment risks with marginal expected benefit given the goal to prolong time with their young children. And someone who is young and able to enjoy a careopen-access life as a retreat from cancer treatment tends to be open to pushing the envelope on aggressive therapies as long as their retreats remain attainable in whatever form is congruent with their functional status. Such goals, preferences, and values can only be fully elicited and supported through ongoing transdisciplinary conversations; and although the associated course of treatment may provide a given young parent with the desired approach to cancer at the EOL, current quality metrics might assess such a scenario as poor-quality care.
Thus, we are tracking the wide range of supportive and clinical activities that our Sarcoma Collaborative performs while qualitatively evaluating patient and caregiver satisfaction with care. This process will enable us to determine the activities that confer the greatest benefit to our patients. Typical measures of care utilization and quality, such as hospitalizations, emergency department visits, provision of supportive care medications, ACP documentation, and hospice enrollment, will assist in characterizing the care needs of our population and where our interventions can contribute. Finally, we are developing a risk stratification algorithm to determine which of our patients are at highest risk for negative experiences with care, which we will pair with targeted interventions to attempt to mitigate that risk.
We believe that this transdisciplinary team-oriented approach (Table 4) will be applicable to other highly complex, nuanced populations spanning the cancer care arena. As we better understand the ways in which the care we deliver can effectively improve patient-centered outcomes, we plan to expand our collaborative model to other common YA cancer types beyond sarcoma, including leukemia, lymphoma, breast, and brain. We also anticipate that a similar model of care may prove beneficial in the pediatric space given the unique needs of adolescents that may not be adequately captured by traditional approaches in pediatric oncology.
We are fortunate at our cancer center to have access to a dedicated team addressing the unique needs of YAs with cancer, and other centers would benefit from implementing a similar program in whatever capacity is feasible. Resources to support such a program must arise from outside the traditional silos of adult and pediatric cancer care or those of hematology versus oncology. They cannot rely solely on measures of clinical productivity given that non-physician effort is critical to the success of this program. In addition, we offer practical steps toward better meeting the needs of this population. Our recommendations for YA-focused cancer care are included in Table 3.
From a sustainability standpoint, it is important to note that this collaboration did not depend on hiring new staff or creating new clinics. Rather, we leveraged preexisting resources within our health system to address what we saw as a critical gap in the clinical care we had been providing. Thus, the model can be readily adapted to other clinical settings with adequate leadership and restructuring of workflows. Our experience suggests that this type of collaborative model may not only enhance the patient experience but also support clinicians in the important work of caring for the young people who fall into the “donut hole” of cancer care, no longer qualifying as pediatric but far removed from the typical adult cancer population. We anticipate that this model of care could be successfully applied to YAs with other cancer types and sustainably adapted to a range of clinical settings.
Authors’ Contributions
J.C., J.S., C.S., S.S., J.H., K.C., V.R., A.S., J.G.-O., and L.L.: Conceptualization, developed the overall research goals and aims, designed the methodology and developed the models or study design. J.C., J.S., D.K., and E.H.: Analysis, performed the data analysis and interpreted the results. J.C., C.S., M.M., A.S., J.G.-O., and L.L.: Writing—Original Draft, prepared the initial draft of the manuscript. J.C.: Created visual representations of the data or conceptual illustrations. All authors Reviewed and edited the manuscript for intellectual content.
Footnotes
Acknowledgments
This work would not have been possible without the generous support of the Be Loud Sophie Foundation. The authors would like to acknowledge the deep honor it is to care for the Sarcoma Collaborative patients and their families, each one unique and very special to them individually and as a team. They are often in awe of their courage and ability to persevere on so many levels and despite profound obstacles.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This work was funded in part through the generous support of the Be Loud Sophie Foundation.