
Abstract
Purpose:
Adolescent and young adult (AYA) cancer survivors (i.e., those diagnosed between the ages of 15 and 39 years) experience significant health and health care disparities. Formal evaluation of the role of community-based organizations in addressing these disparities is limited. Through a novel Health Equity Initiative, which included a series of community-driven conversations), Stupid Cancer, an AYA-focused cancer patient advocacy organization, sought to better understand the perceived impact of racism, homophobia, transphobia, and ableism on supportive cancer care among AYAs.
Methods:
This paper describes how Stupid Cancer developed and implemented its Health Equity Initiative programming (2021–2023) and presents findings from this program. Community-driven conversations comprised of several virtual focus groups, working groups, and town halls conducted via Zoom over the two years. We performed thematic analysis of transcripts from community-driven conversations.
Results:
Three themes were identified from community-driven conversations across initiative events 1) perception, 2) transition, and 3) representation. Based on these findings and further community discussions, four solutions were codeveloped with community members, which serve as proposed mechanisms for addressing identified health care inequities among AYA cancer survivors.
Conclusion:
Inclusivity and representation are vital components of AYA cancer care delivery. More research and quality improvement initiatives are needed to identify community-level interventions to mitigate health care disparities, ensuring all AYAs receive access to high-quality cancer care.
Adolescents and young adults (AYAs; ages 15–39) with cancer face unique risks for health disparities (i.e., preventable differences in opportunities to achieve optimal health) and require tailored solutions toward mitigation.1–3 Disparities are attributable to systematic inequalities in status or power and may be observed in access to health care, disease burden, care quality, and physical and mental health outcomes.1,4,5 Across survivorship, AYAs have poorer health outcomes (e.g., higher rates of obesity, anxiety, depression, and financial hardship).4–6 These disparities often persist post-treatment and are compounded for AYAs from marginalized backgrounds (i.e., Black, Indigenous, or people of color [BIPOC]; nonbinary, lesbian, gay, bisexual, transgender, or queer [LGBTQ+]; and/or with a disability). In addition to higher mortality rates, these patients must navigate medical bias and discrimination, mental distress, and lack of both tailored resources and representation among health care and research teams.11–13 Furthermore, tokenism (i.e., superficial or symbolic means to promoting equity) has intensified the emotional toll of persistent health care inequities.14,15
Stupid Cancer, an AYA-focused advocacy organization based in the United States, responded to a call to action 15 to better understand the impact of racism, homophobia, transphobia, and/or ableism on AYA supportive care. Stupid Cancer planned and implemented a Health Equity Initiative to address and mitigate health disparities among AYA cancer survivors by addressing the experiences of marginalized AYA communities. The purpose of the community-driven conversations was to identify experiences of racism and/or bias in care and develop and implement tools to break those cycles. Herein, we report the development and implementation of Stupid Cancer’s Health Equity Initiative, describe proceedings and findings, and propose solutions.
Methods
Stupid Cancer was founded in 2007 to empower those affected by AYA cancer by ending isolation and building community. 16 The organization is comprised of eight core staff, a Board of Directors, a Scientific Medical Advisory Board, and a Communications Advisory Committee. As of February 2025, Stupid Cancer reached more than 850,000 community members including survivors, caregivers, and AYA professionals across 50 states. Their services include in-person and virtual program offerings and social media resources accessible worldwide and an annual conference, CancerCon, which gathers over 350 attendees annually across the AYA community. 16
This report presents results of the Stupid Cancer Health Equity Initiative, which included a series of focus groups, working groups, and town halls with members of the AYA cancer community who identified as part of a marginalized group based on race/ethnicity, sexual orientation and gender identity, and disability status (Fig. 1). Stupid Cancer staff and members of the medical and community advisory boards provided knowledge and expertise throughout the Initiative. The University of Rochester institutional review board (IRB) deemed this study to be exempt and not require IRB oversight as data shared with researchers were not linked to identifiers and were not considered human subject research.
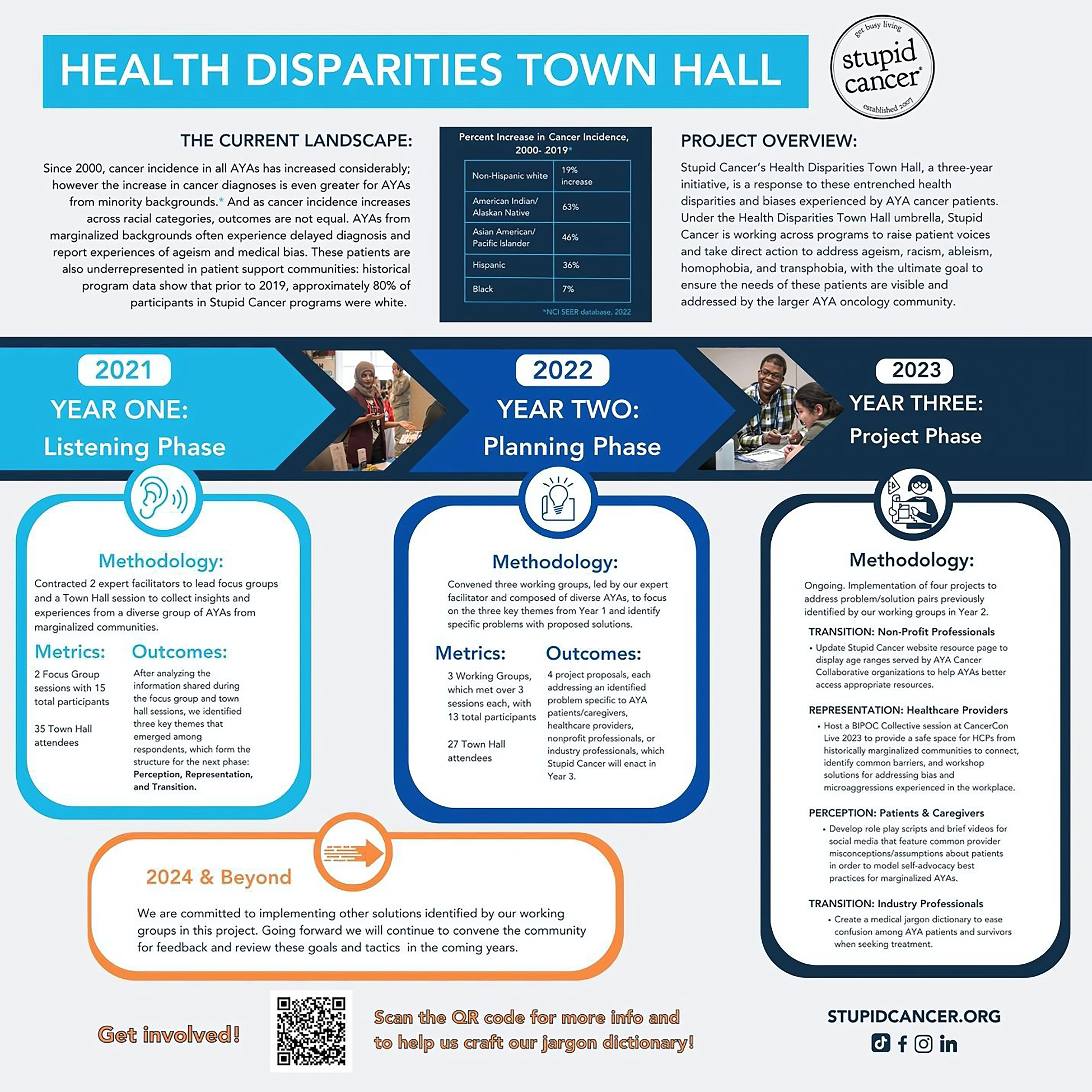
Health Disparities Town Hall summary poster. Note. This poster was presented at the AYA Global Congress in June 2023. The figure captures Years 1 and 2 of the listening and planning phases, which are comprehensively described in the text of the article. Year 3, depicted here, captures the proposed implementation of solutions generated from Year 2. AYA, adolescent and young adult.
Participants and recruitment
Participants included patients/survivors, caregivers, health care providers, and nonprofit professionals. Stupid Cancer community members who self-identified as BIPOC, LGBTQ+, and/or disabled were invited to participate in the Initiative. Recruitment was conducted through social media posts, the Stupid Cancer email listserv, and partnership with peer organizations from October 2021 through January 2024.
Procedures
Participants agreed via email to a Code of Conduct 7 that outlined steps to maintain a safe and productive conversation and to treat participants with respect. All activities (focus groups, working groups, and town halls) were completed online via Zoom, with participant controls (e.g., Participant Chat, Q&A, Raise Hand functions) employed to create a more interactive experience. Participants were compensated $50 for each town hall or focus group attended.
Program planning began April 2021, with a trauma-informed, antiracist lens guiding development and implementation.17,18 Overview of this programming, along with corresponding timing, specific events, program goals, and outcomes, is displayed in Table 1. The purpose of community-driven conversations was to identify points of bias in care and identify solutions. Stupid Cancer staff and two external consultants (D.R. and J.W.) with expertise in emotional intelligence, communication education, and social justice cofacilitated the sessions. In addition, Stupid Cancer’s Scientific Medical Advisory Board provided input throughout program development.
Overview of Stupid Cancer’s Health Equity Initiatives Events, Goals, and Outcomes
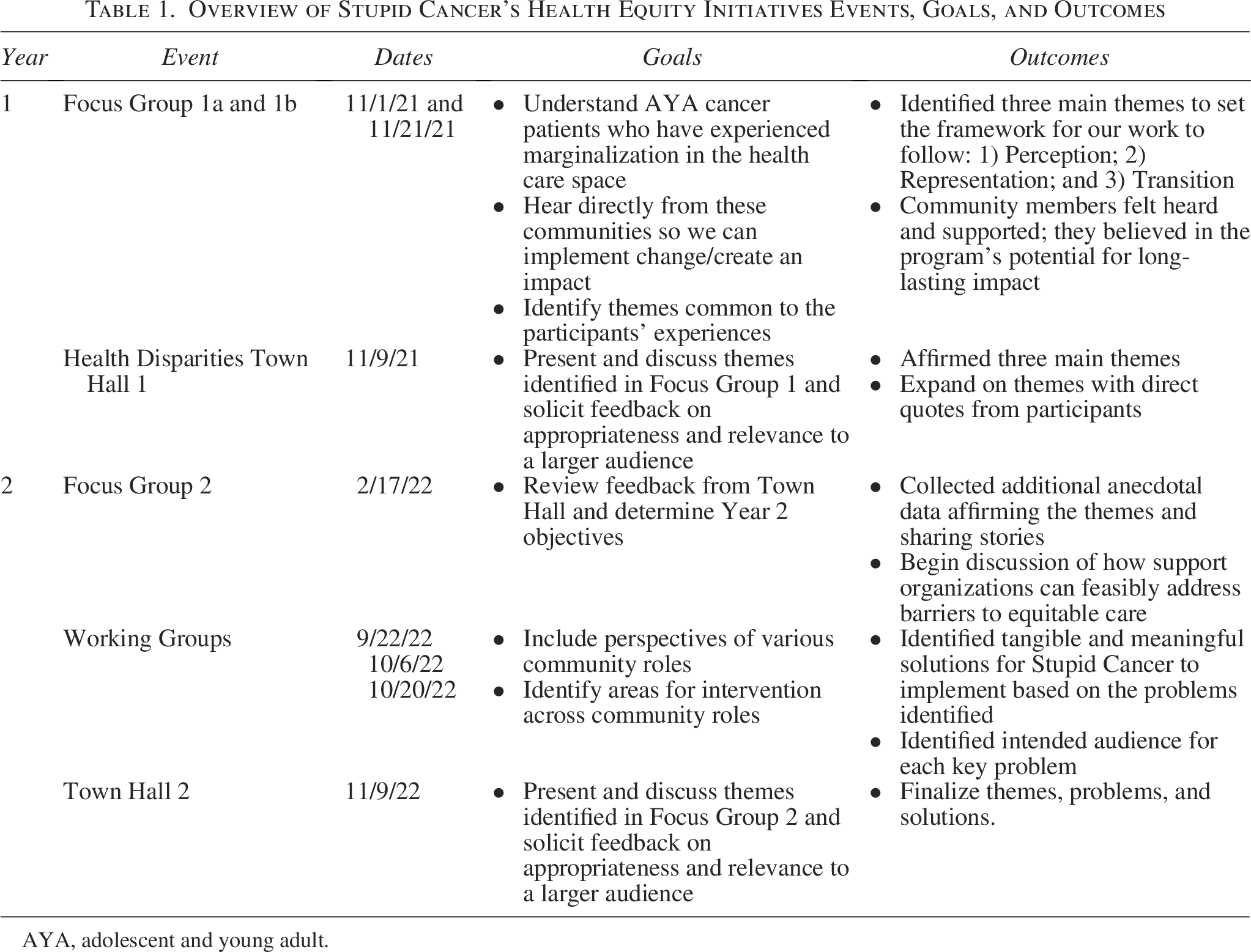
AYA, adolescent and young adult.
Year 1: the listening phase to identify challenges
The first year (2021) was classified as the “Listening Phase” and comprised two focus group sessions and a town hall. Stupid Cancer staff engaged community members who identified as marginalized and/or reported experiencing bias in their cancer care from past Stupid Cancer programming to participate and provide feedback and share personal experiences. Participants (N = 15) were randomly divided between two focus groups (i.e., 7–8 community members per group).
Focus group 1a began with a general discussion of disparities within the AYA cancer experience. A semistructured discussion guide (Supplementary Appendix A1) was used to explore perceived barriers and unmet needs during cancer care including the impact of specific social identities (e.g., “Describe a situation when you felt, as an AYA oncology patient, that you were not getting adequate treatment or access to resources.”).
Themes that were identified in focus group 1a were subsequently presented at the first Health Disparities Town Hall, conducting virtually and moderated live on December 7, 2021. The goal of the town hall was to validate the identified themes and explore how they resonated with the broader community’s experiences. Like the focus group, town hall participants included AYA cancer survivors self-identifying as BIPOC, LGBTQ+, and/or disabled. Participants could submit questions or testimonials ahead of time by email, and these were incorporated into the discussion where appropriate.
To encourage engagement from those unable to join the live Town Hall, questions from the focus group discussion guide (see Supplementary Appendix A1) were put into a Google form survey and shared on Stupid Cancer’s website. Finally, the second focus group (1b) met after the Health Disparities Town Hall to reflect on the conversations, confirm or disconfirm themes, and begin discussions about potential solutions.
Year 2: the planning phase
The second year (2022; referred to the “Planning Phase”) involved three working groups and a second Health Disparities Town Hall. Stupid Cancer staff incorporated results from the few survey responses into working group discussions. During these sessions, which were led by a trained facilitator, participants discussed themes that arose from Year 1, with the goal of further clarifying the nature of challenges along the cancer care continuum and generating potential solutions. In addition to AYA patients, other key stakeholders also participated to offer multidimensional perspectives, including caregivers, industry professionals, health care providers, and nonprofit support organization representatives. Participants were guided in brainstorming solutions that could be applied to each stakeholder category, with the primary intention of generating solutions for Stupid Cancer to implement in the future. Participants were given parameters (e.g., time, funding, and staffing) to encourage feasibility of implementing suggested solutions (Supplementary Appendix A1 for specific resource constraints).
Following these three working groups, Stupid Cancer hosted a second virtual town hall to discuss the findings. Anyone could join, and the town hall was facilitated by an expert facilitator. Participants were invited again to provide feedback via a Google form on other problems and solutions identified but not discussed at the town hall.
Data collection and analysis
Data presented herein were collected by Stupid Cancer over 2 years. Participants completed an online demographic survey when registering to participate in a focus group, working group, or town hall. All programming events were audio recorded via Zoom. Transcripts were generated via otter.ai live transcription, and chat logs were collected. Findings are reported as conference proceedings; accordingly, subject-specific consent was not sought beyond the Code of Conduct agreement.
Qualitative data from focus groups and working groups were characterized using a thematic analysis approach in advance of each town hall. Three Stupid Cancer staff members (A.S., A.A., and C.D.) read each transcript and chat log thoroughly and then jointly extracted general topics through a consensus process in which reviewers identified a recurring concept discussed by participants. A.S. tallied the number of times each topic was discussed, and an initial review of the topics described by AYA community members is shown in Supplementary Appendix A2. The Stupid Cancer team then discussed each topic to refine the definition, determine any overlap among concepts, and make decisions about concept organization (e.g., themes/subthemes). The final themes presented here were selected based on actionability and alignment with Stupid Cancer’s mission, and on feedback from town hall participants, where attendees agreed these themes effectively summarized the main topics and were broad enough to include other identified topics. For example, several of the topics (e.g., ageism, self-advocacy, assumptions) overlapped with the three final themes. Proceedings from both town halls were drawn from staff notes and session transcripts.
Results
Participants
In Year 1, 15 participants engaged in the focus group (i.e., Focus Group 1a and 1b) and 53 in the town hall; in Year 2, 13 participants engaged in the working groups, and 52 engaged in the town hall. Table 2 depicts demographics of the four samples (Year 1 Focus Group; Year 2 Working Group; Year 1 Town Hall; and Year 2 Town Hall). Most participants were female and Black or African American in focus groups; and female and White in working groups and town halls. Across focus groups, 40% identified as LGBTQ+.
Participant Demographics: Focus Groups, Working Groups, and Town Halls

Some participants may have engaged in several multiple events throughout both years (e.g., participating in Y1 Focus Groups, and Y1 Town Hall).
LGBTQIA+, Lesbian, Gay, Bisexual, Transgender, Queer (or Questioning), Intersex, Asexual, and plus.
Disability data and role were not collected for the Town Halls.
Participants were able to select more than one role; Y—year.
Identified key problems
Three themes were identified from the first year of conversation: 1) perception; 2) transition; and 3) representation (Table 3 and Supplementary Appendix A3).
Key Problems Related to AYA Challenges Gathered from Year 1

Perception
AYAs expressed concerns with how they perceived providers viewed them throughout their survivorship. AYAs reported that false assumptions, biases, poor communication, and a lack of respect informed these views. Participants shared their beliefs that health care providers had inaccurate perceptions (that could not be categorized as solely positive or negative) of them based on age, race, gender, sexual orientation, disability status, and/or religion. Because of this, AYAs perceived a delay in their diagnosis and believed discriminatory perceptions from the health care team may have harmed their treatment and access to care and supportive resources.
Patients and health care providers discussed the impact of perceptions on fertility discussions, in particular, based on race and sexual orientation. One oncology social worker discussed her observation of the disparity between fertility discussions and referral for fertility preservation between Black and White patients. Another patient discussed heteronormative assumptions and inappropriate language used during fertility discussions. Some LGBTQ+ AYAs recalled having to “come out” to their health care teams repeatedly, while combating negative assumptions about family planning throughout their care.
Transition
AYAs encountered varying transitory experiences that presented challenges, including going from nonpatient to patient, active treatment to post-treatment survivor, and from young adulthood to middle adulthood. There were challenges with transitioning into and within the health care system; they reported being ill-equipped to navigate health care systems and felt overwhelmed. With each transition, AYAs experienced a lack of support from providers related to their age and stage of development. Participants reported feeling “diminished” by providers because their symptoms were not taken seriously, and/or providers directed conversations to their parents rather themselves. There was a clear overlap in how perceptions and assumptions made by providers impacted patient experiences during these transition periods. For several LGBTQ+ AYAs, the transition to becoming a patient was made worse by providers’ inaccurate assumptions about gender, misuse of language and pronouns regarding sexual orientation and gender identity, and assumptions about support structures. Some participants described the challenge of transitioning as a patient because of systemic biases surrounding race, including minoritized patients’ experiences of late diagnoses and at later staged disease and perceptions of “substandard care.” As AYAs aged into adulthood, they had to learn to navigate health care systems and insurance changes as they aged out of parents’ insurance plans.
Representation
Representation referred to inclusion of diverse groups so that historically marginalized identities were reflected in AYA cancer patients’ providers. AYAs shared their perspectives on the lack of representation among health care providers who were BIPOC, LGBTQ+, or from varying religious affiliations. Patients discussed that lack of representation led to poor cultural awareness, insensitivity, bias, discrimination, and a lack of connection with their health care providers. As one AYA said, “the doctor who was put in charge of my case, before I was diagnosed was just incredible. He was a person of color and came from the same religious background as me. So, we had a bit of that type of connection to really treat me like a person, not a patient.”
Patients and providers discussed the importance of representation in printed/electronic materials and within patient–provider communication and relationship building. As one Black provider stated, “It really does make a difference when it’s coming from you… from someone who looks like them.” Other participants shared the benefit of having a team with whom they could relate, “when I saw when I was having surgery…a bunch of black nurses and Black doctors around me that put me at ease. And I feel like that helped communication a lot.”
Identified solutions
Four solutions were codeveloped in phase II (Table 4). The first aimed to target provider perceptions and assumptions about AYAs that can lead to delayed diagnoses. The group developed an idea to create brief instructional videos for dissemination through social media.
Key Problems and Proposed Solutions Gathered from Working Groups

The second fell under “representation” and also targeted health care providers. Participants wondered if providers from historically marginalized communities might work in psychologically unsafe environments, impacting their ability to serve patients. One solution identified was to host a retreat for these providers to connect, build community, and workshop solutions to address difficulties. The working group identified sessions to include at CancerCon for providers from marginalized communities to network and discuss strategies for addressing psychologically unsafe environments.
The final two solutions fell within “transition,” with the first aimed at nonprofit organization professionals and second at industry professions. One solution was to display age ranges on Stupid Cancer’s website for AYA Cancer Collaborate organizations. Participants believed that this might mitigate some confusion and isolation among AYAs when seeking appropriate resources. The second transition solution was to create a “medical jargon” dictionary to decrease confusion among AYAs when seeking medication, clinical trials, and managing insurance.
In the second Health Disparities Town Hall meeting, the four possible solutions were presented and discussed. Town hall participants reflected on the proposed solutions by sharing ideas to help advance implementation as well as personal narratives. Participants noted the difference in experiences within the large AYA age range, which were often caused by lack of connection and relationships. The discussion amplified the need for greater collaboration across the AYA cancer community.
Discussion
Findings from this initiative highlighted the layered challenges marginalized AYAs face and generated community-driven ideas for solutions. In the first phase, the three themes that emerged as common challenges for BIPOC, LGBTQ+, and/or disabled AYAs who participated in this project (i.e., provider misperceptions, lack of transitional age support, and lack of representation among medical providers) align closely with limited prior work in this space. Studies have highlighted the role of providers’ biases—based on factors including age, race, gender, sexual orientation, disability status, and religion—contributing to health care disparities.19–23 These insights served as a foundation for developing subsequent discussion guides, allowing for deeper understanding of marginalized AYAs experiences and for exploring the complex interplay between age and other marginalized identities.
The second phase of this project identified several patient-centered solutions, including brief instructional videos, health care dictionaries, affinity spaces for health care providers, and instructions for clear communication from AYA organizations. Stupid Cancer has developed, and continues to implement, the four solutions. For example, ABCs of AYAs 8 was launched on Stupid Cancer’s website in 2023 as an ever-evolving resource. Also, a newly updated and clarified resources page addresses many transition challenges unique to AYAs, 9 and novel social media content campaigns have worked to address misperceptions and assumptions of marginalized AYAs. Finally, Stupid Cancer hosted a BIPOC collective space at 2024 CancerCon, which included sessions to learn skills around self-advocacy, and for allies to learn how they can better support BIPOC AYAs. Implementation of these solutions has been done alongside community feedback, and while robust in its codesign, future research should explore the solutions’ feasibility and effectiveness on AYA patient outcomes and cancer care delivery outcomes. There may also be opportunity to enhance dissemination through partnership with academic medical centers, community clinics, and providers to reach AYA patient populations not yet connected to Stupid Cancer. 23 This project is novel in applying AYAs’ lived experiences to generate solutions to challenges minoritized patients encounter. Patients were invited to share their experiences and identify their needs, underscoring the importance of centering patients in collaborations among health care systems, academic institutions, and nonprofit organizations. While issues of racism, ableism, homophobia, and transphobia require large-scale systemic change, this initiative demonstrates how some of AYAs’ concerns may be addressed through simple solutions and resources. 10 We have begun to bring these discussions to broader AYA communities, such as presenting the development of this program at the Global Adolescent and Young Adult Oncology Conference in June 2023 (Fig. 1).
We also recognize that research to mitigate disparities must move beyond prevalence studies to interrogate structural drivers of these disparities, such as discrimination in health care settings, stigma, and limited access to culturally competent care, and that more representative and longitudinal studies are needed. However, this work stands at a critical inflection point. Studying underrepresented and vulnerable populations in cancer research is both an ethical imperative and a scientific necessity to achieve health equity, yet there are challenges (e.g., limitations around sexual orientation and gender identity data collection). Community-engaged research models are even more critical now to build trust and ensure that resources and interventions reflect priorities of populations served. Future research can build on similar community-based participatory research methods for health care provider education. 23 For example, the American Cancer Society’s Project Extensions of Community Health Outcomes brought interdisciplinary teams together for didactic presentations and patient-led consultations that educated health care providers on AYA cancer survivorship. 24
Findings from this project should be considered in the context of our methodological limitations. Data analysis did not include a formal qualitative coding approach; rather, this was a community-driven initiative and was neither formally initiated nor designed as a research study. In addition, while every effort was made to incorporate diverse perspectives of AYAs across minoritized populations, participants were already engaged with Stupid Cancer (or other partner AYA cancer group) in some capacity, and findings may not be generalizable to all AYAs. Finally, implementation of solutions was limited to those that could be feasibly achieved within the time, budget, and staffing considerations of Stupid Cancer. Despite these limitations, this project serves as an important addition to the literature in cancer disparities among AYAs impacted by cancer.
Conclusion
Stupid Cancer developed and led a series of Health Disparity Town Halls, highlighting the unique role community organizations can play in addressing health inequities. Although more research is needed to identify community-level interventions to mitigate disparities, findings from this initiative can help to inform how researchers and health care providers address psychosocial issues AYAs face.
Authors’ Contributions
A.S.: Conceptualization, data curation, investigation, resources, supervision, and writing—review and editing; L.V.G.: Conceptualization, data curation, investigation, resources, supervision, writing—original draft, and writing—review and editing; R.S.: Writing—review and editing; L.M.: Review and editing and resources; J.M.W.: Writing—review and editing; A.M.D.: Writing—review and editing; J.E.S.: Writing—review and editing; C.B.: Conceptualization, writing—original draft, Writing—review and editing, and supervision; B.T.: Writing—original draft, writing—review and editing, and supervision.
Footnotes
Acknowledgments
The authors would like to thank the AYA cancer survivors, and all community members involved in the Health Disparities Town Hall. We would also like to acknowledge Stupid Cancer staff, Chelsea Donahue (C.D.) and Avni Amin (A.A.), for their assistance in data collection, and Denise Rouse (D.R.) for her assistance in facilitating Town Hall sessions.
Author Disclosure Statement
A.S. is the Chief Executive Officer of Stupid Cancer; L.V.G., C.B., and B.T. are on the Scientific Medical Advisory Board of Stupid Cancer. They receive no compensation for their board participation.
Funding Information
L.V.G. was supported by a Patient-Centered Outcomes Research Institute (PCORI) Eugene Washington PCORI Engagement Award (EACB-26540). L.M. was supported in part by the NIH/NCI Cancer Center Support Grant P30 CA008748. A.S. discloses funding for the Health Equity Initiative (focus groups, working groups, Health Disparities Town Hall) from the following: Merck, Genentech, Daiichi Sankyo, Astella, Jazz, Gilead, Exact Sciences, Eisai.