
Abstract
Purpose:
The aim of this study is to understand how adolescent and young adult cancer survivors (AYA-CS) interact with exercise and nutrition information and programs after treatment, to explore their experiences in accessing these supports, and to identify where they perceive gaps to be in their care. This will include the perspectives of both AYA-CS and the health care professionals who deliver these services.
Methods:
A qualitative study using semistructured interviews, undertaken via Zoom. Group 1 consisted of AYA-CS, aged between 15 and 25 years of age at the time of diagnosis who had completed their primary treatment. Group 2 was made up of oncology health care professionals including medical, nursing, and allied health professionals who had a minimum of 2 years’ experience working with AYA cancer patients. Thematic analysis was conducted in an inductive manner to develop themes reflecting the needs and experiences of AYA-CS.
Results:
Eleven AYA-CS and seven health care professionals, from Australia, treated and working across adult and pediatric settings participated in the interviews. The analysis identified three primary themes “The ongoing impacts of a cancer diagnosis,” “age as a critical construct,” and “delivering optimal care.”
Conclusions:
Findings highlight the number of challenges young people face in accessing necessary well-being supports post-treatment, emphasizing the need for individualized exercise and diet interventions. There is a need for health care services to better identify and tailor support for AYA-CS to ensure that their needs are met. Further research is needed to integrate these priorities into clinical practice.
Introduction
Adolescent and young adults (AYA) aged 15–25 who are diagnosed with cancer are recognized in oncology as a unique and vulnerable group, with distinct needs, experiences and challenges that continue long after treatment ends.1,2 A diagnosis of cancer during this life stage can profoundly disrupt critical developmental milestones, affecting not only physical health but also emotional well-being, social relationships, and future aspirations, all of which can hinder a successful transition into adulthood.3–8 Adolescent and young adult cancer survivors (AYA-CS) often face challenges accessing age-appropriate services, which include follow-up care for the long-term physical and psychosocial impacts of their cancer diagnosis and subsequent treatment.2,9 This lack of tailored support leaves many without the resources they need to manage their long-term health and well-being. 9 Consequently, research has demonstrated that AYA-CS are more likely to engage in poor health behaviors, such as low levels of physical activity, diets lacking in fruit and vegetables, smoking, and binge drinking at levels comparable to their peers and siblings.4,10–13 These poor behaviors, particularly insufficient physical activity and poor nutrition, significantly increase the risk of multimorbidity later in life.4,14
There is now substantial evidence that interventions that aim to increase physical activity levels and improve diet quality enhance the long-term physical and psychosocial outcomes for cancer survivors.15–19 AYA cancer clinical guidelines, such as the “optimal care pathway for adolescents and young adults with cancer” also recommend that patients should have access to exercise and nutrition support both during and post-treatment. 3 However, while these guidelines exist, there is significant variability in how they are implemented in practice. For AYA-CS, this issue is particularly critical, as this period is when lifelong habits related to physical activity and dietary habits become established, both in terms of physical development and the acquisition and maintenance of these behaviors across the lifespan. 20 Additionally, it may be an ideal time to intervene for those patients with poor preexisting health habits and harness a “teachable moment” where they are open to lifestyle changes. 21 Despite the potential benefits, little is known about current referral pathways or available programs that promote participation in exercise and nutrition interventions or how young people engage with these supports. Additionally, there is a lack of evidence on the most effective methods for delivering health interventions post-treatment.22,23 AYA-CS struggle to access and navigate health systems, which affects their ability to make informed health decisions and is largely related to the developmental issues they are facing.24,25 Therefore, it is essential to gain insights from young cancer survivors and learn from their experiences on how to deliver optimal survivorship care.
There have been no qualitative studies that have explored the perspectives of Australian AYA-CS and oncology health care professionals regarding exercise and nutrition support after treatment. This gap limits our understanding of engagement, interest, and experience with such programs, along with the factors driving engagement. Therefore, the aim of this study is to understand how AYA-CS interact with exercise and nutrition information and programs after treatment, to explore their experiences in accessing these supports, and to identify where they perceive gaps to be in their care. This will include the perspectives of both AYA-CS and the health care professionals who deliver these services.
Method
Study design
A qualitative study design was implemented using semistructured interviews to elicit AYA-CS experience of accessing exercise and nutrition supports post-treatment along with health care professionals who provide referrals, information, and delivery of these supports. Research procedures and reporting followed the consolidated criteria for reporting qualitative research. 26 The study received ethics approval from the Peter MacCallum Cancer Centre HREC (HREC/89657/PMCC).
Participants
To be eligible to participate, AYA-CS needed to have a diagnosis of cancer between the ages of 15 and 25 years of age and have completed treatment for cancer within the past 5 years. Health care professionals included medical, nursing, or allied health clinicians (Exercise Physiology and Dietetics) with a minimum of 2 years’ experience working in oncology.
Recruitment
AYA-CS were recruited between June and December 2023. AYA participants were identified through a range of sources, including Youth Cancer Advisory Board members from four Australian states, comprising people who had a diagnosis of cancer aged between 15 and 25 years who were emailed an invitation letter to participate in the study; the Leukaemia Foundation monthly newsletter and CANTEEN social media channels (Instagram, Facebook, and Twitter). Health care professionals employed through Youth Cancer Services Australia were sent an email with study information between March and May 2024. AYA-CS and health care professionals interested in the study contacted the principal investigator (A.M.) for further information about the study, discussed the study purpose, reason for participation and if happy to proceed, an online interview was organized via Zoom.
Data collection
The interview was conducted online via Zoom by the principal investigator (A.M.) who is an exercise physiologist and PhD student with experience conducting psychosocial interviews with AYA-CS and health care professionals. Verbal consent was recorded prior to undertaking the semistructured interview. Following consent, initial questions elicited basic demographic and clinical data from the participants. Interviews with AYA-CS and health care professionals were guided by a set of questions developed to retrieve specific information on participants’ attitudes, experiences, information, and knowledge around exercise and nutrition supports post-treatment (Table 1; see Supplementary Data). The interviews were recorded via Zoom and transcribed verbatim. Participants were not provided a copy of the transcript for comment or correction.
Example of the AYA-CS and Health Care Professionals Semistructured Interview Questions

AYA-CS, adolescent and young adult cancer survivors.
Data analysis
Following transcription, any identifying information was removed and de-identified. Thematic analysis was conducted in an inductive manner, to maintain the integrity and closeness of the data to the questions asked. 27 A six-phase process of thematic analysis was conducted. 28 The first interview transcripts were read in full by two authors (A.M. and A.U.), who collaboratively conducted inductive, open coding, with the remaining transcripts coded by A.M. Codes were applied to text and discussed with quotes from the text examined. Discussion took place until the context and meaning were agreed. Codes were grouped into initial themes, which were discussed and named. Data collection and analysis were conducted concurrently, until data saturation was reached.27,28 Coding for AYAs was commenced initially, reflecting the order of interviews, and the coding framework was applied to health care professionals and de-identified quotes have been provided to support this process. The principal investigator and interviewer (A.M.), is an exercise physiologist and PhD candidate and it is important to reflect on how this may have influenced both the approach and interpretation of data. To mitigate potential bias, participants were informed of the interviewer’s background to ensure transparency and minimize perceived conflicts of interest. Throughout data collection and analysis, reflexive practices were employed with A.M. discussing his subjectivity with a second author (A.U.). As an exercise physiologist, A.M. was aware of potential biases and, together with A.U., revisited a select number of recordings. Following this, a reflective discussion took place between A.M. and A.U. to explore these interactions and perspectives between A.M. and study participants, which informed and guided subsequent interviews. Clinical and demographic data were described with means and frequencies. Computing software to manage the data included Microsoft Word and Microsoft Excel.
Results
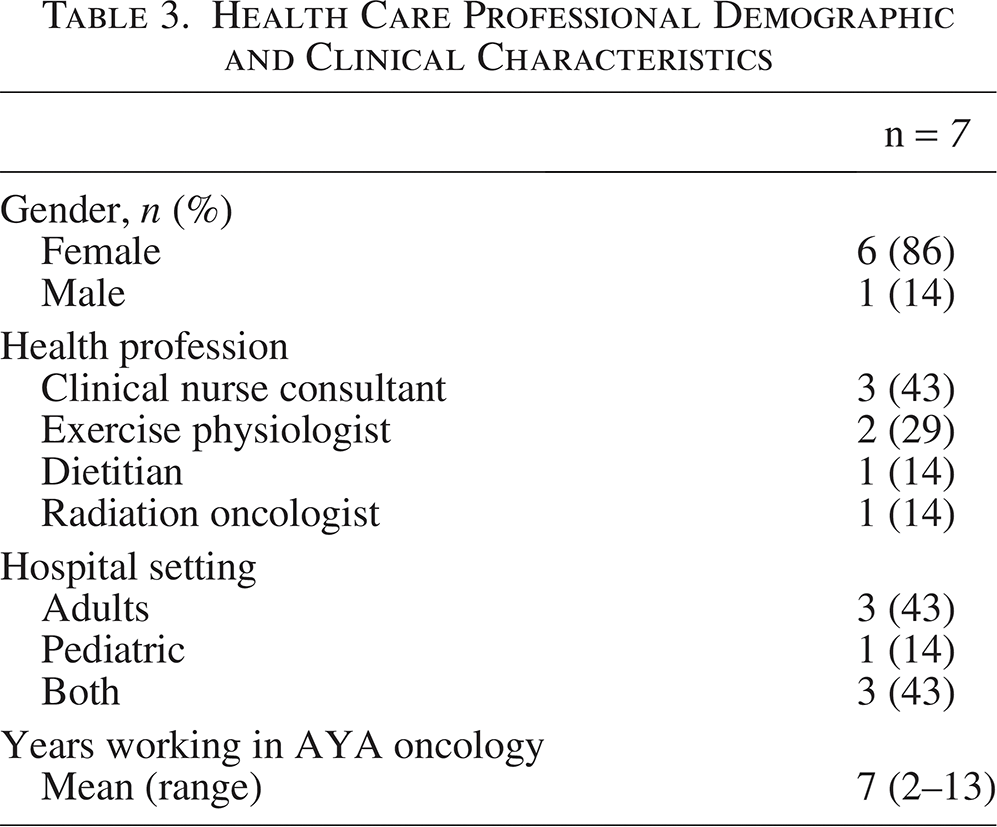
Eleven AYA-CS participated in the interviews with demographic data reported in Table 2. Seven health care professionals were recruited from six different hospitals across Australia, with demographic information presented in Table 3. The mean duration of the interviews was 47 minutes (range: 35–59 minutes) for AYA-CS and 29 minutes (range: 25–34 minutes) for health care professionals.
AYA-CS Participants Demographic and Clinical Characteristics
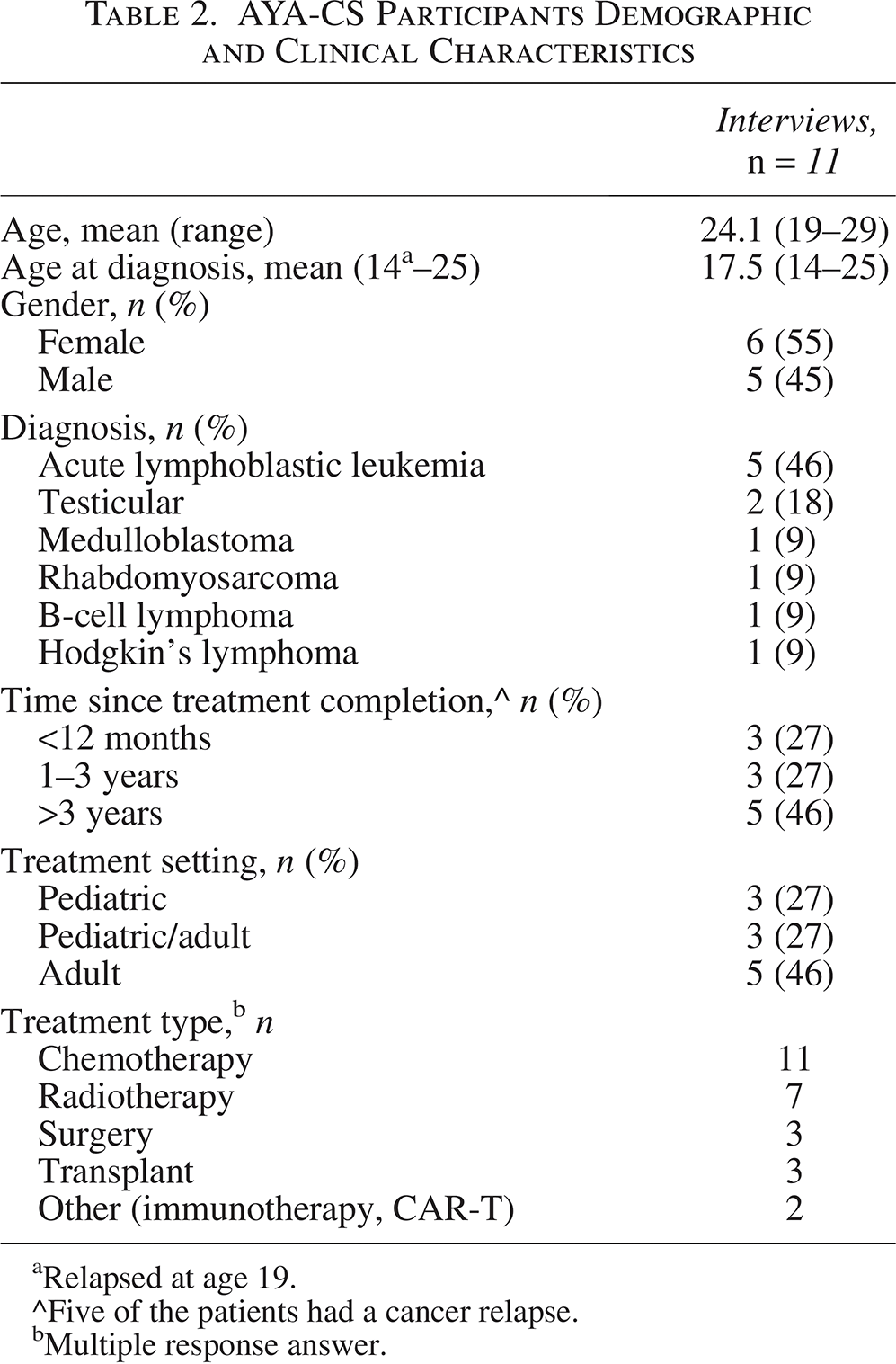
Relapsed at age 19.
^Five of the patients had a cancer relapse.
Multiple response answer.
Health Care Professional Demographic and Clinical Characteristics
Interview themes
Analysis of the interviews identified three primary themes: (1) The ongoing impacts of a diagnosis, (2) age as a critical construct, and (3) delivering optimal care.
The first theme describes the persistent effect of cancer on AYA-CS, both physically and psychosocially, and the enduring influence it has on their ability to manage their overall health and well-being. The second theme highlights the unique needs of AYA as they navigate health, especially in relation to their stage of life development. The final theme identifies the many challenges young people encounter when attempting to access community-based support. It addresses the barriers and facilitators involved and offers insights into the types of programs or supports that could enhance engagement.
The themes are presented in detail below, supported by quotes. Participant numbers represent either young people with cancer (AYA1–AYA11) or health professionals (HP1–HP7).
Theme 1: The ongoing impacts of a diagnosis
All AYA-CS reported at least one example of how the long-term physical impacts of treatment influenced current health behaviors, including physical activity and diet. They spoke to feelings of persistent fatigue, loss of lean muscle mass, musculoskeletal issues, weight gain or loss, and changes in appetite. This had implications for what they were able to do physically and subsequently affected their mental health and sense of self-worth: “But I can’t run, I can’t put any weight on my hips at the moment, I was so healthy, I was so fit … why can’t I just go back to like where I was? I thought I was fat when I didn’t look like the other girls” (AYA1).
Others emphasized the lack of return to normality once treatment had finished and a need for specialized support to address these issues: “I just assumed once I was in remission that I’ll go back to looking and feeling normal. But obviously, that’s not the case” (AYA8). Health care professionals reinforced this: “A lot of them are getting avascular necrosis so they’re very deconditioned” (HP5). Many spoke to the psychological toll of cancer treatment on young individuals: “The battle scars of their cancer diagnosis and how it’s impacted them, whether they be physical changes, emotional changes, some is loss of weight, some is gaining of weight and the hardest thing they struggle with is their physical deconditioning” (HP1).
Some AYA-CS acknowledged that cancer treatment had ongoing negative impacts on their health behaviors. Habits that developed during treatment became ingrained and continued, despite treatment finishing many years ago: “Unfortunately I still struggle in terms of my weight and nutrition, because of the behaviours I developed while undergoing treatment” (AYA7). However, for others, they were aware of the long-term risks of multimorbidity post-treatment and the benefits that exercise, and diet, can provide: “I always wanted to stay on top of my health and fitness, because of a few things like secondary cancer as well as comorbidities. I mean that’s sort of even more important now” (AYA3).
Health care professionals working with AYAs were acutely aware of the importance of fostering lifelong positive health behaviors and their significant impact on health outcomes. Multiple clinicians emphasized the need for skill development when working with young people, equipping them with the skills and knowledge necessary for self-managing their health into the future: “Over the last couple of weeks [of treatment], we educate them on how to write an exercise program and what the benefits are. Then they are given their 12-week exercise program as a resource” (HP4).
Similarly, health care professionals noted their roles in supporting young people affected by cancer: “I guess if you can kind of help empower them when working with them and can at least sort of help develop those skills. Then they kind of get a little more independent, they have the skills to advocate for themselves and provide them with the knowledge of where to go” (HCP3).
Theme 2: Age as a critical construct
AYA also reflected on having cancer as a young person during a critical time of development. There was a sense that cancer interrupted normal developmental tasks, such as learning good health habits (AYA9) “it could be because a lot of my teenage years, I was going through treatment … so I didn’t really set up a good exercise routine” and the subsequent impact it had on their ongoing development. Young people also expressed that they might lack the skills or confidence needed to address concerns with health professionals and seek help, even when they recognized they needed it: “I think as with all teenagers it was hard for me to bring up that I wanted access to some other kind of support even though I knew that I needed it … . it’s a difficult thing to solve, because I don’t know how you kind of give someone support if they don’t necessarily tell you” (AYA11).
A major gap in service provision was the failure to consider age as a developmental factor and address the unique informational needs of AYA-CS in the way information and support were provided. Both AYA-CS and health care professionals noted that age-appropriate resources and services were not open-accessly available or accessible, with a health professional reporting: “Trying to find resources that target their particular age bracket, and what is relevant to them, in the language that they use with familiar faces is a real challenge” (HP7). The written information provided was often not seen as appropriate by AYA-CS: “And I felt the same with the pamphlets. I thought they were very generic and not really meeting my questions … they were not supportive for me at all” (AYA10). When services were available, the environment did not cater to the specific needs of a young person: “I feel like there’s almost a lack of services that provide for young people that actually don’t have as many limitations as say geriatric populations in terms of their fitness and their ability” (AYA5). “You find that the clinics are set up for the older demographic with chronic diseases rather than young people with chronic diseases” (HP3).
A number of AYA-CS also discussed that it was important for health professionals to adapt the way information was communicated and to tailor the guidance, advice, or intervention to meet the needs of the young person: “The physio was just like, oh this is what we normally recommend … we recommend doing this and I was like, but everyone’s needs and goals and outcomes are different and I think that should be a part of the consideration for the advice that’s given” (AYA4). Health care professionals also highlighted the necessity of using various communication methods, such as verbal and written formats, and providing this information on multiple occasions to ensure that patients received and comprehended the essential details: “Multiple dosing, in different ways so not just written or verbal and whatever else at one time-point. But I think survivorship needs to be more than one visit, it needs to be ongoing and at multiple time-points, even if its repetitive” (HP6).
Health care professionals also recognized that developmental age is different from chronological age, and they considered this when providing care for a young person: “It’s such a big period of growth for them and you get a really wide spectrum of presentations where some people might be more in their shell, while others have really found themselves … you really have to be paying attention and noticing what makes them motivated” (HP7). Health care professionals also reported the importance of viewing patients through a developmental lens as part of patient-centered care to allow them to access health services effectively: “I’ll call [an external service provided] on their behalf with consent … I think it’s just about giving them the confidence … when they finish treatment, they want to take control, but they haven’t actually developed the skills to do that. We’ve got to really help them to do that” (HP1).
Theme 3: Delivering optimal care
Many AYA participants reflected that outside of their medical follow-up, other health domains such as physical health and well-being were not addressed. Many AYA reported a sense of falling through the gaps: “Sorting out my diet was something that I have had to do myself” (AYA3). Health professionals held similar views: “You don’t necessarily do anything because you don’t know how to access the correct supports” (HP2).
Young cancer survivors felt that exercise and nutrition support should be available to all and observed that this support was often missing from their care: “I wouldn’t say I got given much information about the nutritional side of things or the exercise side of things in terms of accessing supports” (AYA10). From a clinician’s perspective, when needs were identified, there were either no appropriate services to connect young people to: “And then we’ll talk to them about a healthy diet or exercise, but there are no resources or really referral pathway for it” (HP6); or they lacked confidence in community-based providers to deliver the necessary care: “I struggle referring to people that I don’t trust like that, don’t understand how to work with cancer patients or don’t know the risks of working with cancer survivors” (HP4).
Participants spoke about the benefits of being able to receive the required support when health care professionals were proactive and facilitated referrals to allied health services. They were also more likely to action the referral when placed by a member of their health care team and looked to them to take the lead on this: “For me, referral is the best way, link me in, and then yeah have an action plan” (AYA9). Both AYA-CS and health care professionals highlighted the critical role General Practitioners (GPs) play in promoting sustainable health behaviors and managing the ongoing care needs of AYA-CS. GPs were seen as the person best placed to manage the late effects of cancer treatment, and able to facilitate specialist referrals throughout the survivorship period. “But a lot of the things that benefit AYA in survivorship care, such as diabetes, general health checks, exercise and diet come through the GP and the GP is often best placed to manage these issues. Supporting GPs to provide that care would be beneficial” (HP6).
Participants from both groups identified several critical barriers and facilitators related to accessing exercise and nutrition support. These included financial constraints, waiting lists in the public system, a shortage of specialists, limited service availability, particularly in rural areas along with referral pathways into such programs. “Shortage of specialists including physiotherapists occupational therapists, dietitians and the waitlists are so long … they’ve got public health, and money or finance is a big issue, they have no other choice but to wait” (HP2). Young people were also keen to access health professionals within their local community but would like them to still have specific oncology knowledge: “I want to go to a physio in the community, but I don’t know who is good. I’d like someone who knew my medical history and specialises in oncology” (AYA4).
A major barrier to accessing community-based support for AYA was the financial costs. The costs associated with attending services often made them prohibitive, even though many wanted to attend and believed they would benefit from them during survivorship. Several individuals shared examples of the financial burden of accessing necessary care, such as: “I looked at my bank account last month, and 40% of my spending was on physios” (AYA5). Others were not in a position to access the care they wanted: “Cost is the major barrier for me. I’d love to work with a dietitian and have an exercise physiologist, but I just can’t afford it and can’t justify the expense” (AYA8).
When discussing strategies to improve outcomes for AYA-CS, health care professionals recommended adapting existing care models within hospital settings. They proposed establishing dedicated AYA survivorship clinics or facilitating education sessions that would enable patients to receive comprehensive information and support from multiple health care providers: “I definitely think we should be offering a program periodically through the year, bringing people together with a range of health professionals to discuss patient’s survivorship needs. Patients don’t need or want more clinical follow-up. They want more around lifestyle health and well-being” (HP5). To address challenges related to accessing community-based supports and the associated financial costs, one clinician recommended lobbying the government to enhance support access, similar to what is provided for other chronic health conditions: “It would be great if there was more Medicare based supports or rebates for patients, similar to diabetes, where they can access 10 group exercise classes … more conditions that could fall under that so that people could have even slightly more funded sessions” (HP3).
Young people emphasized the importance of having the right resources and supports that are both convenient and readily accessible: “Even if it just once every year having that information there and being available, because being left to my own devices, I don’t know what is right or wrong” (AYA1). Finally, there was a perception that survivorship care could be more comprehensive and personalized to meet individual needs: “Just more regular comprehensive check-ins post-treatment on all aspects of what we would determine health and wellbeing and then involving whatever allied health is required” (AYA2).
Discussion
Our study explored how AYA-CS engage with exercise and nutrition information and programs following treatment. We sought to identify unmet needs and the barriers and facilitators that influence their engagement with these resources. Key findings highlighted the ongoing health challenges AYA-CS face post-treatment, including difficulties in accessing tailored exercise and nutrition supports, as well as a scarcity of age-appropriate information and resources. Notably, financial toxicity emerged as a significant barrier preventing young people from accessing the support they need to optimize their health and well-being.
This study demonstrated the ongoing impacts of treatment on a young person’s health and well-being, revealing the unique challenges they face in accessing appropriate support. Many participants reported navigating this process without assistance from the health care team, all while dealing with a period of life that coincides with critical stages of physical, social, and emotional development. AYA-CS expressed a clear need for tailored individual exercise and diet support that was age-appropriate. However, referral pathways, information, resources, and programs to address these needs are frequently unavailable. These findings align with previous research, which has highlighted the unmet needs of AYA-CS concerning diet and exercise in the months and years following treatment.11,29,30 Due to the complexity of their challenges, it is essential to provide access to care that addresses both the medical and developmental needs of AYA-CS in order to improve outcomes and quality of life.3,7 Future research should prioritize the creation of care models that promote exercise and nutrition interventions, which are crucial for supporting the long-term health and well-being of AYA-CS during this critical developmental stage.
Considerations for how to support AYA-CS with financial toxicity associated with their cancer diagnosis are necessary. The study found that while young people wanted access to exercise and nutrition supports, the prohibitive cost was a major barrier for many. Financial toxicity is increasingly recognized as a priority, but less research has focused on this in AYA-CS. 31 Addressing financial toxicity requires a multifaceted approach. It involves screening to identify those in need, integrating support systems within health care teams, and providing financial or educational counseling along with assistance programs. 32 More importantly, policy reforms aimed at reducing the economic burden on AYA-CS are crucial for ensuring they thrive in survivorship.
The findings of this study highlight the key areas that require improvement to better support the health and well-being of AYA-CS (Fig. 1). We recommend the development of AYA-specific exercise and nutrition information to create health and well-being information tailored to young people. This information should be appropriate for their developmental stage and be delivered across a variety of accessible platforms, such as websites, mobile apps, social media, and printed materials, to ensure that information is available where and when AYA-CS want to engage, to ensure that all their needs are addressed. Second, providing access to resources that help patients connect with community-based allied health services (i.e., exercise physiology, physiotherapy, dietitians) and educate health professionals on local support options is crucial. Shared care models, referrals, and telehealth can facilitate transitions to community-based support. Third, findings highlight the importance of comprehensive and thorough post-treatment screening to identify risks and health behavior needs. We also recommend developing dedicated clinics within hospitals or services, in early survivorship where young adults are screened, needs are identified and receive the multidisciplinary support that they require. This approach can effectively incorporate the strategies mentioned above and provide pathways to community-based services. Finally, ensuring equitable access to care is crucial. Our results indicate young cancer survivors who receive the care they need tend to be those who have financial resources, strong health literacy, or family support to advocate on their behalf.33,34 Vulnerable groups, such as those from culturally and linguistically diverse backgrounds or low socioeconomic statuses, frequently miss out on the necessary support, with the barriers identified in this study being even more pronounced for these groups.34,35 It is vital to implement systemic mechanisms to guarantee that all young people receive the care they need. By integrating these strategies, young cancer survivors can obtain the personalized and accessible care they need throughout their survivorship journey.
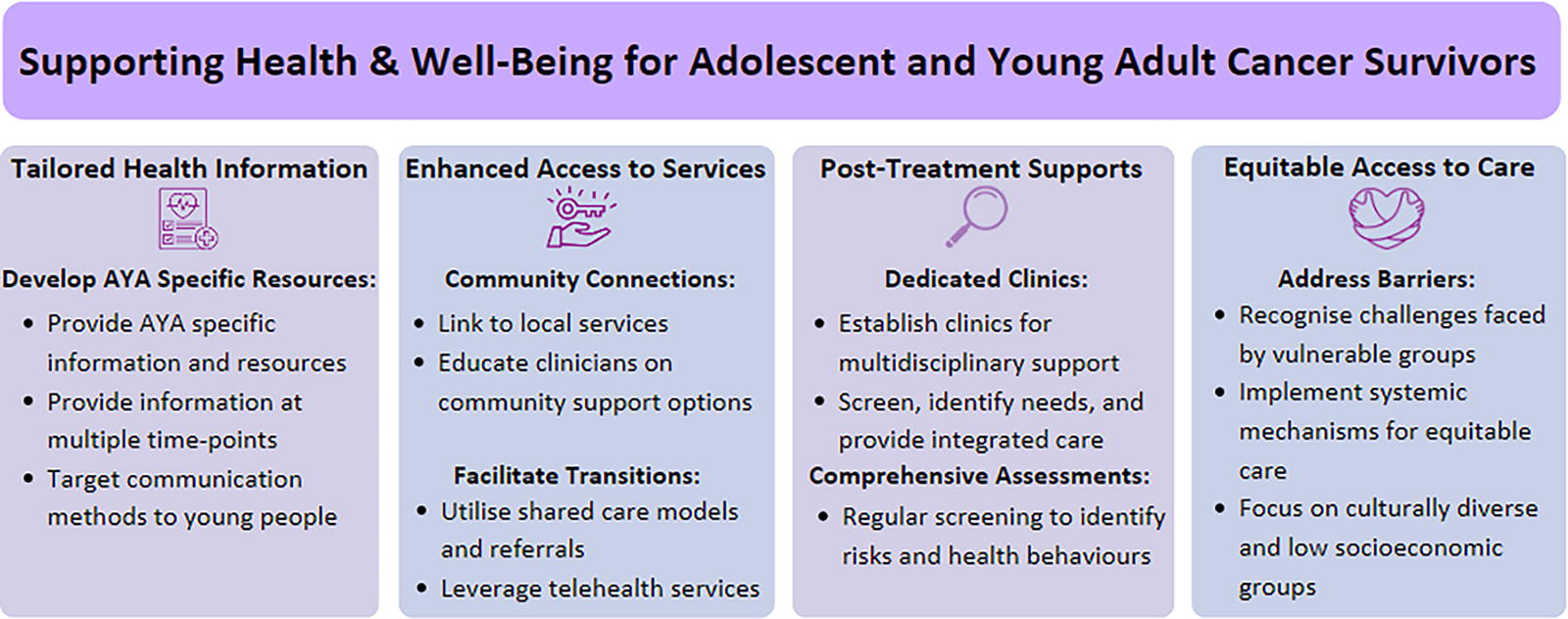
Supporting health and well-being for AYA-CS. AYA-CS, adolescent and young adult cancer survivors.
Strengths and limitations
The current study has several notable strengths and limitations. Among its strengths was the diverse participation of patients and health care professionals from various backgrounds and professions across Australia, encompassing both pediatric and adult health care settings. Including perspectives from both health care professional and AYA-CS during analysis enabled the identification of common barriers and facilitators to accessing exercise and nutrition supports. Limitations of the study include a relatively small sample size and the demographic spread of cancer diagnoses is not reflective of the usual epidemiological spread of AYA cancer. The study design did not incorporate perspectives from primary, community, or regional care providers, all of whom could have offered valuable insights. Furthermore, the generalizability of the results beyond Australia could be constrained due to variations in health care accessibility globally and differences in defining the AYA age range across countries. Future research should also explore the role of family members and caregivers in supporting AYA-CS to access exercise and nutrition support, as their involvement may play a crucial role in post-treatment care. Additionally, a deeper exploration of access to exercise and nutrition services individually may be needed to identify barriers and opportunities for more effective interventions, aiming to improve and tailor post-treatment support for each component of care.
Conclusion
This study offers valuable insights into the ongoing challenges faced by AYA-CS as they navigate post-treatment recovery. It highlights both the persistent impact of cancer treatment on their health and well-being, the numerous difficulties they encounter in accessing appropriate support along with the difficulties faced by health care professionals in managing their physical health and well-being concerns. The findings underscore a clear need for individualized exercise and diet support, which remains largely unavailable, with financial reasons a significant barrier affecting their ability to access the necessary supports. Addressing these issues requires a comprehensive approach that includes enhanced screening to identify needs, integration of support systems within health care teams, and policy reforms aimed at reducing financial burden.
Authors’ Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and transcription were performed by A.M. Analysis was performed by A.M. and A.U. The first draft of the article was written by A.M., and all authors commented on previous versions of the article. All authors read and approved the final article. This study is being used as part of a doctor of philosophy (PhD), which is being undertaken by A.M. through Deakin University.
Footnotes
Acknowledgments
The authors would like to thank the Leukaemia Foundation, CANTEEN, Youth Cancer Services, Australia, and the Youth Cancer Advisory Boards of Victoria & Tasmania, South Australia and Queensland for assistance with study recruitment. The authors would also like to express our gratitude to all the young people and health care professionals who participated in the study.
Author Disclosure Statement
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Funding Information
No funding was received for conducting this study.
Ethics Approval
This study was approved by the Peter MacCallum Cancer Centre Human Research Ethics Committee (approval date: November 17, 2022). HREC reference number (HREC/89657/PMCC) and the local reference number (22/180L). Approval to undertake the study was also received from the Deakin University Human Research Ethics Committee with the local reference number (2022-359). This study was designed, based on knowledge of the literature, and conducted according to globally accepted standards of the Note for Guidance on Good Clinical Practice (CPMP/ICH/135/95) annotated with TGA comments (Australia, July 2000), in agreement with the Declaration of Helsinki (WHO, 2004), the National Statement (Australia, 2007) and in keeping with local regulations and institutional guidelines.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.