
Abstract
Purpose:
No studies regarding embryo freezing as a technique for preserving fertility among patients with cancer have been conducted in Japan. Hence, we surveyed embryologists working at fertility preservation facilities to investigate the current status of embryo freezing for fertility preservation in patients with cancer in Japan.
Methods:
Embryologists from 622 institutions registered for in vitro fertilization and embryo transfer with the Japan Society of Obstetrics and Gynecology were surveyed online about their embryo freezing practices.
Results:
The survey revealed that 352 institutions perform embryo freezing for general assisted reproduction, while only 178 (50.6%) do so for fertility preservation. About 23.0% use different criteria or personnel for cryopreservation based on purpose, 15.2% freeze pronuclear stage embryos, 84.3% freeze cleavage stage embryos, and 92.7% freeze blastocyst stage embryos. All institutions use vitrification, and over 90% follow the manufacturer’s protocol for freezing and thawing.
Conclusions:
Fertility preservation through embryo freezing is not widely used in Japan, and there is inadequate data on the therapy’s current status and results for patients with cancer. Further research is necessary to provide patients with cancer with the opportunity to preserve their fertility without major concerns and ultimately enhance their quality of life after treatment.
Introduction
Recent advances in medical technology have led to significant improvements in the survival rate and life expectancy of patients with cancer, resulting in increased interest in fertility preservation therapy and awareness regarding the psychological impact 1 of initiating cancer treatment after fertility preservation therapy. Moreover, efforts to ensure a high quality of life after cancer treatment have increased. Fertility preservation options for women include freezing of unfertilized egg, embryo, and ovarian tissue. Embryo freezing is a crucial method in assisted reproductive technology (ART). It is considered a well-established treatment, as thawed embryos have implantation rates similar to those of fresh embryos. 2 Therefore, when married women pursue fertility preservation, embryo freezing is the most common method used. In Japan, the incidence of cancer among women of reproductive age 3 is increasing, and the number of patients with cancer who desire embryo freezing for the purpose of fertility preservation is expected to continue to increase.
Embryologists play a major role in ART and cryopreservation techniques. The skill level of embryologists significantly affects the outcome of fertility preservation therapy. However, the present state of embryo freezing for fertility preservation ART in Japan is unclear. For example, the appropriate developmental stages for embryo freezing, freezing and thawing methods, embryo transfer methods after thawing, and culture techniques for patients with cancer are controversial. Therefore, our survey revealed significant regional disparities in access to fertility preservation services, with rural areas having fewer certified facilities and limited access to experienced embryologists. This likely leads to delayed or suboptimal fertility preservation options for patients with cancer in these areas. To address these disparities, it is critical to establish a national network that facilitates the transfer of patients or resources to ensure equal access to fertility preservation services, regardless of geographic location. Previous reports regarding fertility preservation in Japan include a clinical study aimed at establishing clinical application techniques for the cryopreservation of unfertilized eggs that was conducted by the Japan Association of Private Assisted Reproductive Technology Clinics and Laboratories from 2007 to 2015. 4 In 2014, the Japanese Society of Clinical Oncology conducted a survey to formulate clinical practice guidelines for fertility preservation in patients with cancer 5 and reported the actual conditions of fertility preservation in Japan.
Despite the growing need for fertility preservation among patients with cancer, Japan lacks comprehensive data on the current practices and challenges related to embryo freezing for fertility preservation. This study aims to identify key issues such as regional disparities, protocol inconsistencies, and the availability of certified facilities, which are critical for ensuring equitable access to high-quality fertility preservation services across Japan.
Therefore, a survey of embryologists working at fertility preservation facilities throughout Japan was conducted to investigate the current status of embryo freezing for fertility preservation in patients with cancer in Japan and to establish fertility preservation techniques and a medical environment that will enable the provision of uniform and advanced fertility preservation therapies in the 47 prefectures of Japan.
Materials and Method
Study design, participants, and ethics
This study was approved by the Bioethics Committee of St. Marianna University School of Medicine (approval number 5093). The online survey was distributed to 622 facilities that conduct in vitro fertilization (IVF) and embryo transfer and are registered with the Japanese Society of Obstetrics and Gynecology (ART-registered facilities). One embryologist from each participating facility responded to the questionnaire. A letter of invitation and a QR code for the primary survey were sent to the embryology laboratory director or medical department manager of each facility, and the survey was conducted online. Macromill Co. Ltd. (Tokyo, Japan) was commissioned to design the online survey system. The response period was open from February 26, 2021, to March 24, 2021.
Questionnaire
The questionnaire included 21 items regarding the background of the institution, the culture solution and devices used for the cryopreservation of embryos, the freezing method, and the problems encountered while implementing fertility preservation therapy. All respondents provided consent prior to beginning the survey. The survey also allowed respondents to withdraw their consent at any time during the survey. Privacy protection was ensured by setting and managing access restrictions via the assignment of individual identifications and passwords.
Data analysis
This study is based on a survey conducted among embryologists, and the results were analyzed using descriptive statistics only. Since the data represent responses from institutions rather than individual patient outcomes, no inferential statistical analyses were performed. The responses were aggregated and presented as proportions and frequencies. Given the nature of this study, hypothesis testing and statistical comparisons between groups were not conducted.
Survey design and limitations
The questionnaire was designed to broadly capture variations in embryo freezing procedures for both general ART patients and patients with cancer. While the survey did not include separate detailed questions on specific freezing strategies for patients with cancer(e.g., choice of freezing stage at day 3 or day 5, grouping of embryos by grade), the responses provided insights into general trends and practices. Some facilities reported modifying embryo selection criteria and freezing protocols, which indirectly reflects differences in clinical strategies.
In addition, one of the survey questions addressed difficulties in implementing embryo cryopreservation for patients with cancer. The response options focused on challenges related to the management and logistics of cryopreservation, including frozen embryo management, criteria for freezing, patient contact, and storage space. This question was designed to capture facility management issues rather than technical difficulties in cell culture. Therefore, challenges specifically related to embryo culture processes, such as culture media selection or embryo development patterns for patients with cancer, were not included in this survey.
Furthermore, the questionnaire did not include specific items regarding the frequency of oncofertility service provision, the rate of treatment cycle cancellations, or the clinical difficulties encountered during fertility preservation. These aspects were considered beyond the primary scope of this study, which aimed to assess institutional policies and technical practices. However, these are important components of real-world practice and should be explored in future investigations to achieve a more comprehensive understanding of fertility preservation in patients with cancer.
Validation of survey content
The questionnaire used in this study was designed and reviewed by experts in reproductive medicine and oncofertility. The members involved in this survey include physicians and embryologists who have been engaged in IVF treatment in Japan for many years and have extensive experience in reproductive and oncofertility medicine. Their expertise ensured that the survey content was relevant, accurate, and reflective of current clinical practices.
In addition, the survey questions were formulated by incorporating clinical experience and expert opinions. Before conducting the survey, the content was shared with embryologists and physicians to assess its applicability in real clinical settings. This approach ensured the validity of the survey.
Results
General statistics
A total of 352 Japan Society of Obstetrics and Gynecology ART-registered institutions responded to the survey (response rate: 56.6%). All responding institutions (100%) reported performing embryo freezing for general patients undergoing ART. However, only 50.6% (178/352) of institutions reported performing embryo freezing for the purpose of preserving fertility in patients with cancer (Fig. 1). Of the institutions performing embryo freezing for the purpose of fertility preservation for patients with cancer, 83.7% (149/178) were certified by the Japan Society of Obstetrics and Gynecology as facilities for fertility preservation therapy.
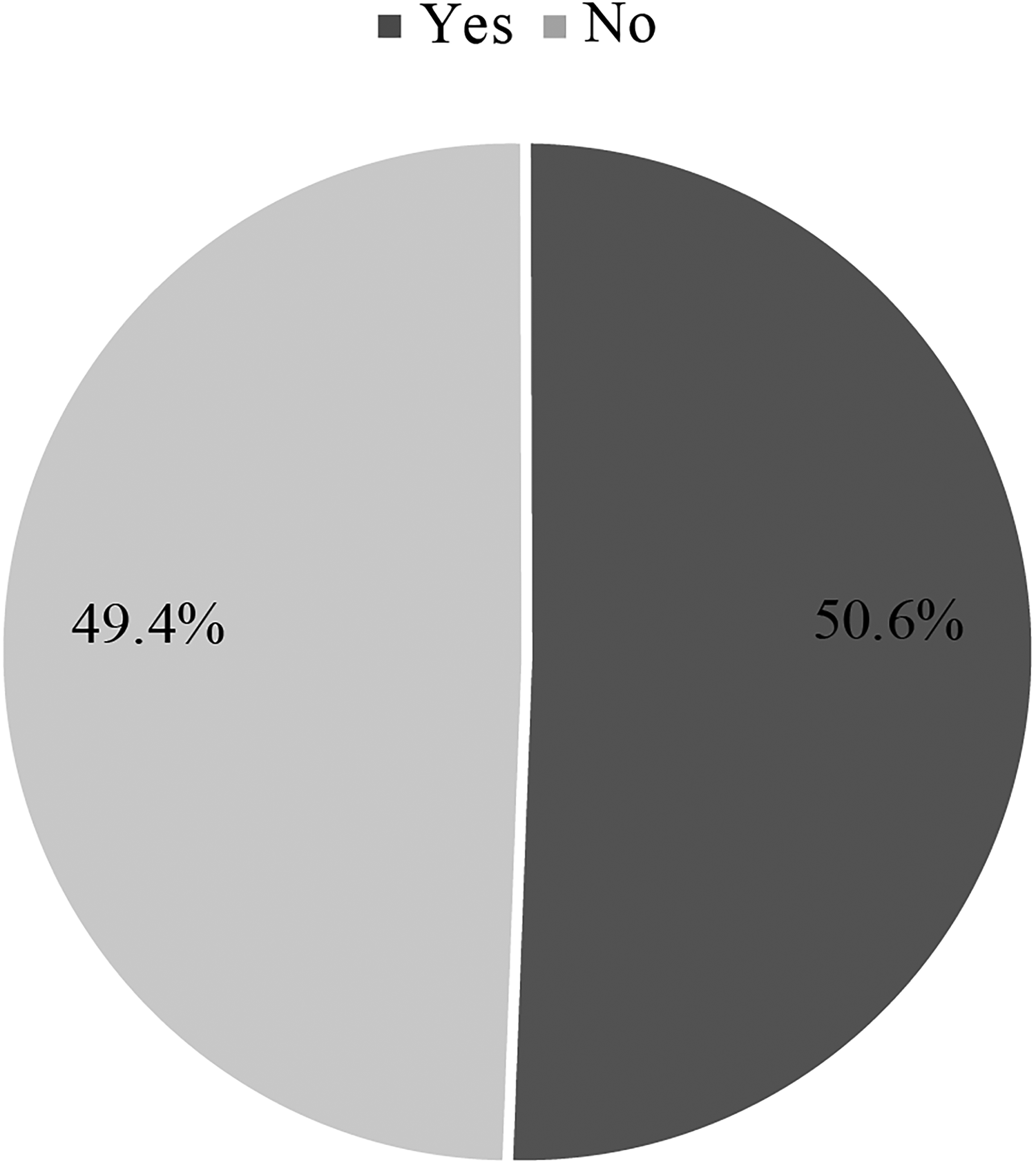
A pie chart depicting the responses to the question “Do you perform embryo freezing for patients with cancer?”
Target age for embryo cryopreservation
The target age for embryo cryopreservation for patients with cancer was restricted by 54.8% of institutions (91/166), including 58.2% (53/91) with an upper limit and 41.8% (38/91) with both upper and lower age limits (Fig. 2). The median upper limit was 45 years (range: 39–50 years), and the median lower limit was 16 years (range: 0–20 years).
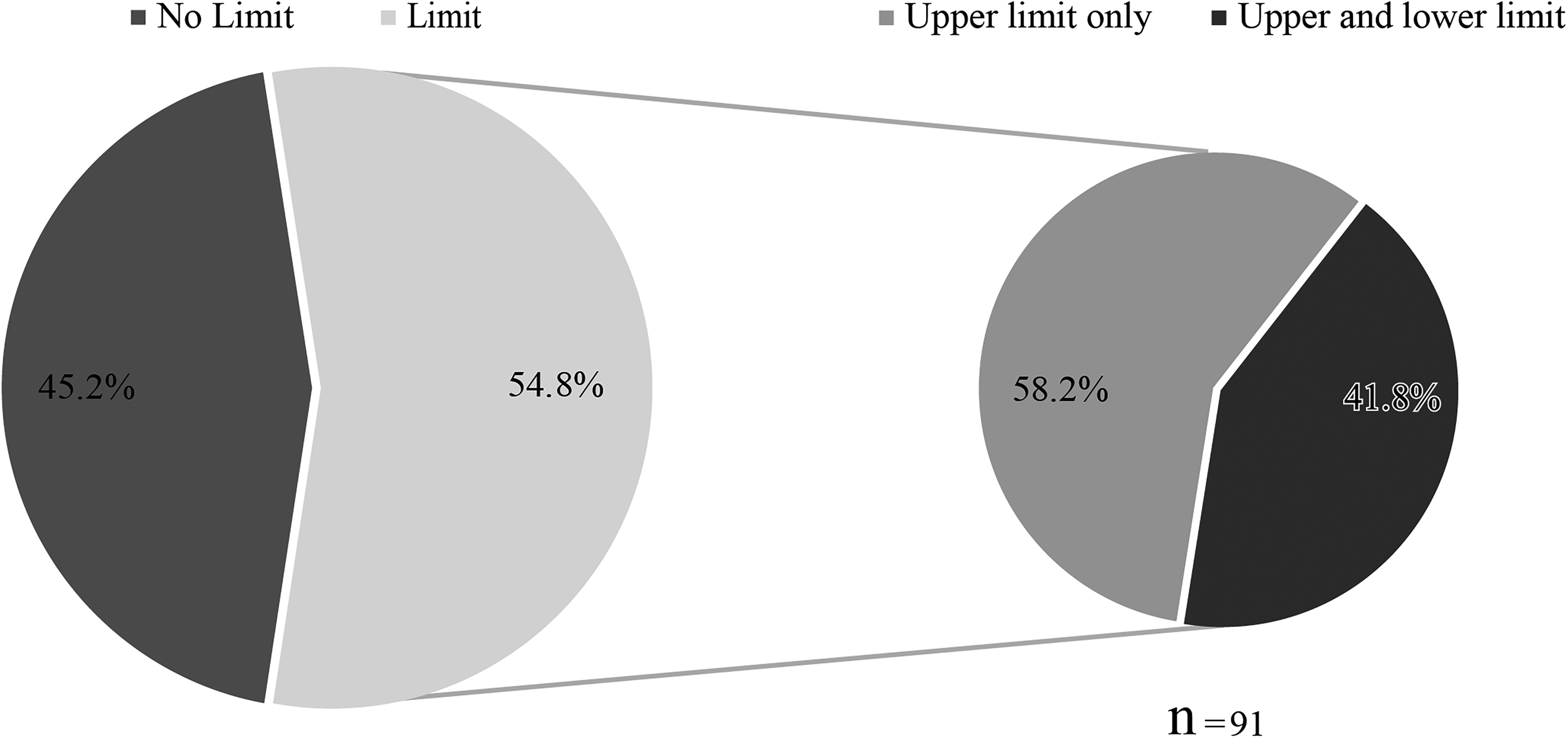
A pie chart depicting the responses to the question “Are there any restrictions on patient age for embryo freezing procedures for fertility preservation therapy at your institution?”
Modifications for patients with cancer
Forty-one institutions (23.0%) reported using an embryo freezing method that differed from that used for general patients undergoing ART (Fig. 3), including 31 (75.6%) that reported lowering the grade of the embryos to be frozen and cryopreserving more embryos; 14 (34.1%) that reported assigning more experienced embryologists for patients with cancer undergoing embryo freezing; and 9 (22.0%) that reported actively implementing split intracytoplasmic sperm injection (ICSI), a combination of conventional IVF and ICSI during the same cycle, to obtain more embryos based on the risk of nonfertilization when conventional IVF was conducted (Fig. 4).

A pie chart depicting the responses to the question “Are you changing anything about embryo freezing procedures for patients with cancer and patients undergoing ART?”

A bar graph depicting the responses to the question “If you answered ‘yes’ to the question about the changes in embryo freezing for patients with cancer and other patients, what did you do differently? (Multiple responses allowed).”
Number of embryologists
Most institutions (79.2%; 141/178) employed five or fewer embryologists who were capable of freezing and thawing embryos for patients with cancer. Twenty-eight institutions (15.7%) employed 6–10 capable embryologists, three (1.7%) employed 11–15, four (2.2%) employed 16–20, and two (1.1%) employed 21 or more (Fig. 5).
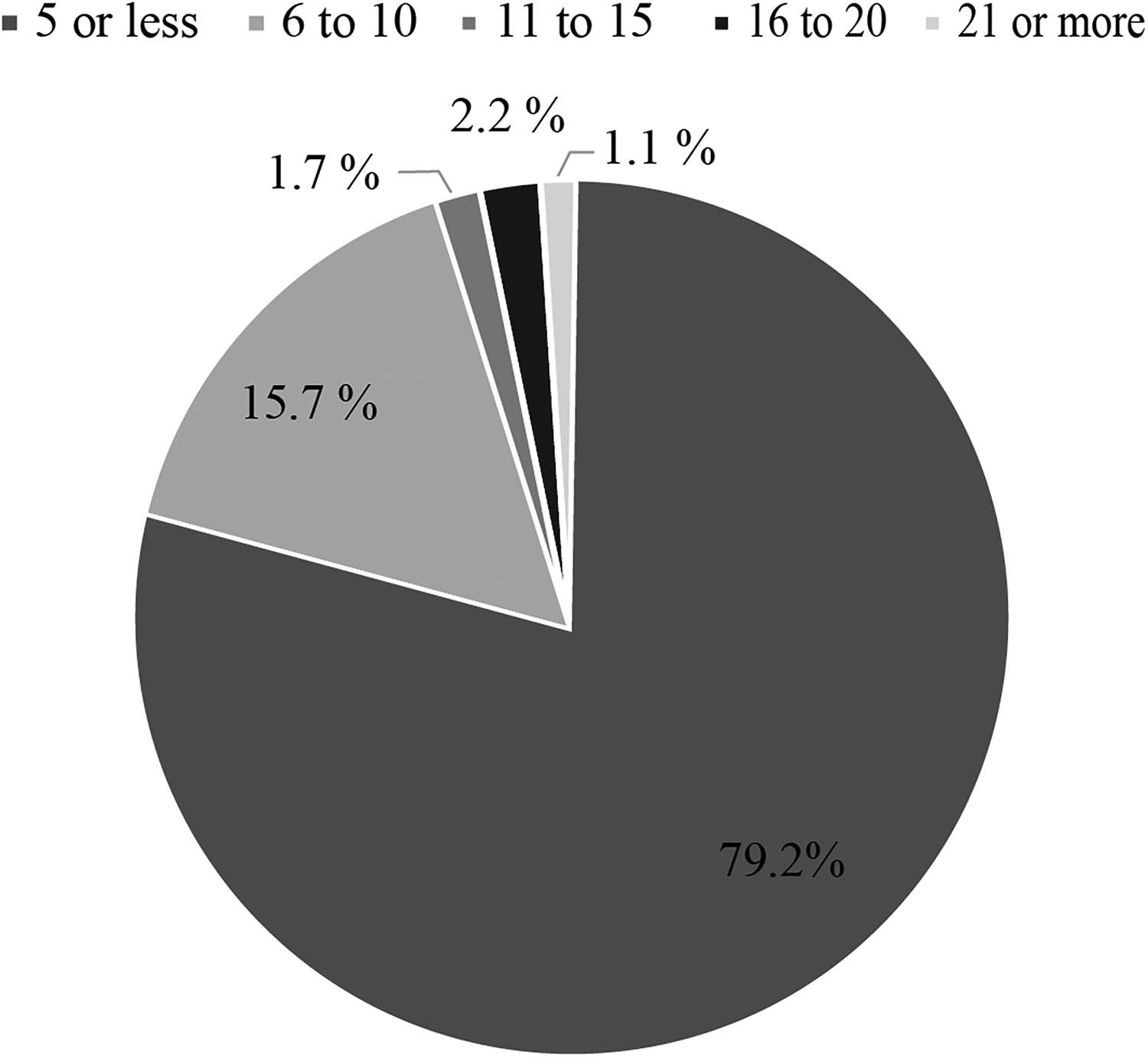
A pie chart depicting the responses to the question “How many embryologists are available to perform embryo freezing for patients with cancer?”
Developmental stage at which the embryo was frozen
The developmental stage at which the embryo was frozen was the pronuclear stage at 15.2% (27/178) of institutions, the cleavage stage at 84.3% (150/178), and the blastocyst stage at 92.7% (165/178) (Fig. 6).

A bar graph depicting the responses to the question “What is the developmental stage of frozen embryos for patients with cancer? (Multiple answers allowed).”
Embryo freezing methods and devices
All 178 institutions (100%) reported using the vitrification method, and one institution (0.6%) reported using the slow-freezing method. The majority of institutions reported using cryopreservation devices from Company A (87.1%; 155/178), while 3.4% (6/178) used devices from Company B, 23.0% (41/178) from Company C, and 0.6% (1/178) from Company D. Two institutions (1.1%) reported using homemade cryopreservation devices, and one (0.6%) used devices from another source (Fig. 7). Most institutions (89.3%; 159/178) reported using an open-type device, 6.2% (11/178) reported using a closed-type device, and 3.9% (7/178) reported using open- and closed-type devices. The type of device was unknown or not reported in one institution (0.6%) (Fig. 8). In addition, most institutions (83.7%; 149/178) reported using cryopreservation solution from Company A, 0.6% (1/178) from Company B, 22.5% (40/178) from Company C, and 5.1% (9/178) from Company D. Five institutions (2.8%) reported using homemade cryopreservation solution (Fig. 9). Most institutions (81.5%; 145/178) reported using thawing solution from Company A, 0.6% (1/178) from Company B, 21.9% (39/178) from Company C, and 5.6% (10/178) from Company D. Seven institutions (3.9%) reported using homemade thawing solution, and one institution (0.6%) used thawing solution obtained from another source (Fig. 10).

A bar graph depicting the responses to the question “What cryopreservation devices are used in the vitrification method? (Multiple answers allowed).”

A pie chart depicting the “Type of device used for cryopreservation.”
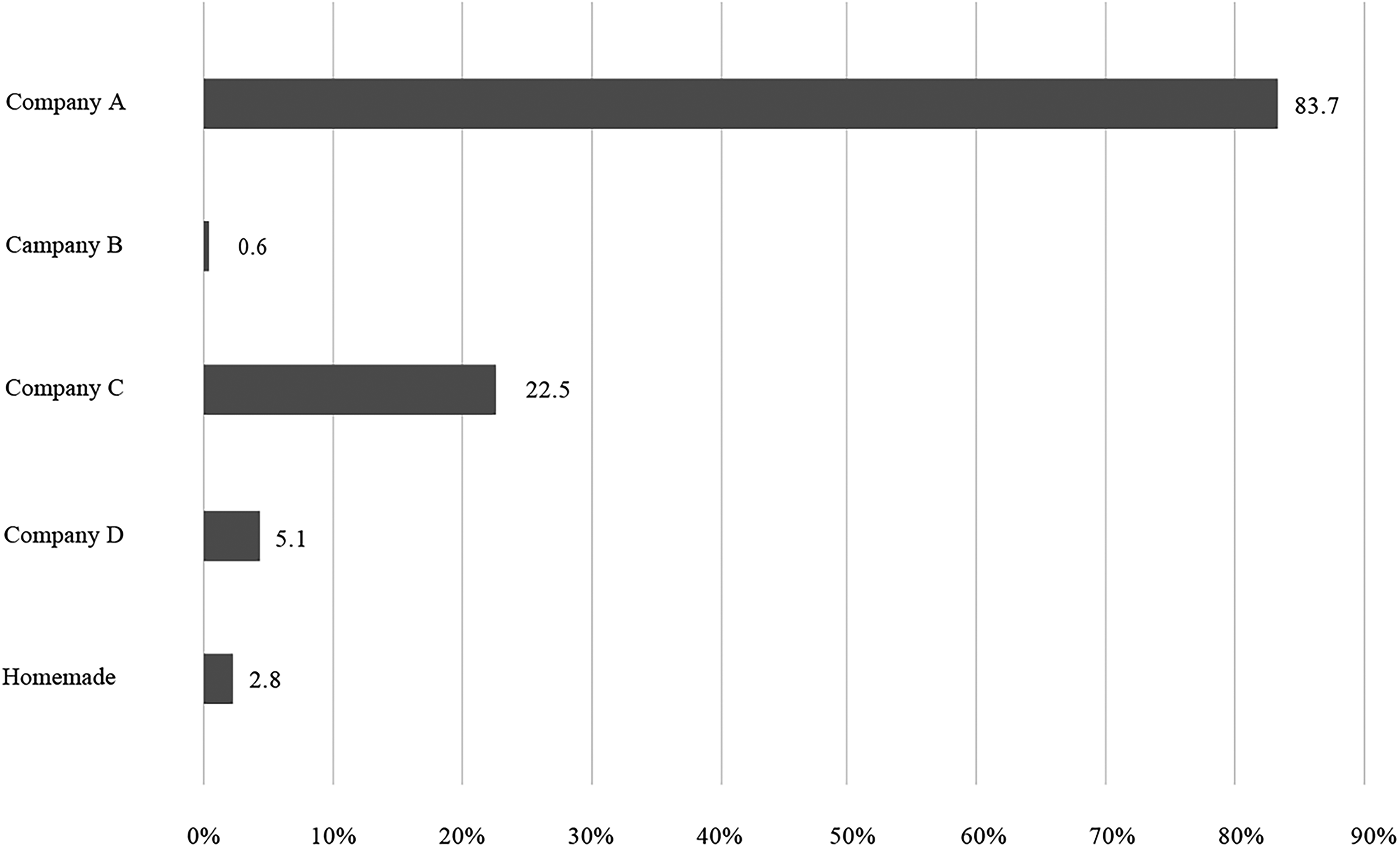
A bar graph depicting the responses to the question “Which manufacturer’s freezing solution is used in the vitrification process for patients with cancer? (Multiple answers allowed).”
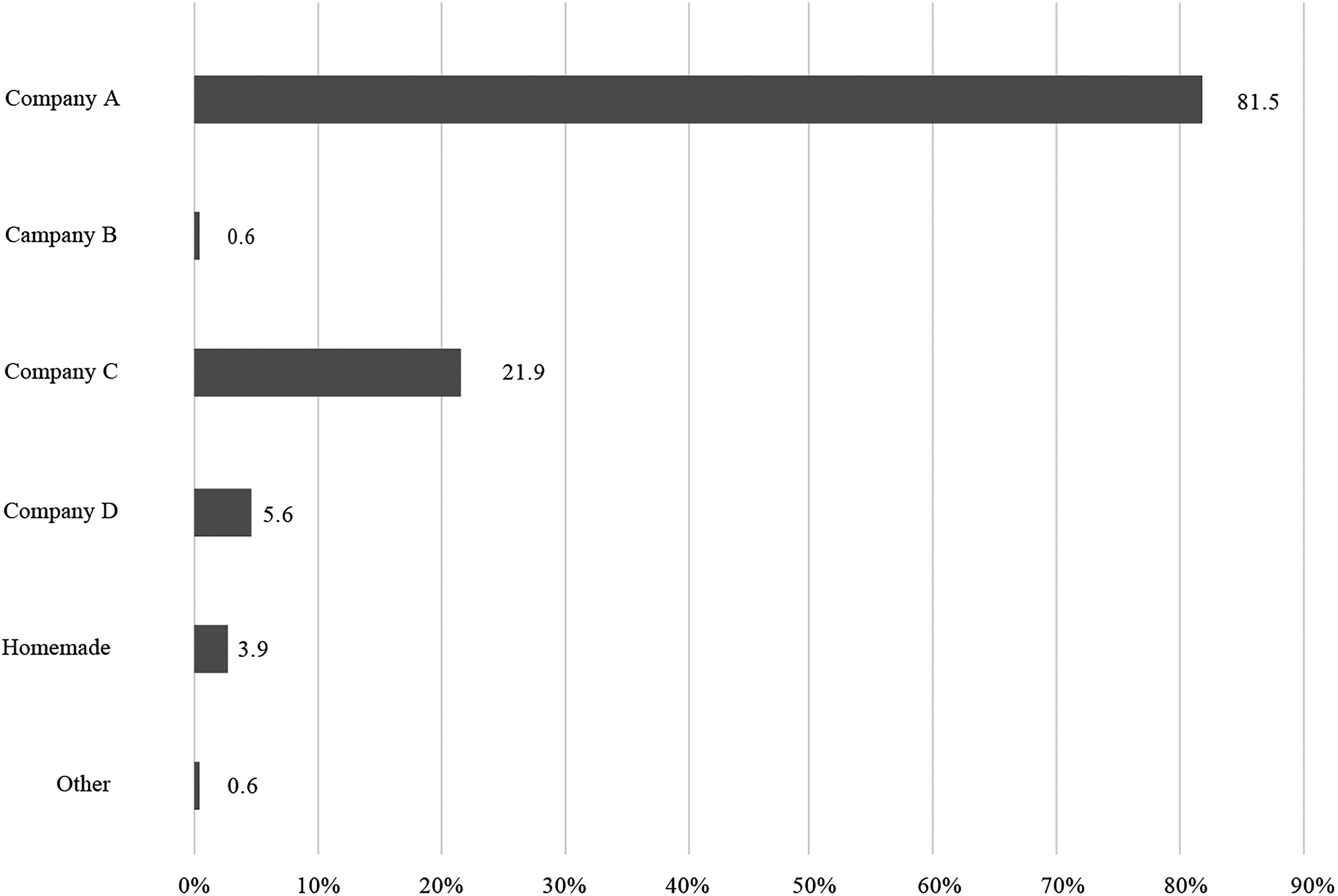
A bar graph depicting the responses to the question “Which manufacturer’s thawing solution do you use in thawing frozen embryos for patients with cancer? (Multiple answers allowed).”
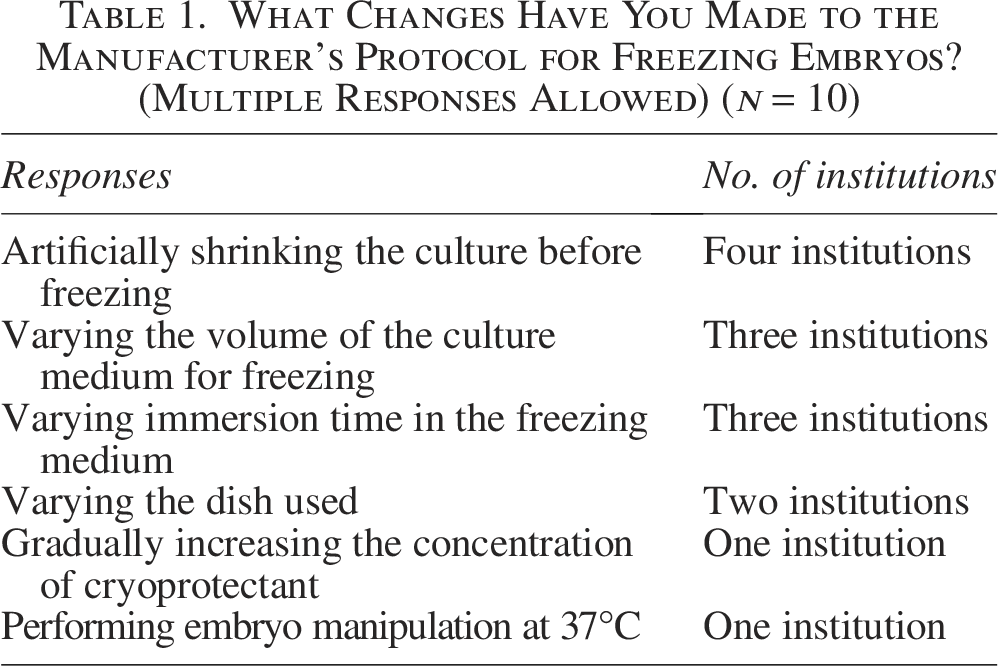
Embryo freezing was implemented according to the manufacturer’s recommended protocols by 98.4% (60/61) of institutions for pronuclear stage embryos, 95% (151/159) for cleavage stage embryos, and 93.2% (165/177) for blastocyst stage embryos (Fig. 11). Modifications to the protocols included performing artificial collapsing treatments before freezing, changing the volume of the freezing culture medium, changing the duration of immersion in the freezing culture medium depending on the developmental stage and condition of the embryo, and changing the dish used (Table 1). Thawing was conducted in accordance with the manufacturer’s recommended protocols at 93.8% (61/65) of institutions for pronuclear stage embryos, 93.1% (149/160) for cleavage stage embryos, and 91.5% (162/177) for blastocyst stage embryos (Fig. 12). Modifications to the protocol included changing the duration of immersion in the culture medium according to the developmental stage and condition of the embryo, changing the osmotic pressure of the culture medium, and changing the volume of the culture medium (Table 2).
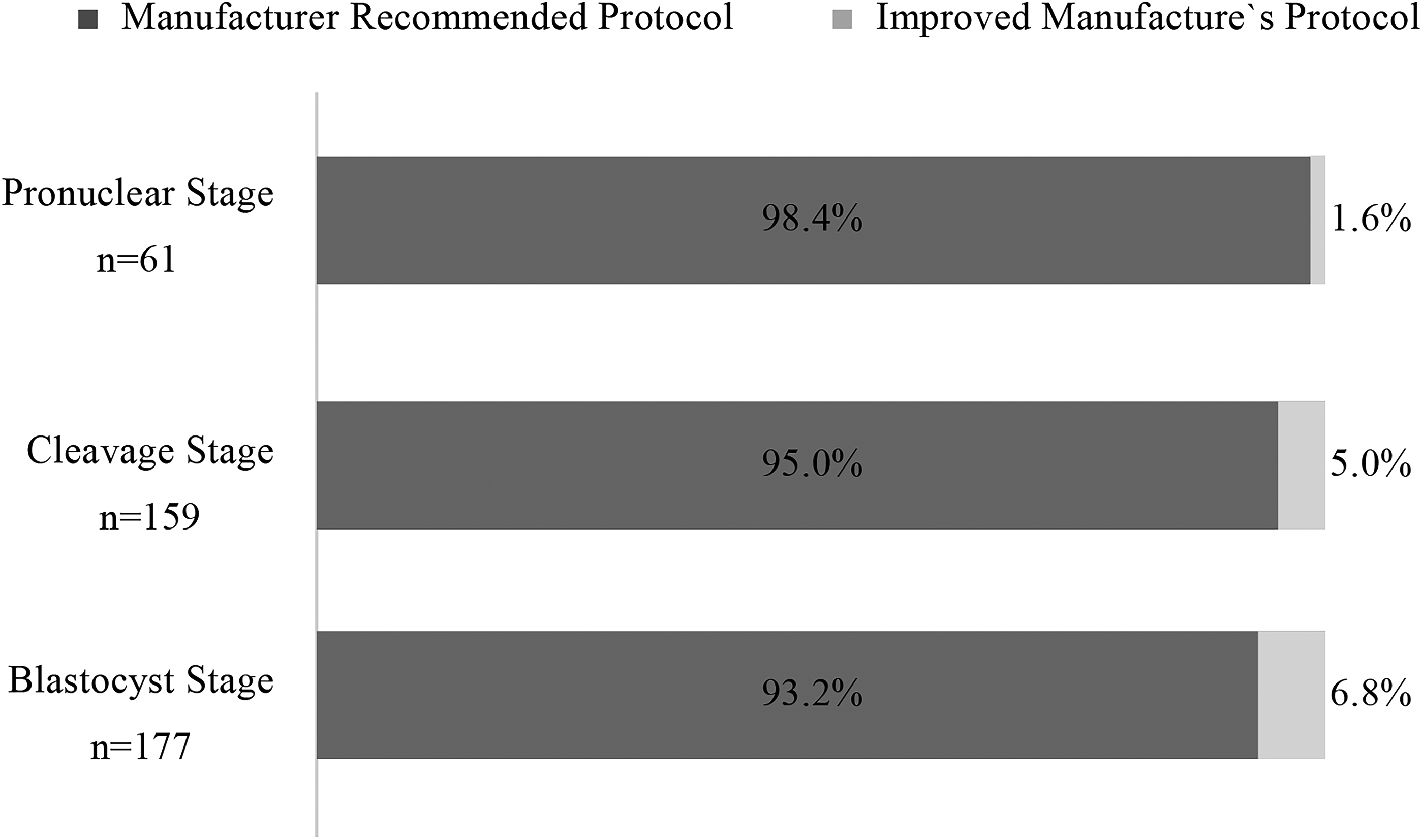
A bar graph depicting the responses to the question “What is the protocol for the vitrification method?”
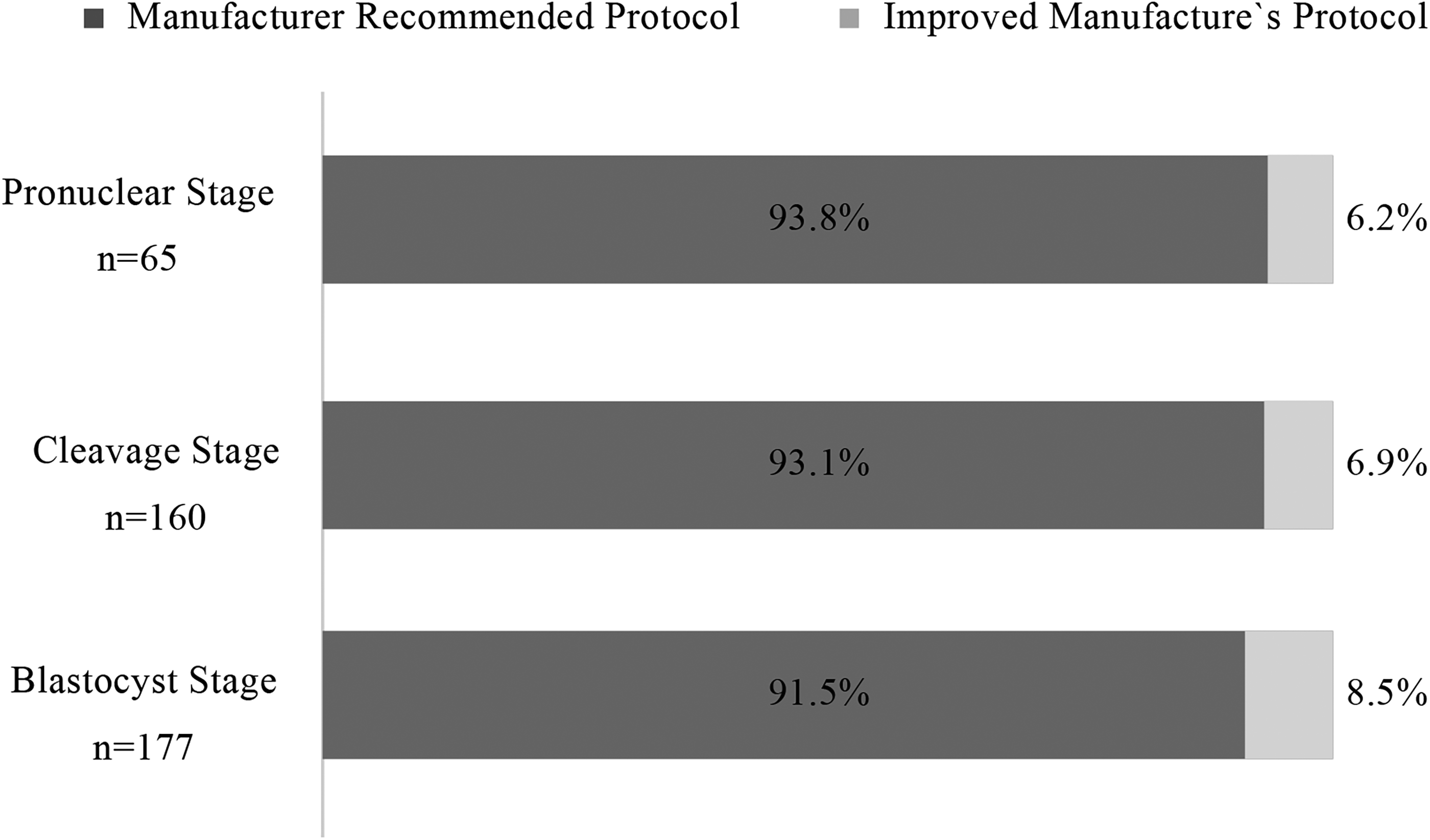
A bar graph depicting the responses to the question “What is the protocol for the thawing method?”
What Changes Have You Made to the Manufacturer’s Protocol for Freezing Embryos? (Multiple Responses Allowed) (n = 10)
What Changes Have You Made to the Manufacturer’s Protocol for Embryo Thawing? (Multiple Responses Allowed) (n = 8)

Associated concerns
A total of 45 institutions responded to an open-ended question regarding problems embryologists face when freezing embryos for patients with cancer, including 14 (31.1%) who expressed concerns regarding the management of frozen embryos after fertility preservation therapy, which included the storage period, cost, renewal procedures, and protocol in the event of closure of such centers. Thirteen respondents (28.9%) expressed concerns regarding the criteria for freezing embryos, including the stage and grade of embryo development and the number of embryos required. Eight institutions (17.8%) reported concerns regarding communication with patients, such as monitoring the treatment status of the primary diseases, changes of address, divorce or bereavement, and loss of communication. Six institutions (13.3%) wrote about securing storage space for preservation tanks. Another six (13.3%) reported other concerns, including an inability to perform egg retrieval due to the prioritization of primary disease treatment, difficulties explaining the expected outcomes without knowing the impact of the primary disease on embryonic development, the pressure of failure, the protocol for responding to a failure, the protocol for transferring embryos after the primary disease was treated, and differences between fertility preservation protocols for patients with cancer and general patients undergoing ART (Fig. 13).

A bar graph depicting the responses to the question “Do you have any difficulties in your cell culture department in implementing embryo cryopreservation for patients with cancer?”
Discussion
Cryopreservation technologies for reproductive cells such as unfertilized eggs, sperm, embryos, and ovarian tissue are essential for fertility preservation in oncofertility. Among these, embryo freezing can be performed using the same methods as those used for general patients undergoing ART. The results of this survey indicate that embryo freezing is performed for general patients undergoing ART at all of the institutions that responded to the survey. However, approximately half of the respondents conduct embryo freezing for the purpose of fertility preservation. Oncofertility treatment requires close collaboration between oncologists who treat the primary disease and reproductive medicine specialists who perform fertility preservation. Our results indicate that only 50.6% of institutions perform embryo freezing for patients with cancer, and significant variations exist in the freezing and thawing protocols. To ensure uniformity and improve patient outcomes, we recommend the development of national guidelines and mandatory certification for all fertility preservation facilities. In addition, training programs for embryologists specializing in cancer-related fertility preservation should be expanded. Interfacility collaboration is being conducted at the national level in the United States and Europe. 6 However, in Japan, most patients undergoing ART are treated in private clinics, highlighting the importance of a network to foster collaboration between facilities that provide cancer treatment. At present, the formation of this network is being led by the Japan Society for Fertility Preservation. 7 The small number of embryo cryopreservation facilities for fertility preservation may be a consequence of regional characteristics and specific conditions at each facility; however, this concern is not within the scope of this study. As approximately 20,000 women in their 20s and 30s are diagnosed with cancer each year in Japan, 8 the treatment environment for fertility preservation therapy is underdeveloped.
In addition, to perform fertility preservation therapy according to the medical indications, the Recommended Medical Indications for Freezing and Preserving Unfertilized Eggs, Embryos (Fertilized Eggs), and Ovarian Tissue were enacted by the Japanese Society of Obstetrics and Gynecology in April 2014. These recommendations require accreditation for fertility institutions. However, according to this survey, 29 facilities were conducting embryo freezing for the preservation of fertility without accreditation. As part of a national research promotion project, financial support for these institutions was initiated in April 2021, though institutions must be accredited as a medical institution for fertility preservation therapy by the Japanese Society of Obstetrics and Gynecology to receive such funds. This research promotion project is expected to establish data regarding fertility preservation therapy for pediatric, adolescent, and young adult patients with cancer.
Several facilities set age restrictions for embryo freezing for patients with cancer. The lower age limit is set due to the need for vaginal manipulation for egg retrieval and sperm for fertilization, while the upper age limit is set in consideration of the perinatal risk during pregnancy, as the thawed embryo transfer that follows fertility preservation therapy occurs after treatment of the primary disease is finished.
Furthermore, fertility preservation therapy for patients with cancer must be performed within the limited time period before treatment for the primary disease, and the primary treatment cannot be delayed. Therefore, some institutions change the patient criteria, fertilization methods, developmental stage during embryo freezing, and grade of frozen embryos. The risk of failure is lowered as experienced embryologists often conduct embryo cryopreservation for fertility preservation in patients with cancer. Approximately 80% of the respondents in this study employed five or fewer embryologists capable of freezing and thawing embryos for patients with cancer, suggesting that the number of embryologists involved in cancer reproductive medicine is relatively small.
Vitrification was used as the freezing method at all of the institutions, and nearly all of the institutions used cryopreservation devices, freezing solutions, and thawing solutions from two companies, Company A and Company C. Announced in 2000, the Cryotop method, 9 which became popular worldwide due to its high survival rate after freezing and thawing, was subsequently improved by various companies that developed products for vitrification freezing. A recent study reported that the addition of fatty acids to the thawing solution improves the developmental capacity of embryos after thawing. 10 Further improvements to embryo freezing methods are expected in the future.
Two types of freezing devices are used: open, in which the embryo is in direct contact with liquid nitrogen; and closed, in which there is no direct contact between the embryo and liquid nitrogen. In Western countries, closed-type devices are used to avoid viral contamination, 11 though most facilities in Japan use open-type devices. Cryopreservation for fertility preservation may require a long preservation period, indicating that significant reviews of the safety, techniques, and cost of cryopreservation and the development of safer methods are necessary.
Though there have been no major changes in the freeze-thaw protocols provided by each manufacturer since the development of cryopreservation supplies, the survival rate of the embryos is high, leading to most institutions adhering to the manufacturer’s recommended protocols. However, several institutions rely on veteran embryologists’ experiences in culture work to modify the protocols, ultimately improving treatment outcomes. The establishment of more effective protocols will require studies regarding the details of these modifications and their effects on treatment outcomes.
The open-response comments regarding problems in fertility preservations provided insight into the challenges of fertility preservation therapy, indicating that several institutions put embryologists in charge of administrative tasks, including direct communication with patients, which is traditionally not a role of embryologists. As patients who require fertility preservation therapy are typically struggling with a variety of health concerns before, during, and after fertility treatment, it is important for embryologists who interact with these patients to improve their social skills, including their bedside manner and word choice.
The results of this survey indicate that embryo freezing for fertility preservation therapy by embryologists in Japan is not being actively implemented despite its similarities to the procedure used for general patients undergoing ART. Embryologists expressed concern regarding the patients’ primary disease, leading to doubts and apprehensions regarding the success of cryopreservation. These concerns may be due to a lack of information regarding the current status of fertility preservation therapy for patients with cancer, current treatments, and outcomes after fertility preservation. This is the first Japanese survey of embryologists regarding the status of fertility preservation therapy, and it has provided insight into the status of embryologists’ work on fertility preservation therapy in Japan. However, further detailed investigations, including those regarding treatment results, are necessary.
Considerations on age restrictions for embryo cryopreservation
The results indicate that more than half of the surveyed institutions have age restrictions for embryo cryopreservation, with a median upper limit of 45 years and a lower limit of 16 years. The rationale for these restrictions varies, with many institutions considering factors such as ovarian reserve, pregnancy risks, and ethical concerns regarding fertility preservation in minors. Some institutions follow established guidelines, while others determine eligibility on a case-by-case basis.
These findings highlight the lack of a standardized approach to age restrictions in fertility preservation therapy in Japan. Future research should explore the long-term outcomes and ethical implications of age limitations, and further discussions among medical professionals may be necessary to establish uniform recommendations.
This study has several limitations. First, participants were selected based on self-reported questionnaires, which may increase the risk of social desirability bias. In addition, the study was limited to a specific population in a particular region, which may limit the generalizability of the findings. Furthermore, the study was not designed to establish the causality between the different groups; hence, the observed relationships do not necessarily indicate causality. Finally, the study used data limited to a specific time frame; hence, it cannot assess the long-term effects. Despite these limitations, this study provides valuable insights and can be a reference point for future research. For patients with cancer to be able to concentrate on treating their primary disease and improving their quality of life after treatment, future research regarding fertility preservation is necessary.
Limitations and future directions
One limitation of this study is that the questionnaire did not explicitly differentiate specific embryo freezing strategies for patients with cancer, such as the choice of freezing stage (day 3 vs. day 5) or detailed storage policies (e.g., grouping of grade 1 and grade 2 embryos). While some responses indicated modifications in embryo selection criteria and freezing practices, future research should include more specific questions to better capture clinical decision-making in fertility preservation for patients with cancer.
In addition, this study focused on challenges related to the management of cryopreservation facilities rather than the technical difficulties in cell culture. The questionnaire included items on issues such as frozen embryo management, criteria for freezing, patient communication, and storage space, reflecting operational and logistical concerns in fertility preservation programs. However, it did not specifically investigate difficulties in embryo culture processes, such as media selection, optimal culture conditions, or developmental characteristics of embryos from patients with cancer. Future studies should explore these aspects to gain a more comprehensive understanding of the technical challenges in fertility preservation for patients with cancer.
Another limitation is that the names of the manufacturers of cryopreservation devices and media were anonymized (e.g., Company A, Company B) in this study. This decision was made to avoid commercial bias and because the primary objective was not to evaluate specific products but to highlight the national trend showing that only a limited number of products are predominantly used across Japanese institutions. While the actual product names were not disclosed, the observed pattern indicates a concentration in product selection rather than diversity.
Furthermore, this study did not assess the frequency of oncofertility services, rates of treatment cycle cancellations, or clinical difficulties encountered during fertility preservation treatment. These are critical for understanding the feasibility and accessibility of fertility preservation services in real-world settings. Future surveys should incorporate these elements to provide a more complete picture of the barriers and facilitators in the implementation of fertility preservation for patients with cancer.
In conclusion, by identifying the current practices and challenges in embryo freezing for patients with cancer, this survey provides a foundation for improving the quality and consistency of fertility preservation services across Japan. The data collected will serve as a basis for policy recommendations and further research aimed at reducing disparities and standardizing practices nationwide. The findings of this survey study will enable embryologists to actively engage in fertility preservation therapy and create an environment in which patients with cancer can receive a high standard of treatment anywhere in Japan.
Authors’ Contributions
Conception and design: All authors. Survey development and review: All authors. Data collection and aggregation: Macromill Co. Ltd. (Tokyo, Japan). Analysis and interpretation: Research team members. Article writing: T.O. Critical revision: All authors. Final approval: All authors. Supervision: N.S.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
N.S. received funding from the Ministry of Health, Labour, and Welfare Science Research Grants (Cancer Policy Research Project) Research Group (20EA1004).
Human/Animal Rights
This article does not contain any studies with human and animal subjects performed by any of the authors.