
Abstract
Objectives:
This study aimed to assess the correlation of exacerbation and the mortality rate in patients with chronic obstructive pulmonary disease (COPD) between biomedical treatments with or without Chinese herbal medicine (CHM) as an adjunct.
Design:
A total of 81,261 COPD patients were identified from the National Health Insurance Research Database in Taiwan between 2001 and 2012. After screening and matching, 3176 COPD patients were included in the study. Statistical analyses were performed to assess the differences in the baseline characteristics. The authors used the Cox proportional hazard regression analysis to calculate the risks of mortality and hospitalization due to acute exacerbation of COPD within 1 year between a CHM user cohort and non-CHM user cohort. The cumulative incidence of mortality in COPD patients with or without CHM treatment was calculated by the Kaplan–Meier method.
Results:
COPD patients in the CHM user cohort demonstrated a significantly lower risk of mortality (p < 0.001) and acute exacerbation (p < 0.05), compared with the non-CHM user cohort. In addition, the CHM users exhibited a reduced cumulative incidence of mortality compared with the non-CHM user cohort (p < 0.001). Xiao Qing Long Tang and Fritillariae thunbergii were the most common Chinese herbal formula and single Chinese herb prescribed for COPD patients.
Conclusion:
Combining CHM with biomedical treatment might reduce the risk of acute exacerbation and incidence of mortality in patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent respiratory symptoms and airflow limitation due to exposure to noxious particles or gases. 1 Despite modern medical advances, COPD is a common respiratory disease causing significant morbidity and mortality globally; indeed, it is currently the fourth leading cause of death in the world, resulting in significant economic and social burdens. 2,3 It is therefore critical to reduce the disease burden by establishing effective intervention strategies for the prevention and management of COPD.
Acute exacerbation of COPD (AECOPD) is defined as an acute worsening of respiratory symptoms requiring additional therapy, 4 with episodes triggered by bacterial or viral infections, environmental pollutants, or unknown factors. 5 AECOPD reduces lung function and quality of life, and increases mortality risk. 6 The severity of exacerbations may be classified as mild, moderate, and severe, 7 with severe exacerbations of COPD requiring hospitalization and potential for emergency room admission, leading to substantial burdens on health services. 6,8 Reducing the rate of AECOPD is a crucial challenge facing the medical community, and would have notable benefits for patients and health care systems globally. 9
The pharmacologic treatments of COPD by biomedical medications currently include bronchodilators (β2 agonists and anticholinergics), inhaled glucocorticosteroids, theophylline, and phosphodiesterase 4 inhibitor. 1 Other managements of COPD involve smoking cessation, vaccination, pulmonary rehabilitation, oxygen therapy, and surgical intervention. 10 However, reports have indicated that Traditional Chinese Medicine (TCM) may also play an essential role in the treatment of COPD, as a complementary and alternative therapeutic option for COPD patients. 11,12 While TCM is extensively used for COPD in China and East Asian countries, it has been gaining interest in Western countries. 11,13
The use of TCM as an adjunct combined with standard biomedications exerts the beneficial effects of relieving respiratory discomfort, reducing incidence of COPD exacerbations, and improving quality of life. Although previous studies have reported on the application of TCM in the treatment COPD, the studies were confined to a specific region, with short-term follow-up, and small sample sizes. 14 –16 Currently, there is limited evidence indicating that TCM treatment reduces the risk of mortality in COPD patients.
Taiwan's National Health Insurance (NHI) was launched in 1995, covers >99% of the Taiwanese population, and reimburses TCM costs including Chinese herbal medicine (CHM) and acupuncture. Of note, TCM is the most common form of medical treatment in Taiwan after biomedicine. According to statistics, ∼30% of all patients in Taiwan have used TCM, with 90% of TCM users having received CHM therapy for various diseases. 17,18 This study aimed to evaluate whether the use of CHM in patients with COPD could correlate with reducing the risks of acute exacerbations and mortality. The study also analyzed the most common CHM prescriptions by clinical TCM practitioners to serve as a candidate list for future pharmacologic and clinical trial investigations.
Materials and Methods
Data source
The NHI program in Taiwan has established the National Health Insurance Research Database (NHIRD), which covers >99% of Taiwan's citizens. The database contains records regarding outpatient services, hospitalizations, medical treatments, and prescription records for each patient. For this study, the authors analyzed data using the Longitudinal Health Insurance Database (LHID 2000), which randomly selects 1 million study subjects from the NHIRD with confirmed distributions of gender and age similar to the NHIRD. The patient identification numbers are hidden before the database release for research purposes to protect privacy. The diagnoses are coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
The lack of identification numbers allowed for the approval of this study by the Research Ethics Committee of China Medical University and Hospital, Taichung, Taiwan [CMUH104-REC2-115(CR-4)] and was in compliance with the Declaration of Helsinki. Informed consent from patients was waived.
Study population and covariates
To examine the association between CHM users and non-CHM users among COPD patients relating to the incidence of mortality and emergency department (ED) visits or hospitalization due to AECOPD within 1 year, the authors identified patients with at least two outpatient visits or one inpatient admission with a diagnosis of COPD (ICD-9-CM: 491, 492, 496) between the years 2000 and 2012. AECOPD, as defined in this study, when COPD patients were given systemic corticosteroid treatment in the ER or during hospitalization and confirmed without other inflammatory diseases. COPD patients younger than 40 years and older than 100 years, and those diagnosed with asthma (ICD-9-CM: 493) were excluded.
To confirm as CHM stable users, only COPD patients receiving CHM treatment ≥14 days after the initial diagnosis of COPD were enrolled in the CHM user cohort. COPD patients without recorded CHM outpatient visit were selected for the non-CHM user cohort. The date of the first CHM prescription was defined as the index date. Cases started from the index date and ended on December 31, 2013, the date of death, or case withdrawal from the NHIRD. Cases and controls were 1:1 propensity-matched by age, gender, monthly salary, geographic region of residence, COPD diagnosis year, index year, comorbidities, and prescribed COPD medications.
The details of the population stratification are shown in Table 1. As comorbidities are important confounding factors in NHIRD studies, the authors defined comorbidities with at least two outpatient visits and/or one hospitalization record before the index date, including coronary artery disease (CAD) (ICD-9-CM: 410–414, A270, A279), congestive heart failure (CHF) (ICD-9-CM: 398.91, 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 425.4–425.9, 428), diabetes (ICD-9-CM: 250, A181), hypertension (ICD-9-CM: 401–405, A260, A269), stroke (ICD-9-CM: 430–438), arrhythmia (ICD-9-CM: 426, 427, 785.0, 996.01, 996.04, V45.0, V53.3), lung cancer (ICD-9-CM: 162), depression (ICD-9-CM: 296.2, 296.3, 300.4, 309.0, 309.1, 311), and osteoporosis (ICD-9-CM: 733.0).
Demographic Characteristics, Comorbidities, and Medications of Chronic Obstructive Pulmonary Disease Patients With or Without Chinese Herbal Medicine in Taiwan During 2000–2012
A standardized mean difference of ≤0.2 indicates a negligible difference.
CHM, Chinese herbal medicine; COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids; LABA, long-acting muscarinic antagonist; LAMA, long-acting beta-agonist; NT$, The New Taiwan dollar; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; SMD, standardized mean difference.
In addition, according to the severity of COPD by GOLD guidelines, the prescribed medications were categorized into only short-acting bronchodilator (short-acting beta-agonist [SABA] and/or short-acting muscarinic antagonist [SAMA]); long-acting bronchodilator (long-acting beta-agonist [LABA], and/or long-acting muscarinic antagonist (LAMA); inhaled corticosteroids (ICS) and LABA; as well as combined therapy with ICS, LABA, and LAMA. Moreover, the COPD patient was also divided by the visiting outpatient times into three subgroups, <5 times, 5–10 times, >10 times, to categorize the different severities.
Statistical analyses
To compare demographic characteristics, comorbidities, and COPD medications between the CHM user and non-CHM user cohorts, standardized mean difference was used for category and continuous variables. The authors calculated the risk of mortality and emergency or hospitalization due to AECOPD within 1 year between the two cohorts by using crude and multivariate Cox proportional hazard models presented by hazard ratios (HRs), and adjusted HRs with 95% confidence intervals. The cumulative incidence curves of the CHM and non-CHM cohorts were shown by the Kaplan–Meier method, and the difference between the two curves was tested by the log-rank test and plotted by R studio (3.5.2).
The network plot showed the pattern of any two CHM herbs or formula by NodeXL (
Results
Demographic characteristics
Of the 81,261 patients with COPD identified in the NHIRD between 2000 and 2012, 4523 patients were CHM users and 7099 were non-CHM users. After propensity score-matched (1:1) analysis, the final study consisted of 1588 patients in both cohorts (Fig. 1). Details of the characteristics of the CHM user and non-CHM user cohorts are shown in Table 1.
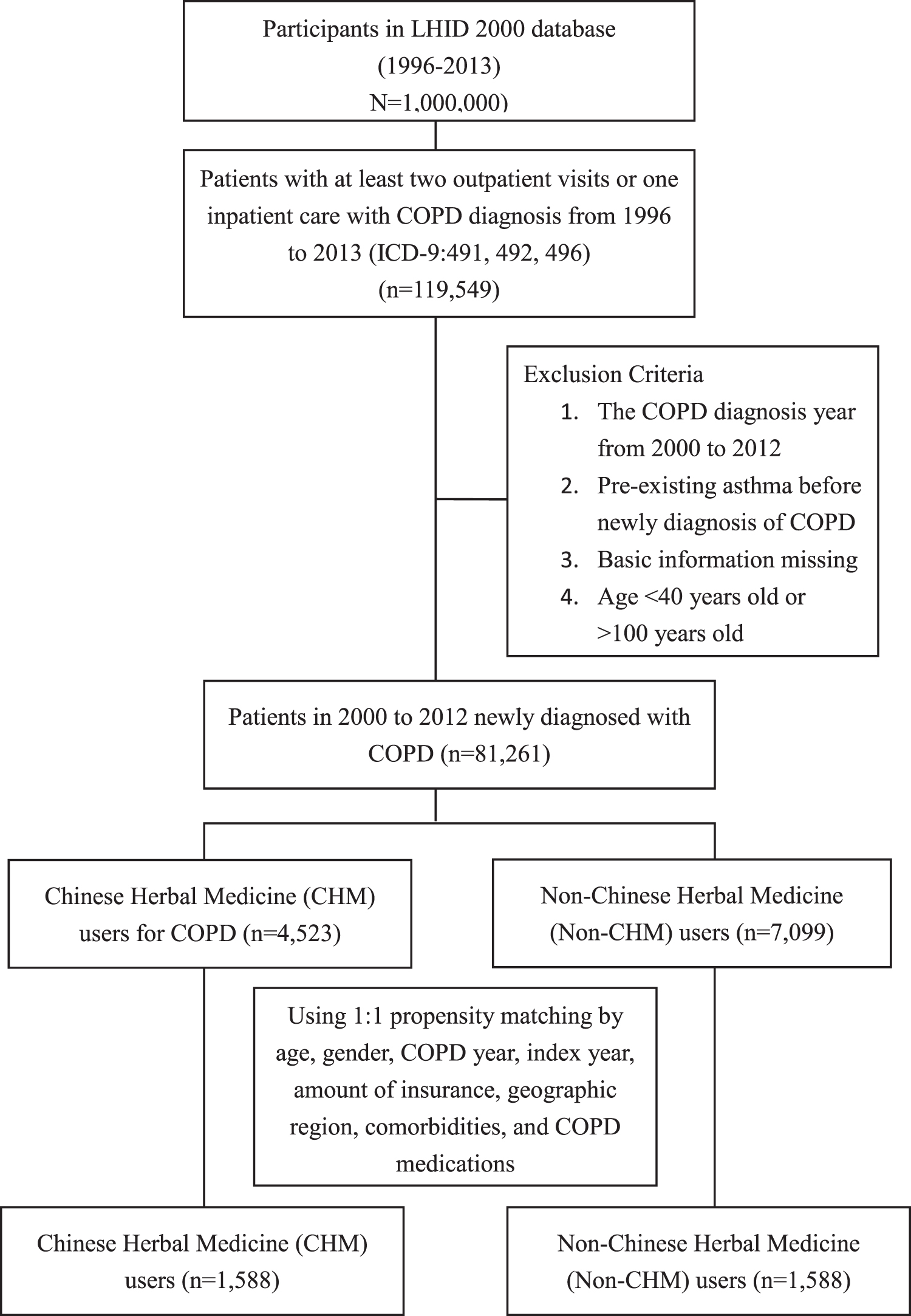
Flowchart of study cases identified from Longitudinal Health Insurance. Database in Taiwan between 2000 and 2012. CHM, Chinese herbal medicine; COPD, chronic obstructive pulmonary disease; ICD, International Classification of Diseases; LHID, Longitudinal Health Insurance Database.
Among the COPD patients, ∼40% were female, ≥65 years, with The New Taiwan dollar (NTD) 15,841–28,800 monthly salary, and residing in the northern geographic region. Comorbidities among patients in the CHM user cohort included 561 (35.3%) patients with CAD; 164 (10.3%) patients with CHF; 427 (26.9%) patients with diabetes; 940 (59.2%) patients with hypertension; 329 (20.7%) patients with stroke; 250 (15.7%) patients with arrhythmia; 8 (0.5%) patients with lung cancer; 128 (8.1%) patients with depression; and 201 (12.7%) patients with osteoporosis. The prescribed treatments for patients in the CHM user cohort included 328 (20.7%) patients with only SABA and/or SAMA; 169 (10.6%) patients with LABA and/or LAMA; 162 patients (10.2%) with ICS and LABA; and 41 (2.6%) patients with ICS, LABA, and LAMA.
Of note, the demographic characteristics, comorbidities, and COPD medications showed no significant differences between the two cohorts.
HRs and cumulative incidence of mortality for the CHM and non-CHM user cohorts
As shown in Table 2, the CHM user cohort demonstrated a lower risk of mortality compared with the non-CHM cohort. In addition, COPD patients in the CHM user cohort showed a decreased risk of ED visits or hospitalizations due to AECOPD within 1 year, compared with non-CHM users (Table 3). Furthermore, the 10-year cumulative incidence of mortality was significantly lower in the CHM user cohort than the non-CHM user cohort (Fig. 2).
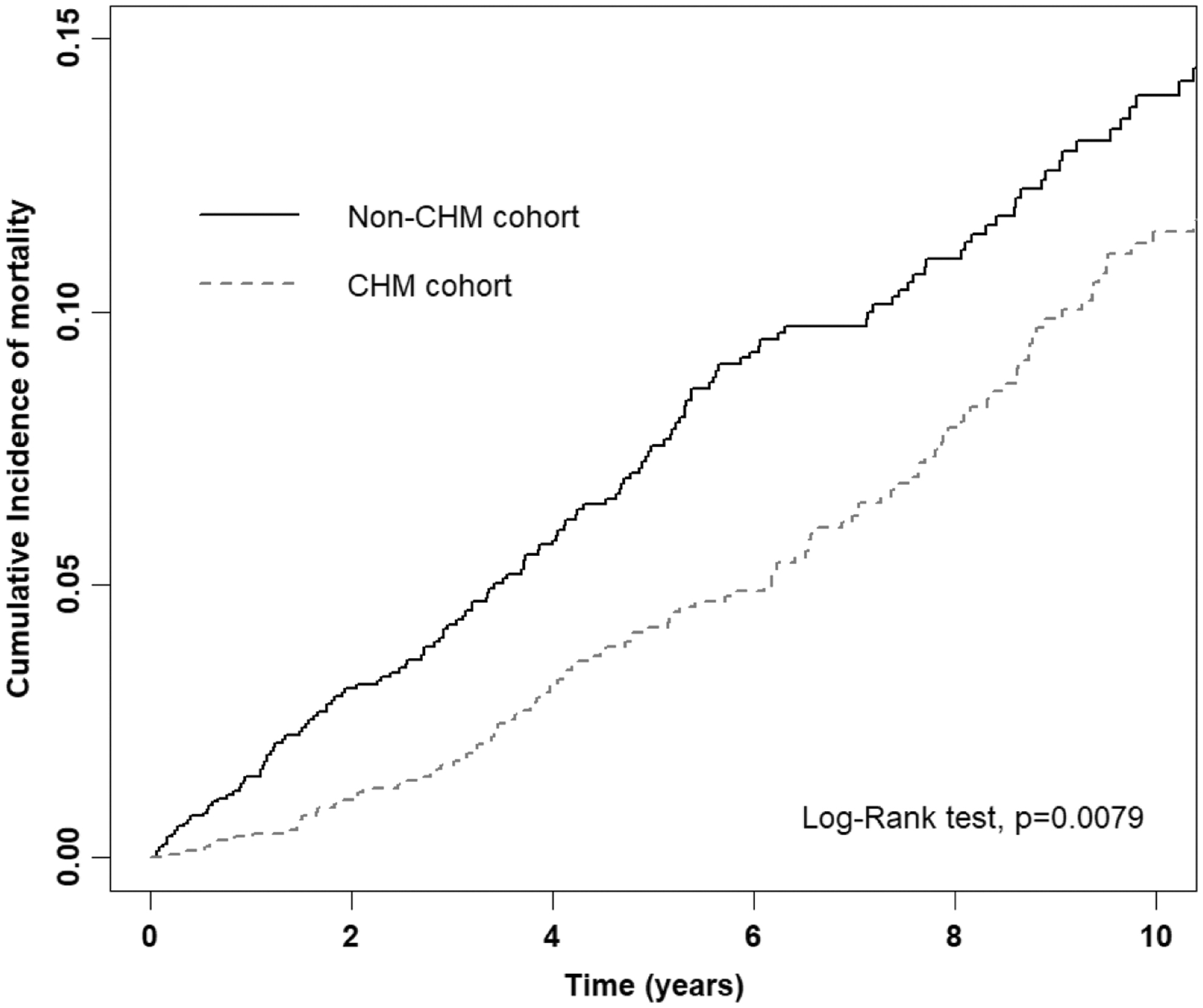
Comparison of Kaplan–Meier estimates of the 10-year cumulative incidence of mortality in chronic obstructive pulmonary disease patients with and without CHM usage (log-rank test, p < 0.001). CHM, Chinese herbal medicine.
Incidence Rates, Hazard Ratios, and Confidence Intervals of Acute Exacerbation of Chronic Obstructive Pulmonary Disease by Admission to Emergency Department or Hospitalization
p < 0.05.
aHR, adjusted for age, monthly income, geographic region, all comorbidities and all medications in Cox proportional hazard regression; CHM, Chinese herbal medicine; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; IR, incidence rates, per 10,000 person-years;
Incidence Rates, Hazard Ratio, and Confidence Intervals of Mortality in Different Stratifications
*p < 0.05.
p < 0.01.
p < 0.001.
aHR, adjusted for age, monthly income, geographic region, all comorbidities and all medications in Cox proportional hazard regression; CHM, Chinese herbal medicine; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HR, hazard ratio; ICS, inhaled corticosteroids; IR, incidence rates, per 10,000 person-years; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; NT$, The New Taiwan dollar; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist.
The authors also investigated the incidence of mortality among the two cohorts, with analyses stratified by age, gender, insurance premium based on salary, area of residence, comorbidities, and prescribed medications (Table 2). Compared with non-CHM users, CHM users were associated with a lower risk of mortality among patients ≥65 years of age, including both female and male patients. Of the patients with a monthly salary of less than NT$ 45,800, the CHM cohort demonstrated a significantly higher risk of mortality than the non-CHM cohort. In addition, patients in the CHM user cohort residing in the northern region of Taiwan showed a significantly lower mortality rate than non-CHM users.
In the comorbidity subgroup, patients with CAD, CHF, diabetes, hypertension, stroke, arrhythmia, and depression exhibited lower mortality rates. In terms of the standard prescribed medication subgroup, patients having received only SABA and/or SAMA exhibited a lower mortality rate. Moreover, patients with less than five outpatient visits in the COPD severity subgroup demonstrated a lower mortality rate.
Top 10 individual herbs and formulas prescribed by clinical practitioners
In terms of herbal formulas, the three most frequently prescribed formulas for treating COPD patients were Xiao-Qing-Long-Tang, followed by Ding-Chuan-Tang and Mai-Men-Dong-Tang. Detailed information regarding herbal ingredients is shown in Supplementary Table S1. In addition, the average duration in each time prescription for the three herbal formulas was 11.1, 10.9, and 11.1 days, with average daily dosages of 6, 8, and 4.9 g, respectively (Table 4).
Ten Most Common Formulas and Herbs Prescribed for Patients with Chronic Obstructive Pulmonary Disease
As for the prescribed single herbs, the top 3 single herbs prescribed by clinical practitioners were Fritillaria thunbergii (Thunberg Fritillary), Platycodon grandiflorum (Platycodon Root), and Prunus armeniaca (Ansu Apricot Seed). The average duration in each time prescription for these three single herbs was 11.5, 11.8, and 11.1 days, with average daily dosages of 1.8, 1.9, and 1.2 g, respectively (Table 3). The network plot revealed that the two most common combinations in the prescriptions were F. thunbergii (Thunberg Fritillary) and P. grandiflorum (Platycodon Root), as well as P. armeniaca (Ansu Apricot Seed) and P. grandiflorum (Platycodon Root) (Fig. 3).
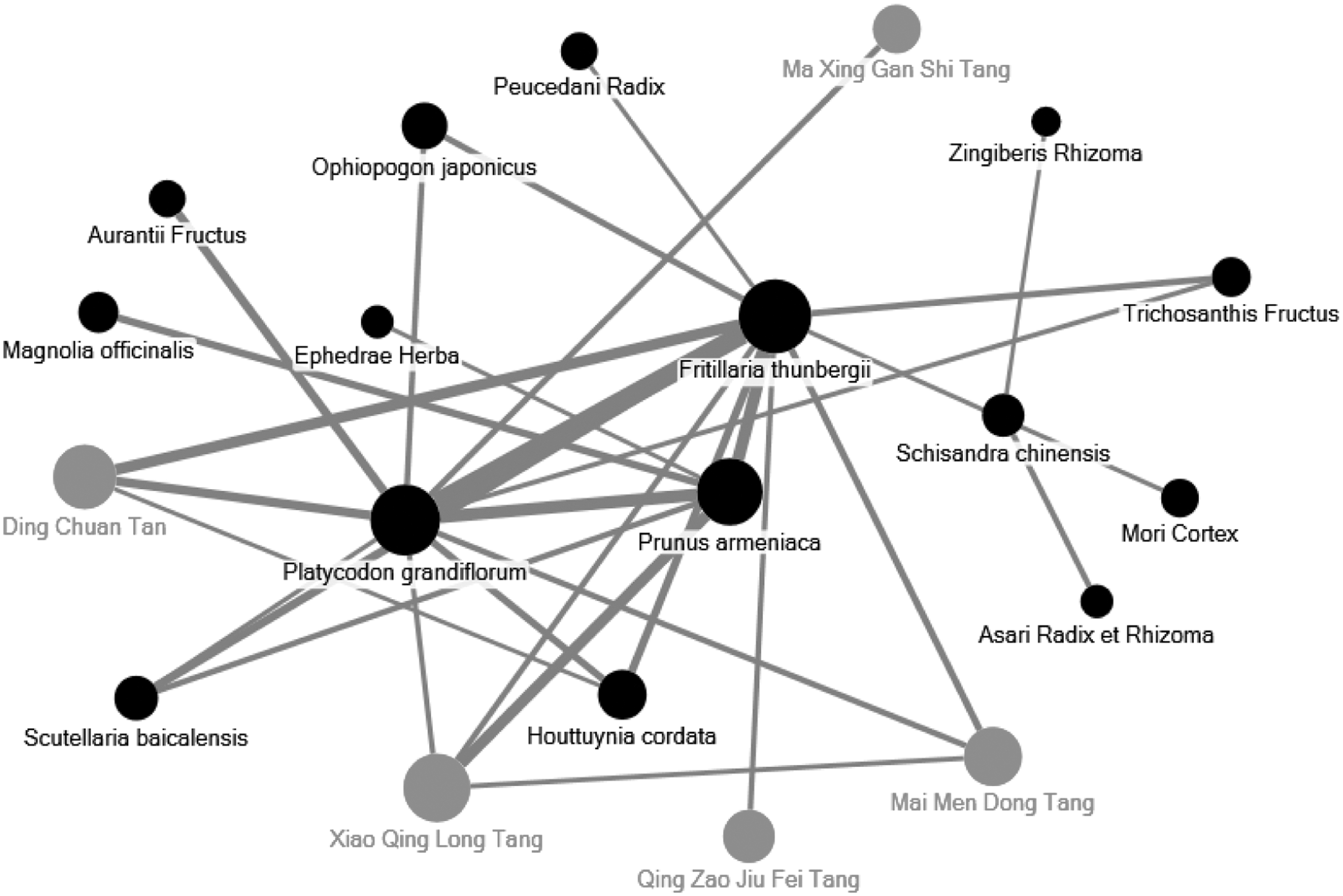
Network analysis of the most frequent 30 herb and formula combinations in chronic obstructive pulmonary disease patients by open-source freeware NodeXL. The size of spot indicates the frequency of Chinese herbal product, and the width of line indicates the frequency of combinations of two Chinese herbal products.
Discussion
COPD is a common progressive disease associated with high morbidity and mortality rates, while AECOPD is a significant factor associated with mortality. Exacerbations and comorbidities contribute to the overall severity in individual patients. Previous studies have reported that patients admitted to intensive care units due to AECOPD had a mortality rate of ∼11%–24%. 4,19 As such, reducing exacerbation frequency is a fundamental goal for COPD management, and an indicator for evaluating treatment. In this 10-year nationwide cohort study, the authors examined whether CHM treatment reduced the incidence of acute exacerbation and mortality among COPD patients by using the LHID in Taiwan.
After propensity score matching, COPD patients in the CHM user cohort demonstrated significantly decreased mortality and acute exacerbation rates compared with the non-CHM cohort. In addition, CHM users maintained a significantly reduced risk of mortality and acute exacerbation in the subgroup with comorbidities such as CAD, CHF, hypertension, diabetes, stroke, arrhythmia, and depression compared with those without CHM treatment. Comorbidities not only significantly influence COPD prognosis but are also negatively impacted by COPD. 20 Cardiovascular diseases are regarded as frequent comorbidities affecting COPD patients. 21 This study revealed that patients with CAD experienced an increased risk of myocardial damage for at least 30 days after AECOPD. 22
The study also indicates that both the progression and prognosis of COPD could be negatively impacted by diabetes; meanwhile, treatments for COPD, including corticosteroids, may lead to increased risk of developing type 2 diabetes. 23 Furthermore, it is commonly accepted that COPD could elevate the risks of ischemic and hemorrhagic stroke. 24 This study suggests that CHM treatment may be beneficial for COPD patients with comorbidities. Notably, in terms of COPD medication, the authors found that CHM treatment combined with SABA demonstrates more positive effects than other medications. These results indicate that the intervention of CHM could be more effective in patients with mild COPD. However, this finding may be biased due to insufficient case numbers of patients with moderate to severe COPD included in this study.
Although the authors defined the stable CHM users as the patients receiving ≥14 days in total, the TCM doctors could change the CHM prescription based on their condition of each outpatient department services. According to Taiwan's medical record, most of TCM practitioners prescribed medication for patients about 1–2 weeks each time. This situation resulted in 10–11 days of each prescription that was <14 days.
The underlying pathogenesis of COPD involves chronic inflammation, 25 increased oxidative stress, and protease/antiprotease imbalance, 26 leading to characteristic physiological abnormalities, including mucous hypersecretion, airflow obstruction and hyperinflation, gas exchange abnormalities, and pulmonary hypertension. 27,28 According to the TCM theory, Xiao-Qing-Long-Tang, the most frequently prescribed formula in this study, is used to dissipate cold, warm the lungs, and resolve fluid retention. It has been shown to suppress inflammatory cytokines, inducible nitric oxide synthase expression, and nuclear factor-κ B phosphorylation in smokers in both in vivo and in vitro studies. 29 In addition, it has been demonstrated by an in vivo study to inhibit COPD progression by attenuating autophagy. 30
Meanwhile, Ding-Chuan-Tang is traditionally used to treat wheezing, cough with sticky sputum, and dyspnea. It is applied to diffuse the lung to ease shortness of breath and clear heat to resolve phlegm. A previous study reported the effects of Ding-Chuan-Tang on the suppression of inflammation via regulation of the interleukin-1 receptor-associated kinase/nuclear factor-κ B, interleukin-1 receptor-associated kinase/activator protein-1, and TANK-binding kinase 1/interferon regulatory factor 3 pathways in lipopolysaccharide-stimulated macrophages. 31 In another clinical study, Ding-Chuan-Tang combined with standard biomedical treatment was shown to ameliorate clinical symptoms, reduce the recurrence rate, and improve lung function in AECOPD patients. 32
Furthermore, Mai-Men-Dong-Tang has been used for hundreds of years to treat coughs corresponding with the pattern of “lung yin deficiency.” A clinical study indicated that it had beneficial effects in attenuating chronic cough severity in COPD patients. 33 It has also been confirmed to suppress airway hyper-responsiveness by inhibiting release of vagal neuroeffector transmitters. 34,35
With regard to the single herbs identified in this study, F. thunbergii (Thunberg Fritillary, Zhe-Bei-Mu), P. grandiflorus (Platycodon Root, Jie-Geng), and P. armeniaca (Ansu Apricot Seed, Xing-Ren) were the three most prescribed herbs used in the treatment of COPD. F. thunbergii (Thunberg Fritillary) has been well documented to clear heat, transform phlegm, and suppress coughing. In an animal study, F. thunbergii (Thunberg Fritillary) has been reported to exert antitussive, expectorant, and anti-inflammatory effects. 36 Meanwhile, P. grandiflorus (Platycodon Root) facilitates the flow of lung-qi to dispel phlegm from the lungs. P. grandiflorus root-derived saponin is reported to inhibit acrolein-induced expression of mucin 5 by suppressing the activation of nuclear factor-κ B phosphorylation. 37
P. armeniaca (Ansu Apricot Seed) is used to diffuse the lung, suppress coughing, and moisten the lungs to resolve phlegm. P. armeniaca (Ansu Apricot Seed) has reported antioxidant, antimicrobial, and antitussive effects. 38 In addition, in a rat model of COPD induced by cigarette smoke, H. cordata (Fish mint) exhibited an anti-inflammatory effect. 39 Based on the results of previous studies, all of these herbs and formulas have been applied to ameliorate clinical symptoms, reduce inflammation, and inhibit oxidation. A summary of the most commonly prescribed formulas and herbs for treatment of COPD is shown in Supplementary Table S1.
The authors know that adverse medication events are essential in every study and population. However, the NHIRD study cannot assess the adverse interaction from the database directly. Thus, they made a literature review to disclose the related information. Although some herbs with non- or low toxicity are considered, F. thunbergii (Thunberg Fritillary) with an overdose consumption might lead to tremor and reduce spontaneous motor activities, and the recommended dose is 5–10 g for adults. 40 The P. grandiflorum (Ansu Apricot Seed) may possess sedative effects, such as movement inhibition and respiration decrease. 41 P. armeniaca (Ansu Apricot Seed) could have side effects such as nausea, vomiting, diarrhea, dizziness, weakness, mental confusion, and convulsions; generally suggested to eat <3–10 per day. 42
To the best of knowledge, there is no direct adverse record of the Xiao-Qing-Long-Tang 43 and Mai-Men-Dong-Tang, 44 but some studies reported that Ding-Chuan-Tang might have a few side effects, including hypertension, tachycardia, palpitation, and seizure, 45 and should be carefully monitored.
Inevitably, there are several limitations to this study. First, self-purchased Chinese herbal products or decoctions were not recorded in the database. Taiwan's NHI program reimburses only granular herbal products that are manufactured in accordance with Good Manufacturing Practice guidelines provided by pharmaceutical facilities. Second, detailed information of COPD assessment such as pulmonary function tests, laboratory data, and images is not recorded in the database. Third, lifestyle-related information such as drinking, smoking status, and environmental/chemical exposure is not collected. Fourth, the safety issues correlated to adverse events or interactions induced by herbal supplements are absent in the NHIRD database.
Conclusion
Collectively, this study provides clinical evidence that CHM in combination with biomedicine may lower the risk of acute exacerbation and the incidence of mortality in COPD patients. Further clinical and experimental studies with longer follow-up are warranted to confirm the efficacy further and elucidate the mechanisms of the most common single herbs and formulas prescribed for COPD patients.
Footnotes
Authors' Contributions
J.H.H. and W.C.C. wrote the article and interpreted the data. H.M.C. and M.C.L. collected, assembled, and analyzed the data. J.L.W., P.K.F., and C.P.L. checked the data and amended the references. S.T.H. designed and conceived the study and amended the article. All the authors approved the final article.
Acknowledgment
The authors thank James Waddell for the critical reading and revision of their article.
Author Disclosure Statement
None declared.
Funding Information
This work was supported and funded by the Ministry of Science and Technology of Taiwan (MOST 108-2320-B-039-022), Health and Welfare Surcharge of Tobacco Products, China Medical University Hospital Cancer Research Center of Excellence (MOHW108-TDU-B-212-124024), China Medical University Hospital (DMR-110-189, DMR-110-004, DMR-110-009, and CRS-108-001), and An-Nan Hospital, China Medical University (ANHRF-108-06 and ANHRF-108-08). This work was also supported by grants from the Ministry of Health and Welfare, Taiwan (MOHW107-TDU-B-212-123004), China Medical University Hospital, Academia Sinica Stroke Biosignature Project (BM10701010021), the MOST Clinical Trial Consortium for Stroke (MOST 107-2321-B-039 -004-), Tseng-Lien Lin Foundation, Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.