
Abstract
Objectives:
There is currently no exact and effective treatment for postoperative delirium (POD). The purpose of this study was to observe the effect of transcutaneous electrical acupoint stimulation (TEAS) before surgery and during surgery in elderly patients with POD.
Materials and Methods:
A total of 90 patients were randomly divided into three groups: a preoperative TEAS group (group E1), an intraoperative TEAS group (group E2), and a control group (group C). In group E1, TEAS was applied at the Shenting, Baihui, bilateral Neiguan, and Hegu points for 30 min 1 day before surgery and before the induction of anesthesia. In group E2, TEAS was applied during surgery. In group C, electrodes were applied to the points just cited, but no electric stimulation was administered. The incidence of delirium was assessed within 5 days after surgery, and the plasma concentration of propofol at bispectral index (BIS) = 50 was recorded. Blood samples were collected to measure neuron-specific enolation (NSE), tumor necrosis factor-α (TNF-α), and interleukin (IL)-1β 1 day before surgery and 1 and 5 days after surgery.
Results:
The incidence of delirium in group E1 was decreased in comparison with group C and group E1 (both p < 0.05). The propofol plasma concentration at BIS = 50 in group E1 was also decreased in comparison with group C and group E2 (both p < 0.05). Compared with group C, the concentrations of NSE, TNF-α, and IL-1β in plasma were decreased in group E1 and group E2 1 and 5 days after surgery (both p < 0.05), and the concentrations of NSE and IL-1β in plasma in group E1 were decreased 1 and 5 days after surgery in comparison with group E2.
Conclusion:
The TEAS can reduce the dosage of propofol required during surgery and the occurrence of delirium after surgery. Its mechanism may be related to inhibiting inflammation response and alleviating brain injury. Compared with intraoperative application, the effect of preconditioning with TEAS before surgery is better.
Clinical Trial Registration:
ChiCTR-INR-17012501. Date of registration: August 29, 2017
Introduction
Postoperative delirium (POD) is an acute fluctuating neurological syndrome that usually occurs within a few hours to a few days after surgery. It mainly manifests as a decrease in consciousness and attention deficit and thinking disorder, 1 especially in critically ill patients. In different research populations and types of surgery, the incidence rate is 20%–80%, 1,2 the duration of delirium exceeds 48 h, and the mortality of patients increases by 11%. 3
The high-risk factors for POD are advanced age and surgery, which are the main challenges faced by the rapidly growing ageing population in China. 2 According to data from the National Bureau of Statistics, there were 249 million people in China aged 60 and older at the end of 2018, accounting for 17.9% of the total population. 4 With the aging of the population and the increasing demand on health care systems, both the proportion and absolute number of elderly patients undergoing surgery have increased rapidly and are expected to continue rising. 5
A large number of basic studies have shown that acupuncture treatment can improve postoperative cognitive function and have demonstrated that its effect is multifaceted. Baihui, Shenting, Neiguan and Hegu are commonly used acupoints in clinical practice that have a variety of functions. Acupuncture at these points has a good curative effect on cerebrovascular diseases.
Shenting is positioned 0.5 cun (equal to 0.66 inches) above the middle of the front hairline (in modern anatomy, at the junction of the left and right frontal muscles, where there are branches of frontal arteries and veins and where frontal nerves are distributed). Traditional Chinese medicine states that acupuncture at Shenting can clear the head, calm the nerves and mind, and treat diseases related to mental illness. The Baihui point has branches of the greater occipital nerve, the anastomotic network of the left and right superficial arteries and veins, and the left and right occipital arteries and veins, 6 which are closely related to brain function.
Modern research has also suggested that Shenting and Baihui are located in the projection areas of the frontal, temporal, and parietal lobes, which are closely related to advanced thinking, memory, and spirit. Acupuncture can, therefore, affect and improve brain function. 7,8
An animal study found that electroacupuncture 1 day before and 1–7 days after hepatectomy could improve the cognitive function of rats with postoperative cognitive dysfunction by reducing the number of glial fibrillary acidic protein-positive astrocytes in the hippocampus and inhibiting oxidative stress. 9 Electroacupuncture can also inhibit neuronal apoptosis. In another study, Baihui was selected for electroacupuncture treatment 5 days before elderly rats underwent laparotomy. Postoperative cognitive function was found to improve, and the rate of neuronal apoptosis in the hippocampus was found to decrease. 10
Electroacupuncture at the Shenting acupoint might also improve the cognitive function of patients with Alzheimer's disease by decreasing the levels of Aβ, phosphorylated tau (p-tau) (s396) and p-tau (s404) in the brain. 11 The current study confirmed that acupuncture at the Hegu point can modulate the functional activity and connectivity of specific cognition-related regions in patients with Alzheimer's disease, 12 and acupuncture at the Neiguan point has been found to reduce the duration of postoperative cognitive decline in the elderly, which may be related to the regulation of inflammatory factors and neuropeptides interacting with the intestinal brain axis. 13
Further, electroacupuncture has also been found to reduce microglia activation and inflammatory response by increasing the expression level of miR-124, which regulates microglia activation, in the hypothalamus and hippocampus. 14 At present, however, there are a few human studies on acupuncture improving cognitive function.
There is currently no exact and effective treatment for POD. Studies have found that transcutaneous electrical acupoint stimulation (TEAS) can effectively alleviate the symptoms of POD, but the timing of its use still needs to be explored. 15 Dong 16 suggested that electroacupuncture and TEAS can effectively simulate the central regulation of traditional acupuncture, therefore exerting similar physiological effects, and the three may have similar neurochemical mechanisms. The TEAS has the advantages of being simple to operate, safe, and noninvasive, so the present study selected it to explore the preventive effect of acupoint electroacupuncture on patients with POD.
Materials and Methods
Clinical data
General information
The diagnosis of POD mainly referred to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). 17
Inclusion criteria: (1) patients who were scheduled to undergo lumbar (cervical) pedicle internal fixation and bone-graft fusion between September 2017 and January 2019 in our hospital; (2) estimated operation time >2 h; (3) patient age >60 years; (4) American Society of Anesthesiologists (ASA) grade I–III 18 ; (5) patient body mass index 18–24.9 kg/m2; (6) patient able to communicate normally, including normal language ability, normal writing ability, normal vision, and normal hearing (hearing aids could be worn); and (7) patient was willing to accept acupoint-stimulation anesthesia. Exclusion criteria: (1) patient did not meet the inclusion criteria; (2) patient did not want to participate.
Fall-off criteria: (1) patient developed serious adverse reactions during the treatment; (2) patient developed other diseases during the treatment; and (3) patient with aggravation required other emergency treatment measures.
This study was approved by the Medical Ethics Committee of the hospital, and the patients and their families provided signed informed consent.
Grouping
This randomized trial was in conformity with CONSORT 2010 (Supplementary Table S1). SAS9.4 software Proc Plan process programming was used to generate random numbers for random distribution. The generated random distribution sequence was placed in a sealed and opaque envelope according to the coding order. Each subject corresponded to an envelope. When the study was officially launched, the researcher opened the envelopes and assigned each subject to the corresponding test group. Using this random method, participants were divided into three equal groups: a preoperative TEAS group (group E1), an intraoperative TEAS group (group E2), and a control group (group C), with 30 cases in each group.
Baseline characteristics before surgery
The baseline characteristics before surgery were recorded. (1) Cognitive function: There was cognitive dysfunction if the patient's mini-mental state examination (MMSE) score was <27. (2) Nutrition status: There was nutritional risk if mini-nutritional assessment (MNA) score was ≤23.5. (3) Activity of daily living: There were defects in the activity of daily living if ≥1 item was fully restricted. (4) Weakness: There was obvious weakness if the patient's Fried score was ≥3. (5) Operation time. (6) Volume of blood loss.
Implementation plan
All patients were informed about TEAS and the methods of anesthesia and surgery by an anesthesiologist 1 day before the surgery to gain their understanding and trust. After entering the operating room, all patients were given midazolam 0.04–0.06 mg/kg via an intravenous drip.
Anesthesia and intraoperative intervention methods: After the patient entered the operating room, venous access was established and connected to an anesthesia monitor to monitor electrocardiogram, noninvasive arterial blood pressure, respiratory rate (RR), and pulse oxygen saturation (SpO2). Radial artery puncture and catheterization was performed under local anesthesia to monitor invasive arterial blood pressure.
A target-controlled infusion of propofol at a plasma target concentration of 0.6–3 μg/mL, sufentanil at 3 μg/kg, and rocuronium bromide at 0.6 μg/kg was administered. Mechanical ventilation was performed by tracheal intubation and connected to an Ohmeda anesthesia machine with a flow rate of 2 L/min, tidal volume of 8 mL/kg, RR of 12 breaths/min, peak airway pressure <30 mmHg, and end-expiratory CO2 partial pressure of 35–45 cmH2O. The bispectral index (BIS) and hemodynamics were used to adjust the concentrations of propofol and remifentanil. The BIS was maintained between 40 and 60, and blood pressure was maintained at baseline ±10%.
Patients in the E1 group were treated with TEAS 1 day before surgery and before the induction of anesthesia. The Baihui, Shenting, bilateral Neiguan, and Hegu points were selected as the sites of electrical stimulation (According to the theory of acupuncture, Baihui and Shenting are on the head, Neiguan is on the wrists, and Hegu is on the palms). The patient's acupoints were cleaned with ethanol, after which non-dry gel electrode patches were applied to each acupoint and connected to an LH402 Korean transdermal acupoint stimulation device (Beijing Pukang Medical Technology Development Co., Ltd., China).
The stimulation method used a density wave of 2–100 Hz, with stimulation intensity starting at 4 mA and gradually increasing to the maximum stimulation that the patient could tolerate (adjusted between 4 and 15 mA). This was identified based on whether the patient experienced discomfort, including pain and unbearable numbness.
The E1 group received TEAS for 30 min before surgery, followed by conventional anesthesia to induce tracheal intubation, but no electrical stimulation was given for the rest of the procedure. The E2 group received no preoperative TEAS, only receiving it during the surgery until the skin was sutured. Point selection and instrument connection were the same as those in the E1 group. In group C, the electrodes were attached to the same acupoints, but no electrical stimulation was administered. Doctors performing TEAS were not involved in the evaluation of POD. Doctors involved in the evaluation of POD did not know the grouping of patients, which reduces the bias of the evaluation.
Blinding
The outcome evaluator blind method was used to separate researchers, evaluators, and statisticians. First of all, electrodes were affixed to the patients before induction of anesthesia, the on current or off current was carried out at the corresponding time according to the groups, and verbal hints were given to the patients in the process. All the patients were independently separated during evaluation to ensure the blindness of the patients. At the same time, TEAS was performed by a single physician, and the researchers performing clinical anesthesia, evaluation of POD, and statistical analysis of data were not aware of patient grouping information to ensure the implementation of the blind method.
Observation indicators
Safety index
Blood pressure, heart rate, and blood oxygen were monitored to evaluate safety.
Assessment of delirium
The confusion assessment method (CAM) was carried out on the first and fifth days after surgery and completed within 5 min. Four items in the CAM were assessed by a doctor. When items 1 and 2 were present, along with one of items 3 or 4, delirium was diagnosed. (1) Acute attack and fluctuating course: an acute change in the patient's mental state from baseline, or the patient's behavior fluctuated in the past day (the appearance or disappearance of symptoms, aggravated or weakened). (2) Inattention: it was difficult for the patient to concentrate, they were easily distracted, or they found it difficult to maintain a line of thinking. (3) Incoherent thinking: for example, concepts were unclear or illogically eloquent, or the patient unpredictably changed from one topic to another. (4) Consciousness changes: the patient's level of consciousness was abnormal, including vigilance, over-alertness, sleepiness, lethargy, or coma. Diagnostic requirements must meet both (1) and (2), and at least one of (3) or (4).
Anesthetic dose
The amount of propofol in patients and the plasma concentration of propofol during tracheal intubation.
Serological test
A total of 4 mL of venous blood was collected 1 day before surgery, 1 day after surgery, and 5 days after surgery. Each sample was added to a coagulation tube and allowed to stand at a low temperature for 30 min, and it was then centrifuged at 4000 revolutions/min for 10 min at a radius of 10 cm. The supernatant was stored in a refrigerator at −80°C, and the enzyme linked immunosorbent assay (ELISA) method was used to determine neuron-specific enolase (NSE), serum tumor necrosis factor-α (TNF-α), and interleukin-1β (IL-1β) concentrations.
Sample size calculation
According to the results of the pretest and previous reports, the incidence rate of delirium in the group C was 46% in the 5 days after surgery, whereas in group E1 and group E2 it was 20%; the significance level of the test was 5%, and the degree of confidence was 80%. Considering the 10% drop rate, the sample size was 148. Because fewer patients met the screening criteria and the enrolment was slow, the final sample size of each group was 20% of the calculated sample size (30 cases in each group).
Statistical processing
Statistical analyses were performed by using SPSS13.0 statistical software. Measurement data were expressed as mean plus or minus standard deviation (
Results
Screening
A consort diagram is shown in Figure 1. A total of 432 patients were screened, and 90 cases were included. Five cases fell off during the study, so 85 cases finally entered the analysis set.
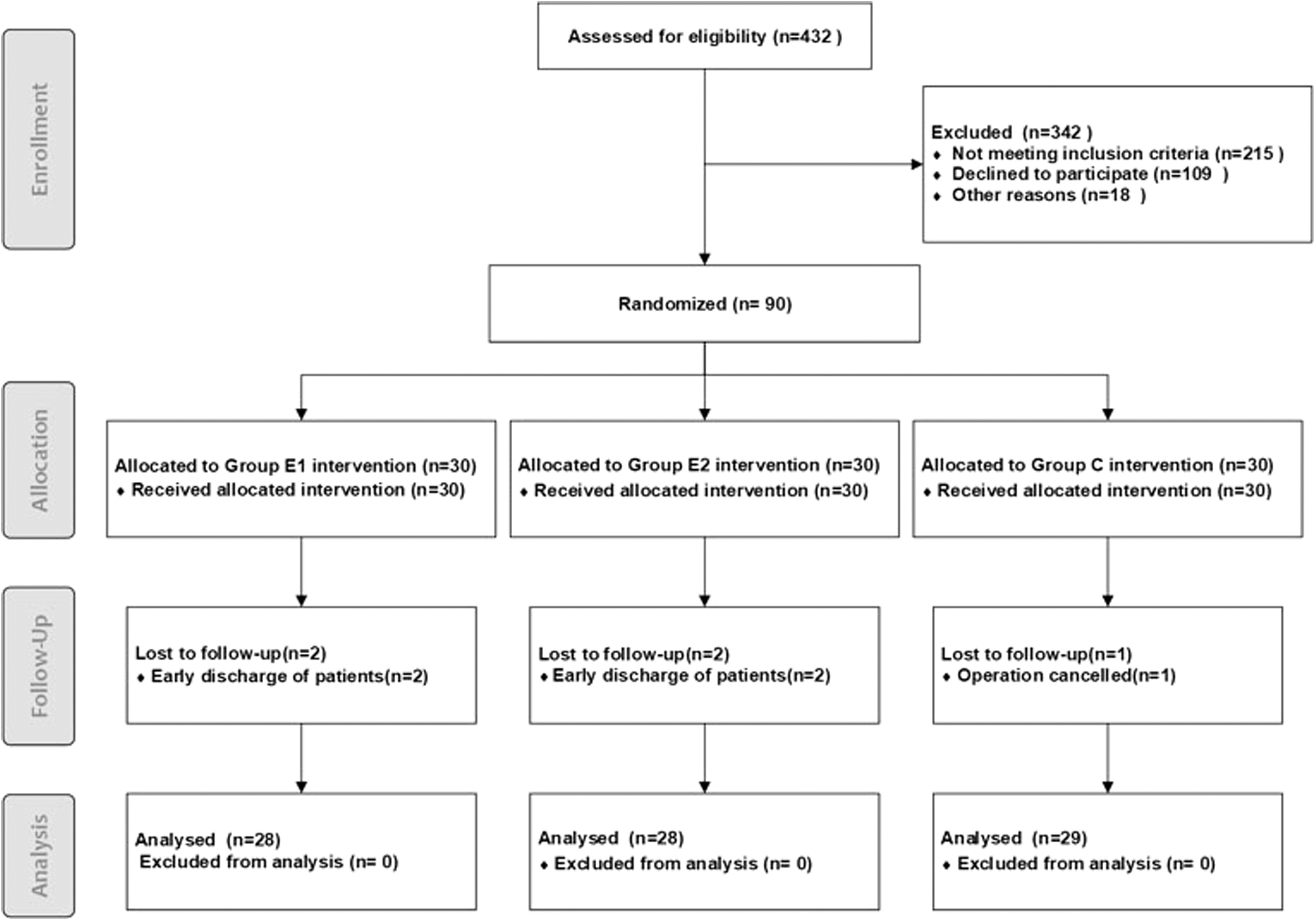
Consort diagram.
Safety indexes
The safety indexes included hypotension (mean arterial pressure <70 mmHg), hypertension (mean arterial pressure >105 mmHg), bradycardia (heart rate <50 bpm), tachycardia (heart rate >110 bpm), and hypoxemia (SpO2 < 90%). The incidence of hypotension was 6.7%, 6.7%, and 10% in the E1, E2, and C groups, respectively; the incidence of hypertension was 6.7%, 3.3%, and 3.3%, respectively; the incidence of bradycardia was 3.3%, 3.3%, and 0%, respectively; and the incidence of tachycardia was 0%, 3.3%, and 0%, respectively.
There was no hypoxemia in any of the groups. There were no significant differences in the earlier cited indexes between the groups (p > 0.05).
General conditions
There were no significant differences between the three groups in terms of age, weight, gender, composition ratio, and ASA composition ratio (all p > 0.05; Table 1). Further, there were no significant differences between the three groups in MMSE score, MNA score, BIS, Fried score, operation time, and volume of blood loss (Tables 2 and 3).
Comparison of Three Groups of General Situation (
ASA, American Society of Anesthesiologists.
Comparison of Three Groups of Cognitive Function (MMSE), Nutrition Status (MNA), Activity of Daily Living (BI), and Weakness (Fried) (
BI, bispectral index; MMSE, mini-mental state examination; MNA, mini-nutritional assessment.
Comparison of Three Groups of Amount of Blood Loss and Operation Time (
The incidence of delirium
The incidence of POD was an important observation index. In this study, there were significantly differences in the POD incidence among different groups. A total of 10 patients (33.3%) in group C, 4 patients (13.3%) in group E1, and 8 patients (26.7%) in group E2 developed POD within 5 days of surgery. Compared with group C, the incidences of delirium in groups E1 and E2 were reduced, and the difference was significant (p < 0.05).
Compared with group E2, the incidence of POD in group E1 was reduced, and the difference was significant (p < 0.05), suggesting that electrical stimulation before the induction of anesthesia can help reduce the occurrence of POD.
Concentration of propofol
Compared with group C, the plasma concentration of propofol and the dosage of propofol during tracheal intubation in group E1 decreased (p < 0.05). The concentration of propofol at BIS = 50 during the induction of anesthesia was 2.3 ± 0.3 μg/mL in group C, 1.8 ± 0.2 μg/mL in group E1, and 2.3 ± 0.3 μg/mL in group E2. Compared with groups C and E2, the plasma concentration of propofol in group E1 decreased during tracheal intubation (p < 0.05).
Serum concentrations of NSE, TNF-α, and IL-1β
We collected the serum concentrations of NSE, TNF-α, and IL-1β to evaluate the effect of TEAS. Compared with those on the day before the surgery, the serum concentrations of NSE, TNF-α, and IL-1β in the three groups increased 1 and 5 days after surgery (p < 0.05). Compared with group C, the serum concentrations of NSE, TNF-α, and IL-1β decreased in the E1 group 1 and 5 days after surgery (p < 0.05). Compared with group C, the serum concentration of TNF-α in group E2 decreased 1 and 5 days after surgery (p < 0.05). Compared with the E2 group, the serum concentrations of NSE and IL-1β in the E1 group decreased 1 day after surgery (p < 0.05) (Table 4).
Plasma Concentrations of NSE, IL-6, and TNF-α at Different Time Points (
p < 0.05 versus 1 day before operation.
p < 0.05 versus control group.
p < 0.05 versus E2.
IL, interleukin; NSE, neuron-specific enolation; TNF-α, tumor necrosis factor-α.
Discussion
The CAM is currently the most widely used delirium screening tool in the world. It has high sensitivity and specificity and is a suitable screening tool for non-psychiatric doctors and nurses. 19 In the present study, the degree of delirium was assessed on the first and fifth day after surgery. Based on a conversation with the patient and observations before and after the conversation, a doctor immediately evaluated the CAM at the end of the conversation to ensure its accuracy.
The evaluation showed that the incidence of delirium in group C was the highest, and the incidence of delirium in group E1 was the lowest. The difference between the groups was significant (p < 0.05), suggesting that TEAS can reduce the incidence of delirium and that it is better to administer it before the induction of anesthesia. Compared with those of group C and group E2, the plasma concentration of propofol in group E1 was the lowest at BIS = 50 intubation, indicating that electrical stimulation 30 min before the induction of anesthesia can reduce the target concentration of aesthetic drugs during intubation.
The latest research suggests that POD is closely related to the inflammatory response caused by surgical stress, in which the injured area directly releases various inflammatory mediators, activates body-fluid cascade systems, and causes the body's IL-1β, TNF-α, and other pro-inflammatory factors to increase. This reaction is closely related to the degree of damage caused by surgical trauma: The greater the surgical stimulation, the greater the body's inflammatory response. 20,21
As an important initiating factor, TNF-α can act on a variety of cells, trigger a series of cascade reactions at the cellular and subcellular levels, promote the accumulation and activation of leukocytes in inflammatory sites, and release a variety of inflammatory mediators. IL-1β is an important inflammatory mediator produced by monocytes and vascular endothelial cells. It can stimulate the proliferation of activated β cells and the production of immunoglobulins.
It can also stimulate the liver to produce acute-phase reactive proteins and to catalyze and amplify inflammatory reactions and toxic effects. Cytokines represented by IL-1β and TNF-α are involved in many neuropathological processes and play roles as triggering factors in the inflammatory response after cerebral ischemia and within a few days to a week after the onset. 22 As TNF-α can be affected by a variety of inflammatory factors and lacks specificity, the changes in IL-1β levels may be more related to the occurrence of POD.
NSE is a specific enolase in the neuronal cells of the brain. After craniocerebral injury, NSE is released into the intercellular space and cerebrospinal fluid or blood through the damaged blood–brain barrier. 23 The more severe the brain damage, the higher the damage to the blood–brain barrier and the greater the amount of NSE is released by neurons. Therefore, the measurement of NSE level can indirectly reflect the degree of central nervous system damage and is a specific biochemical indicator. 24
NSE can also be used as a biochemical indicator of neuronal damage, as an effective indicator for detecting the number of neuronal deaths, and as a direct marker of neuronal damage. 25 NSE presents obvious dynamic changes after central nervous system injury. After the acute phase, the level of NSE depends on the degree of brain injury. At the same time, post-traumatic ischemia and hypoxia can further aggravate brain injury. 26
In this study, we collected the serum concentrations of NSE, TNF-α, and IL-1β to evaluate the effect of TEAS. The results of this study show that TEAS could reduce serum concentrations of NSE, TNF-α, and IL-1β, and the effect of preoperative TEAS was better.
POD is accompanied by the potential neuronal disease of vascular dementia. It also has cognitive and memory dysfunction as a primary clinical manifestation, and its incidence increases with age. 27 In the field of traditional Chinese medicine, both cognitive and memory dysfunction can be attributed to dementia. As a product of the combination of traditional acupuncture and modern electrical stimulation techniques, TEAS has been widely used in various treatments, and its therapeutic effects have been confirmed by a large number of clinical and experimental studies. 28
Existing studies have shown that acupuncture at the Baihui, Neiguan, and Hegu points can be used to improve the cognitive function of patients with vascular dementia, and its mechanism is related to improving cerebral blood flow and brain metabolism and reducing nerve cell damage. 6,27 Electroacupuncture at the Baihui point has also been found to improve cognitive deficits, which may be induced by increasing cerebral blood flow and stimulating an anti-inflammatory effect. 29
Modern medical research has also confirmed that acupuncture at the Baihui point can improve blood circulation in the brain, repair neurons, enhance memory, and resist depression. In animal experiments, TEAS has been found to reduce the degree of cerebral oedema in rat models of cerebral ischemia and reduce the occurrence of postoperative cognitive impairment. Further, studies have found that 30 perioperative electroacupuncture can effectively reduce the incidence of delirium and its duration after hip replacement, but the timing and duration of the stimulation remain controversial topics.
The results of the present study showed that, compared with the day before surgery, the serum concentrations of NSE, TNF-α, and IL-1β in all three groups were increased 1 and 5 days after surgery (p < 0.05). This suggests that surgical trauma, anesthesia, and other stress can produce a strong peripheral inflammatory response, which promotes the production of inflammatory cytokines, which is consistent with the results of previous research. 2,25
Compared with group C, serum NSE, TNF-α, and IL-1β levels in the E1 group were significantly lower than in group C, suggesting that preoperative treatment with TEAS can inhibit postoperative inflammatory response and reduce brain injury. Compared with the E2 group, serum NSE and IL-1β levels were decreased in the E1 group 1 and 5 days after surgery, suggesting that, compared with TEAS being administered during surgery, TEAS being administered before the induction of anesthesia is more beneficial for the inhibition of postoperative inflammatory reaction and the reduction of brain injury.
The present study had some limitations. First, the number of cases in the study was small, which may cause bias in the results. Second, the study failed to further explore the correlation between the level of inflammation and the severity of delirium. Third, although we ensure the fairness of the assessment through the division of doctors, the blinding of patients was not sufficient, which may lead to the bias of results. In future studies, the sample size should be expanded and the blinding of patients should be ensured to explore the correlation between inflammation level and severity of delirium.
Conclusion
The TEAS can reduce the dosage of propofol required during surgery and the occurrence of delirium afterward. Its mechanism may be related to inhibiting inflammation response and alleviating brain injury. Compared with intraoperative application, the effect of preconditioning with TEAS before surgery is better. The results of this study have important significance for the clinical application of electroacupuncture in the prevention of POD.
Footnotes
Authors’ Contributions
Ruiling Zhou and Bo Yu performed the operation and wrote the manuscript; Shishun Kou and Hai Ke performed the operation and collected data; Yuhong Guo and Qi Wang analyzed the data and performed the statistical analysis; Lingling Ding and Jiaqi Ning designed and supervised the study, and revised the article. All authors have read and approved the article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University (No: 2017BL-025-02). All patients informed and agreed to participate in this study.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by “Capital characteristic” science and technology project of Beijing (No. Z171100001017061); Capital Chinese Medicine research special key project (No. 17ZY04); and Scientific research cultivation Program of Beijing municipal hospital (No. PZ2017028). CFH, (No. 2022-2-2232).
Supplementary Material
CONSORT Checklist.doc
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.