
Abstract
Objective:
An open-label placebo (OLP) is a placebo treatment in which the patient is aware that the treatment is a placebo. OLPs are considered effective for reducing pain, and previous studies have shown a stronger placebo effect for placebo acupuncture than for placebo pills. In this study, the authors compared the analgesic effects of OLP pills, OLP acupuncture, and a no treatment condition in healthy participants, and then examined the factors contributing to the OLP effect.
Design:
Randomized controlled crossover trial.
Settings/Location:
College of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea.
Subjects:
34 healthy participants.
Intervention:
Participants received three different treatments (“OLP-pill,” “OLP-acupuncture,” and “no treatment”) on three separate days in random order.
Outcome Measurements:
Before and after the treatment, heat pain stimuli were applied to the participants' hands, and pain tolerance, intensity, and unpleasantness were measured using a visual analog scale (range, 0–10).
Results:
Data of 31 participants were included in the analysis. The authors found significant analgesic effects of the placebo pill and placebo acupuncture in the OLP condition. Regression analyses revealed that expectations regarding treatment and practitioner identity influenced the analgesic effects of OLP acupuncture. There was no adverse event.
Conclusions:
Expectations regarding treatment and practitioner identity influenced the analgesic effect of placebo acupuncture without deception. These findings provide new information regarding the cognitive factors underlying pharmacologic and nonpharmacologic treatments.
Clinical Trial Registration Number:
KCT0004928.
Introduction
Placebos play an important role in medicine, mainly as control treatments in randomized clinical trials, and also as treatments with documented effects. 1 The use of placebos as treatments, without a patient's knowledge, has a two-century-long history. However, ethical issues have led to the development of open-label placebos (OLPs). 2 Although deception was previously regarded as an essential component of the placebo effect, recent studies have shown that placebos remain effective when patients are aware that they are receiving sham treatments. 3 Placebo administered without deception significantly improved symptoms in patients with irritable bowel syndrome. 4 Many studies have shown that OLPs led to improved symptoms for a range of conditions, including allergy-related rhinitis, depression, cancer-related fatigue, chronic lower back pain, and menopausal hot flushes. 5 –9 Furthermore, OLPs can have an analgesic effect in healthy participants undergoing experimental pain. Specifically, OLPs reduce subjected pain ratings (pain intensity and pain unpleasantness) and enhance pain tolerance. 10,11 Despite these findings, most previous studies used either placebo pills or placebo creams, and studies investigating the effect of OLP acupuncture (i.e., a nonpharmacologic treatment) have not yet been conducted.
Placebo acupuncture was originally developed as a control technique in acupuncture research. However, placebo acupuncture has been shown to produce an analgesic effect. 12,13 A previous randomized-controlled trial conducted on arm pain patients found that placebo acupuncture was more efficient in alleviating subjective pain and symptom severity, compared with placebo pills. 14 Another study comparing placebo pills, placebo acupuncture, and genuine acupuncture reported no association between the effect of placebo pills and the effect of placebo acupuncture. 15
Based on these findings, the authors suspected that the effects of OLP acupuncture (OLP-acu) and OLP pills (OLP-pills) might differ because placebo acupuncture involves tactile stimulation and thus may be perceived by participants as a more active treatment. 16 Furthermore, practitioner/patient interactions, touch, and needling pain associated with OLP-acu might lead participants to experience a sense of ritual, eliciting greater expectations regarding the outcome, compared with OLP-pills. 17 The therapeutic alliance between the practitioner and patient is very important to clinical care, and even associated with improvement of outcomes in chronic pain patients. 18 Enhanced patient/practitioner relationship, one of the placebo components, produced significant improvement of symptoms in patients with irritable bowel syndrome. 19 Thus, compared with OLP-pills, OLP-acu might produce a greater analgesic effect in an experimental pain condition. The authors presumed that participants who underwent OLP-acu would have greater expectations regarding treatment outcome, and would subsequently report greater analgesic effects, compared with participants who took OLP-pills.
The current study had two main hypotheses: (1) the analgesic effect of OLP would be present for participants who underwent OLP-acu and those who took OLP-pills, and (2) the characteristics of placebo acupuncture (e.g., tactile stimulation and practitioner/patient interaction) would be important factors contributing to the analgesic effect of OLP-acu. The authors also examined factors contributing to the OLP effect.
Materials and Methods
Participants
Participants were recruited through online advertisements titled “a study comparing placebo acupuncture with placebo pills.” Participants were right-handed, healthy, and 19–40 years of age. To include only participants who fully understood the description of the OLP, only native Koreans were enrolled. The authors excluded potential participants with any diseases that could interfere with the study evaluation (e.g., vascular disorder, use of anticoagulant agents, chronic or acute pain, diabetes mellitus, psychologic or psychiatric disorders, sensory abnormalities, cognitive impairments, or skin pathologies affecting the fingers), individuals who were pregnant, and medical students or health care workers. The participants were prohibited from smoking, drinking alcohol or caffeine, or taking any other drugs during the experiments. Cohen d was used to provide an effect size estimate (small d = 0.2, medium d = 0.5, large d = 0.8). The effect size d of placebo effect between the OLP group and control group was 0.43 based on the previous study, 10 and the authors estimated that ∼35 participants would be needed in each group for α level 0.05% and 80% power.
All participants received a detailed explanation of the study and provided written informed consent. This investigation was conducted in accordance with the guidelines issued by the Human Subjects Committee and was approved by the Institutional Review Board of Kyung Hee University, Seoul, Republic of Korea (Approval No.: KHSIRB-19-158). The study was registered with the Clinical Research Information Service (
Study procedure
This randomized-controlled crossover trial was conducted at the College of Korean Medicine, Kyung Hee University. The participants were required to visit the laboratory on three separate days (Fig. 1). On the first day, they were asked to complete a questionnaire that measured their psychologic state and expectations regarding the treatments. Subsequently, the participants were informed that they would receive OLP treatments, and pretreatment measurements were conducted. Pretreatment measurements were each participant's pain tolerance (objective outcome) and pain intensity/unpleasantness ratings (visual analog scale [VAS]; subjective outcome) after exposure to thermal pain stimuli. Electrocardiography was also conducted for 6 min.
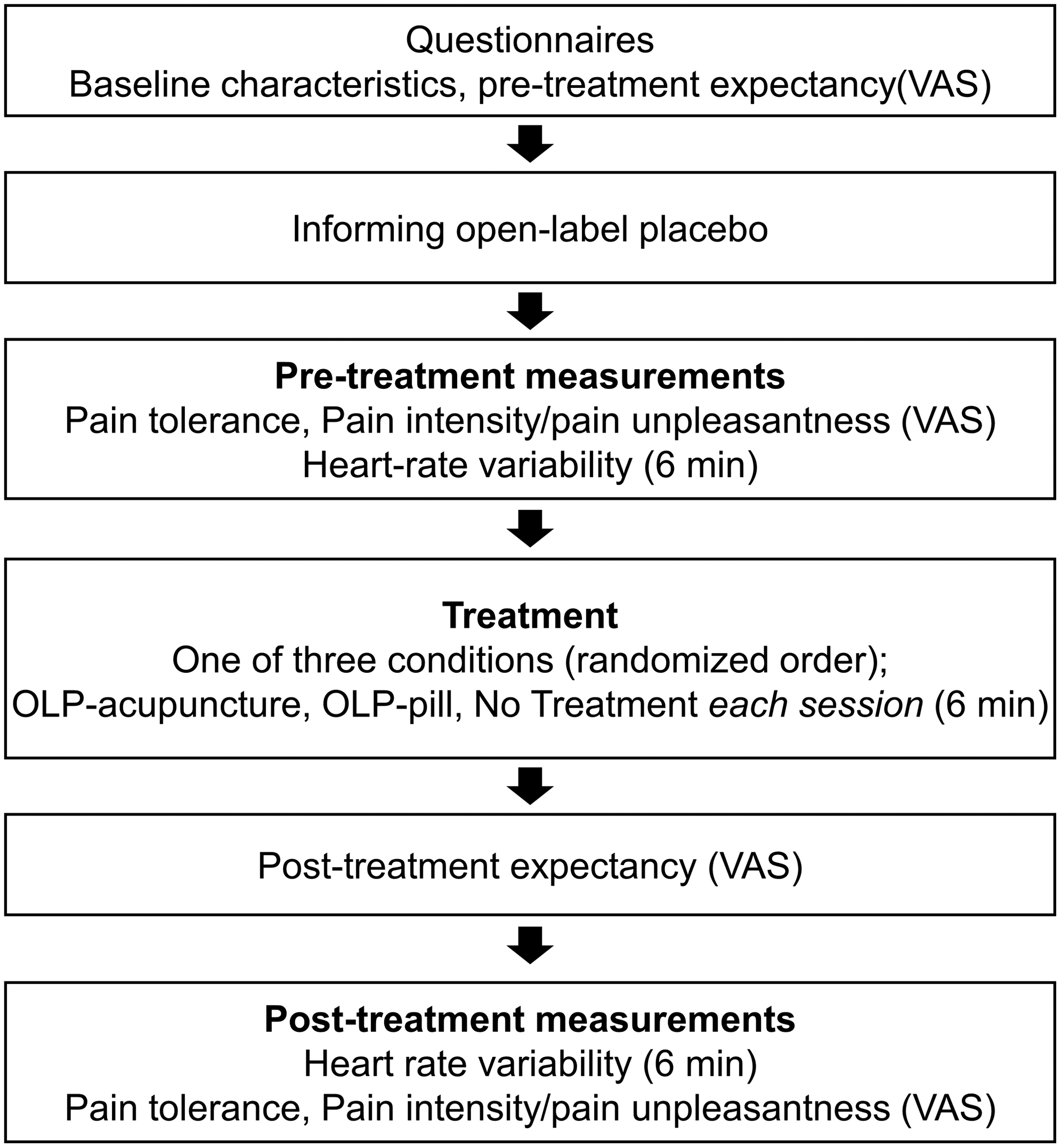
Experimental design. The procedure during one experimental day in sequential order. This procedure was repeated on three separate days. On each experimental day, participants received a different treatment session condition (randomized order). OLP, open-label placebo; VAS, visual analog scale.
There were three treatment sessions, each on a separate day. In each session, the participants received one of the two treatments (OLP-acu or OLP-pill) or no treatment (NT, as a control). The order of sessions was randomized. Each participant was randomized to one of the six condition orders (ACP, APC, CAP, CPA, PAC, PCA; A = OLP-acu, P = OLP-pill, C = control). The random allocation sequence was generated using the built-in random number generator in Microsoft Excel (Microsoft Corp., Redmond, WA) with a 1:1:1 allocation using block sizes of 6 (I.L.). The researcher enrolling participants (S.L.) was concealed from the allocation before actual enrollment. After consent, the researcher called a staff who was otherwise not involved in the study. Directly after the phone call, the staff opened a sequentially numbered opaque envelop and sent the allocation via text message to the researcher. This study was designed as an open-label trial, thereby blinding of treatment was not applied in this study. Instead, pain measurement was separately evaluated by the second author (D.C.).
Each treatment session lasted 6 min, and was conducted with the participants resting comfortably on a recliner chair. After the treatment session, the participants in the OLP-acu and OLP-pill conditions rated their post-treatment experiences. Following the 6-min treatment session, heart rate variability was measured for 6 min. Pain tolerance and pain intensity/unpleasantness were measured using methods identical to those conducted during pretreatment measurements.
OLP instruction
A practitioner informed the participants that they would receive a placebo treatment. Because OLPs with a plausible rationale are more effective, 10 participants were provided additional information regarding the OLP using the following text, which was modified from the instructions provided in previous OLP studies. 4,20 “You will receive a placebo needle that will not penetrate your skin and a placebo pill without any active ingredients. However, the placebo effect is powerful. For instance, pain ratings decreased by 30% in previous studies involving patients with irritable bowel syndrome and migraines. According to the classical conditioning theory, the body may automatically respond to placebos in a way that is similar to Pavlov's dogs, which salivated upon hearing a bell after they had been conditioned to associate the sound with food. Additionally, a positive attitude may enhance the placebo effect, although this is not necessary.” After the instructions had been provided, the participants were permitted to ask questions regarding the OLP.
Experimental conditions
As mentioned above, the participants received the three treatment conditions (“OLP-pill,” “OLP-acu,” and “no treatment”) on three separate days in a randomized order. Before each condition, the participants were reminded that all of the treatments were placebos and not genuine treatments.
For the “OLP-acu” condition, the participants underwent placebo acupuncture using a Park sham needle. 21 This device has a blunt needle, which enabled participants to see and experience sensations similar to those that occur during acupuncture without penetration of the skin. The needle was placed on the LI4 acupoint on the left hand, which is on the dorsum of the hand, radial to the midpoint of the second metacarpal bone. The practitioner rotated the needle for 10 sec. Afterward, the participants rested comfortably on a recliner chair for 6 min, and then the needle was removed. On removal, the participants were asked to evaluate the psychophysical characteristics of the DeQi (needle) sensations using the Acupuncture Sensation Scale.
For the “OLP-pill” condition, the participants were administered one placebo pill (Zeebo, South Burlington, VT). The placebo pill was free of active ingredients, and mainly contained microcrystalline cellulose. The participants were asked to consume the pill, and were provided a cup of water. Then they were asked to rest comfortably on a reclining chair for 6 min. In the “no treatment” condition, the participants were asked to rest comfortably on a reclining chair for 6 min.
Two practitioners administered the treatment sessions and each participant received all three treatment conditions by the same practitioner. To ensure equivalence between the conditions, the two practitioners practiced with each other to maintain concordance in terms of verbal/nonverbal expressions and the placebo acupuncture procedure.
Objective and subjective pain measurements
In this study, the authors defined subjective measurements as ratings solely based on subjects’ reports and objective measurements as pain tolerance, which were measured by pain response behavior quantitatively. To investigate the analgesic effects of OLP, responses to thermal pain applied were measured using a heat pain device (7360; Ugo Basile, Italy). This device was used in previous studies to measure the nociceptive threshold for an infrared heat stimulus applied to the fingers. 22,23 To prevent any harm from the heat stimuli, they set the device to a low intensity (IR 15) with a 30-sec cutoff time.
To minimize the researcher allegiance effect, 24 the thermal pain session was conducted by a staff member (D.C.) who was blinded to the experimental conditions and who had never met the participants before. Each participant placed his or her right index finger on the thermal sensor of the device. When the session began, a constantly increasing thermal stimulus was delivered to the participants, who were told to wait to remove their finger until they could no longer tolerate the pain. In this study, the authors measured the change of pain tolerance and investigated the changes of the escape-avoidance behavior response (i.e., finger withdrawal latency) as an index of objective marker.
The time latency until finger withdrawal was automatically counted in seconds, and the latency was used as a measure of pain tolerance. Furthermore, the participants rated the intensity and unpleasantness of the thermal pain stimuli using a VAS. The pain intensity VAS (ranging from 0 to 10) was shown on a 10-cm horizontal line anchored with “no pain” at the left and “worst imaginable pain” at the right end. Similarly, the pain unpleasantness VAS (ranging from 0 to 10) was presented on a 10-cm horizontal line with “no unpleasantness” on the left end and “worst imaginable unpleasantness” on the right end. The pain tolerance served as an objective assessment of pain. The pain intensity and pain unpleasantness were measures of participant-reported subjective pain. The thermal pain test was repeated on the middle finger of the same hand after a 3-min interval.
Heart rate variability measurement
To investigate the autonomic response of the OLP on pain modulation, heart rate variability measurements were analyzed. A meta-analysis study has demonstrated decreased high frequency in chronic pain, implicating a decrease in parasympathetic activation. 25 Systematic review on heart rate variability and experimentally induced pain also found that pain responses to nociceptive stimulation can be reflected by changes in autonomic reactivity such as decreased vagal-parasympathetic activity. 26 Before and after each treatment session, the participants underwent electrocardiography recording at rest for 6 min. Each participant sat on a reclining chair, and three electrodes were attached to his or her chest. Heart beat data were recorded using a data acquisition system (PowerLab 8/30 ML870; ADInstruments, Bella Vista, Australia).
The authors analyzed indexes of heart rate (beats/min) and heart rate variability using a low-frequency (LF) component (0.04–0.15 Hz) and a high-frequency (HF) component (0.15–0.40 Hz). The absolute powers of the LF and HF components were calculated in milliseconds squared (ms 2 /Hz) and, respectively, divided by the total power to measure each component as a percentage. The LF component reflects sympathetic nervous system activity and the HF component denotes parasympathetic (vagal) tone. 27,28 The LF/HF ratio, which is an estimate of the balance between sympathetic and parasympathetic activities, was calculated as the ratio of the powers of the LF and HF bands. 29
Questionnaires
Placebo responses are not the same across individuals. 30 Many psychosocial factors, such as optimism, are involved in individual differences in placebo analgesia. 31,32 To investigate psychosocial factors contributing to individual differences in placebo analgesia without deception, the authors attempted to build a model to predict the placebo response by combining potential psychosocial measurements.
On the first day of the study, the participants completed the Beck Depression Inventory to assess the intensity of depressive symptoms, 33 the Revised Life Orientation Test to assess optimism, 34 the State-Trait Anxiety Inventory (STAI-1, -2) to assess anxiety, 35 the Positive and Negative Affect Schedule (PANAS) to assess positive and negative moods, 36 Korean Multidimensional Assessment of Interoceptive Awareness (K-MAIA) to assess interoceptive awareness, 37 the Acupuncture Fear Scale to assess fear regarding acupuncture treatment, 38 the Acupuncture Expectancy Scale (AES) to assess general expectations regarding acupuncture, 39 and a pill expectancy questionnaire that was modified from the AES for this study.
The authors also measured expectations regarding placebo acupuncture and placebo pill (i.e., placebo acupuncture analgesia expectancy and placebo pill analgesia expectancy) with this question “How much do you feel that this therapy will help you to reduce your symptoms?” (using a VAS anchors 0%–100%) before the treatment sessions. They asked each participant whether he or she had previously received acupuncture or pills, and if he or she had, to state the number of experiences with each treatment. Among these questionnaires, the participants were asked to repeat the Beck Depression Inventory, STAI-1, and PANAS on the second and third day of the study. The post-treatment expectancy VAS was collected after the participants had received placebo acupuncture and placebo pill treatments, and the Acupuncture Sensation Scale was conducted after the placebo acupuncture treatment. At the end of each session, the participants rated their experience with the practitioner using a modified version of the Consultation and Relational Empathy (CARE) questionnaire. Specifically, the authors selected 5 of the 10 questions most closely related to the study objectives. 40
All participants were debriefed about the aims of the experiment. After completing the three sessions, participants were asked to guess whether they have received real treatments (real acupuncture or pills) or placebo treatments even though they were told that they received the placebo treatments (placebo acupuncture or pills) without deception. The authors carried out a qualitative interview study investigating how participants described their experiences receiving placebo pill or placebo acupuncture without deception. They will address the phenomenology of the OLP in a separate article.
Statistical analyses
To determine the analgesic effects in each condition, the authors used a 2 × 3 repeated-measures analysis of variance (ANOVA) to analyze pain outcomes, pain tolerance, and subjective pain ratings. Pain tolerance was the dependent variable, and time (pretreatment/post-treatment) and condition (OLP-acu/OLP-pill/NT) were entered as within-participants factors. Pretreatment differences versus post-treatment differences for each condition were evaluated using paired t-tests for pain tolerance. Paired t-tests were also conducted to evaluate differences in heart rate variability for each condition. To examine the effect of treatment order, differences in pain tolerance (Δ pain tolerance, post-treatment pain tolerance − pretreatment pain tolerance) were analyzed using one-way ANOVA with experimental day as the grouping variable. The authors applied the Benjamini/Hochberg (B-H) method to control the false discovery rate at level α.
Before the study, they made predictions regarding factors that they expected to contribute to the OLP-induced analgesic effect. To identify which factors could predict the analgesic effect, they designed a multivariate regression model with differences in pain tolerance (Δ pain tolerance, post-treatment pain tolerance − pretreatment pain tolerance) as the dependent variable. For statistical analyses, they used R version 4.0.3. Unless stated otherwise, all values correspond to means ± standard errors. p-Values <0.05 were considered statistically significant.
Results
Baseline characteristics
Participants were recruited from April 2020 to August 2020. The demographic characteristics of the 34 participants who completed all 3 experimental days are summarized in Table 1. Among the 37 participants who completed at least 1 day, 34 participants (age: 21.7 ± 0.40; 18 women) completed all 3 days of the study. Three participants did not complete the study due to scheduling issues (two participants) and voluntary withdrawal (one participant). The authors excluded data from three participants who had extremely high values for heat pain tolerance (>20 sec, mean ± 3 standard deviations). Thus, data from 31 participants were analyzed. They analyzed pretreatment pain tolerance by ANOVA to investigate the order effect and learning effect. Results showed that pretreatment pain tolerance did neither differ by condition (F = 0.295, p = 0.745) nor the day of study (F = 0.184, p = 0.832), thus indicating minimal order effect and learning effect.
Demographic and Baseline Characteristics of Participants
K-MAIA, Korean Multidimensional Assessment of Interoceptive Awareness; PANAS, Positive and Negative Affect Schedule; VAS, visual analog scale.
Expectancy ratings
VAS scores reflecting expectations were measured at baseline (pretreatment expectancy) and after each treatment (post-treatment expectancy). Paired t-tests showed no differences in pretreatment expectations between the OLP-acu and OLP pill (5.94 ± 0.46 vs. 5.90 ± 0.48, t = 0.12, p = 0.908). With regard to post-treatment expectancy, paired t-tests showed no differences between the OLP-acu and OLP pill (4.67 ± 0.46 vs. 5.09 ± 0.45, t = −0.87, p = 0.393).
Objective pain ratings
Two-way repeated-measures ANOVA showed a significant effect of time (F = 13.248, p < 0.05) and a significant time by treatment interaction (F = 3.708, p < 0.05) (Fig. 2). The paired t-tests for each condition showed significant differences between the pretreatment and post-treatment acupuncture (8.66 ± 0.46 vs. 9.55 ± 0.52, t = −2.44, p < 0.05, B-H corrected), and between the pretreatment and post-treatment pill (8.26 ± 0.35 vs. 9.80 ± 0.53, t = −4.16, p < 0.001, B-H corrected). However, there were no significant differences between the pretreatment and post-treatment NT (8.33 ± 0.37 vs. 8.83 ± 0.47, t = −1.62, p = 0.175, B-H corrected).

OLP analgesia. Repeated-measures ANOVA revealed a significant effect of time (F = 13.248, p < 0.05) and a time by condition interaction (F = 3.708, p < 0.05). Significant differences before versus after treatment were found for OLP acupuncture (OLP-acu) and OLP pills (OLP-pills), but not in the control condition (NT). Each box plot shows the interquartile range, and horizontal lines indicate the median pretreatment and post-treatment scores. *p < 0.05, ***p < 0.001. ANOVA, analysis of variance; NT, no treatment; OLP, open-label placebo.
Subjective pain ratings
Subjective pain ratings were measured using the VAS to assess pain intensity and unpleasantness (Table 2). For pain intensity, two-way repeated-measures ANOVA revealed a significant pretreatment versus post-treatment difference (F = 22.51, p < 0.001) and a marginal effect of the time by condition interaction (F = 3.02, p = 0.056). When repeated-measures ANOVA was conducted with pain unpleasantness as the dependent variable, the effect of time was significant (F = 29.51, p < 0.05) and the time by condition interaction also had a significant effect (F = 7.27, p < 0.01) on pain unpleasantness.
Pain Intensity and Pain Unpleasantness Pretreatment Versus Post-Treatment, Measured via Visual Analog Scale
OLP, open-label placebo; VAS, visual analog scale.
Heart rate variability
Paired t-tests showed significant decreases in heart rate after treatment in all three conditions (OLP-acu, 68.8 ± 1.8 vs. 66.8 ± 1.7, t = 3.565, p < 0.05; OLP-pill, 67.9 ± 1.7 vs. 66.6 ± 1.5, t = 2.552, p < 0.05; NT, 68.7 ± 1.5 vs. 67.2 ± 1.5, t = 2.550, p < 0.05). In terms of the LF/HF ratio, an increase was present after the NT (1.4 ± 0.3 vs. 1.5 ± 0.3, t = −0.286, p = 0.777), but values decreased after both the OLP-acu (1.2 ± 0.2 vs. 0.9 ± 0.1, t = 1.688, p = 0.102) and OLP-pill treatments (1.1 ± 0.3 vs. 0.8 ± 0.1, t = 1.020, p = 0.316). However, these tendencies were not statistically significant.
Prediction of factors contributing to the OLP effect
Table 3 shows the results of the multivariate regression model predicting the OLP effect in the OLP-acu condition (R 2 = 0.519). Participants with a higher AES score had a greater OLP effect after sham acupuncture (β = 0.531, p < 0.05). In addition, the practitioner significantly contributed to the analgesic effect in the OLP-acu condition (β = 1.442, p < 0.05), indicating a difference between practitioners. The authors conducted analyses using the same multivariate regression model for the OLP-pill, but found that none of the factors significantly explained the OLP effect (R 2 = 0.331).
Multivariate Regression Model Predicting Open-Label Placebo Effect in Open-Label Placebo Acupuncture
K-MAIA, Korean Multidimensional Assessment of Interoceptive Awareness; PANAS, Positive and Negative Affect Schedule.
Adverse effects
No adverse events were reported during the trial.
Discussion
This crossover study involving healthy participants investigated the OLP effect of sham acupuncture and placebo pills. Compared with the NT condition, OLP-acu and OLP-pill were effective in terms of both objective outcome (increased pain tolerance) and subjective outcome (lower pain intensity/unpleasantness). These results suggest that OLPs can effectively produce objective outcomes, in contrast to the findings of previous OLP studies that have mainly demonstrated subjective/self-reported outcomes in patients with clinical conditions. 10 For example, a recent study involving patients with chronic back pain that measured both objective and subjective outcomes reported significant OLP effects only in terms of patient-reported subjective outcomes (i.e., pain and disability ratings). 20 Moreover, in OLP studies involving the application of experimental pain to healthy individuals, Locher et al. showed meaningful results in terms of subjective pain relief and Kube et al. showed an increase in pain tolerance. 10,11 Thus, the present study provides a unique contribution to the body of knowledge regarding the analgesic effects of OLPs.
Although this is the first trial to compare OLP-acu and OLP-pills, previous studies involving deceptive placebos have explored the combined effects of sham acupuncture with a placebo pill. Consistent with the previous studies, they initially hypothesized that the effect of OLP-acu would be greater than the effect of OLP-pills. Kaptchuk et al. compared placebo acupuncture with placebo pills in patients with arm pain to examine whether an invasive treatment (i.e., placebo acupuncture) would have a stronger placebo effect than placebo pills. They found that placebo acupuncture had greater analgesic effects on patient-reported pain and symptom severity. 14 Moreover, a systematic review comparing the effectiveness of different placebo treatments on migraines showed that elaborately designed placebo methods (e.g., sham acupuncture and sham surgery) had stronger treatment responses, compared with orally administered pharmacologic placebos. 41 However, in contrast to the initial hypothesis, the authors found no prominent effects of OLP acupuncture in this study. As mentioned above, placebo acupuncture is conducted using an intricately designed sham device that induces substantial tactile sensations, thus increasing the probability that participants will perceive the placebo as a real treatment. 16 In this regard, the authors additionally asked participants to guess whether their treatments were real or placebo. Since, all participants were well informed that their treatments were placebo, only 5 out of 31 subjects guessed OLP-acu to be real and 6 subjects guessed OLP-pill to be real. Interestingly, there were no differences in the credibility between OLP-pill and OLP-acu, even if tactile stimulation was involved in the OLP-acu group. However, the tactile components of OLP acupuncture in the present study may have played a different role from those in placebo acupuncture because the participants were already aware that the treatment was not genuine.
Regarding the factors related to each OLP effect, the authors found that both expectations regarding acupuncture and practitioner identity influenced the analgesic effect of OLP-acu. However, multivariate regression analyses did not demonstrate any factors influencing the analgesic effect of the OLP-pill. In terms of the role of expectations in placebo acupuncture, Kong et al. previously reported that high expectations regarding the efficacy of placebo acupuncture induced a significant reduction in subjective pain, and that brain activity during placebo acupuncture differed from brain activity during verum acupuncture in analgesic circumstances. 42 Despite these findings regarding expectations, a recent OLP study suggested that, compared with expectations, despair and desire for relief might be more closely related to the effects of OLPs. In that study, expectations in a lay population were greater for deceptive placebos than for OLPs. Thus, participants exhibited greater acceptance of deceptive placebos, and were less confident regarding OLPs. 43 Likewise, the authors found a significant effect of acupuncture expectancy (as indicated by the AES score), but no effect of placebo acupuncture expectancy. Overall, general expectancy regarding acupuncture therapy was able to predict the OLP-acu effect, but expectancy regarding placebo acupuncture could not explain the OLP-acu effect. Thus, they predict that expectancy is involved in OLPs, although general expectancy regarding acupuncture made a difference in terms of pain tolerance, whereas expectancy regarding OLP did not.
Along with the effects of expectancy, these results showed a significant effect of practitioner identity in the OLP-acu condition (Table 3). Post hoc analyses revealed a significantly different pain tolerance difference (Δ pain tolerance, post-treatment pain tolerance − pretreatment pain tolerance) between the two practitioners (1.21 ± 0.59 vs. 0.50 ± 0.38, t = −2.276, p < 0.05). When they further analyzed differences in pain reduction by comparing the CARE and acupuncture sensation values, they found no significant differences in CARE (22.9 ± 0.79 vs. 21.6 ± 1.16. t = 0.910, p = 0.370) and Acupuncture Sensation Scale scores (1.44 ± 0.40 vs. 1.39 ± 0.341, t = 0.090, p = 0.929) between the two practitioners, which implies that the extent of care provided and acupuncture sensations felt were equivalent. Remarkably, this practitioner effect was only present in the OLP-acu condition. The authors assume that this difference originated from the details of the interaction during the acupuncture procedure. The practitioners were more involved during the OLP-acu condition. Specifically, they were required to be gentle when searching for the precise acupoint in the participant's hand, applying the sham needle device, and rotating the needle. Thus, the practitioner effect in the OLP-acu condition may have been induced by subtle technical differences in how the two practitioners conducted the OLP-acu procedures, and were not directly related to either the CARE score or the acupuncture sensations. Previous researchers have proposed that C tactile processing may explain the influence of affective-social touch during acupuncture. 44,45 C tactile afferents respond to light skin-to-skin contact between individuals, and are involved in the emotional elements of tactile stimulation. 46 Consistent with these studies, the authors suspect that the social-tactile aspect of acupuncture may explain these results regarding the effect of practitioner in the OLP-acu condition alone. Because they did not measure C tactile processing, further studies are needed to investigate the roles of affective and social touch in analgesia during acupuncture.
The level of established rapport between practitioners and participants might interact with OLP. In the current study, two practitioners showed different levels of placebo effect in the acupuncture session, even though they were asked to explain the instruction and to deliver the pill or sham acupuncture in a standardized procedure. However, nonverbal cues, such as including bodily expressiveness and evocative symbols, might be associated with the level of trustworthiness of practitioners and influence on the doctor/patient relationship. 3 Further study is necessary to investigate the interaction between the doctor/patient relationship and the OLP effect. Due to the limited resources, the authors did not record the video during participant/practitioner interactions in this study. Thus, they were not able to further analyze the additional data on practitioner/patient interaction. Recently, an fMRI study using hyperscanning in patient/clinician dyads has shown that patient analgesia can be mediated by patient/clinician nonverbal behavioral mirroring and brain-to-brain concordance in circuitry associated with theory of mind and social mirroring. 47 It will be more interesting to investigate nonverbal behavioral mirroring during practitioner/participant interaction between OLP-pills and OLP-acupuncture conditions in the future.
Kaptchuk has recently proposed that Bayesian brain and embodied cognition would be more appropriate models for understanding OLP. 3 According to Bayesian model, brain can predict the upcoming sensory inputs and minimize error by continuously updating prior knowledge. 48 Pain perception can be regarded as a process of prediction, based on an integration of bottom-up sensory signals, top-down expectation of prior experience, and contextual cues. 49 Pain relief by medical ritual can be considered the brain process that interprets interoceptive changes in the body as a consequence of healing. 50 In their previous study, the authors found that Bayesian modeling can predict placebo analgesia in a simulated clinical situation. 51 When patients are honestly told that they are receiving a placebo, their body might respond unconsciously under the embodied assumption of medication taking. 50 Even in a placebo condition without deception, brain minimizes prediction error and individuals tend to experience pain relief because embodied pill-taking behavior or needling is given in the context of medical intervention. 3 Within the framework of predictive coding, it is expected that patients can experience pain reduction in OLP condition, in which placebo pills or placebo acupuncture are honestly prescribed.
This preliminary study comparing OLP acupuncture and OLP pills had some limitations. First, all participants were healthy individuals and the experimental setting did not reflect a real clinical environment. Although the mechanisms of OLPs have not yet been fully revealed, the effect appears to involve conditioning, expectancy, and the patient/health care provider relationship. 3,52,53 Because this experimental design included healthy participants, the authors might have observed psychologic processes distinct from those that would be expected in a clinical setting. Indeed, a recent OLP study with healthy individuals suggested that healthy individuals may be more skeptical regarding OLP. 11 Second, they did not observe any significant results related to heart rate variability except a decrease in heart rate in all conditions, which might have been due to the resting state during which the heart rate was measured. 54 Therefore, future studies should measure neurophysiologic signals (e.g., brain activity) to reveal the mechanisms underlying OLP-induced analgesia. In addition, to measure truly objective measures in pain threshold, it will be more appropriate to evaluate sensory nerve function by determining current perception threshold. Due to the limited resources, the authors did not include the measurement of Neurometer CPT/C in this study.
This crossover design study was performed to compare OLP-acu and OLP-pills. In this novel study to compare the open-label effects of two placebo treatments, they found that both the OLP-acu and OLP-pill had an analgesic effect. To exclude other effects, they kept all conditions equivalent except for the treatment device. A recent study by Blease et al. produced recommendations regarding the design of OLP trials. 24 This study was performed in accordance with the recommendations: the authors constructed a control condition that was equivalent to the other conditions and included an independent blinded assessor who measured the primary outcome to avoid researcher bias. Although this was a preliminary study, these results showed that OLP-acu has potential applications in alleviating pain. Further research involving patients with chronic pain may lead to more promising results. For instance, OLP-acu may be useful in clinical settings for patients who should not undergo acupuncture.
Conclusions
In conclusion, the authors found a potential analgesic effect of OLP in terms of both placebo acupuncture and a placebo pill. Furthermore, they found that expectations regarding treatment and practitioner identity influenced the analgesic effect of placebo acupuncture without deception. These findings help to explain how different psychosocial factors are involved in pharmacologic and nonpharmacologic treatments, as well as between open-label and conventional placebo treatments. Although further research is required, these findings suggest that both placebo acupuncture and placebo pills could be used to reduce pain as possible supplementary interventions (e.g., in patients afraid of needle insertion) without patient deception. However, more clinical research is needed to obtain evidence of the OLP effect.
Footnotes
Authors’ Contributions
S.L. and Y.C. designed the study. S.L, D.H.C., and M.H. performed the trial. S.L. and I.S.L. performed the statistical analysis. S.L. and Y.C. wrote the first draft of the article. All the authors reviewed and approved the article.
Data Availability Statement
Data available on request from the authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (No. 2021R1F1A1046705, No. 2020R1A4A1018598, and No. 2020R1A5A2019413). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.