
Abstract
Objectives:
To assess the efficacy and safety of Eucalyptus globulus Labill (Eucalyptus) on cough.
Background:
Cough is a common symptom of upper respiratory tract infections (URTIs) and bronchitis. Eucalyptus products are frequently used as over-the-counter cough medications but their efficacy and safety are uncertain.
Methods:
Randomized controlled trials (RCTs) investigating efficacy and safety of Eucalyptus for cough were systematically searched in electronic databases till February 2021. Two reviewers independently performed study selection, data extraction, and quality assessment. Clinical outcomes including improvement or resolution of overall cough symptoms, cough frequency (CF), and adverse events (AEs) of Eucalyptus were evaluated and analyzed using a random-effects model. Heterogeneity was evaluated using I2 and chi-squared test.
Results:
Six RCTs with 1,857 participants with cough were included in this study. Most of the included studies used Eucalyptus in combination formula (four of six studies). Based on Cochrane's risk of bias criteria, three of six studies (50%) were rated low risk of bias, whereas the remaining were judged as high risk of bias. This study found that Eucalyptus products are more effective than placebo in terms of improvement or resolution of overall cough symptoms with relative risk 1.45 (95% confidence interval (95% CI) 1.26–1.67). Whereas all Eucalyptus formulae reduced CF with weighted mean difference 0.44 (95% CI 0.28–0.60), when compared with placebo. There are no serious AEs associated with Eucalyptus during treatment periods. Mild-to-moderate gastrointestinal symptoms were common AEs reported in a comparable study between Eucalyptus and control groups.
Conclusion:
The findings indicate that Eucalyptus products are safe for use in cough related to respiratory diseases such as URTIs and bronchitis. However, their efficacy is minimal and of uncertain clinical importance. Further high-quality studies are still necessary to confirm this finding.
Introduction
Cough is a common and troublesome symptom in both children and adults worldwide. 1,2 It results in personal health, quality of life, and economic problems. In year 2004, there were 26 million office visits of patients with cough in the United States. 3 In Australia and the United States, acute cough is the fifth of common reasons for treatment in ambulatory care with 10 ambulatory visits per 1,000 visits each year, whereas in the United Kingdom, there are about 50 cases per 1,000 people each year. 4 In the United Kingdom, economic effect of cough has been estimated to be £979 million including loss of productivity cost (£875 million) and health care cost (£104 million). Furthermore, the cost of all treatments for cough has been estimated to be £104 million from a government report in 2001. 5
Cough is an important defensive reflex for protecting against foreign substances to the lower airways. 5 Based on duration of symptoms, cough can be classified into three types: acute, subacute, and chronic cough. Duration of each type of cough was <3, 3–8, and >8 weeks, respectively. 6 The most common causes of acute cough are bronchitis and upper respiratory tract infections (URTIs) including common cold and acute bacterial sinusitis, whereas chronic cough can be caused by a number of chronic respiratory diseases such as chronic obstructive pulmonary disease (COPD) and asthma. 7 The prevalence of cough in patients having URTIs varies between 9% and 64%, whereas 50% of patients having sore throat have cough symptom. 8
Cough was treated to the specific disease- and symptom relieved by using antitussive. Early treatment of cough could prevent or stop the cycle of cough. Currently, several therapeutic options are available for relieving cough symptoms. 1,9 However, there is no agreement on the current treatments. 10,11 This led many researchers to investigate the efficacy of other remedies for relieving cough such as Andrographis paniculate, ivy/primrose/thyme, and Eucalyptus. 12
One of the main treatment modalities traditionally is herbal medicine. Complementary and alternative medicine is increasingly used among the general population. Clinical evidence of efficacy and safety of herbal products has increased, leading higher confidence of people consuming these products. 13,14 Eucalyptus globulus or Eucalyptus citriodora or commonly named “Eucalyptus” is an important herb providing essential oil named “Eucalyptus oil.” The main active component of Eucalyptus oil is 1-8-cineol (citronellal). Eucalyptus is of interest for its pharmacologic effect such as antibacterial, antiviral, antifungal, anti-inflammatory, and insect-repellent properties. It is being used as cosmetic, pharmaceutical, and nutraceutical agents. It also has been widely used in several conditions such as cough, common cold, influenza, and other respiratory diseases. 15,16 In Lao PDR, Eucalyptus syrup containing Eucalyptus oil, potassium sulfoguaiacolate, sodium camsylate, and Mentha arvensis oil is listed as one of the herbal medicines for cough in the national list of essential medicines. 17 Although Eucalyptus has been widely used for a long time, there is no strong evidence to support its efficacy and safety for relieving cough in humans. Therefore, a systematic review and meta-analysis of relevant randomized controlled trials (RCTs) were conducted to evaluate the efficacy and safety of Eucalyptus for relieving cough symptoms.
Methods
A systematic review and meta-analysis were conducted following the Cochrane Collaboration guidelines, 18 and this review was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 19 The registration number of the systematic review on PROSPERO was CRD42019131504.
Systematical search and study selection
The studies on Eucalyptus used for cough were searched from its inception to February 2021, through the PubMed, Scopus, Cochrane Library, Embase, CINAHL, Science Direct, ProQuest, and Thai Library Integrated System (ThaiLIS) databases. The RCTs evaluating the clinical effects of Eucalyptus for relieving cough symptoms were searched without language restrictions. Strategic search terms were used in the following Boolean format: “cough (MeSH)” AND (“bronchitis” OR “common cold” OR “respiratory tract infection” OR “upper or lower respiratory tract infection” OR “pneumonia” OR “chronic pulmonary diseases or pulmonary disease” OR “chronic obstructive pulmonary disease” OR “respiratory dysfunction” OR “flu or influenza”) AND (“Eucalyptus” OR “cineole”) AND (“randomized controlled trial” OR “clinical controlled trial”). The references lists of selected articles were assessed to identify potential studies not included in the selected databases.
The articles were included if they were RCTs evaluating the clinical effects of any Eucalyptus formulation on cough in patients having upper or lower respiratory tract infection, bronchitis, and diseases related to respiratory tract infection such as acute exacerbation of COPD. Studies investigating effect of Eucalyptus on cough caused by chronic disease including lung cancer, tuberculosis, severe pneumonia, known immune deficiency, postextubating, and pulmonary fibrosis were excluded.
One independent reviewer (L.H.) initially screened the titles and abstracts of all retrieved articles, then other investigators (R.S. and J.K.) reviewed selected articles to confirm. The full texts of potentially eligible articles were then independently examined by two investigators (L.H. and J.K.) to choose those that fulfilled the eligibility criteria. Discussion with R.S. and N.C. was used to resolve disagreements of study selection between L.H. and J.K.
Data extraction and quality assessment
One investigator (L.H.) independently extracted the data, then another investigator (J.K.) confirmed the data independently. Discussion with a third investigator (R.S. or N.C.) was used to resolve disagreement between L.H. and J.K. This strategy was also performed for the quality assessment process. The standardized data extraction form was used to obtain the following data from all included articles: author, publication year, study design, intervention or patient characteristics, sample size, treatment duration, and outcome.
The same process that was used in data extraction was used to evaluate the quality of each included study. The Cochrane risk of bias 2.0 tool 20 was used for this. This tool examines five major sources (domains) of bias including the randomization process, intended intervention deviations, missing outcome data, outcome measured, and reporting selective outcome. The risk of bias in each study was judged, against each source as low, high, or some concern risk of bias. The overall risk of bias for each outcome (across domains) within studies was rated as low risk of bias, if all domains were assessed as being at low risk of bias, whereas the outcome was rated as some concern risk of bias if at least one domain is classified as being some concern risk. Overall risk of bias was rated as high risk of bias if at least one domain is judged as being at high risk.
Discussion with a third investigator (R.S. or N.C.) was used to resolve disagreement between L.H. and J.K. If possible, the authors were contacted to get the missing data.
Outcome measure and statistical analyses
The primary outcome was clinical efficacy defined as proportion of patients who achieved improvement or resolution of overall cough symptoms. Improvement or resolution of overall cough symptoms was evaluated using a verbal rating scale (VRS) ranging from 0 to 3 (VRS: 0 = no cough or cured, 1 = cough symptom improved from baseline, 2 = cough symptom unchanged from baseline, 3 = cough symptom worsening from baseline). This evaluation incorporated all perceptions of cough including intensity or severity, frequency, and quality of cough at the same time of assessment, so overall cough symptoms were called. Responder is a patient with improvement or resolution of overall cough symptoms (VRS = 0 or 1). Secondary outcomes were frequency and severity of cough, quality of cough, and adverse events (AEs). Each outcome of interest was pooled separately. For binary outcomes such as proportion of patients who achieved improvement or resolution of overall cough symptoms, pooled effect was present as a relative risk (RR) with 95% confidence interval (95% CI). Pooled effect of continuous outcome was expressed as weighted mean difference (WMD). The chi-squared test and I2 were used to assess heterogeneity between included studies. p-Value <0.05 was considered as significant difference for heterogeneity test. I2 of 50% or above was considered as high heterogeneity. 21 When there was evidence of high heterogeneity, it as attempted to explore the reasons for heterogeneity. If data are sufficient, subgroup analyses were performed. Egger test and funnel plots were used to assess small study effect in meta-analysis. 22,23 The Dersimonian and Laird random-effects model 24 was used for all analyses.
Sensitivity and subgroup analyses
Sensitivity analysis by included only high-quality trials (trials with low risk of bias) was performed to ensure robustness of results. If data are sufficient, types of comparators, age of patients, dosage form of Eucalyptus, and duration of follow-up data were used for subgroup analyses.
Results
The 340 related articles were identified from database search and other sources. After duplication removal, 201 articles were screened by title and abstract. Twenty-five RCTs were selected for full text review, then 19 RCTs were excluded because they did not study the effect of Eucalyptus on cough. Therefore, six RCTs 25 –30 were included in this review (Fig. 1).

PRISMA flow chart of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The summarized characteristics of all studies are provided in Table 1. Six studies with 1,866 participants with cough (870 were males and 996 were females) were included. Among six studies, one study was conducted in Israel 25 and five studies were conducted in Germany. 26 –30 All studies were multicenter double-blind randomized controlled trials. Only one study had sample size of fewer than 100 patients. 25 The average age of the included patients was 44.85 years with a range from 18 to 83 years. The major causes of cough were bronchitis, 26 –29 followed by URTI 25 and acute exacerbation of COPD. 30 Four studies used Eucalyptus in combination formula whereas only two studies used pure Eucalyptus extract (cineole 200 mg 3 times/day). 26,30 Among the combination formula studies, three studies used Eucalyptus oil mixed with essential oil from lime (Citrus aurantifolia) and pine (Pinus spp.) 300 mg for 3–4 times/day, 27 –29 whereas the remaining studies used Eucalyptus oil mixed with aromatic oil spray 12 mcg for 4–5 times/day. 25 All studies used placebo as a control group. Treatment durations of most studies were <30 days, 25 –28 ranging from 325 to 180 days. 29,30 The main outcome measurements were cough frequency (CF) and AEs, 26 –30 followed by overall effect. 25,27 –29 Measurement time was varied from 3 to 180 days. However, data were insufficient to determine long-term effects (treatment duration >30 days), thus measurement time used for data analysis of efficacy outcomes ranged from 3 to 30 days.
Characteristics of Included Studies
Mixed aromatic oil spray containing 20% Eucalyptus globulus, 10% Eucalyptus citriodora, 20% Rosmarinus officinalis, 30% Origanum syriacum, 20% Mentha piperita.
Myrtol or Gelomyrtol capsule containing of essential oil from E. globulus, Pinus spp. (pine), Citrus aurantifolia (lime).
CF, cough frequency; CS, cough severity; COPD, chronic obstructive pulmonary disease; DB, double blinded; N/A, data not available; QS, quality of sleep; RCT, randomized controlled trial; URTIs, upper respiratory tract infections.
The quality of each included study is summarized in Table 2. Based on risk of bias version 2.0 assessment, half of six RCTs were judged as low risk of bias, 25 –27 whereas others were judged high risk of bias. Missing outcome data 28,29 and bias in selection of the reported result 30 were the main reasons for the judgment of high risk of bias.
Risk of Bias Assessment of Included Randomized Controlled Trials
Four studies 25,27 –29 with 1,395 patients reported effect of benefit of Eucalyptus in terms of proportion of patients who achieved reduction of overall cough symptoms. Main analysis of this outcome is shown in Figure 2. This meta-analysis revealed that Eucalyptus had a statistically significant effect on achieving improvement or resolution of overall cough symptoms compared with placebo (n = 1,061, RR: 1.45, 95% CI 1.26–1.67, p-value <0.001), with no evidence of heterogeneity (I 2 = 0.00%; p-value = 0.421). However, the effect of Eucalyptus was not significantly different when compared with active control such as cefuroxime and ambroxol (Fig. 2).
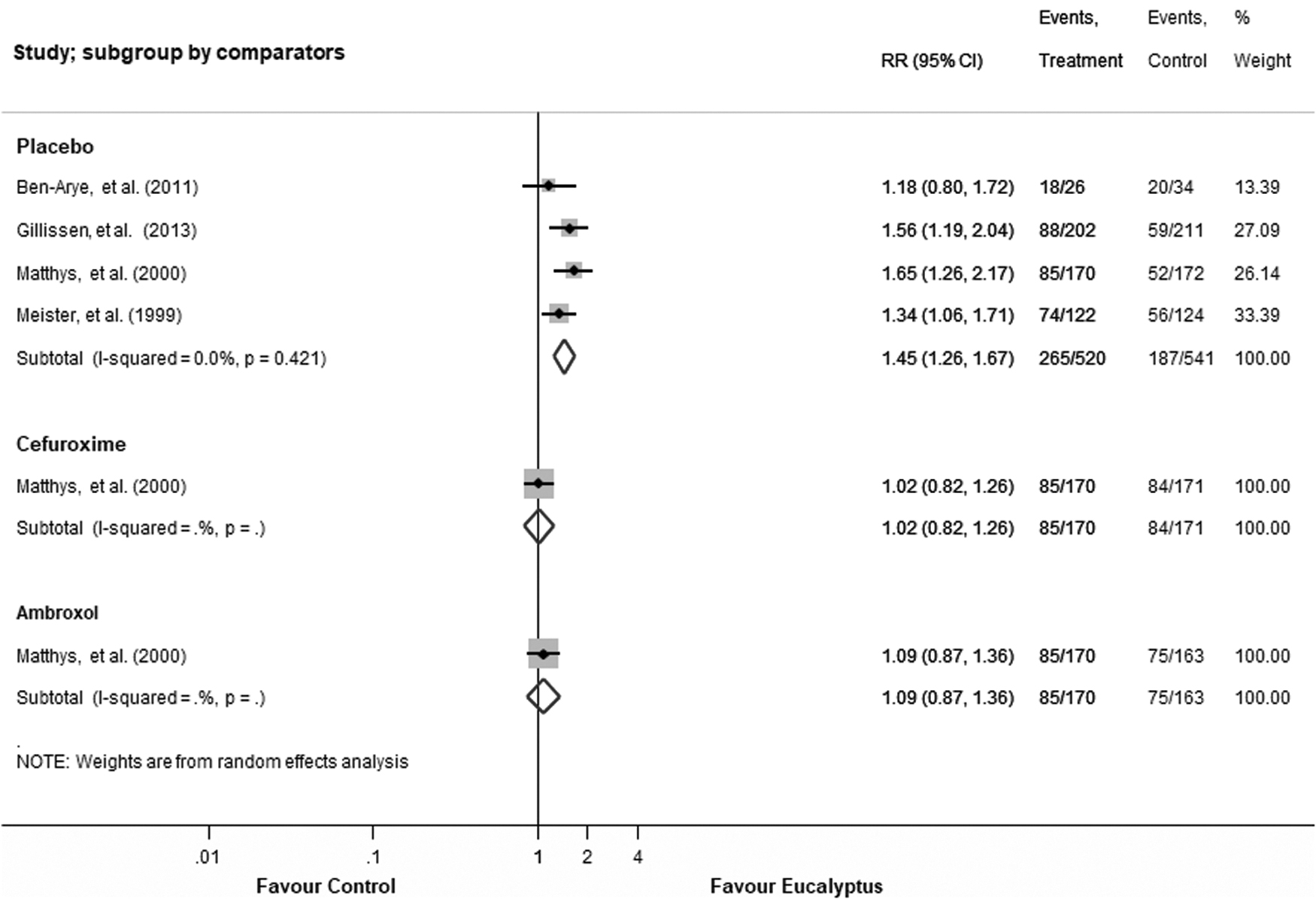
Effects of eucalyptus on improvement or resolution of overall cough symptom.
Five studies 26 –30 with 1,797 patients reported an average reduction of CF. However, only two studies 26,27 had sufficient data for meta-analysis. The result indicated that Eucalyptus had a statistically significant reduction on CF when compared with placebo (n = 655, WMD: 0.44, 95% CI 0.28–0.60, p-value <0.001), with mild heterogeneity (I 2 = 4%; p-value = 0.308) (Fig. 3).
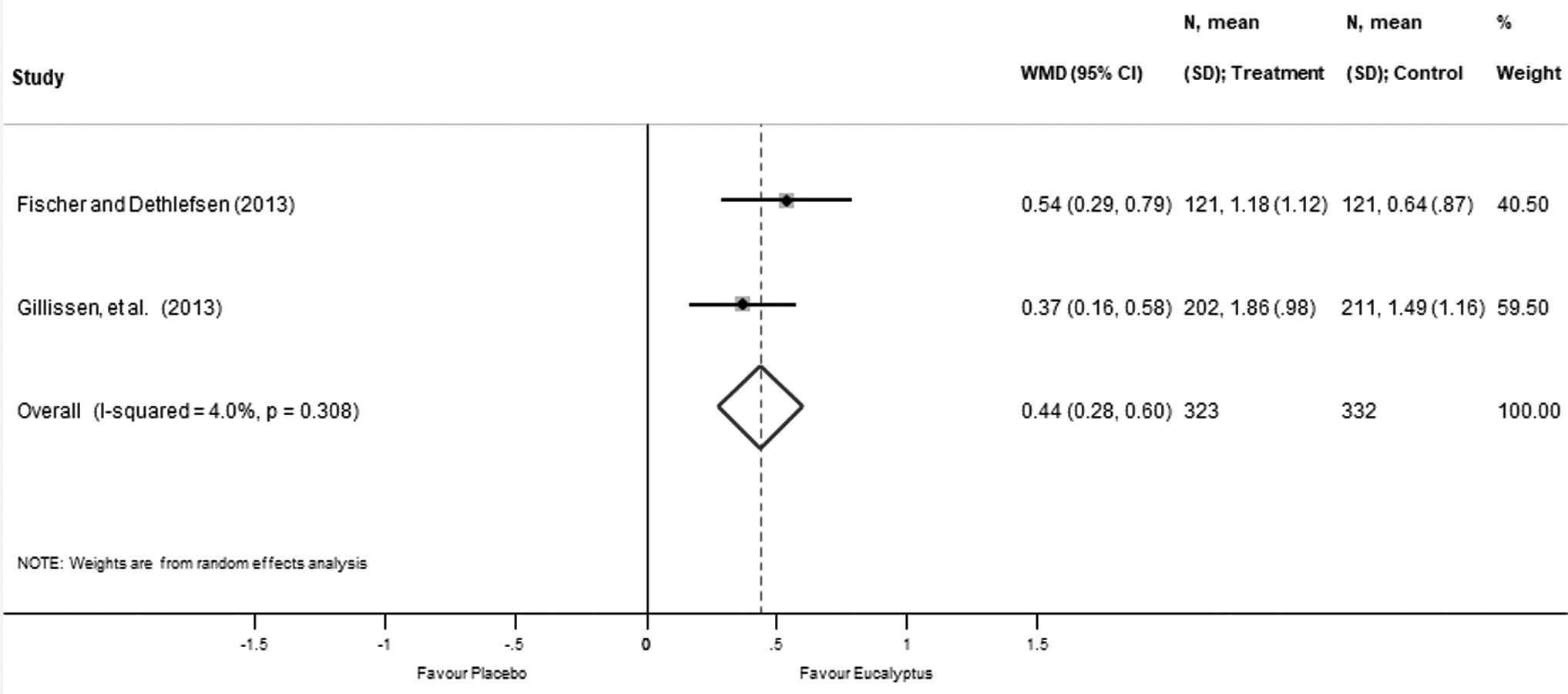
Effects of eucalyptus on reduction of cough frequency.
Safety data were reported in five of six studies with 1,797 patients. 26 –30 The number of AEs was comparable in the Eucalyptus and control groups. There was no report of serious AEs or death during administration of any form of Eucalyptus for 3 to 180 days. The most common AEs reported in the Eucalyptus (Eucalyptus alone and in combination) groups were mild-to-moderate gastrointestinal symptoms such as heartburn, stomach aches, diarrhea, and nausea. These AEs were reported as mild severity. The number of dropout patients reported from four included studies were 55 out of 520 (10.6%), 19 out of 171 (11.1%), 21 out of 163 (12.9%), and 95 out of 541 participants (17.6%) for Eucalyptus, cefuroxime, ambroxol, and placebo, respectively (Table 3). 25,27 –29
Summary of Adverse Events Report in Included Trials
Control groups in this study were placebo, cefuroxime, and ambroxol (respectively).
AEs, adverse events; N/A, data not available; No., number.
For clinical therapeutic efficacy outcome, the results of funnel plot, Begg's, and Egger's tests consistently showed that there was no evidence of small study effect (p-value = 0.414) (Fig. 4).
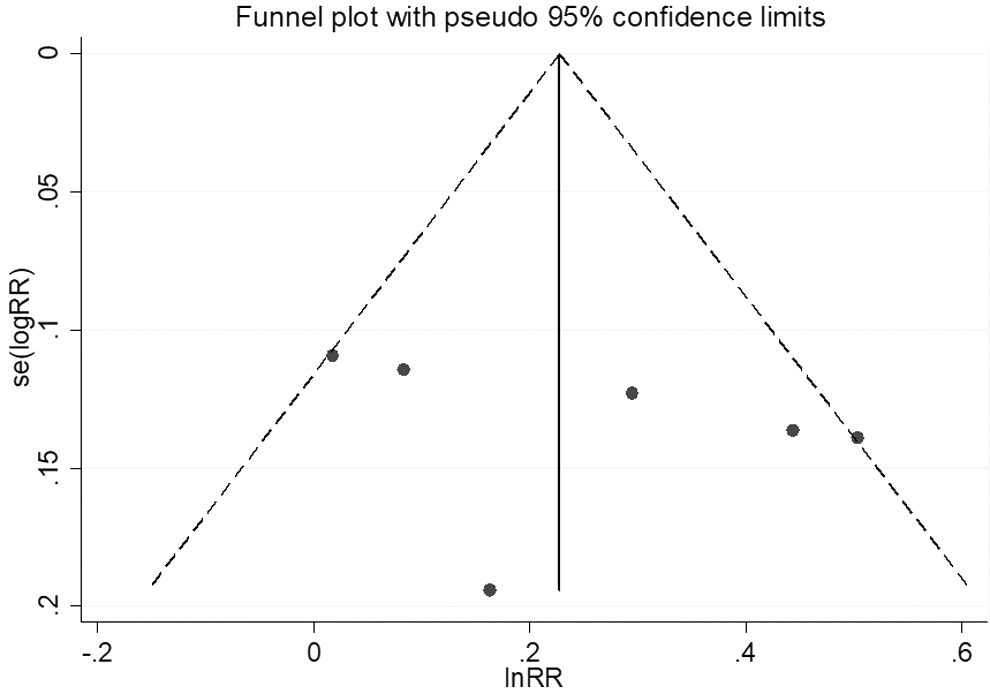
Funnel plot for small study effect test.
The results of sensitivity analyses by using data from studies with high quality and using fixed effects model and subgroup analyses by quality of study (low risk or high risk of bias), and dosage form of Eucalyptus (spray vs. capsule) indicated that the main result of Eucalyptus on achieving improvement and resolution of overall cough symptoms was not changed (Table 4).
Sensitivity and Subgroup Analyses for Eucalyptus on Overall Cough Reduction
CI, confidence interval; RR, relative risk.
Discussion
This study showed benefit of Eucalyptus (used either as monotherapy or in combination with other treatments) on cough induced by URTI and related diseases with a comparable adverse effect compared with other interventions (placebo, cefuroxime, and ambroxol).
Previous study has reported the effects of essential oil extract from herbs including Eucalyptus on reducing cough symptoms. 12 However, they included only four studies and the results are summarized from multiple herbs, not specific to Eucalyptus data. Previous study concluded that multiple herbal medicines including Eucalyptus can improve both severity and frequency of cough symptoms. We updated the previous review by including six trials investigating the efficacy of Eucalyptus on cough. This finding confirmed the previous study that, compared with placebo, Eucalyptus significantly resulted in improvement or resolution of overall cough symptom and reduction of CF without any serious AEs. It is important to point out that a possibility of having small study effect despite the lack of significance of all tests cannot be fully excluded. Cochrane handbook recommended the use of these statistical tests for small-study effects where there were at least 10 studies. As this review assessed a few trials, the finding should be carefully interpreted.
The mechanism of Eucalyptus oil on cough is unknown. The postulated mechanisms of Eucalyptus oil on cough may be related to its mucolytic, bronchodilating, antibacterial, antiviral, and anti-inflammatory activities. 15,16,31 Moreover, a product containing Eucalyptus oil also decreases nasal ciliary beat frequency and mucociliary transport time. 31 According to these properties of Eucalyptus oil, it will be effective in treating cough induced by URTIs and their related diseases such as bronchitis and COPD. In addition, other herbs in the included Eucalyptus formulations such as Pinus spp. (pine), C. aurantifolia (lime), Mentha piperita (Peppermint), Rosmarinus officinalis (Rosemary), and Origanum syriacum (Origanum) have anti-inflammatory, antibacterial, and antioxidant properties. 32,33 These properties may enhance the benefit of Eucalyptus on cough, the finding result of this study.
Despite no information on onset of Eucalyptus oil, previous pharmacokinetic studies of products containing Eucalyptus such as Myrtol® (Gelomyrtol®, Gelomyrtol forte®) revealed that these products were rapidly absorbed by the enteric epithelium and reached high level plasma concentration. The plateaued plasma concentration was reached in a few hours after use of oral medications. 34,35 Whereas use of inhaler form provided peak plasma concentration (Cpeak) at 18 min after administration, and elimination half-life of this formulation was 104.6 min, 36 implying that Eucalyptus may have a rapid onset of action.
The strength of this study is a comprehensive summary of the effects of Eucalyptus on cough, undertaken with the high standard of systematic review and meta-analysis and report aligned with PRISMA. 19 The meta-analysis of RCT is at the top in the hierarchy of clinical evidence. The current evidence on efficacy and safety of any dosage form of Eucalyptus on cough due to URTI and their related diseases such as bronchitis and COPD from RCTs regardless of language was updated. In addition, the safety of Eucalyptus used for 3 to 180 days was summarized. The finding showed that there was no reported serious AE and no difference of AE reported between the control and Eucalyptus group. Thus, use of Eucalyptus products for cough was safe. However, most common AEs reported in included studies were gastrointestinal (GI) symptoms including nausea, vomiting, diarrhea, stomachache, gastrointestinal infection, and abdominal pain. Patients with previous peptic ulcer or GI symptoms should avoid or use this product with caution.
Considering magnitude of Eucalyptus benefit, although CF was significantly less in patients using Eucalyptus compared with those in the placebo group, it should be carefully interpreted because it was unclear whether the magnitude of CF reduction observed was of clinical significance. In addition, the number of studies evaluated for this outcome was small and the baseline CF was not reported in the included studies. In current practice, the challenge of cough treatment is an absence of good evidence supporting the effectiveness of most current cough medicines. Notably, the outcome measurement differed across studies and most studies were of low quality. 12 Therefore, there is a big room to develop a product from herbal medicines or new drugs to be an alternative treatment of cough in the future.
Although our study demonstrated benefits of Eucalyptus for either as monotherapy or fixed combination product, most evidence was based on those studies evaluating effect of Eucalyptus in fixed combination product compared with placebo. Therefore, interpretation and clinical application of Eucalyptus extract (cineole) alone on cough, and Eucalyptus products comparing active treatment such as cefuroxime or ambroxol results should be performed with caution.
A number of limitations should be mentioned. Half of the included studies were high risk of bias. High dropout rate and difference of dropout rate between study groups were a major reason for low methodological quality. Only short-term efficacy of Eucalyptus was evaluated in this study. Although two included studies mentioned to follow-up effect of Eucalyptus products for 180 days, their effects on cough reduction were not reported at that time point. Therefore, further high-quality large multicenter randomized controlled trials compared with placebo or active agents and studying for the long-term effects of Eucalyptus products, especially cineole, are needed to support this evidence.
Conclusion
Based on current evidence, Eucalyptus products may be effective and safe for alleviating cough induced by URTIs and their related diseases. However, further multicenter well-designed randomized controlled trials investigating the long-term effects of these products on cough should be performed to support current evidence.
Footnotes
Authors' Contributions
L.H., J.K., and R.S. conceived and designed the study, reviewed the quality of data, and wrote the article. All authors (L.H., J.K., R.S., and N.C.) performed the experiments and extracted the data, read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research project is financially supported by Mahasarakham University (Fast track 2020). The grant number is 6307017/2563.