
Abstract
Background:
In integrative medicine, complementary healing methods, such as external applications (massages, rhythmic rubs, and compresses), are part of the practice and clinical application and have proven their therapeutic effect in various fields.
Objective:
Aim of this exploratory, controlled, single-blinded study was to investigate the effects of three different warming chest compresses on cardiovascular regulation by analyzing heart rate variability (HRV) in healthy subjects.
Methods:
Over a period of 4 weeks, three different warming chest compresses (a hot water compress, a ginger powder compress, and a mustard flour compress) in 30 healthy subjects were analyzed. For all subjects, 48-h long-term electrocardiograms were recorded, and afterward, epochs of 5 min length extracted and analyzed by different linear and nonlinear HRV indices.
Results:
A moist chest compress did not result in any significant short- and long-term stimulation of the autonomic regulation, except for a short-term significant decrease in heart rate (meanNN, p < 0.05). Warm and moist chest compresses with ginger flour led to significantly increased HRV (sdNN, p < 0.05; symbolic dynamics2, p < 0.05) and its complexity (renyi4 entropy, p < 0.05) and a significant decrease in heart rate (meanNN, p < 0.00036), and thus to a short-term relaxation effect. In contrast, warm and moist chest compresses with mustard flour led to significantly decreased HRV and their complexity (time-, frequency-, and nonlinear dynamics domain, p < 0.00036), which can be interpreted as a stress reaction of the autonomous nervous system.
Conclusions:
The application of chest compresses led to short-term relaxation effects (ginger) as well as short-term stress effects (mustard) but not to any significant longer-term effect on HRV in healthy subjects.
Introduction
External applications, such as baths or compresses, have been used for thousands of years in many cultures to improve well-being. For example, the first reference to compresses applications dates back to around 1500 BC, when hot Nile mud packs were applied for health/healing/wellness/relaxation purpose in Egypt. 1 In anthroposophic medicine (AM), complementary healing methods, such as external applications (massages, rhythmic rubbing, and compresses), are part of care. Applications of external applications (compresses) completely encircle the body part with a wrapping in one or more cloths that necessitate a certain temperature and/or can be coated with substances, an important part of AM 2 practice and clinical application.
Few studies on compresses exist. Of the available studies, some evidence has been demonstrated in reduction of inflammatory joint pain 3 and with a review of studies by Bächle-Helde. 4 Bächle-Helde's review summarizes evidence, including the use of warm, moist tea bag compresses for chest pain in nursing mothers, 5 as well the pain-relieving effect of cabbage leaf compresses 6 ; accelerated excretion performance of the liver with hot liver compresses 7 ; and the analgesic effect of arnica support in acute back pain. 8 Additionally, a recent randomized prospective pilot trial investigating the effect of external application of yarrow liver compresses to reduce fatigue in patients with metastatic cancer undergoing radiation therapy could show that external application of liver compresses reduces fatigue within a clinically relevant range. 9
Ginger and mustard are two substances that have been found to have a unique effect on the sensation of warmth when applied to the skin. Ginger has been found to have a wide range of effects, such as immunomodulating, antitumorigenic, anti-inflammatory, antiapoptotic, antihyperglycemic, antilipidemic, antiemetic, and strong antioxidant effects. 10,11 For people with chronic osteoarthritis prewarmed ginger patch/compress applied to the mid-lumbar region has been found to improve the overall health and increase independence of people with chronic osteoarthritis. 12 Application of ginger compresses was found to provide a multiphase warming of the body in subjective descriptions by study participants, highlighting an initial direct warmth of the cloth followed by a long-lasting, deep, and radiating warmth initiating from the compress contents after 15 min. 13
Mustard flour is traditionally used externally for rheumatic diseases, respiratory tract infections, and migraines. Vagedes et al. has found a significant increase in heat sensation by adding mustard powder to a hot foot bath. 14 Known for its strong warming properties, some case reports even report severe skin burns after self-applied mustard compresses. 15 Both ginger and mustard flour have been found to have the potential to be skin irritating, stimulate blood circulation and have a warming effect when applied as hot chest compresses.
Manjuladevi et al. conducted a randomized crossover study to investigate the effects of hot chest compresses on the cardiorespiratory system in healthy subjects and reported a significant reduction in systolic blood pressure, decrease in diastolic blood pressure (including mean arterial pressure and pulse rate), and a significant improvement in peak expiratory flow rate during the application of hot chest compresses. 16 Moreover, their study provides evidence of changes in healthy cardiac system after the application of compresses by measuring heart rate variability (HRV).
In this study, we investigated the effect of ginger and mustard as warming ingredients in chest compresses for warmth and relaxation in healthy young adults. We aimed to differentiate between short and long-term effects of different compress interventions (hot water, ginger powder, mustard flour) on autonomous nerve system (ANS) in respect to HRV. A dysregulation of the ANS may lead to increased sympathetic activity considered as an indicator for reduced autonomic health, and may be a risk factor for various diseases and an indicator for chronic stress. 17,18 The ANS rapidly promotes physiological changes through the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). The PNS promotes the sympathetic response to stress, commonly referred to as the “fight-or-flight” response, by inhibiting the inhibitory effect. 19
One way to identify adaptive abilities and resulting stability of the ANS is to measure the variability and complexity of heart rate fluctuations. 20 Stress is reported to enhance sympathetic activity, alter sympathovagal balance, and reduce total HRV power. 21 Stress responses are associated with increased energy expenditure 22 along with associated changes in heart rate, breath rate, and blood pressure. Acute stressors lead to an acute increase in blood pressure, heart rate, and decreased metabolic efficiency. 23 HRV indices are useful markers to evaluate stress and ANS activity. sdNN is an index of physiological resilience against stress (it consists of parts from SNS and PNS). The variables RMSSD, pNN50, and HF are impacted by the PNS (higher values indicate increased parasympathetic activity), whereas LF reflects the activity of the SNS.
Regarding the literature, it could be shown that HRV indices changed in response to stress induced by various methods. The most frequently reported factor associated with variation in HRV variables was low parasympathetic activity, which is characterized by a decrease in RMSSD, pNN50, and HF, and an increase in the LF. 19 Nonlinear HRV methods showed that mental arithmetic stress leads to an increase in blood pressure, heart rate, and a decrease in HRV, accompanied by a shift toward an increase in sympathetic tone and an increase in predictability, regularity, and decrease in HR complexity. 24
In addition, aerobically trained subjects have been shown to have lower SNS reactivity (e.g., heart rate) and improved cardiovascular efficiency in response to physical and/or psychological stress. In addition, resistance training has been shown to attenuate cardiovascular responses and improve mental health. 23
To our knowledge, there are no studies about the effect of compress applications in the context of HRV. In a former exploratory, controlled, single-blinded study design of Stritter et al., 25 the effect of ginger and mustard as warming ingredients from the effect of calmness and attentiveness, and thermal warmth in the application of chest compresses through psychometric and qualitative phenomenological data was investigated.
No significant changes in somatic complaints could be found. After the application of the ginger powder compress, the questionnaire on mental state found a significant shift toward good mood and calmness (also for the mustard compress); the 5-point rating scale found significant changes toward relaxation, balance, deep and slow breathing, as well as warm hands and feet. The 5-point rating scale did not reveal significant changes after the application of the mustard compress. These findings demonstrated the different qualities of warmth with the warming ingredients, ginger and mustard, through the qualitative phenomenological data.
In this study, we aim to close this gap by using well-established linear and nonlinear HRV measures that have been shown to provide reliable results in patients with various cardiovascular diseases even with short recording times. 26 –29
In comparison to traditional linear HRV methods, nonlinear HRV methods have provided new insights into changes of the cardiovascular and/or cardiorespiratory systems under various physiological and pathological conditions and offer additional prognostic information. Linear approaches in the time and frequency domains (FDs) are often insufficient to quantify the complex dynamics of physiological systems and their associated time series. Most physiological systems (biosignals), for example, heart rate, exhibit a very complex behavior that is far from simple periodicity. Such complexity within the obtained heart rate time series is caused by various components of the system's inherent dynamics and in particular by the nonlinear interaction of different physiological control loops.
Therefore, several efforts have been made to apply nonlinear complexity measures to analyze HRV. These approaches differ from traditional time- and FD HRV analyses in that they quantify signal properties rather than assessing only the magnitude or frequency power of the heart rate time series. They assess the self-affinity of heartbeat fluctuations over multiple time scales (fractal measures); the regularity/irregularity or randomness of heartbeat fluctuations (entropy measures); the coarse-grained dynamics of HR fluctuations based on symbols (symbolic dynamics [SD]); and heartbeat dynamics based on a simplified phase space embedding. 30
The HRV analysis is a valuable supplement to conventional questionnaires (qualitative examination). Additional information by HRV parameters about the activation and strength of autonomic regulatory processes (sympathetic, parasympathetic) during and after the application of compresses, provide a clear justification for a mixed method approach in this study.
Methods
Study design
In this explorative, controlled, single-blinded study, we examined the effect of ginger and mustard as warming ingredients in chest compresses for warmth and relaxation in healthy young adults. Our aim was to investigate the changes in autonomic balance, especially due to altered HRV, caused by different compress interventions.
Simple blinding was ensured by the subjects having only the information that compresses were applied to them, but nothing about the substances or the sequence. An electrocardiogram (ECG) was recorded beforehand, during and after each intervention to evaluate the different compresses and their effect on the ANS using HRV analysis.
The study protocol was approved by the Ethics Committee of the Charité—Universitätsmedizin Berlin and was carried out in accordance with the Declaration of Helsinki. 31
The studies involving human participants were reviewed and approved by the Ethics Committee of the Charité—Universitätsmedizin Berlin (project registration number: EA1/235/15) and was carried out in accordance with the Declaration of Helsinki. The study is registered in the German Clinical Trial Register under registration number DRKS00009359. The patients/participants provided their written informed consent to participate in this study.
Subjects
In this study, 30 age/gender-matched healthy participants (15 men, mean age 27.8 years, standard deviation 4.5 years; 15 women, mean age 26.2, standard deviation 4.4 years) were enrolled and received three different warming chest compresses during a 1-week interval. The inclusion criteria provided for eligibility of persons were between 18 and 40 years of age who were not having chronic or acute illnesses or taking medication. To be eligible to participate, neither alcohol nor drugs had been consumed, and the participants had not actively participated in sports from the day before to the day after the intervention. The interventions took place in the same calm, comfortable, and quiet room in a therapeutic facility at the Charité—Universitätsmedizin Berlin once a week in the morning between 9.00 a.m. and 13.00 p.m. Results of physiological, psychometrical, and phenomenological data were published elsewhere. 25
Intervention
The study period spanned 4 weeks with four different chest compresses. During the first week, participants received a simple dry compress (C, control) to get the participants accustomed to the procedure of the compress applications. This was done to minimize and exclude confounding effects (increased stress level and sympathetic tone due to excitement) on the HRV analyses of the subsequent compress applications. During the second week the compress was warmed with hot water (I2) without other ingredients (70°C). During the third week, ginger powder (I3) (70°C) was added to the warm water. During the fourth week, mustard flour (I4) (60°C) was added.
Participants were instructed to lie down on a medical couch and settle comfortably in a warm environment with warm blankets. The compresses were applied for 30 min for C, I2, and I3, but only 5 min for I4 to avoid discomfort and possible skin burns 25 (Fig. 1).

Timeline of ECG measurements for HRV analyses. ECG, electrocardiogram; HRV, heart rate variability.
Data recording and data preprocessing
For each participant, a 48-h ECG was recorded before, during, and after the intervention. All recordings were performed in a resting position and environment (supine position, a quiet environment, and the same time of day and location). From the 48-h ECG records, quasi stationary 30-min heart rate time series consisting of successive beat-to-beat intervals (BBI) were extracted per intervention, and afterward shortened to 5-min length (comparable data length for each intervention) and filtered by applying an adaptive variance estimation algorithm to remove and interpolate ventricular premature beats and artefacts to ensure normal-to-normal (NN) beat time series. 32
The 48-h ECG was applied the day before and removed the morning after the compress application. Thus, the HRV analyses of the night before the intervention (T1), during the intervention (TI), during the rest phase immediately after the intervention (T2), and the night after the intervention (T3) could be analyzed to quantify the different phases of the autonomic regulation.
In this study, we investigated the short and longer-term effect of different compress interventions. Therefore, we compared the intervention phase (TI) with the resting phase after the intervention (T2) to quantify short-term effects, and compared the night before the intervention (T1) with the night after the intervention (T3) to quantify longer-term effects on autonomic regulation with respect to different compress effects.
HRV analysis
We applied some of the most commonly used indices of HRV analysis in the time-, frequency-, and nonlinear dynamics domains. They are based on various concepts, thereby revealing multiple aspects of cardiovascular variability. 20,33
Linear HRV analyses
In the time domain (TD), the following indices were calculated:
meanNN: The mean value of the NN-intervals of BBI (ms);
sdNN: Standard deviation of the NN-intervals of BBI (ms);
rmssd: Square root of the mean squared differences of successive NN intervals (ms);
pNN50: Proportion derived by dividing the number of interval differences of successive NN intervals >50 ms by the total number of NN intervals (%);
renyi4: Rényi entropy as a complexity measure of the BBI estimated from α-weighted probabilities distributions (α = 4) (bit).
In the FD, the following indices were calculated:
LF/HF: The ratio between the low (LF: 0.04–0.15 Hz) and high (HF: 0.15–0.4 Hz) frequency power of the estimated spectrum (a.u.);
LFn: Normalized low-frequency power (0.04–0.15 Hz) of BBI (a.u.);
HFn: Normalized high-frequency power (0.15–0.4 Hz) of BBI (a.u.).
The power spectra of equidistant linear interpolated (10 Hz) NN interval time series (resampled to 2 Hz) were obtained by applying the Fast Fourier Transformation (Blackman Harris window).
Nonlinear HRV analyses
Symbolic dynamics
The concept of SD is based upon a coarse-graining of the nonlinear dynamics within time series. 34 Therefore, the BBI were transformed into a symbol sequence of four symbols with a given alphabet A = {0,1,2,3}. From this new alphabet (consisting of a symbol string), words were created with three successive symbols that allowed for 64 different word-type combinations (bins) (000, 001,…,333). The following SD indices from the probability distribution of each word-type within the symbol sequence were estimated:
wpsum02: Relative portion (sum/total) of words consisting only of the symbols “0” and “2,” a measure for reduced HRV (a.u.), and
wpsum13: Relative portion (sum/total) of words consisting only of the symbols “1” and “3,” a measure for increased HRV (a.u.).
Detrended fluctuation analysis
The method of detrended fluctuation analysis (DFA) is based on a modified random walk analysis to quantify the presence or absence of fractal correlation properties in nonstationary time series. 35 DFA is based on the computation of one index α1 of short-term fractal scaling properties and another index α2 of long-term fractal scaling properties (α = scaling exponent or self-similarity factor). 35
Poincaré plot analysis
The Poincaré plot analysis (PPA) is a two-dimensional graphical representation (scatter plots), where each beat-to-beat interval of the BBI time series is plotted against its subsequently corresponding beat-to-beat interval of the BBI time series. Thus, the shape of the plot is assumed to reflect changes in vagal and sympathetic modulation. 36,37 Two indices were calculated:
SD1: The standard deviation of short-term NN variability (minor axis of the cloud, [ms]), and
SD2: The standard deviation of long-term NN variability (major axis of the cloud, [ms]).
Although the PPA method is a nonlinear method, the parameters (SD1 and SD2) are linear measures. 30
Statistics
The nonparametric Wilcoxon test was applied (SPSS 21) and for the statistical evaluation of significant univariate differences in linear and nonlinear indices of HRV between the time points and the related interventions. Univariate significance was considered for values of p < 0.05 (Bonferroni Holm correction: p < 0.00036). Descriptive statistics were used to describe the data's basic features in terms as median value and quartile values at 25 and 75 percentiles (25%–75%).
Results
Short-term effects on autonomic regulation—comparison of the compress intervention phase (TI) with the resting phase after the intervention (T2)
The HRV analysis for I2 revealed that the only significant difference in TD was the increased meanNN (p < 0.05) for T2 compared with TI.
I3 also showed a significant difference in TD meanNN (p < 0.00036), sdNN (p < 0.05), and renyi4 (p < 0.05), as well as in SD2 (p < 0.05) through PPA by comparing TI with T2 that pointed to a decreased heart rate, and increased HRV and HRV complexity in T2.
The most significant differences (p < 0.00036) between both time points (TI, T2) for HRV indices were found for I4 in all domains (TD, FD, SD, DFA, PPA) showing a highly decreased HRV and HRV complexity inT2 as compared with TI (Table 1, Fig. 2).
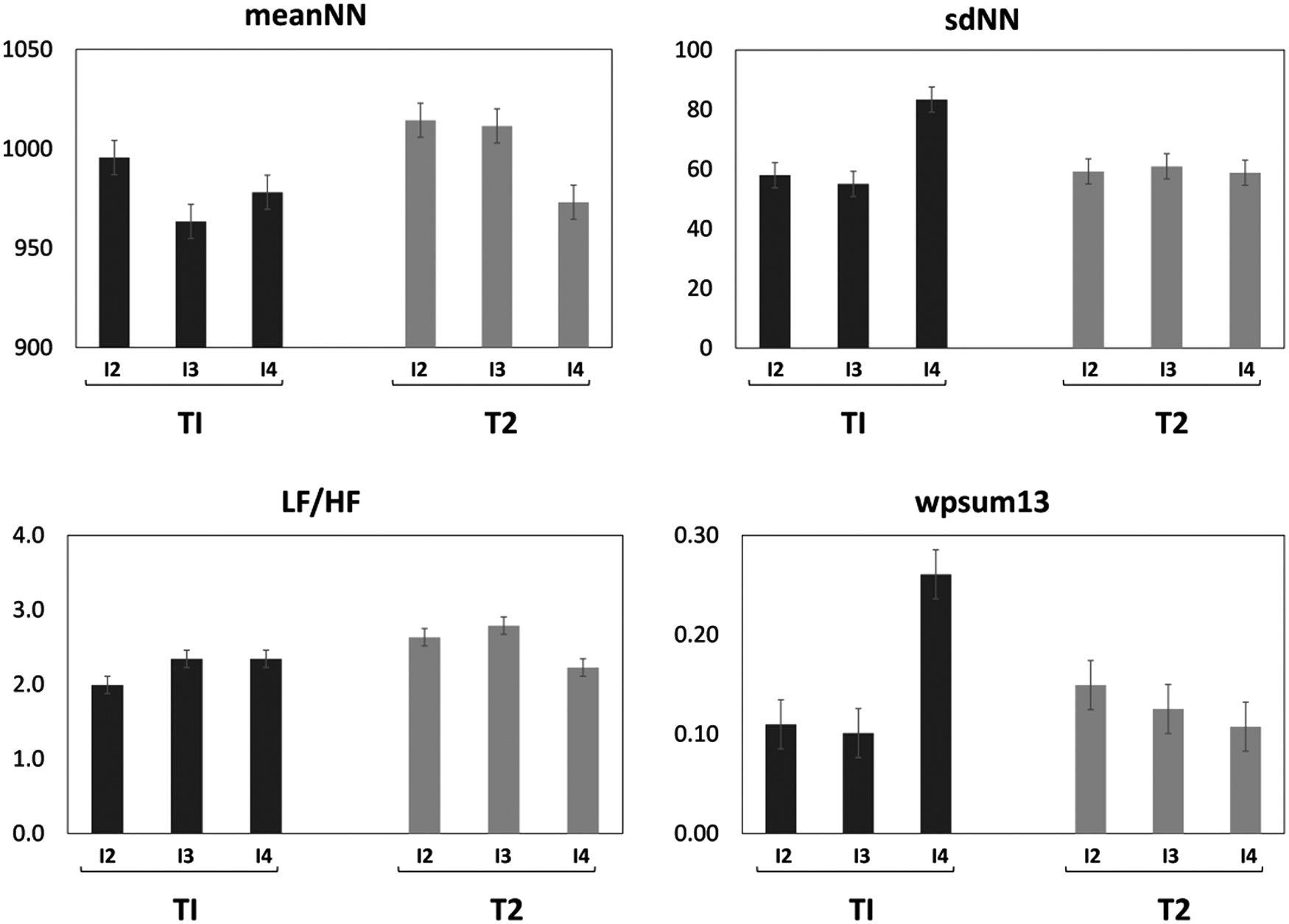
Bar charts with standard error of significant HRV indices from the time-, frequency-, and nonlinear dynamics domains for the comparison of the compress intervention phase (TI) with the resting phase after the intervention (T2) for the compress warmed with hot water (I2), for the compress with ginger powder (I3), and the compress with mustard flour (I4). (meanNN as the mean value of the NN-intervals [ms]; sdNN as standard deviation of the NN-intervals of BBI [ms]; LF/HF as the ratio between the low [LF: 0.04–0.15 Hz] and high [HF: 0.15–0.4 Hz] frequency power of the estimated spectrum [a.u.], and wpsum13 as the relative portion [sum/total] of words consisting only of the symbols “1” and “3,” a measure for increased HRV [a.u.]). BBI, beat-to-beat intervals; HRV, heart rate variability; NN, normal-to-normal.
Significant Heart Rate Variability Indices for the Comparison of the Compress Intervention Phase (TI) with the Resting Phase After the Intervention (T2) for the Compress Warmed with Hot Water (I2), for the Compress with Ginger Powder (I3), and the Compress with Mustard Flour (I4)
Descriptive statistics as the median value and quartile values at 25 and 75 percentiles (25%–75%).
p < 0.05; *** p < 0.0036.
DFA, detrended fluctuation analysis; FD, frequency domain; n.s., not significant; PPA, Poincaré plot analysis; SD, symbolic dynamics; TD, time domain.
Longer-term effects on autonomic regulation—comparison of the night before the intervention (T1) with the night after the intervention (T3)
HRV analysis only showed significant differences between T1 and T3 in SD2 (p < 0.05) from PPA for I4 pointing to higher long-term HRV during T3 (Table 2).
Significant Heart Rate Variability Indices for the Comparison of the Night Before the Intervention (T1) with the Night After the Intervention (T3) for the Compress Warmed with Hot Water (I2), for the Compress with Ginger Powder (I3), and the Compress with Mustard Flour (I4)
Descriptive statistics as the median value and quartile values at 25 and 75 percentiles (25%–75%).
p < 0.05.
DFA, detrended fluctuation analysis; FD, frequency domain; n.s., not significant; PPA, Poincaré plot analysis; SD, symbolic dynamics; TD, time domain.
Discussion and Conclusion
The aim of this study was to differentiate between short and long-term effects of different compress interventions (hot water, ginger powder, mustard flour) on the ANS in healthy participants, which were assessed by HRV analysis.
We could demonstrate that warm and moist chest compresses with ginger flour led to significantly increased HRV and complexity and a significant decrease in heart rate, and thus led to a short-term relaxation effect. In contrast, warm and moist chest compresses with mustard flour led to significantly decreased HRV and complexity, which can be interpreted as a stress reaction of the ANS in the short term. The overall short-term effect of the application of chest compresses with ginger led to short-term relaxation effects, whereas with mustard they led to short-term stress effects. None of the compresses led to longer-term effects to the ANS in healthy subjects. This corresponds to the findings from the psychometric and qualitative phenomenological data (questionnaire). 25
For the application of warmed compresses with hot water (I2), we investigated the effect factor of externally applied moist warmth using a hot chest compress. This did not result in any measurable relaxation or changes in HRV. Various reasons could have led to this result. First, a habituation effect of the procedure could have already occurred after the first application (a simple dry compress, C) despite the same baseline conditions, thereby inhibiting a relaxation response. However, this seems unlikely due to the simple blinding, since the study participants did not know how each application would differ from the previous one, so that uncertainty and surprise remained before each application. A further argument against the habituation effect is that HRV changes could be measured again in the subsequent applications (I3, I4).
In a future study, it would be recommended to ensure a different order of application of the compresses among the participants to exclude a habituation effect. This would answer the overarching question of whether patients can benefit from sequential applications. Second, subjective perception and assessment of the compress application by individual subjects. Insights from the questionnaires and interviews elucidate that the second compress application was largely perceived as unpleasant, mainly due to a rapid cooling of the moist warmth that created a cooling effect. 25 A logical conclusion is that discomfort would prevent a relaxation response. During the compress application, it was perceived as unpleasant by the subjects, but after the compress was removed, the subsequent time was described as a relaxation effect that spread through the body like a wave. 25
Externally applied moist warmth does not obligatorily lead to relaxation or HRV stimulation. It is possible that patients with chronic conditions/diagnosed with existing indications may experience moist/hot chest compress application differently. Manjuladevi et al. showed that hot chest compress applications led to improvement of the cardiorespiratory system, including a significant decrease in systolic and diastolic blood pressure and pulse rate. 16 A significant decrease in heart rate was also demonstrated in their study—analogous to the results of our study, in which a significant change in heart rate was induced in healthy subjects by the hot chest compress without herbal additive. Further clinical investigation is needed to explain why moist warmth does not contribute to relaxation and HRV enhancement.
The application of warmed compresses with ginger powder (I3) investigated an additional warming reaction of the body. In contrast to I2, this application led to a short-term relaxation effect evidenced by a significantly increased HRV, complexity, and a significant decrease in heart rate. However, significant results indicating a long-term HRV stimulation effect were not found. The overall altered HRV with ginger flour compresses had a contrasting effect compared with hot compresses without added substances. This may be due to the prolonged warming property of ginger itself. 13,38 This could also possibly be explained by an induction in the ANS to relax and achieve higher HRV.
Consideration of the time course of the HRV indices during the respective applications shows a clear increase in parasympathetic activity (increase: sdNN, rmssd, SD1) and reduced heart rate and increasing warming effect during each successive compress application. Based on the subjective reports of many test persons, the warming rather than cooling provided by I2 may provide the ideal warming effect duration. 25 On the other hand, this would at the same time, ginger itself can intensify and/or prolong the warming effect, which may explain why greater relaxation changes were measurable in the after-rest during I3.
In line with the hypothesis of the duration of the warming effect, Vagedes et al. found a significant increase in the sensation of warmth after a footbath with mustard or ginger flour compared with a footbath without plant additives, which lasted for at least 10 min in the case of the footbath with ginger flour. 14 This speaks for the presumed prolonged warming effect of ginger and that this perceived warmth lasts longer than thermal warmth alone. 14 Stritter et al. could show that in addition to the immediate physical and mental relaxation elicited by the ginger compress, a feeling of alertness and feeling refreshed resulted after the intervention. 25 The invigorating tonic effects of the external application of ginger are also described in other studies. 39,40 The effect of ginger can be explained, among other things, by the stimulation of metabolism and blood circulation in the involved skin regions, which trigger reflex vegetative processes. 39,40
However, a central finding of the warmth of the ginger powder compress in this study attributed as a sensation “more than just warmth” that spread throughout the body; quite a different description from blood circulation stimulation were also reflected in the rating scales. 25 Whether there is an optimal duration of the warming effect for health promotion remains unclear at this time. Ginger powder appears to enhance the warming effect of a moist hot chest compress, leading to a more effective body response that would not be achieved without the addition of a substance. Possibly, ginger flour in combination with a rest application leads to a more effective relaxation and an increase in HRV.
Further possible applications from this study for healthy people in the promotion health maintenance, especially heart health and stress reduction should be explored in long-term studies. With regard to applications in sick patients, further studies are also necessary, for example, to promote HRV stimulation in patients who have had a myocardial infarction for secondary prophylaxis and cardiac risk reduction. Moreover, chest compresses have already been used in patients with bronchial asthma, recurrent respiratory tract infections, bronchitis, pleurisy, and pneumonia. 41
For the mustard flour compresses applied (I4), the warmth was described as “burning heat” and intense warmth that is “just bearable.” After removing the mustard flour compress, most participants described relief and relaxation. Subjects described how the warmth persisted during the resting phase and only subsided slowly. The spread of the warmth was not very pronounced, which was also reflected in the rating scale. This could be explained by the strong stimulus on the cardiovascular system, causing primary peripheral vasoconstriction during the compress. Homeostatic feedback of the organism in the resting phase afterward may also explain after sweats that were experienced. 25
The significant decreased HRV and complexity in contrast to I2 and I3 of these compresses can be interpreted as a short-term stress reaction of the ANS. This ANS response was characterized by decreased activity of the PNS (decrease: sdNN, rmssd, SD1, wpsum13) during the resting phase after the intervention (T2) in I4 compared with I2 and I3. These significant, short-term changes indicate that the chest compress with mustard flour was a stressor for the body (ANS) and did not lead to an immediate relaxation effect after removal (resting phase after the intervention, T2).
However, it has been shown that mustard compresses elicit a strong and sustained response to the perceived heat balance and lead to relaxation, 25 thus mustard can be considered a stimulus therapy that elicits a strong positive relaxing effect. Mustard flour acted on the autonomic nervous system within a very short time (already during the first 5 min) and stimulated HRV. The effect of mustard flour is thought to potentially develop warmth through transient receptor channels 42 and a spasmolytic effect in pneumonia has been reported. 41
Vagedes et al. measured a significant increase in sensation of warmth with the addition of mustard powder to a hot foot bath, but this was no longer measurable 10 min after the bath ended. 14 Comparable studies investigating the effect of mustard powder in external applications on the cardiovascular system are not available. Physiological effects of a hot chest compress with mustard flour showed in our study an immediate HRV stimulation (increase of SNS), which continuously decreased after removal of the chest compress, but showed no effects in the longer term.
In general, it is assumed that the body recognizes externally supplied warmth as an external trigger that leads to the activation of self-regulating autonomic processes in the body.
Two different explanations may explain the autonomic processes that mustard and ginger compresses trigger and activate in the body. First, the mustard and ginger compresses may activate the hormesis mechanisms that may be stimulated by low levels of stress or upregulated by existing cellular and molecular pathways to enhance the ability of cells and organisms to withstand greater stress. These stressors activate biochemical messengers, which in turn activate various signaling pathways that regulate gene expression and adaptive responses. The fundamental benefit of using external warmth involves an increase in local blood flow that likely improves the supply of oxygen and nutrients. 43,44
Further studies should also analyze blood pressure and respiration in addition to the HRV results.
From the point of biosignal processing traditional linear HRV methods in the time and FDs are often insufficient to quantify the complex dynamics of heart rate generation. HRV analyses in the TD evaluates variability by determining variations of RR intervals over a period of time. Here, a huge amount of statistical and geometrical indices can be directly determined from the RR intervals or can be derived from the differences between them. These indices involve mean, standard deviation, counting of the samples above or below a certain threshold, and other statistical measures that are based on the distribution of the data and not their order.
HRV analysis FD uses spectral analysis of a sequence of RR intervals and provide information on how variance is distributed as a function of frequency or as a function of time and frequency. The power spectrum analysis in HRV enables a quantitative representation of the contributing frequencies to an underlying time series enabling the classification of sympathetic and PNS components involving in heart rate regulation.
Although time and FD methods enable the quantification of HRV on different time scales, nonlinear methods provide additional prognostic information regarding the dynamics and structure of beat-to-beat time series. Nonlinear methods analysis has opened up new ways to analyze HRV since they provided new insights into the HRV changes under various (patho)physiological conditions. 30,45
Limitations: The chosen study design could not control for effects over the course of the 4 weeks outside of the study, but the inclusion of homogeneous groups helped prevent confounding effects through external influences. The compress interventions were carried out in the same order for all test persons, thus a certain adaptation and habituation effect of the compress applications on ANS cannot be excluded.
In this exploratory, controlled, single-blinded study design, the single blinding was ensured by the fact that the test persons only had the information that compresses would be applied to them, but nothing about the substances or the sequence.
However, when ginger and mustard powder were used, some subjects smelled and named the aromas during the compress applications. A possible confounding effect on the results of this on the study seems unlikely, since the subjects had no comparable experiences or studies on the same topic. A double-blinded study design would be desirable, but seems to be not applicable because of the smell. With 1 week between each application, a carry-over effect from the previous compress application was prevented. Moreover, we can exclude any significant confounding effect of the study period (season), since standardized conditions for each compress application were given.
In conclusion, ginger powder and mustard flour chest compresses induced a strong and sustained response of the autonomic nervous system. The main differences between the two warming substances were that ginger led to short-term relaxation effects (mild and harmonious effect, warming the whole body), which was supported by physiological, psychometrical, and phenomenological data, and mustard led to short-term stress effects (activating response of the ANS in positive sense), which in the longer term was perceived by the patients as relaxation in healthy subjects. Nevertheless, all subjects felt warmer at the end of the application, but due to two different warmth types (activating stimulus), which led to relaxation in the end.
Footnotes
Authors' Contributions
S.S.: analyzed and interpreted the data, writing—original draft; writing—review and editing. W.S.: conceptualization; data curation; funding acquisition; project administration. M.M.G.: data curation; formal analysis; investigation. D.M.: data curation; formal analysis; investigation. D.R.: conceptualization; investigation. B.W.: conceptualization; investigation. A.E.: resources. R.S.: methodology; interpreted the data. A.V.: methodology; interpreted the data; writing—original draft; writing—review and editing. G.S.: conceptualization; funding acquisition; methodology; roles/writing—original draft; writing—review and editing.
Acknowledgments
The authors would like to thank all the participants in the study as well as Claudia vom Hoff-Heise and Jonas Röttger for administrative support, Sarah Blakeslee for the language editing, and the Akademie Havelhöhe for the provision of therapeutic facilities.
Author Disclosure Statement
R.S. was employed by the company UST Umweltsensortechnik GmbH. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
The study was funded by the foundations Dr. Hauschka (Bad Boll, Germany), Christophorus Stiftungsfond (Stuttgart, Germany) and Helixor (Rosenfeld, Germany). We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité—Universitätsmedizin Berlin.