
Abstract
Introduction:
Breast cancer patients undergoing chemotherapy experience multiple distressing symptoms. The authors investigated the feasibility and potential benefits of auricular acupuncture during chemotherapy infusion in this population.
Materials and Methods:
Women with stage I–III breast cancer undergoing chemotherapy were enrolled and followed for three chemotherapy cycles. During the first cycle of chemotherapy that participants received after study enrollment, they were provided with educational materials. During the second and third cycles of chemotherapy after enrollment, they received auricular acupuncture. The primary outcome was feasibility, assessed by recruitment, retention, and completion of assessments. Secondary outcomes included symptom burden (Edmonton Symptom Assessment System-Revised Version) and anxiety (State-Trait Anxiety Inventory-State), assessed at four timepoints for each cycle: day 1, pre-education/acupuncture (T1); day 1, post-education/acupuncture (T2); day 2 (T3); and day 5 (T4). Nausea and vomiting (Multinational Association of Supportive Care in Cancer [MASCC] Antiemesis Tool) were assessed on days 2 and 5. Paired t test was used to compare patient-reported outcomes during cycle 1 (education) versus an average of outcomes during cycles 2 and 3 (acupuncture).
Results:
Twenty-six patients were enrolled, of which 24 completed all acupuncture sessions and 22 completed all outcome assessments. In cycles 2 and 3 versus cycle 1, participants experienced significant reductions in symptom burden (change from T1 to T4: −7.9 ± 13.6, p = 0.02), anxiety (change from T1 to T2: −3.3 ± 6.5, p = 0.02), and nausea severity on day 2 (−1.3 ± 2.6, p = 0.04).
Conclusions:
The delivery of auricular acupuncture during chemotherapy infusion was feasible and associated with reduction of symptom burden, anxiety, and nausea in breast cancer patients. Larger-scale clinical studies are needed to confirm these findings.
Clinical Trial Registration number: NCT03170648.
Introduction
Chemotherapy leads to multiple distressing symptoms, such as anxiety, fatigue, and nausea, in women with early breast cancer. 1 –7 The sum of these symptoms, with its overall severity and perceived impact by patients, is collectively referred to as symptom burden. 8 Higher symptom burden is associated with substantially lower quality of life and reduced function in breast cancer patients. 9,10 Given the negative impact of symptom burden, the importance of early integrated symptom control has been increasingly recognized in caring for individuals with cancer. 11 –13 Pharmacologic interventions are the current standard of care for managing treatment-related symptoms, but they often have adverse effects and often do not completely mitigate symptoms. 14,15 Other treatment options are needed to help alleviate symptom burden in this population.
In recent years, acupuncture has been increasingly utilized for symptom management in cancer populations. 16,17 Acupuncture is a therapeutic modality rooted in Traditional Chinese Medicine, which involves insertion and stimulation of fine needles over specific sites on the body. It has been studied for various cancer- and treatment-related symptoms, including pain, arthralgia, hot flashes, fatigue, anxiety, insomnia, appetite loss, and nausea and vomiting, with demonstrated efficacy and minimal adverse effects. 18 –23 Although the physiologic mechanisms of acupuncture are still largely unclear, neuromodulation of the vagus nerve and release of endogenous opiates are thought to play an important role in mediating acupuncture effects. 24,25
Auricular acupuncture is a subset of acupuncture, whereby specific points on the external auricle are stimulated to elicit therapeutic responses. 26 Previous studies in noncancer populations suggest that auricular acupuncture reduces anxiety and depression, insomnia, and fatigue. 27 –29 In cancer patients, a small number of studies have also suggested that auricular acupuncture is beneficial for reducing cancer-related pain and chemotherapy-induced nausea and vomiting. 30,31 Based on these results, auricular acupuncture could be a promising therapy for symptom control during chemotherapy. However, there is little information regarding the impact of auricular acupuncture on overall symptom burden related to chemotherapy, including in women with breast cancer.
Many breast cancer patients have demanding schedules as they juggle their treatment, work, and families, which may make it challenging for them to find time to utilize supportive care services and integrative therapies, including acupuncture. 32,33 Previous literature also indicates that commuting imposes a significant burden for breast cancer patients. 34 –36 Thus, it is important for supportive care services to not only be effective, but also time-efficient to best serve this patient population. In this pilot study, the authors evaluated the feasibility and potential benefits of delivering auricular acupuncture treatment at the time of chemotherapy infusion in women with breast cancer.
Materials and Methods
Study design
This was a single-arm pilot intervention study. Study participants were followed for three consecutive cycles of chemotherapy. Patients could enroll into the study at any point during their chemotherapy treatment as long as they had three chemotherapy cycles remaining. During the first cycle of chemotherapy that participants received after study enrollment, they were provided with an educational booklet developed by the National Center Institute that included information on chemotherapy, its side effects, and strategies for self-care. 37 During the second and third cycles of chemotherapy after study enrollment, participants received a 30-minute standardized auricular acupuncture treatment during chemotherapy infusion.
All participants were informed of the study details and signed the informed consent. The study was approved by the Institutional Review Board of the Dana-Farber/Harvard Cancer Center and registered in ClinicalTrials.gov.
The primary aim of the study was to evaluate the feasibility of providing auricular acupuncture for breast cancer patients during chemotherapy infusion. Secondarily, the authors sought to collect preliminary data on the effect of auricular acupuncture on symptom burden, anxiety, and nausea in breast cancer patients receiving chemotherapy. Study staff collected patient-reported outcomes at four timepoints for each of the three cycles: on the day of chemotherapy infusion or day 1, pre-education/acupuncture (T1); day 1, immediate post-education/acupuncture (T2); day 2 (T3); and day 5 follow-up (T4).
Study population
Eligible participants were recruited and enrolled into the study from June 2017 to September 2017 from the Breast Oncology Center at the Dana-Farber Cancer Institute. Participants were eligible if they had histologically confirmed stage I–III breast cancer, were receiving intravenous chemotherapy every 14 or 21 days, were at least 18 years of age, and had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Participants were excluded if they received chemotherapy on a weekly basis, had received acupuncture within 3 months before study entry, had metastatic breast or other cancer, had unstable cardiac disease or history of myocardial infarction within 6 months before study entry, or had uncontrolled infection, seizure disorders, or a major psychiatric disorder.
Acupuncture procedure
Auricular acupuncture was administered to study participants in a seated position while they were concurrently receiving chemotherapy in the infusion center at Dana-Farber. The acupuncture treatment was administered by licensed acupuncturists on staff at the Leonard P. Zakim Center for Integrative Therapies and Healthy Living at Dana-Farber. Figure 1 shows the names and approximate locations of the six auricular acupoints chosen for this study (Fig. 1). The detailed description of acupoint locations can be found in the Supplementary Data. Points were selected based on their usage in previous literature and traditional indications. 38
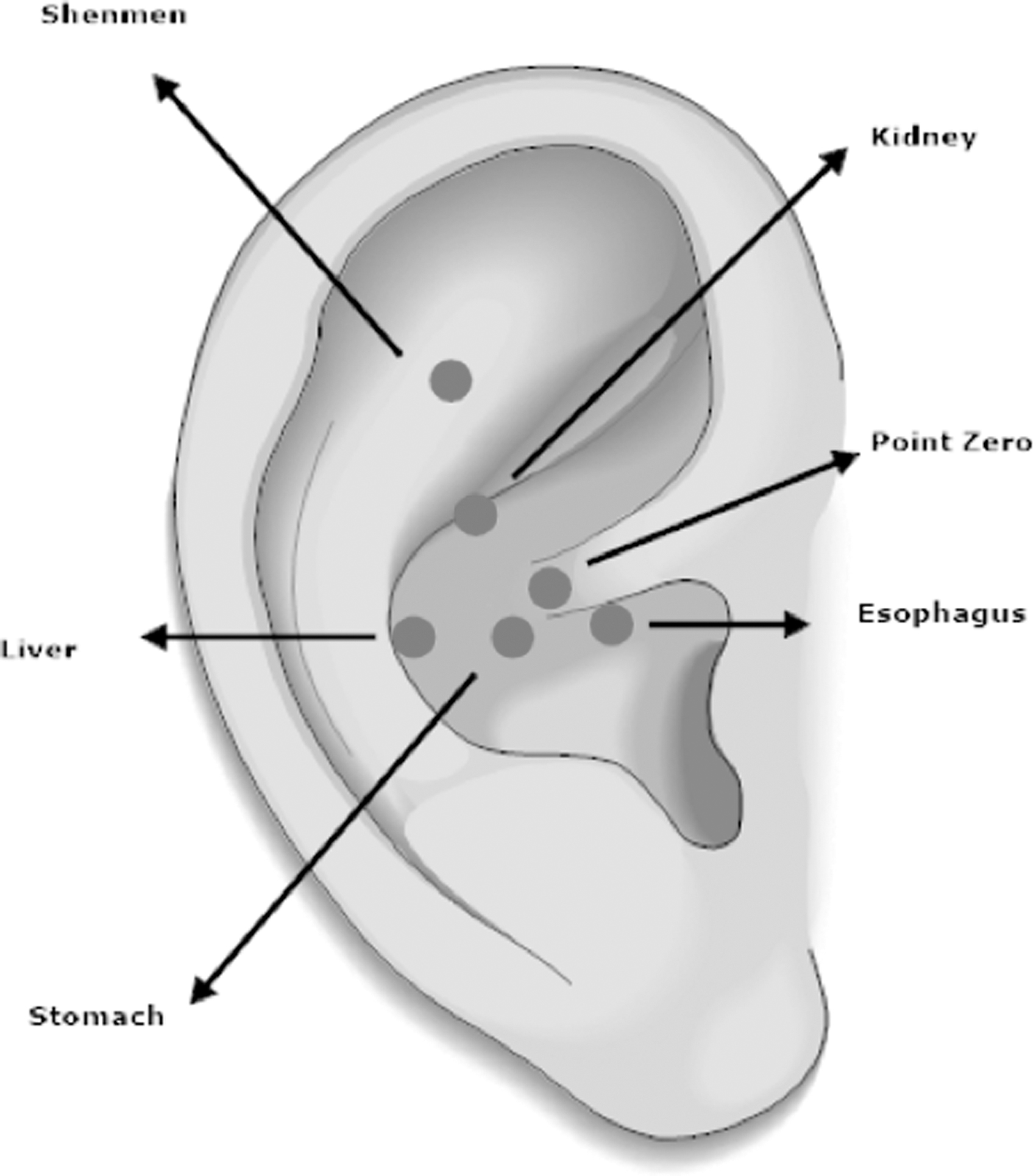
Ear acupuncture protocol.
In brief, Shenmen and Point Zero are traditionally indicated to calm the mind, commonly used to alleviate anxiety, and have been shown to induce parasympathetic activation. 39,40 The Kidney and Liver points, along with Shenmen, are part of the National Acupuncture Detoxification Association (NADA) protocol, which has been shown to be beneficial in improving energy and overall sense of well-being. 41 The Stomach and Esophagus points, along with Shenmen and Liver points, have also been frequently used in previous studies to treat chemotherapy-induced nausea and vomiting. 31 Acupuncture needles (SEIRIN®, No. 1, 15 × 0.16 mm) were inserted to a depth of ∼2 to 3 mm at each point on both ears and gently manipulated by hand for a few seconds. The needles were then retained for 30 min and gently manipulated again before removal.
Study endpoints
Feasibility
The primary aim of this study was feasibility, defined by (1) enrollment of at least 20 patients (80% of the target sample size) over the course of 3 months, (2) completion of at least 75% of the auricular acupuncture sessions, and (3) completion of at least 75% of the Edmonton Symptom Assessment System (ESAS) assessments.
Secondary endpoints
Secondary aims of the study included comparing changes in symptom burden and other patient-reported outcomes between education (cycle 1) and acupuncture (cycles 2 and 3) cycles. The following timepoints were evaluated during each cycle: T1: Day of chemotherapy infusion, before administration of educational materials (first cycle after enrollment) or acupuncture treatment (second and third cycles after enrollment) T2: Day of chemotherapy infusion, immediately after administration of educational materials (first cycle after enrollment) or acupuncture treatment (second and third cycles after enrollment) T3: Day 2 follow-up (one day after chemotherapy infusion) T4: Day 5 follow-up (4 days after chemotherapy infusion).
The following measures were used to evaluate symptom burden and other patient-reported outcomes.
Edmonton Symptom Assessment System-Revised Version
Edmonton Symptom Assessment System-Revised Version (ESAS-R) is a 9-item scale that assesses the current severity of common symptoms, including pain, fatigue, drowsiness, nausea, loss of appetite, shortness of breath, depression, anxiety, and lack of well-being. The ESAS-R has been validated in cancer populations. 42,43 Each symptom is scored from 0 to 10 on a 11-point numerical rating scale, with total scores ranging from 0 to 90. Higher scores indicate greater symptom burden. The ESAS Total Score is subdivided into physical, emotional, and well-being subscales. The ESAS Total, Physical, and Emotional Scores were used to assess symptom burden in this study. This measure was collected at all timepoints (T1–4) for each cycle of chemotherapy on study.
State Trait Anxiety Inventory-State
State Trait Anxiety Inventory-State (STAI-S) is a validated commonly used measure for evaluating patient's current state of anxiety and has been widely used in cancer populations. 44 It consists of 20 items, with each item scored from 1 to 4 and the total score ranging from 20 to 80. Higher scores indicate greater level of anxiety. 45 The STAI-S was also collected at all timepoints for each cycle of chemotherapy on study.
Multinational Association of Supportive Care in Cancer Antiemesis Tool
The Multinational Association of Supportive Care in Cancer (MASCC) Antiemesis Tool (MAT) is a validated questionnaire for assessing the severity of acute and delayed chemotherapy-induced nausea and vomiting. 46 It was collected at the T3 and T4 timepoints for each cycle of chemotherapy on study.
Safety
Any incidences of acupuncture-related adverse effects were noted by the treating acupuncturists during the acupuncture sessions. The acupuncturists used the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) v.4.0 to collect safety data related to adverse events, including skin bruising, hematoma, presyncope, syncope, and nausea. In addition, the study acupuncturists completed a study protocol and safety training session before starting the trial.
Statistical methods and sample size determination
All data were analyzed using SAS software (version 9.4; SAS Institute, Cary, NC). Patient-reported outcomes (ESAS-R, STAI-S, and MAT scores) during cycles 2 and 3 (acupuncture) at each timepoint were averaged and compared with outcomes from cycle 1 (education), using paired t tests.
There were three pairwise comparisons of interest for analyzing changes in ESAS-R and STAT-S scores between education and acupuncture cycles: change from T1 to T2; change from T1 to T3; and change from T1 to T4. The overall type-I error was set to be 0.1 (two-sided) and was equally divided among the three pairwise comparisons. Therefore, a two-sided p-value ≤0.033 was considered statistically significant. The severity of acute and delayed chemotherapy-induced nausea and vomiting were compared for days 2 and 5, respectively. A p-value ≤0.05 was considered statistically significant for MAT analyses.
The authors set the target accrual as the sample size required to detect the minimal clinically important difference (MCID) in their secondary endpoint, the within-patient change in ESAS-R Total Score. The MCID for ESAS-R Total Score has been reported in previous literature to be about a 6-point change. 47 Based on one-sample t tests, 80% power, a two-sided alpha of 0.033, and within-patient correlation of 0.6 between two assessments for the same cycle, the target sample size was estimated to be 26 patients.
Results
Patient characteristics
Patient baseline characteristics are shown in Table 1. The mean age of enrolled participants was 46.5 years (standard deviation [SD] = 9.2), and the mean weeks between breast cancer diagnosis and enrollment was 16.1 (SD = 7.9). A majority of the patients had stage II breast cancer (64.5%), followed by stage III (23.1%) and stage I (15.4%). For chemotherapy regimens, most patients were receiving doxorubicin plus cyclophosphamide (AC) (38.5%), followed by docetaxel and cyclophosphamide (TC) and AC plus paclitaxel (ACT) combination (23.1% each). At the time of study enrollment, 50% of patients had completed two chemotherapy cycles, 23.1% five cycles, and 11.5% three cycles.
Baseline Participant Characteristics
SD, standard deviation.
Feasibility
As shown in the CONSORT diagram (Fig. 2), all three a priori feasibility goals were met: (1) 26 patients, or 100% of the target sample size, were enrolled into the study over the course of 3 months, at an enrollment rate of about 8.7 patients per month; (2) all auricular acupuncture sessions were completed by 24 out of 26 patients (92.3%); and (3) all outcome assessments were completed by 22 out of 26 patients (84.6%).
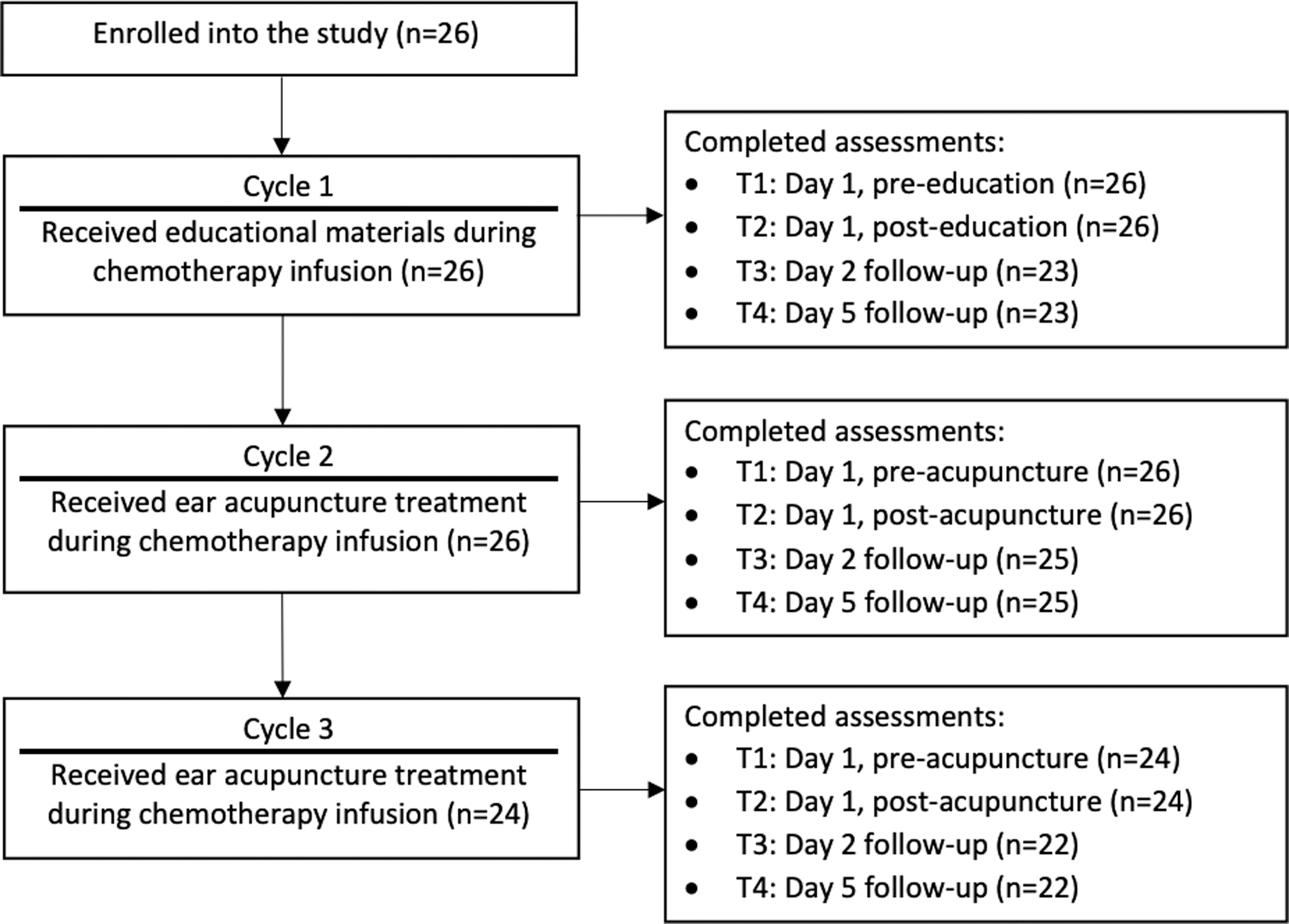
CONSORT diagram.
Secondary endpoints
Symptom burden
The results for ESAS-R Total, Physical, and Emotional Scores are shown in Table 2. Compared with the first chemotherapy after enrollment (education), there was a significant improvement of ESAS-R Total Score during the second and third chemotherapy cycles after enrollment (acupuncture) from day 1, pre-education/acupuncture (T1) to day 5 follow-up (T4) (−7.9 ± 13.6; p = 0.02). Evaluation of ESAS-R subscales show that changes in the ESAS-R Physical Score, but not the Emotional Score was significantly different between education and acupuncture cycles for this same time interval.
Changes in Edmonton Symptom Assessment System-Revised Version Symptom Burden Assessments
Patients received educational materials during the first of three cycles of chemotherapy on study.
Patients received auricular acupuncture during the second and third cycles of chemotherapy on study. ESAS-R scores from two acupuncture sessions are averaged and shown in table.
Changes in ESAS-R scores for cycles during which patients received acupuncture (A) were compared with that for the cycle during which patients received education materials (E).
Paired t test. Bold item is significant at p-value <0.033.
Higher score indicates greater symptom burden. Negative change in scores indicates reduction/improvement of symptom burden.
ESAS-R, Edmonton Symptom Assessment System-Revised Version; n/a, not applicable.
The other two pairwise comparisons, representing changes from T1 to immediate post-education/acupuncture (T2) and from T1 to day 2 follow-up (T3), were not significantly different between education and acupuncture cycles. Graphical representations of the nine ESAS-R subscale scores can be found in the Supplementary Data.
Anxiety and nausea
Table 3 shows the results for the STAI-S and MAT assessments. Of the three pairwise comparisons between education and acupuncture cycles for STAI-S scores, only the change from T1 to T2 in cycles 2/3 versus cycle 1 was statistically different (−3.3 ± 6.5 p = 0.02). For MAT assessments, the severity of nausea was significantly lower with acupuncture compared with education on day 2 (−1.3 ± 2.6; p = 0.04), but not on day 5 (−0.7 ± 2.1; p = 0.15). There were no significant differences in the frequency of MAT vomiting between education and acupuncture cycles.
Changes in State Trait Anxiety Inventory-State and Multinational Association of Supportive Care in Cancer Antiemesis Tool Assessments
Patients received educational materials during the first of three cycles of chemotherapy on study.
STAI-S and MAT assessments from two acupuncture sessions are averaged and shown in table.
Changes in STAI-S scores for cycles during which patients received acupuncture (A) were compared with that for the cycle during which patients received education materials (E).
Paired t test. Bold item is significant at p < 0.033 for STAI-S or p < 0.05 for MAT.
Higher score indicates greater anxiety. Negative change in scores indicates reduction/improvement of anxiety.
Higher score indicates worse nausea.
MAT, Multinational Association of Supportive Care in Cancer (MASCC) Antiemesis Tool; STAI-S, State Trait Anxiety Inventory-State; n/a, not applicable.
Adverse events
There were no acupuncture-related adverse events reported during the study.
Discussion
In a study of women receiving chemotherapy for early breast cancer, the authors found incorporation of an auricular acupuncture intervention during chemotherapy infusion to be feasible, based on their achievement of a priori feasibility goals. The authors' target sample size of 26 patients was enrolled into the study during a 3-month study period, and >75% of participants completed all acupuncture sessions and outcome assessments. Auricular acupuncture was also found to be beneficial and without any major adverse effects in reducing symptom burden on day 5, nausea on day 2, and anxiety immediately post-acupuncture. These findings suggest that auricular acupuncture is a potentially effective and safe intervention for improving symptom burden, acute nausea, and anxiety in this population and can be delivered while patients are receiving chemotherapy.
Anxiety and nausea are among the most common symptoms experienced by breast cancer patients. In a recent systematic review, which included 36 studies with over 16,000 patients, the prevalence of anxiety among breast cancer patients was found to be 41.9%. 48 Although management of chemotherapy-induced vomiting has improved with advances in antiemetic medications, chemotherapy-induced nausea is still poorly understood and remains highly prevalent. 49
In addition to anxiety and nausea, it is common for breast cancer patients to simultaneously experience many other distressing symptoms, including fatigue, depression, and pain, which contribute to the overall symptom burden. 8 Because these symptoms can interact and exacerbate one another, comprehensive assessment and management of symptom burden are increasingly recognized to be an important part of cancer supportive care research and practice. 11 –13
In this study, the overall symptom burden, as assessed by the ESAS-R Total Score, was 22.2 ± 13.2 on the day of chemotherapy infusion during cycle 1. Although this score is generally classified as mild in severity, 50 during cycle 1 on study (education), there was a clinically meaningful increase (7.4 ± 13.1 points) in overall symptom burden between T1 (day 1, before delivery of the education materials) and T4 (day 5). This symptom burden trajectory is consistent with findings from previous longitudinal studies, which suggest that symptoms generally worsen and peak in severity a few days to a week after chemotherapy infusion. 51,52
A growing body of evidence suggests that acupuncture may be used to help attenuate cancer-related symptoms. 27,28 In a recent retrospective analysis of 375 patients receiving outpatient acupuncture treatment in a comprehensive cancer center, acupuncture was associated with a significant improvement in ESAS Total, Physical, and Emotional scores. 53 Many other clinical trials have also demonstrated that acupuncture improves a wide range of symptoms in cancer populations, thereby addressing the multidimensional aspects of symptom burden. 18 –23 Previous studies also suggest that auricular acupuncture is effective for reducing cancer-related pain and chemotherapy-induced nausea and vomiting. 30,31
Similar to general body acupuncture, auricular acupuncture has also been shown in previous studies to improve vagal tone and regulate autonomic functions of cardiovascular, respiratory, and gastrointestinal systems. 54 Specifically, in the case of auricular acupuncture, these effects are thought to be mediated through an activation of the auricular branch of the vagus nerve (ABVN), which projects onto the nucleus of the solitary tract (NTS), an important brain region involved in modulating autonomic functions. 54,55 However, there is less information in the literature about the potential benefits of auricular acupuncture on multiple symptoms or the overall symptom burden in cancer populations, especially during chemotherapy.
To the authors' knowledge, this was the first study to investigate the impact of an auricular acupuncture intervention delivered on-site during chemotherapy infusion on symptom burden. The authors' preliminary data show that auricular acupuncture is effective in reducing symptom burden in women with breast cancer receiving chemotherapy. In the first cycle after enrollment (education), there was an average increase in symptom burden from day 1, pre-education to day 5 of 7.4 points.
Conversely, in the second and third cycles after enrollment (acupuncture), there was an average decrease in symptom burden of 0.5 points during the same time interval. This finding suggests that auricular acupuncture may help prevent worsening of symptoms that normally occurs several days after chemotherapy infusion. Auricular acupuncture was also significantly effective in attenuating anxiety immediately postacupuncture and nausea on day 2 follow-up. Although preliminary, these findings support the potential effectiveness of auricular acupuncture in moderating multiple symptoms commonly experienced by breast cancer patients undergoing chemotherapy.
Notably, for breast cancer patients who need to frequently travel to medical centers for care, commuting is considered a significant burden and has been shown to affect their treatment decisions. 34 Travel difficulty has also been identified as one of major barriers to patients' willingness to participate in acupuncture trials. 56 In this study, no extra commuting was required for participation, as acupuncture was administered during patients' scheduled visits for chemotherapy infusion. Although the authors did not assess travel burden or reasons for participation, the lack of extra commuting likely increased patients' willingness to participate in this study. It would be important to collect these data in future studies, as to ascertain whether timing of acupuncture administration during chemotherapy increased patient interest and/or contributed to the overall benefit of the treatment.
There are several limitations in this study. First, this was a pilot feasibility study with a small sample size, so data pertaining to patient-reported outcomes should be considered preliminary. It is also important to note that improvements in symptoms were not statistically significant across all timepoints. It would be interesting to investigate the temporal sequence of how different symptoms improve over time in future studies.
This was also not a randomized clinical trial; it was a single-arm prospective study, wherein the same group of individuals was followed for three cycles of chemotherapy. With this design, it is impossible to definitively state that acupuncture was responsible for the differences in symptom burden in later versus earlier chemotherapy cycles, as these improvements could possibly be related to the natural course of the symptom trajectory or regression to the mean.
In addition, there was considerable variability among participants as to how many cycles of chemotherapy they had received before study enrollment, which could have confounded the study results. It is also possible that improvements in nausea may have been due to changes in antiemetic regimens. However, given that all patients had already completed two or more cycles of chemotherapy before enrolling into this study, it is likely that antiemetic regimens were optimized before study enrollment for most patients and less likely that adjustments in antiemetic medications were responsible for the improvement in nausea. Finally, patients were not blinded to the acupuncture treatments, so it is possible that their expectations of clinical benefits influenced treatment outcomes.
Conclusion
This pilot study demonstrated that it is feasible to treat women with early breast cancer undergoing chemotherapy with auricular acupuncture during chemotherapy infusion. The authors' preliminary findings show that auricular acupuncture is potentially effective for improving symptom burden, anxiety, and acute nausea. Given the multiple co-occurring symptoms experienced by breast cancer patients undergoing chemotherapy, these findings provide the groundwork for a future large-scale randomized controlled trial, evaluating the impact of an auricular acupuncture intervention delivered on-site during chemotherapy on symptom burden and other patient-reported outcomes in this population.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Dana-Farber/Harvard Cancer Center. Informed consent was obtained from all participants included in this study.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors thank study acupuncturists Anne Drogin, Zhi Ping Li, Dongyan Yu, Yue Zhang, and Xiaoqin Zhao as well as research staff Winnie Ng and Roxanne Quinn for their contribution to this study.
Authors' Contributions
W.L., J.A.L., and I.H.S. conceived of the study and planned the study design. J.A.L., W.Y.C., C.C.B., A.P., R.M.J., S.M.T., and R.A.F. helped with patient recruitment. A.G.-H. provided statistical expertise and analyzed the data. E.Y. drafted the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Comprehensive and Integrative Medicine Institute (CIMI), South Korea (Grant No.: 090-091-3000-3038-301-320-01). E.Y. is supported by NIH/NCCIH training grant (T32 AT000051). The funders had no role in the study design, collection, analysis, and interpretation of data, and preparation of the article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.