
Abstract
Objective:
The aim of this study is to investigate the association between acupuncture therapy and the risk of fracture in patient with osteoarthritis (OA).
Design:
The authors performed a 1:1 propensity score-matched cohort study to analyze patient with OA between January 1, 1997 and December 31, 2010 through the Taiwanese National Health Insurance Research Database. Patients who received acupuncture therapy from the initial date of diagnosis of OA to December 31, 2010 were included in the acupuncture cohort. Patients who did not receive acupuncture during the same follow-up period were defined as the no-acupuncture cohort. A Cox regression model was used to adjust for sex, age, comorbidities, prescription, and surgical experiences. Hazard ratios (HRs) were compared between the two cohorts.
Results:
A total of 3416 patients were identified after 1:1 propensity score matching. The patients had similar basic characteristics. In the final analysis, 292 patients in the acupuncture cohort (30.06 per 1000 person-years) and 431 patients in the no-acupuncture cohort (56.08 per 1000 person-years) developed fractures (adjusted HRs 0.57, 95% confidence interval 0.49–0.67). A reduced cumulative incidence of fracture was found in the acupuncture cohort (log-rank test, p < 0.001). The association between acupuncture and reducing the fracture incidence was independent of sex, comorbidities, drugs use, and surgical experiences.
Conclusion:
Their results revealed the association between acupuncture therapies and a reduced incidence of fracture development in patients with OA. This finding provides noteworthy ideas for further research.
Introduction
Thousands of years ago, acupuncture therapy was applied to treat diseases using needles to puncture acupoints on the skin. Acupuncture is used to redistribute energy in the human body to correct the imbalance caused by diseases. Traditionally, patients prefer to undergo acupuncture therapies for respiratory diseases, neurological problems, gastrointestinal discomfort, and musculoskeletal disorders. 1 Currently, the World Health Organization has recommended 64 indications that are suitable for acupuncture therapy, including arthritis, based on clinical evidence. 2 The role and effect of acupuncture therapies have been established gradually.
Osteoarthritis (OA) is the most common type of arthritis and can cause chronic disability, especially in elderly individuals. 3 The prevalence of knee OA increases from 8% in men aged 45–49 years to 22% in men aged over 80 years and 13%–55% in women. 4 Greater than 37% of Taiwanese individuals over 50 years old have OA of knee. 5
Although age and genetic and inflammatory reactions of joints have been reported as risk factors for OA, the precise etiology is not completely understood. 6 Several pro-inflammatory and anti-inflammatory cytokines, including interleukin (IL)-1β, IL-4, IL-6, IL-10, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ, have been detected in OA joints and have roles in the mechanism, leading to OA. OA development is associated with synovial membrane inflammation, subchondral bone remodeling, and cartilage destruction. 7
Deformity and limited range of motion of joints are observed in severe OA cases. 8 Pain control agents and surgery are well-known interventions for OA. 9 However, joint pain and motion restriction may still cause immobilization in OA patients, which are great risks of osteoporosis and fracture. 10 The relationship between OA and osteoporosis has been widely discussed in recent years, and both factors are related with obesity. 11
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed for OA treatment. 9 Patients should be closely observed when they use these medications because NSAIDs have the risks of inducing gastrointestinal bleeding, renal impairment, and cardiovascular events. 12 These side effects cause an increasing number of OA patients to accept acupuncture therapy for symptom relief. Significant improvements in pain (standardized mean difference [SMD], −0.35; confidence interval [CI], −0.55 to −0.15) and physical function (SMD, −0.35; CI, −0.56 to −0.14) through acupuncture in OA patients have been reported by a meta-analysis study. 13
Acupuncture is also helpful for regulating pro-inflammatory cytokines and controlling the inflammatory process. 14 However, the authors do not know much about the association between acupuncture and the possible comorbidities of OA, such as fracture.
In 1995, the National Health Insurance Administration (NHIA) in Taiwan started the National Health Insurance (NHI) program, and Traditional Chinese Medicine (TCM) services were reimbursed by the NHI program in 1996. 15 In 2021, NHI covered 99.6% of the population in Taiwan. In other words, the information from the Taiwanese National Health Insurance Research Database (NHIRD) could represent almost the entire Taiwanese population. The NHIRD is a large-scale and long-term follow-up medical database, and it has the advantage of sampling bias prevention. 16 Acupuncture is a popular TCM intervention in Taiwan. With the help of the NHIRD, the authors wanted to determine the association between acupuncture therapy and the risk of fracture in Taiwanese patients with OA.
Materials and Methods
Data sources
The authors conducted a nationwide, population-based, 1:1 propensity score-matched retrospective cohort study using data derived from the NHIRD. The data source was the Insurance Database 2000, which offered all the original claims data of 1 million beneficiaries randomly sampled from the registry of all beneficiaries in 2000. No significant differences in sex, age, birth year, or average insured payroll-related costs were noted between the general population and their samples. The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) was used in this database to code diseases.
Because personal information was removed from their database, all records were secondary data. Thus, informed consent is not needed. Their study was approved by the research ethics committee of China Medical University and Hospital (CMUH104-REC2-115).
Study cohort identification
Patients newly diagnosed with OA from January 1, 1997 to December 31, 2010 were identified (Fig. 1). Then, patients with at least two ambulatory or inpatient claims with the diagnosis of ICD-9-CM codes 715 and 721 were included. The authors excluded patients younger than 18 years and those with incomplete age or sex data and interrupted health insurance services during the follow-up period. Participants who underwent acupuncture treatment from the initial diagnosis of OA to December 31, 2010 were enrolled in the acupuncture cohort. Those who did not accept acupuncture intervention in the same period were defined as the no-acupuncture cohort.

Study population flow chart. Total 4253 patients with osteoarthritis were newly diagnosed from 1997 to 2010. After 1:1 propensity score-matched cohort by sex, age, comorbidities, drugs used, and surgery experience, 1708 patients were included in the acupuncture cohort and no-acupuncture cohorts, separately. LHID2000, Longitudinal Health Insurance Database 2000; NHI, National Health Insurance.
Propensity score approaches were used to minimize confounding factors based on the indication of acupuncture treatment. Through multiple logistic regression analysis, 1:1 propensity score matching was performed based on age, sex, drug use, comorbidities, and surgical experience. 17 Finally, the numbers of patients in the acupuncture and no-acupuncture cohorts were the same. The index date was defined as the first time that patients accepted acupuncture therapy. Immortal time was defined as the period from initial diagnosis of OA to the index date. The incidence of fracture is their main outcome, which was defined as patients with at least two ambulatory or inpatient claims with the diagnosis of ICD-9-CM codes 800–829.
Covariate assessment
The sociodemographic factors in their study were age and sex. The authors divided patients into three subgroups based on age: 18–39, 40–64, and ≥65 years. Comorbidities were defined as conditions that occurred more than equal to two times in outpatient or inpatient records coded by ICD-9-CM before the primary diagnosis of OA, including hyperlipidemia (ICD-9-CM code 272), diabetes mellitus (DM; ICD-9-CM code 250), hypertension (HTN; ICD-9-CM codes 401–405), congestive heart failure (CHF; ICD-9-CM codes 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, and 428.0), depression (ICD-9-CM codes 296.2–296.3, 300.4, and 311), alcoholism (ICD-9-CM codes 291, 303, 305.00–305.03, 790.3, and V11.3), obesity (ICD-9-CM codes 278 and A183), and tobacco use (ICD-9-CM code 305.1).
Types of acupuncture and disease categories in the acupuncture cohort
Acupuncture types were identified by manipulation codes, including electroacupuncture (B43, B44, B86, B87, B88, B89, and P33032) and manual acupuncture of TCM type (B41, B42, B45, B46, B80, B81, B82, B83, B84, B90, B91, B92, B93, B94, P27041, P31103, P32103, and P33031). The disease categories were classified by ICD-9-CM codes for patients with OA who underwent acupuncture.
Statistical analyses
The authors used SMD to compare the baseline characteristics of the acupuncture and no-acupuncture cohorts. Negligible differences in mean values or proportions between the two cohorts were defined as <0.1 standard deviation. Cox proportional hazard regression analysis was conducted to estimate crude and adjusted hazard ratios (HRs) of acupuncture therapy, sex, age, drugs used, and comorbidities. The Kaplan–Meier method and the log-rank test were performed to reveal the difference between the two cohorts in the development of fracture. Statistical analysis was performed, and figures were generated using SAS 9.4 (SAS Institute, Cary, NC) and R software (R Foundation for Statistical Computing, Vienna, Austria). The authors defined p < 0.05 in two-tailed tests as statistically significant.
Results
A total of 5572 patients were newly diagnosed with OA with at least 2 clinical visits in the NHIRD from January 1, 1997 to December 31, 2010 (Fig. 1). Patients without detailed information, younger than 18 years old, or with a fracture history before the diagnosis date of OA were excluded. The number of included patients was 4253 with 1890 patients in the acupuncture cohort and 2363 patients in no-acupuncture cohort. After 1:1 frequency matching was performed based on age, sex, drugs used, comorbidities, surgical experiences, diagnosis year of OA, and index year to compare the two groups, each cohort had 1708 participants.
Table 1 shows the baseline characteristics of both cohorts with similar distributions of age, sex, comorbidities, drugs used, and surgical experiences. Female and middle-aged (40–64 years old) participants were the predominant groups in both cohorts. HTN was the most common comorbidity, and greater than 51% of patients had this condition. Among patients with OA, 23% had DM, 40% had hyperlipidemia, 5% had CHF, and 17% had depression. The proportions of patients with alcoholism, tobacco dependence, and obesity were similar in the two cohorts. NSAIDs were the most common prescriptions in both cohorts; over 99% of patients were prescribed NSAIDs. Statin agents were used by 35% of participants.
Characteristics of Osteoarthritis Patients According to Accept Acupuncture or Not
The mean (median) of follow-up period were 5.69 (5.12) and 4.50 (4.09) years for acupuncture cohort and compared cohort.
NSAID, nonsteroidal anti-inflammatory drug; SD, standard deviation; TCM, Traditional Chinese Medicine.
Manual acupuncture was practiced in 87% of patients, 2% had only electroacupuncture, and the other 11% of participants experienced a combination of two interventions. The mean duration from diagnosis of OA to the first acupuncture therapy was ∼980 days. Mean times of acupuncture visits were 11.14. Before the endpoint, 6% of patients in each cohort underwent total knee and hip replacements.
During the follow-up period, 723 patients developed fractures (Table 2). The incidence of fracture in OA patients increased with age, and the elderly had a higher risk. The adjusted HRs of the 40- to 64-year-old and over 65-year-old groups were 2.11 and 3.91, respectively. Patient with depression had a higher risk of fracture, and the adjusted HR was 1.31. The acupuncture cohort had a lower cumulative incidence of fracture (log-rank test, p < 0.001, Fig. 2).
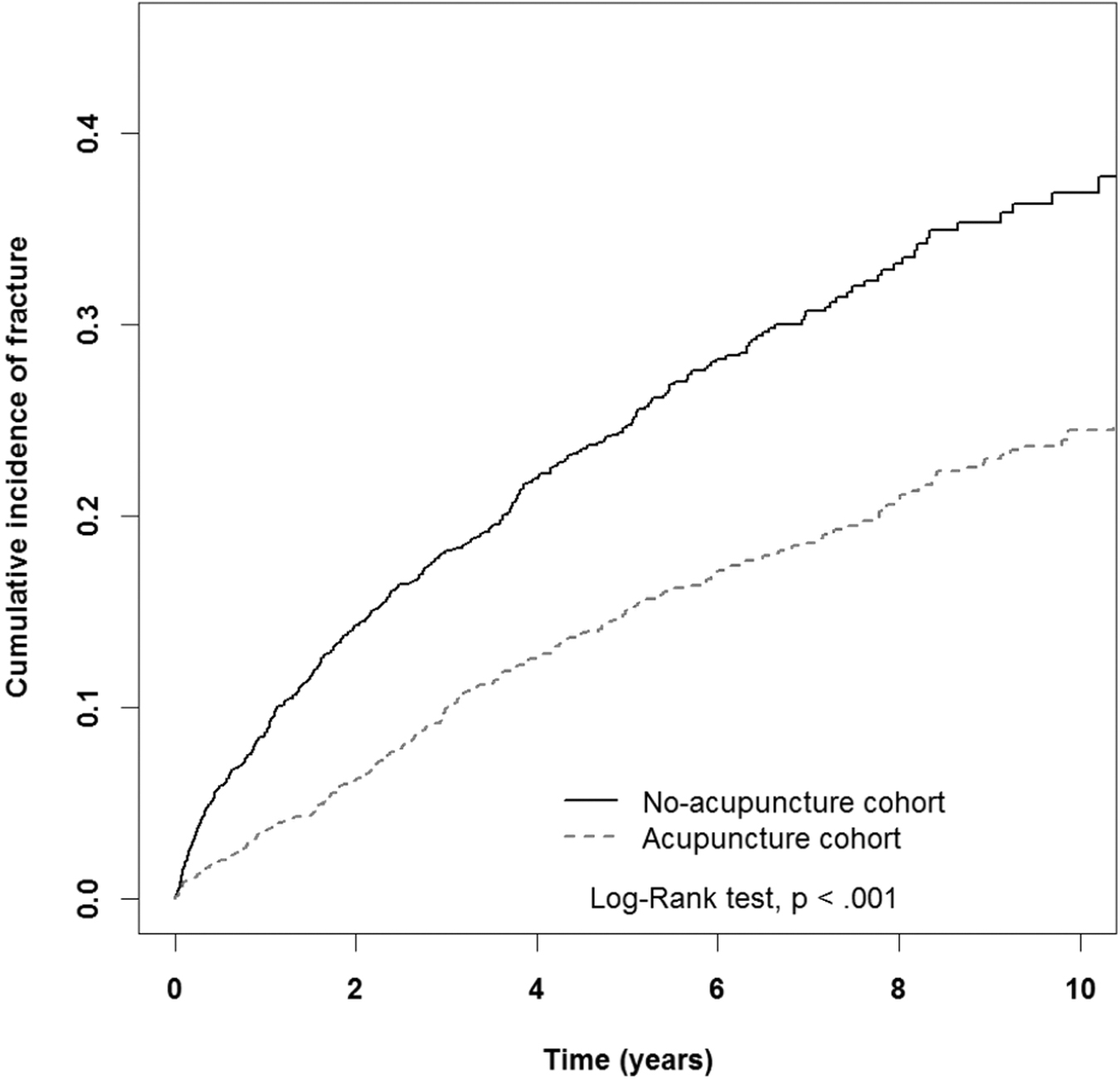
Cumulative incidence of fracture in acupuncture (dashed line) and the no-acupuncture cohort (solid line). Patients in acupuncture group had lower incidence of fracture (log-rank test, p < 0.001).
Cox Model with Hazard Ratios and 95% Confidence Intervals of Fracture Associated with Accepted Acupuncture and Covariates Among Osteoarthritis Patients
Crude HR represented relative HR.
Adjusted HR: adjusted for accepted acupuncture, age, gender, diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, depression, obesity, NSAID, and statin in Cox proportional hazard regression.
CI, confidence interval; HR, hazard ratio; NSAID, nonsteroidal anti-inflammatory drug.
Table 3 reports that 292 patients in the acupuncture cohort (30.06 per 1000 person-years) and 431 patients in the no-acupuncture cohort (56.08 per 1000 person-years) developed fracture (adjusted HR 0.57, 95% CI 0.49–0.67). The results of fracture prevention were observed in both the male and female groups. The adjusted HR was 0.54 in the female group (95% CI 0.45–0.65), and the adjusted HR was 0.66 in the male group (95% CI 0.49–0.88). Patients over 40 years of age had a lower risk of fracture after acupuncture therapy (adjusted HR 0.5, 95% CI 0.41–0.63 in the 40–64-year-old group; adjusted HR 0.66, 95% CI 0.53–0.82 in the ≥65-year-old group).
Incidence Rates, Hazard Ratio, and Confidence Intervals of Fracture for Osteoarthritis Patients Who Accepted and No-accepted Acupuncture in the Stratification of Sex, Age, Comorbidities, Drug Used, and Surgery Experience
Crude HR represented relative HR.
Adjusted HR: adjusted for accepted acupuncture, age, gender, diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, depression, obesity, NSAID, and statin in Cox proportional hazards regression.
Comorbidity included diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, depression, and obesity; Western drugd included oral steroid, NSAID, and statin.
<0.05; **<0.01; ***<0.001.
CI, confidence interval; HR, hazard ratio; IR, incidence rates; NSAID, nonsteroidal anti-inflammatory drug.
Regardless of whether the patient had comorbidities, the final results still supported the association between acupuncture therapy and reducing the fracture incidence. Coadministration with NSAIDs or statins did not affect the final results. Interventions of total hip and knee replacement could also not change the advantage of fracture prevention from acupuncture.
Table 4 reveals the top ten disease categories for which the patients with OA in the acupuncture cohort received acupuncture treatment. Musculoskeletal system and connective tissue disorders (ICD-9-CM codes 710–739) were the major problems leading to acupuncture treatment and were also highly related to OA.
The Distribution of Acupuncture Cohort Was Listed by Disease Categories/Diagnosis in Patients with Osteoarthritis During Follow-Up Period
Discussion
To the best of their knowledge, this is the first study to reveal the association between risk controlling of fracture and acupuncture treatment in patients with OA. Therapy results of acupuncture in OA are typically reported based on a visual analog scale; Western Ontario McMaster Osteoarthritis Index; profile of quality of life in chronically ill; 36-item short form for physical health; and 50-ft walk time. 18 Studies conducted in different countries, such as Germany, Spain, and Israel, have demonstrated the effectiveness of acupuncture in the treatment of OA. 19,20
The reduced risk of fracture in OA patients after acupuncture has never been reported. Their results showed that the effectiveness of acupuncture intervention was independent of sex, comorbidities and drugs (NSAIDs), and surgery. Joint disorder is the top 7 diagnostic reason for acupuncture visits in Taiwan, and greater than 40% of patients have accepted acupuncture therapy according to their results. 21
A large-scale, comprehensive, and long-term follow-up database, such as the NHIRD in Taiwan, is helpful for decreasing participation and selection biases given its large sample size. The basic characteristics of enrolled patients with OA in this study were compatible with the worldwide epidemiology of this disease: female predominance and high prevalence of those aged over 40 years old. 22 Similar characteristics were noted between the two cohorts after 1:1 propensity score matching.
Hyaluronic acid is a lubricant and shock absorber and helpful for relieving symptoms of OA. Hyaluronic acid is also commonly used in a procedure called viscosupplementation, and the FDA has approved the use of hyaluronic acid for the treatment of OA. 23 However, viscosupplementation was not reimbursed by the NHIA in Taiwan until 2000, and its effectiveness remains controversial. The authors did not compare the effectiveness of viscosupplementation with that of acupuncture. 24 No evidence has demonstrated that NSAIDs or hyaluronic acid is helpful for maintaining bone density, but acupuncture treatment has been found to potentially increase bone mineral density (BMD). 25 Further research is needed to determine the role of acupuncture in patients undergoing viscosupplementation.
Pro-inflammatory and anti-inflammatory cytokines are significantly related to the symptoms of OA. IL-1β, IL-6, and TNF-α are major cytokines and are generally catabolic, and IL-1 and TNF-α can cause the destruction of articular cartilage. 26 The anti-inflammatory cytokines IL-4, IL-10, and IFN-γ are inhibitory cytokines that can block the reactions of catabolic cytokines. 27 Stimulation by acupuncture could regulate these cytokines and contribute to anti-inflammatory reactions. 28
Osteoporosis is the major risk factor for fracture in patients over 50 years old in Taiwan, but most fractures in young adults are due to accidents. 29 However, the relationship between OA and osteoporosis is controversial. Although an inverse relationship has been reported, no correlation between OA and osteoporosis and worse BMD in OA patients has also been reported. 30,31 Higher production of IL-1β, IL-6, and TNF-α has been noted in patients with osteoporosis. 32 Bone loss in the hip, spine, and total body is associated with these pro-inflammatory cytokines. 33,34 Cytokine balance mediated by acupuncture therapy may represent a possible mechanism to decrease the incidence of fractures in middle-aged and older OA patients in their study.
At the beginning of OA, bone formation is increasing, which could explain the results of higher BMD in OA patients in some cross-sectional studies. 35,36 However, when patients experience muscle weakness and postural instability due to pain and restriction of the joint, a negative effect of BMD can be observed. 37 In other words, worse limb functions could contribute to an increased incidence of fracture. Acupuncture treatment has the advantages of relieving joint pain and improving muscle power, which could be beneficial for not only musculoskeletal disorders but also degenerative disease. 38 In contrast, through acupuncture therapy, stroke patients could preserve their limb function and attain a better quality of life. 39 This notion is also the basis of another hypothesis regarding fracture prevention in OA patients using acupuncture treatment.
Not only fractures but also comorbidities of OA, including DM, HTN, and CHF, are correlated with inflammatory reactions. 40 –42 The anti-inflammatory effect of acupuncture has been reported in several diseases, such as rheumatoid arthritis, inflammatory bowel disease, asthma, rhinitis, and vasculitis. The hypothesis of releasing calcitonin gene-related peptides and vasodilation effects are possible anti-inflammatory mechanisms of acupuncture. 28 Furthermore, acupuncture also has positive effects on risk factors for osteoporosis, such as smoking, drinking, and rheumatoid arthritis. 43 –45 But there is no direct evidence to support the correlations between risk factor control by acupuncture and fracture prevention. However, the authors still note the potential benefit of acupuncture in these studies, but more investigations are warranted to prove these advantages.
There are several limitations in their study. The NHIRD does not include detailed information about the severity of OA, such as information from the Kellgren–Lawrence Grading Scale, and social and work disabilities. The authors used a 1:1 propensity score match to minimize the differences between the two cohorts, 1,46 and the percentages of patients administered NSAIDs were similar. Basic characteristics and personal habits, such as height, weight, smoking and drinking consumption, exercise, and diet habits, were difficult to ascertain from the NHIRD. Thus, the authors tried to define these features based on the diagnosis of obesity, alcoholism, and tobacco use, and a 1:1 propensity score match was used to eliminate differences.
The distribution of patients with these problems was similar, and these comorbidities and surgical experiences did not change the effects of acupuncture on fracture prevention in patients with OA. The acupoints for OA treatment could not be found from NHIRD. And the dose of acupuncture therapy, including frequency and duration, is variable and depends on the severity of OA and the experience of the TCM doctors. Although the causation could not be offered by their study, their study still reveals the association between acupuncture use and the development of fracture.
Conclusions
The results of their study reveal the association between reducing the incidence of fracture by acupuncture in OA patients over 40 years of age in Taiwan. This study provides important ideas for further studies to investigate the relationship more comprehensively.
Data Availability Statement
The datasets the authors used in this study were released by the Taiwan NHIRD (
Footnotes
Authors' Contributions
Dr. Chia-Yu Huang designed, performed the research, analyzed, and helped writing the article; Dr. Mei-Yao Wu interpreted the data; Dr. Ming-Cheng Huang interpreted the data; Mr. Greg Zimmerman interpreted the data; Dr. Liang-Yo Yang interpreted the data; Ms. Cheng-Li Lin analyzed the article; Dr. Sio-Ian Tu conceptualized the study, drafted the article, and finalized the article; Dr. Hung-Rong Yen conceptualized the study, supervised the study, and finalized the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported by the “Chinese Medicine Research Center, China Medical University” from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan (CMRC-CHM-1). This study was also supported, in part, by China Medical University (CMU103-BC-4-2), China Medical University Hospital (DMR-108-011 and DMR-110-002), Ministry of Science and Technology (108-2638-B-039-001-MY2 and 109-2622-8-039-002-TB1), and health and welfare surcharge of tobacco products, China Medical University Hospital Cancer Research Center of Excellence, Ministry of Health and Welfare (MOHW109-TDU-B-212-114004 and MOHW110-TDU-B-212-144024), Taiwan.
None of the funders and institutions listed had a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.