
Abstract
Background:
The prevalence of anxiety disorders in primary care is 20%, with 41% of these patients reporting no current treatment. Patients with anxiety are also more likely to have comorbidities with other medical and/or psychiatric conditions, increasing medical costs. Integrating mindfulness-based interventions (MBIs) into a group medical visit (GMV) format has been successfully used to manage pain, but limited literature is available on the effectiveness of these visit formats for patients with stress and anxiety.
Methods:
Ninety-two adult patients with self-reported stress and/or anxiety were recruited from three university outpatient primary care clinics between 2016 and 2019. Participants attended at least 4 of 6 weekly GMVs focused on MBIs. Change in heart rate, blood pressure, Generalized Anxiety Disorder-7 (GAD-7) score, and 9 item Patient Health Questionnaire (PHQ-9) score from the first to last visit were evaluated using mixed effect linear regression models.
Results:
Both GAD-7 (estimated change: −5.1; 95% confidence interval [CI]: −6.4 to −3.7) and PHQ-9 (estimated change: −3.3; 95% CI: −4.3 to −2.2) scores significantly decreased from the first to last visit. These reductions were independent of age, sex, and number of visits attended. No significant changes in heart rate or blood pressure were found.
Conclusions:
Significant reductions in anxiety and depression in primary care patients were observed after a 6-week standardized mindfulness based GMV. Intergroup variability was not significant indicating that the intervention is reproducible over time and across providers. Future randomized controlled trials with appropriate controls will better evaluate which components of the intervention account for findings.
Introduction
The prevalence of anxiety disorders in urban primary care settings is estimated at 19.5% with 41% of patients reporting no current treatment. 1 In addition, anxiety and depression in the general population increased threefold during the COVID pandemic. 2 Patients with anxiety disorders have high rates of comorbidity with physical symptoms and medical and psychiatric conditions, including depression, 3 increasing the overall burden of medical costs. 4 There is also a gender discrepancy with twice the prevalence of anxiety in women compared to men. 5 Finally, patients prefer to seek care for anxiety disorders in primary care. 6
Mindfulness-based interventions (MBIs) in groups are effective in reducing perceived stress, 7 depression, and anxiety 8,9 with effect sizes at or above those of standard medication therapy for depression and anxiety. 10 Mindfulness also reduces inflammation and increases immunity. 11 Finally, mindfulness has been associated with changes in cellular DNA functioning. Telomeres are terminal DNA protein structures stabilizing DNA, synthesized by telomerase. 12 Shorter telomeres have been associated with increased mortality. 13 Stress, especially prolonged chronic stress, is associated with shorter telomeres and reduced telomerase levels. 14,15 MBI shows the opposite, with increases in telomerase activity and length. 11,16
MBIs were introduced into medical settings in the form of Mindfulness Based Stress Reduction (MBSR) for medical patients with chronic pain. 17 MBSR is an 8-week, 2.5-h training that focuses on increasing moment to moment awareness in a nonjudgmental and accepting manner. 17,18 Other MBI programs have emerged, including compassion-based meditations 19 and mindfulness based cognitive therapy. 20 Various forms of structured MBI for anxiety have been reported, including 2- to 3-day retreats, 2- to 3-week sessions, and even smartphone applications. 10,19,21 Common elements to these MBI include a structured curriculum with regular meetings in a group format, facilitation by an experienced meditator, focus on instruction of meditation, and encouragement of home practice. 10
Group medical visits (GMVs) are visits where a provider sees several patients simultaneously in a 1.5- to 2-h session(s), increasing access with high provider and patient satisfaction. 22 Integrating mindfulness interventions into a GMV format has been used to successfully manage pain 23 but there is sparse literature on the effectiveness of a mindfulness based GMV for patients with stress or its associated anxiety and depression.
A 6-week educational and mindfulness based GMV for primary care patients with stress or anxiety is described, and associated clinical changes are presented. Anxiety and depression were primary outcomes given their relationship with stress and health outcomes. 24
Stanford University Institutional human subjects review board approval was obtained (Protocol No. 47943).
Materials and Methods
Group medical visit
The GMVs were 2 h, sequential 6-week sessions conducted by one to two providers (physician and/or nurse practitioner). The content reproduced what was typically covered in a 1:1 office visit for stress or anxiety (stressors, symptoms, mechanisms of stress, mindfulness, barriers to change, and lifestyle changes for stress). These topics led to establishing six separate 2-h sessions. A curriculum was developed for each week containing the format, educational topics, meditations, and time allotments. Over the course of the study, three different providers with at least 5 years of personal meditative practice experience facilitated the GMVs. Provider training included 1-h presession reviews of each week's curriculum, participation in a full 6-week session, then facilitation with the senior provider, and finally lead facilitation of sessions with postsession review and evaluation with the senior provider.
Each visit began with one-to-one sessions lasting ∼5 min each between patient and provider. Blood pressure and heart rate were obtained, and medication and general meditative practice were reviewed during this portion of the visit. Participants, ranging from 3 to 13, then met as a group for the remainder of the visit which covered: (1) 5–10 min of short breathing meditation, (2) 30 min review of previous week's action plan and meditation practice, (3) 20- to 30-min educational presentation, (4) a longer 20-min meditation that varied by week, (5) 5–10 min review of the meditation practice experience, and (6) 5–10 min for development of individual action plan for the subsequent week and adjournment.
Different educational topics were presented (Table 1) weekly. Patients actively participated with questions and shared experiences. In the group setting, the providers facilitated the discussion, presented the weekly topic, and led the mindfulness practice. Each week a different type of mindfulness practice was introduced, including mindful breathing, guided imagery, compassion meditation, body scan, and movement meditation (yoga). All practices were standardized and delivered in a consistent format. A yoga instructor led the session on week 6. Patients were encouraged to practice any of the meditations throughout the week. The patient's primary care provider was contacted when depression scores included suicidal ideation and when patients were interested in starting medications.
Education Topics Covered Each Week
Recruitment and study design
The study was conducted at three university-based outpatient primary care clinics from January 19, 2016 to January 10, 2019. Adult patients (age 18+ years) with either self or provider identified stress and anxiety were referred. Inclusion criteria included English speaking and ability to attend at least 4 of the 6 weekly group visits. Exclusion criteria included non-English speaking, those with psychosis or severe psychiatric or medical disorders that interfered with participation. No new participants were added after the third of six visits. While participants were able to continue if they participated in less than four sessions, only those with four completed sessions were included in data analysis. Patients consented to participate in the GMV and complete the clinical assessments, verbally at the first visit as per clinical standard of care. Please see Supplementary Table S1 for further details.
Outcome measures
Participants were asked to complete questionnaires at the end of their first and last sessions, and scores were entered into the electronic medical record.
Anxiety was measured using the Generalized Anxiety Disorder-7 (GAD-7) questionnaire. The GAD-7 is a 7-item questionnaire with scale scores ranging from 0 to 21 with higher scores correlating to higher levels of anxiety. It has good internal consistency (Cronbach α = 0.92) and reliability (interclass correlation = 0.83). 25 Scores of ≥10 are consistent with GAD, and cut points of 5, 10, and 15 represent mild, moderate, and severe anxiety, respectively. 25 Depressive symptoms were measured using the 9 item Patient Health Questionnaire (PHQ-9); scores ranged from 0 to 27 with higher scores representing greater depressive symptoms. 26 Scores ≥10 have 89% sensitivity and specificity for major depression; in addition, scores of 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression.
Systolic and diastolic blood pressure, as well as heart rate, was measured at the beginning of each of the six visits.
Data were extracted from the patients' electronic health record at the end of the study.
Statistical analysis
Baseline characteristics were reported using means, standard deviations (SDs), counts, and percentages. Since participants needed to attend at least four sessions to be included in the analysis, the baseline could have been session 1, session 2, or session 3 depending on which session the participant first attended. End of study values were collected at session 6.
To evaluate changes from baseline (first session) to end of program (last session), mixed effect linear regression models were implemented using the lme4 package in R. 27 Mixed effect models allow for inclusion of patients with at least one nonmissing value for a given outcome. 28 For physiological outcomes measured at each visit, data from all visits were included in the models, but only the estimate for change from baseline to end of study was reported.
Preliminary models were fit to each outcome as a function of session number with a group-level random effect to determine whether significant group variation in study outcome changes was present and needed to be accounted for in their modeling strategies. The authors found that group-specific random effect was not needed after examining the intraclass correlation coefficient and therefore only included a subject-level random effect. Unadjusted mixed effect linear regression models were fit to each outcome as a function of session number with a subject-level random effect to account for possible within-subject correlation. Multivariable models were then fit adjusting for age, sex, and number of sessions attended. For both unadjusted and adjusted models, change in outcome from baseline to end of study, 95% confidence intervals (CIs), and p-values were reported. Assumptions of linearity, normality of errors, and normality of random effects were checked.
To determine whether change in study outcomes differed by number of sessions attended, a post hoc Kruskal–Wallis rank sum test was conducted. To determine if differences in age, sex, or number of sessions attended were present by directionality of change for significant study outcomes (decrease vs. no change/increase), the Kruskal–Wallis rank sum test and Fisher's exact test were used for continuous and categorical variables, respectively.
All analyses were conducted using R 3.5.2. 27 p-Values <0.05 were considered statistically significant.
Results
Baseline demographics
Ninety-two patients were recruited into the study corresponding to a total of 11 groups ranging in size from 3 to 13 participants. Of the 92 enrolled patients, 37 participants were excluded because they attended <4 sessions. One group was cancelled due to low enrollment (after changing time of session), and another did not have follow-up data collected at the time this analysis was conducted. Three patients were excluded due to missing demographic data. Therefore, a total of 52 participants, corresponding to 9 groups, were included in the analysis. The mean age of participants was 50 years old (SD 15.4), and the majority were women (79%; Table 2). Fifteen of the 52 (29%) participants completed the minimum four sessions, while 23 (44%) completed five, and 14 (27%) completed all six sessions.
Baseline Demographics
SD, standard deviation.
Change in study outcomes
Both GAD-7 and PHQ-9 scores significantly decreased from first to last session with reductions in GAD-7 from 10.6 to 5.5 and PHQ-9 from 8.0 to 5.2 (p < 0.001 for both; Table 3; Fig. 1).
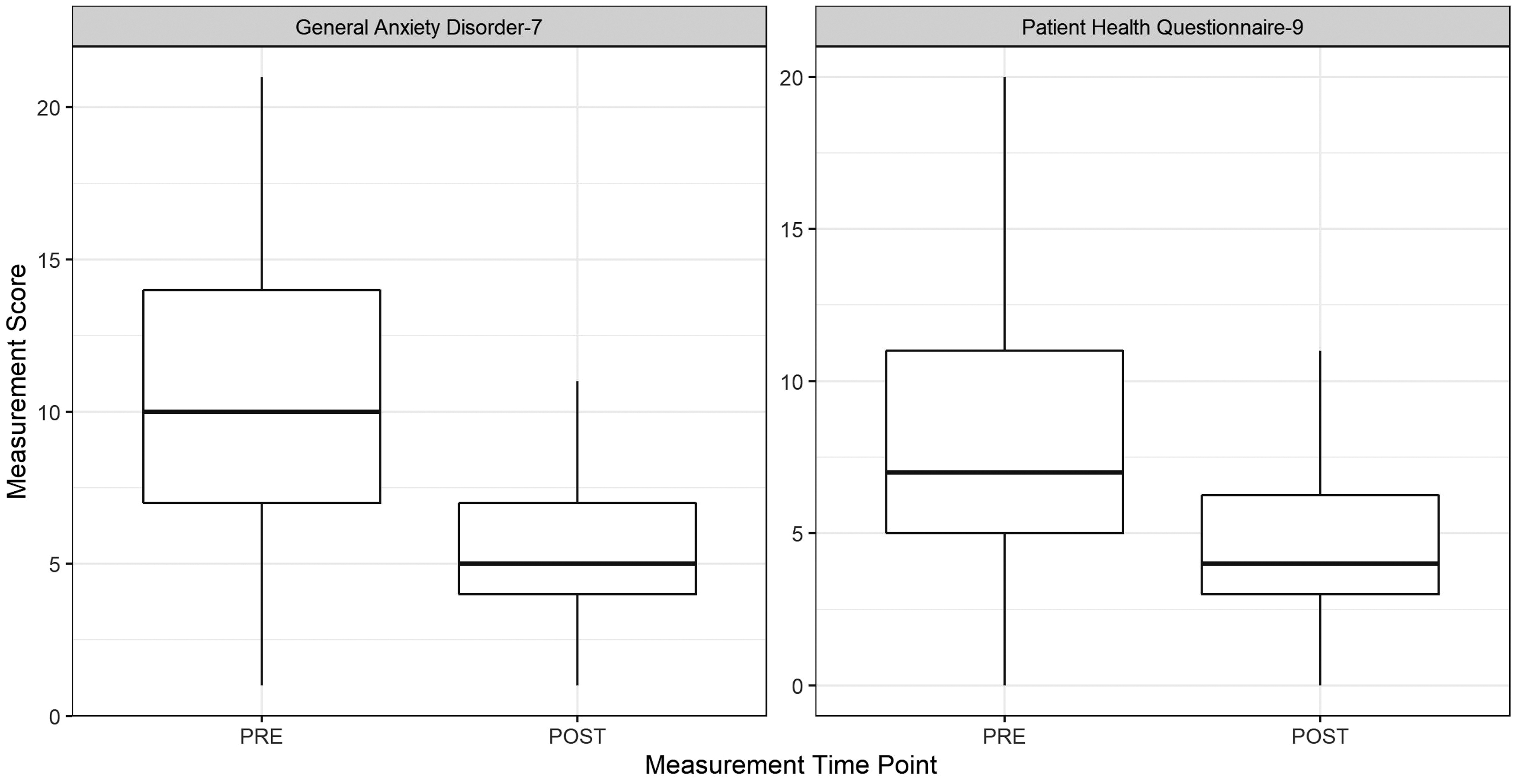
Boxplots of pre and post General Anxiety Disorder-7 and Patient Health Questionnaire-9 scores. Both scores significantly decreased (p < 0.001).
Change in Study Outcomes
First session may have taken place at visit 1, visit 2, or visit 3.
Based on a mixed effect linear regression model of outcome as a function of session with a random subject-level effect.
Based on a mixed effect linear regression model adjusted for age, gender, and number of visits attended. Model includes measurements from all attended sessions.
Only first and last session values were recorded for these outcomes.
CI, confidence interval; GAD-7, Generalized Anxiety Disorder-7; PHQ-9, 9 item Patient Health Questionnaire.
Participants reported less anxiety and depression at the end compared to the beginning of the GMV; on average, GAD-7 scores decreased by 5.1 points (adjusted 95% CI: −6.4 to −3.7) corresponding to a reduction from moderate-to-mild anxiety. The PHQ-9 decreased by 3.3 points (adjusted 95% CI: −4.3 to −2.2) between first session and last session. These reductions in anxiety and depression scores were independent of age, sex, and number of visits attended. Decreases in heart rate, systolic, and diastolic blood pressure were not statistically significant, but the direction of the change was in the hypothesized direction (Fig. 2).
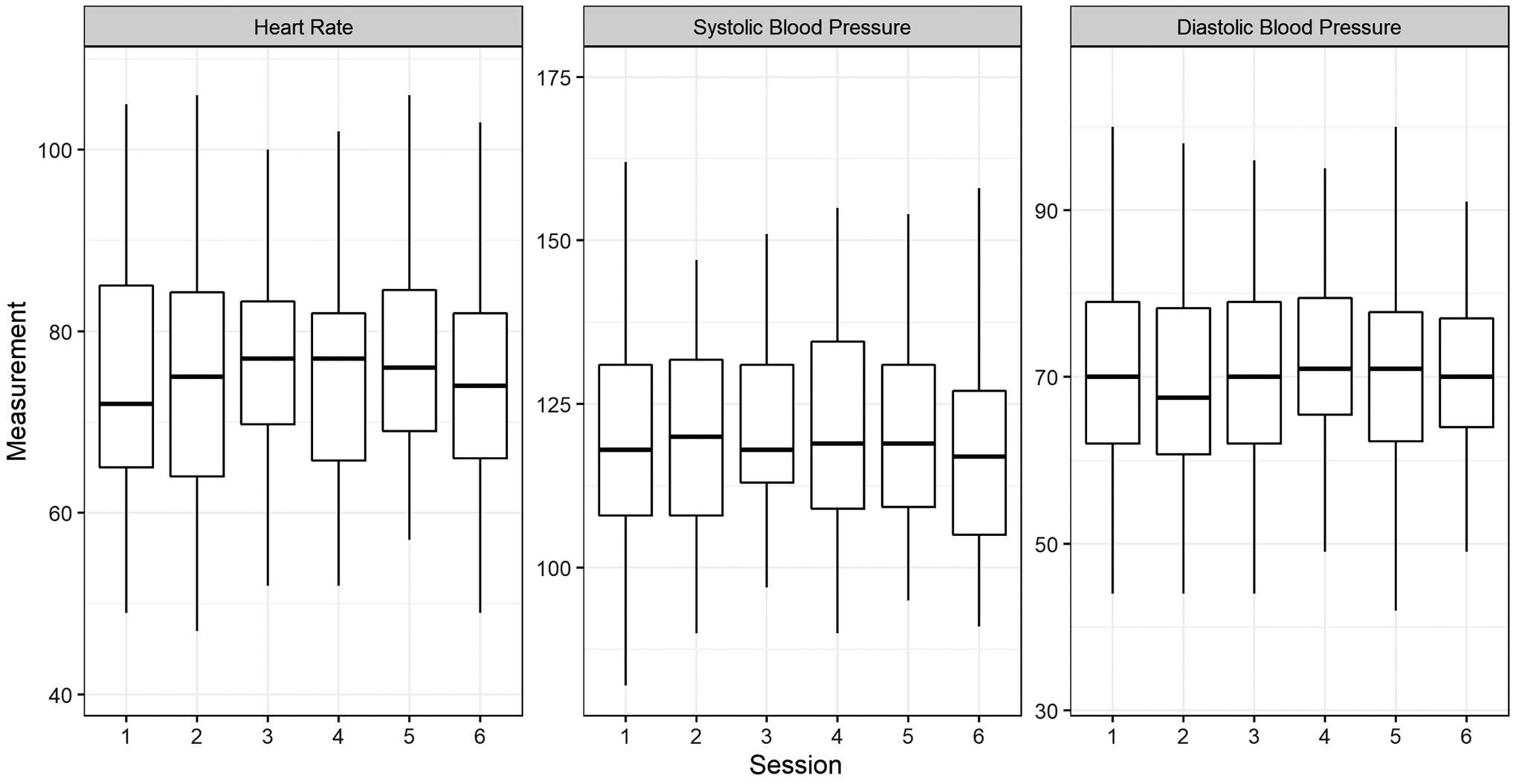
Boxplots of heart rate and systolic and diastolic blood pressure across sessions. There were no significant changes across sessions although the trend was in the hypothesized direction.
Larger changes in outcome were generally present for participants who attended more than four sessions; however, these differences were not statistically significant (Fig. 3).

Boxplots of change in study outcome by number of sessions attended. Dots correspond to individual values. Red lines indicate no change in outcome from first to last visit (session 6); a desirable change in outcome is below the red line. There were no significant differences in change in outcome by number of sessions attended for any outcome (Kruskal–Wallis rank sum test, p-values ranged from 0.14 to 0.54).
There were no differences in age, sex, or number of visits attended in the participants who had decreases in anxiety and depression compared to those that had no changes or increases in clinical score (Table 4). In addition, all participants who attended six sessions experienced a decrease in GAD-7 scores from baseline to end of study.
Characteristics by Direction of Change in Generalized Anxiety Disorder-7 and 9 Item Patient Health Questionnaire
Fisher's exact test and the Kruskal–Wallis rank sum test were used to test change in outcome across categorical and continuous variables, respectively.
Limitations
There were several limitations to the current observational study. First, the study did not randomize patients or include a control group, limitations that need to be addressed to establish effectiveness and control for confounding factors, such as initiation of medication or psychotherapy while participating in the intervention. The latter is not consistently captured in the electronic medical record, especially if it is with an external provider. The analysis was limited to those patients who participated in four or more sessions which may have introduced selection bias. The majority (79%) of the sample was female. While anxiety disorder is higher in women compared to men by 2:1, 5 it would be important to increase sample of male participants in future studies to evaluate effectiveness across genders. Participants were primary care outpatients with symptoms of stress or anxiety, but not necessarily with a psychiatric diagnosis of anxiety disorder or depression, so results may not be generalizable to a psychiatric population with diagnosed anxiety disorders.
Furthermore, there was low intergroup variance indicating a homogenous sample across groups, and thus, this intervention needs to be tested with additional patient populations. There was a high attrition rate (∼25%, data not shown) as has been cited with GMV, 22 but future studies would be necessary to identify factors that predict attrition and successful completion of the mindfulness based GMV. While the authors did advertise that mindfulness was part of the curriculum, some patients discontinued after the first or second visit because they were uncomfortable with the group format or felt greater anxiety in the groups (data not available as reported by patient message when advising of their withdrawal from the program). Thus, reported reductions in anxiety may be conservative as the more anxious patients with the greatest room for improvement may have not continued with the intervention.
Future studies would benefit from investigating patient's reasons for discontinuing the group visits and comparing their baseline GAD-7 scores to those who completed the intervention, to examine if in fact they had higher levels of anxiety.
Discussion
Primary care patients attending a 6-week standardized mindfulness based GMV had reductions in anxiety and depressive symptoms. Reductions in anxiety and depression were independent of age, sex, and number of visits attended (with a minimum number of visits being 4). Data analysis was limited to patients who had attended at least four visits as previous MBI demonstrated dose effects with stronger outcomes the more visits patients attended. 29
These results are consistent with other findings of lowered anxiety and depression scores following MBI. 8,9,29 The 5-point reduction in anxiety score was clinically significant as this is the level of change needed to move from severe-to-moderate or moderate-to-mild. The 3-point reduction in depression scores, while statistically significant, is of unclear clinical significance as a 5-point change in PHQ-9 is needed to change clinical status (i.e., from moderate-to-mild, or moderately severe-to-moderate, etc.). 26 While depression and anxiety often coexist, 30 the authors may have undersampled patients with clinically significant depression given recruitment focus on stress and anxiety. A larger sample size of both participants with anxiety and depression or specifically depression in the future will further evaluate the effect on depression.
It is difficult from this observational study to determine if the intervention components (mindfulness, education, or group support) or simply group participation was responsible for the decrease in anxiety and depression scores. Prior MBIs have demonstrated reductions in anxiety and depression scores in both the mindfulness and educational control groups compared to usual care (unlimited primary care access). 31 In addition, reductions in stress have been reported in educational weight loss 32 and group exercise programs 33 suggesting benefits from group participation in the absence of mindfulness or educational components.
Geller discusses a “Group Inclusion Effect,” a social network with a shared sense of purpose, 34 that may explain findings of both experiential and control groups. If a Group Inclusion Effect is established in a control group just by the nature of being in a social network this might explain the lack of significant findings when an educational or support group is used as controls for MBIs. It would be important in future studies to not only randomize patients to either treatment or control groups but also to include an active placebo (i.e., listening to relaxing music alone) and usual care (therapy or medication) control groups. These would then control for both a Group Inclusion Effect and the intervention. In addition, noninferiority trials (i.e., MBI compared to active therapy groups or active medication group) may help determine usefulness of these interventions.
Many MBIs using MBSR format emphasize specific facilitator training programs of several weeks with dedicated retreats. 35 There has also been a call for a more rigorous description of standardized training procedures in MBI studies. 36 The authors found no intergroup variance in outcomes using three different practitioners who, while being experienced meditators, were asked to follow a very standardized procedure for each session, including the meditation practices, and participate in a specific training protocol. The authors agree that an essential criterion for instructors in MBI is the practice of meditation themselves 36 ; however, the specific components of training instructors will need more evaluation. In addition, the lack of intergroup variability in outcomes supports the reproducibility of this intervention which emphasized training with a standardized curriculum and providers committed to their own and the participants understanding of the practice.
Finally, while formal diagnosis of either anxiety disorder or depression was not obtained, results showed that across a wide spectrum of symptoms and behavioral health status, the intervention was associated with reduction in symptoms (Fig. 1). In fact, those with lower symptom scores tended to be those few who had increase in symptoms, while the opposite is true for patients with higher symptom scores (data not shown). Future studies analyzing change by symptom groups (mild, moderate, severe) will evaluate whether specific symptom groups have greater benefits.
Conclusion
In summary, a significant reduction in both anxiety and depression scores was demonstrated after this 6-week mindfulness based GMV for primary care patients with stress and anxiety. Reductions in anxiety scores correlated to clinical reduction in symptoms from severe-to-moderate or moderate-to-mild anxiety. Intergroup variability was not significant indicating that the intervention is reproducible over time and across providers. In addition, the standardized format of the intervention and the training procedures were appropriate for reproducibility of the intervention. Finally, future randomized controlled trials with appropriate controls and follow-up surveys will better evaluate which components of the intervention account for findings and who might benefit most from this type of intervention.
Footnotes
Acknowledgments
The authors thank Dr. Catherine Forest for her early support and participation with the Beyond Stress program. The authors are also grateful for their program coordinator Karina Torres Maldonado.
Authors' Contributions
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Seed grant from Division of Primary Care and Population Health, Department of Medicine, Stanford University.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.