
Abstract
Introduction:
Preoperative anxiety before cesarean section is a major issue. Nonpharmacologic anxiety control is believed to be more suitable in pregnant women. Auricular acupuncture (AA) is an inexpensive, easy-to-use, and validated intervention to reduce anxiety in different surgical settings. We evaluated the effect of AA on preoperative cesarean section anxiety.
Methods:
In a prospective, blind, controlled trial, pregnant women with a scheduled cesarean section under spinal anesthesia were randomized to receive AA with needle, AA without needle (sham), or usual care (no intervention). Anxiety level was assessed by using a visual analogue scale for anxiety (VAS-A; 0-minimal anxiety, 100-maximal anxiety) at three time points: inclusion (pre-induction room–T0), when entering the operating room (T1), and before incision (T2). The primary outcome was the VAS-A variation (percentage changes) between T0 and T1 in the AAe group compared with that in the sham AA group. The secondary outcomes were the VAS-A variation between T0 and T1 in the AA group compared with that in the control group, and the variation between T0 and T2 compared between the three groups, the effect of AA on parasympathetic tone, and the incidence of adverse effects.
Results:
In women immediately before anesthesia for cesarean section, the AA produced a 19% decrease of anxiety, compared with a 21% anxiety increase in sham AA, which is significantly different. The effect of AA was more present in women with low initial anxiety. The proportion of patients reaching clinically significant anxiety reduction (>33% from the initial level) was 2.5 times higher in the AA group (p = 0.02) compared with the sham group. No differences in anxiety variations were found compared with the no-intervention group. No effect of AA was noted on parasympathetic tone.
Conclusion:
Compared with sham, AA decreased maternal anxiety level when arriving in the operation room and just before the beginning of the cesarean section, with a trend toward improvement compared with usual care.
Introduction
Cesarean section (C-section) is the most common surgical procedure in pregnant women, with about 18.5 million being performed worldwide yearly. 1 Preoperative anxiety before C-section is prevalent and may be severe; the mean visual analogue scale for anxiety (VAS-A) value among such patients has been reported to be 53/100 mm. 2 As such, it may have deleterious consequences on the perioperative period.
For instance, stress-induced catecholamines release may increase the hypotensive effect of sympathetic blockade after spinal anesthesia. 3 The anxiety level before C-section is inversely proportional to satisfaction and the success of postoperative rehabilitation (mobility, attention to the newborn, pain and activity, fatigue). 4 The options for reducing anxiety before C-section are limited. Preoperative antenatal education is not sufficient to reduce preoperative anxiety. 5 Pharmacological therapy, which is widely used for common anxiety disorders treatment, does not systematically improve patients' experience, may be associated with adverse effects, and is willingly restrained in pregnant women due to transplacental passage. 6,7
Hypnosis may be a valuable adjunct for the treatment of anxious and apprehensive patients 8 ; however, time constraints may limit the use of this therapy. Auricular acupuncture (AA) is an inexpensive, rapid, and easy-to-perform technique with a few significant side effects 9 and is, therefore, applied in pregnant women. 10 This method was systematized by Paul Nogier (Lyon, France) in 1950, 11 and it has already been used to treat anxiety in various situations such as outpatient surgery, dental surgery, or for parental anxiety treatment before their child's surgery. 12 –15
The potential mechanisms' anxiolytic effect of auricular stimulation are explained via the involvement of cranial nerves, leading to the modulation of the brain areas involved in the stress response. This includes the limbic system, locus coeruleus, and hypothalamus. 16,17 Interestingly, only a few studies have investigated the methods to reduce anxiety in parturient women before C-section, and these concerned acupressure and not AA. 18 We, therefore, conducted a study to determine the effect of AA before scheduled C-section on preoperative anxiety in pregnant women.
Methods
Design and settings
This single-center parallel-groups randomized blind (participant, investigator), controlled trial was conducted at the Croix-Rousse hospital, Hospices Civils de Lyon, a tertiary academic center. The ethics approval was granted by the regional committee (Comité de protection des personnes Sud-Est II, France, N° 2015-45-2). Written informed consent was obtained from all participants before inclusion. The trial was registered with
Participants were randomized to receive one of the following interventions: (1) AA, (2) needleless sham on auricular acupuncture (SAA) points, or (3) no-intervention control (NIC).
The approval N2015-45-2 was granted by the regional ethical committee, written informed consent was obtained from all participants.
Participants
Pregnant women aged 18 years or older, the American Society of Anesthesiologists (ASA) classification 1–2, with no prior experience with AA, scheduled for C-section under spinal anesthesia were eligible. The investigators verified that patients were able to understand and follow the study protocol. The exclusion criteria were as follows: refusal to consent, mood disorders, generalized anxiety and psychiatric disorders, long-term antidepressant/anxiolytic treatment, C-section for placenta accreta, pacemaker, and ear piercings (except a regular earring). Patients were recruited during the preoperative appointment with the anesthesiologist (eighth month of pregnancy), where the study protocol was explained.
Group assignments
On the day of the planned C-section procedure, the recruited patients were approached. After a patient had agreed to participate and signed written informed consent, the initial measurement of anxiety level using a VAS (VAS-A) was recorded. Patients were stratified into two subgroups according to the self-evaluation of the VAS-A; a 40/100 threshold was chosen to delimit no anxiety (VAS-A < 40/100) and anxiety (VAS-A ≥ 40/100). 19 Such stratification was conceived to have homogenous arms, as patients with higher baseline anxiety may have more response to the anxiolytic interventions. Then, patients were randomly assigned to receive, in each subgroup and before the surgery, either AA, SAA, or NIC, by using a centralized computer-generated sequence.
Interventions
In patients, randomized in AA and SAA groups, three anxiolytic auricular points of the right ear were identified by a single certified acupuncture specialist, using an Agiscop DT® differential detector (Irigny, France). This device is used for the detection of skin zones with lower electrical resistance. 20 The chosen auricular points included MA-TF1 (apex of the triangular fossa), MA-LO1 (central side of the ear lobe), and MA-TG2-TG4 (along the whole length of the vertically ascending tragus) 11,21 (Supplementary Appendix Fig. S1).
AA group
In the AA group, for all patients ear acupuncture was performed by using three New Pyonex needles. A New Pyonex represents an adhesive plaster with a needle with length 0.9 mm, diameter 0.2 mm (Seirin Corp.®, Shizuoka City, Japan). These needles were applied on MA-TF-1, MA-LO1, and MA-TG2-TG4 of the right ear; maintained through the C-section procedure; and removed on admission to the post-anesthesia care unit (PACU).
Sham AA group
In the SAA group, patients received an adhesive plaster without needle, similar in appearance to the New Pyonex, applied to the same auricular points as in the AA group, maintained through the C-section procedure, and removed on admission to the PACU. Although applied to the same AA points as for AA, this placebo intervention cannot be considered as acupressure, since no pressure was maintained after the application of adhesive plaster.
In both groups, AA and SAA were implemented immediately after randomization (Supplementary Appendix Fig. S2A, B).
NIC group
Women in this group received no AA treatment. We included the NIC group to assess the potential placebo effect in the SAA group. 22 Patients from this group were not blinded to the intervention.
Measures
Baseline characteristics
Baseline characteristics (age, weight, height, gestational age, gravidity, and parity) were systematically recorded.
Anxiety measurement
Three time points were defined to assess the effect of intervention—before randomization (T0), before the departure to the operating theater (T1), and before incision (T2). The time in minutes between each time point was recorded. Anxiety level was assessed by using self-reported measures. A VAS-A 19 with a single score ranging from 0 (no anxiety) to 100 (maximal anxiety) was used at time points T0, T1, and T2. For the secondary analysis, we used Amsterdam Preoperative Anxiety and Information Scale (APAIS) at time points T0 and T1. 23
Perioperatively, hemodynamic parameters (standard anesthesia monitoring) and the level of parasympathetic tone were recorded with the analgesia-nociception index (ANI) monitor. 24 The ANI provides a dimensionless value ranging from 0 to 100. Higher scores reflect increasing parasympathetic tone and decreasing nociceptive or sympathetic levels. Postoperative pain was assessed starting from the patient's admission to the PACU (time point T3).
Any adverse events potentially related to the AA technique were recorded. 25
Study protocol
On the day of the scheduled C-section, patients were admitted to the pre-anesthesia room ∼1 h before the surgery. Patients assessed their anxiety by using VAS-A and APAIS, and the anesthesiologist recorded the level of anxiety, hemodynamic parameters, and ANI level (time point T0). After stratification into anxious (VAS-A ≥ 40) and non-anxious (VAS-A < 40) patients, a randomization procedure was initiated. In patients assigned to AA or SAA arms, the AA points were detected, and AA or SAA was applied accordingly by an independent specialist. This procedure was masked from clinicians, managing patients during the surgery.
For all patients in three arms, an opaque disposable surgical cap covering both ears was placed to mask the arm from the assessor (Supplementary Appendix Fig. S2C).
Immediately before the admission to the operating theater, a second measurement of anxiety was performed (Time point T1) by using VAS-A and APAIS; again, hemodynamic parameters and ANI level were recorded.
In the operating theater, a standard spinal anesthesia was given (11 mg of hyperbaric bupivacaine +3 mkg of sufentanil and 100 mkg of morphine, L4L5 puncture level, 27G Pajunk needle) and patients were installed on the surgical table. Immediately before the incision, the anxiety level was evaluated with the VAS-A and APAIS scale (Time point T2); hemodynamic parameters and ANI level were recorded.
At all three time points, the same clinician, masked from the randomization arm and intervention, performed anxiety evaluations. No patient received any anxiolytic drugs before or during surgery.
Outcomes
The primary outcome was the T0–T1 VAS-A difference in the AA group compared with that in the SAA group (percentage change).
The secondary outcomes included the T0–T1 VAS-A difference in the AA group compared with that in the NIC group, the T0–T2 difference in anxiety between all three groups, the proportion of patients that reached a minimal clinically relevant decrease in anxiety (>33%) at T1 and T2; the effect of AA on parasympathetic tone; the effect of AA on postoperative pain at time point T3; the measurement of correlation between anxiety assessment tools (VAS-A and APAIS); the measurement of correlation between VAS-A and parasympathetic tone changes; and the incidence of adverse events and side effects from intervention.
Sample size
The sample size was estimated from the results of a preliminary study carried out in the obstetrics department of our hospital from February to April 2014. This study found in 10 patients who received AA a mean of 21-point decrease in anxiety measured with VAS-A (standard deviation = 27), representing a 33% reduction. In current practice, a decrease of 20 points or 33% on the standardized 100 points scale is considered as a minimal clinically relevant difference for self-reported acute conditions measurement (e.g., pain). 26
We, thus, hypothesized that the AA treatment, applied in women scheduled for C-section, would result in a 20-point reduction (∼30%) in VAS-A, measured before the entrance in the operating theater, and compared with the SAA. A sample size of 30 in each group had 80% power to detect a difference in means of 20 points (30%) (20 points vs. 0 in AA and SAA groups, respectively), assuming that the common standard deviation is 27 and using a two-group t-test with a 0.050 two-sided significance level. This sample size was calculated by using nQuery Advisor®, 7.0 (Statistical Solutions Ltd, Cork, Ireland).
Randomization
Randomization was carried out by using Ennov Clinical® software (Paris, France), which incorporates an IWRS (Interactive Web Response System) randomization system. The configuration of the randomization and the implementation of the list in the software was carried out by the statistician who was not involved in the process of patient inclusion and randomization. The list was created with variable block size by using nQuery Advisor, 7.0 (Statistical Solutions Ltd). Nobody except the statistician had access to the randomization list.
On inclusion, the investigator randomized directly into the patient's eCRF via the CSOnline site (Ennov Clinical, Paris, France). The result of the randomization was displayed directly in the eCRF randomization page. Auricular Acupuncture or Sham AA was applied accordingly by an independent specialist, and this procedure was then masked from clinicians managing patients during surgery.
Statistical analysis
Categorical data are described as numbers and percentages; continuous data are expressed as means and standard deviation for normally distributed variables or medians and interquartile ranges (IQRs) for non-normally distributed variables. Comparisons between groups were made by using Pearson's Chi-2 test for categorical variables (or Fisher's exact test, as appropriate), and by using non-parametric Wilcoxon signed-rank or Kruskal–Wallis (one-way analysis of variance [ANOVA] on ranks for multiple comparisons) test for continuous variables.
A post hoc test using nonparametric comparisons for all pairs with Steel-Dwass (protects the overall errors rate, a non-parametric extension of Tukey's HSD test) method was implemented for multiple-group repeated measurements.
The percentage change in anxiety for each patient between different time points was calculated as follows:
A regression analysis was performed to assess the effect of intervention on the proportion of patients reaching a clinically significant decrease in anxiety. The results are expressed as odd ratios and 95% confidence intervals (CIs).
An intention-to-treat analysis was used. A threshold of p < 0.05 was considered statistically significant. All analyses were performed by using IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp. Armonk, NY) and R (R Foundation for Statistical Computing, Vienna, Austria).
Results
Ninety-one patients were enrolled in the study from March 2016 to February 2018; one patient was not included because of C-section cancellation on the admission day. After the inclusion and stratification, a total of 90 patients were allocated into three groups (Fig. 1). In all patients from the AA and SAA arms, three AA points were used (MA-TF1, MA-LO1, MA-TG2-TG4). There were no missing data.

Trial flowchart. AA, auricular acupuncture; C-section, Cesarean section; NIC, no-intervention control; SAA, Sham auricular acupuncture group; T0, inclusion (pre-induction room); T1, departure to operating room; T2, incision; VAS-A, visual analogue scale for anxiety.
Patients' baseline characteristics were similar; the delay between time points T0, T1, and T2 was comparable (Table 1).
Patients' Baseline Characteristics and Time Between Three Measurements in Study Groups
Values are expressed as means ± SD or medians [IQR].
AA, auricular acupuncture group; IQR, interquartile range; NIC, no-intervention control group; SAA, Sham auricular acupuncture group; SD, standard deviation; T0, time-point 0; VAS-A, visual analogue scale for anxiety.
Primary outcome
A median 19% [IQR −53 to 23] decrease in anxiety was found in the AA arm, which was significantly different compared with the SAA arm (21% [IQR −11 to 66] increase, p = 0.01) (Table 2). The proportion of patients with clinically relevant anxiety decrease (≥33%) was more important in the AA group (43%, 13 patients), compared with the SAA group (13%, 4 patients, p = 0.02).
Effect of Auricular Acupuncture on Anxiety, Compared with Sham, Before Entering the Operating Room (Primary Outcome)
A negative value indicates a decrease. A Wilcoxon signed-rank and Fisher Exact test were used.
AA, auricular acupuncture; SAA, Sham on auricular acupuncture; T0 and T1, measurement time points; T1–T0, difference in measurements for time points accordingly.
Secondary outcomes
Compared with the no-intervention arm, we found no significant differences either in percentage changes or in the proportion of patients reaching a clinically relevant anxiety decrease threshold at T1.
At the time point T2, there was a 5.8% [IQR −46 to 19] decrease in anxiety compared with the initial level in the AA arm, which was significantly different from the SAA arm (34.6% [IQR −19 to 100] increase, p = 0.02), and non-different to the NIC arm. No significant difference in the proportion of patients reaching a clinically relevant anxiety decrease threshold was found between all three arms at this time point (Table 3, Fig. 2).
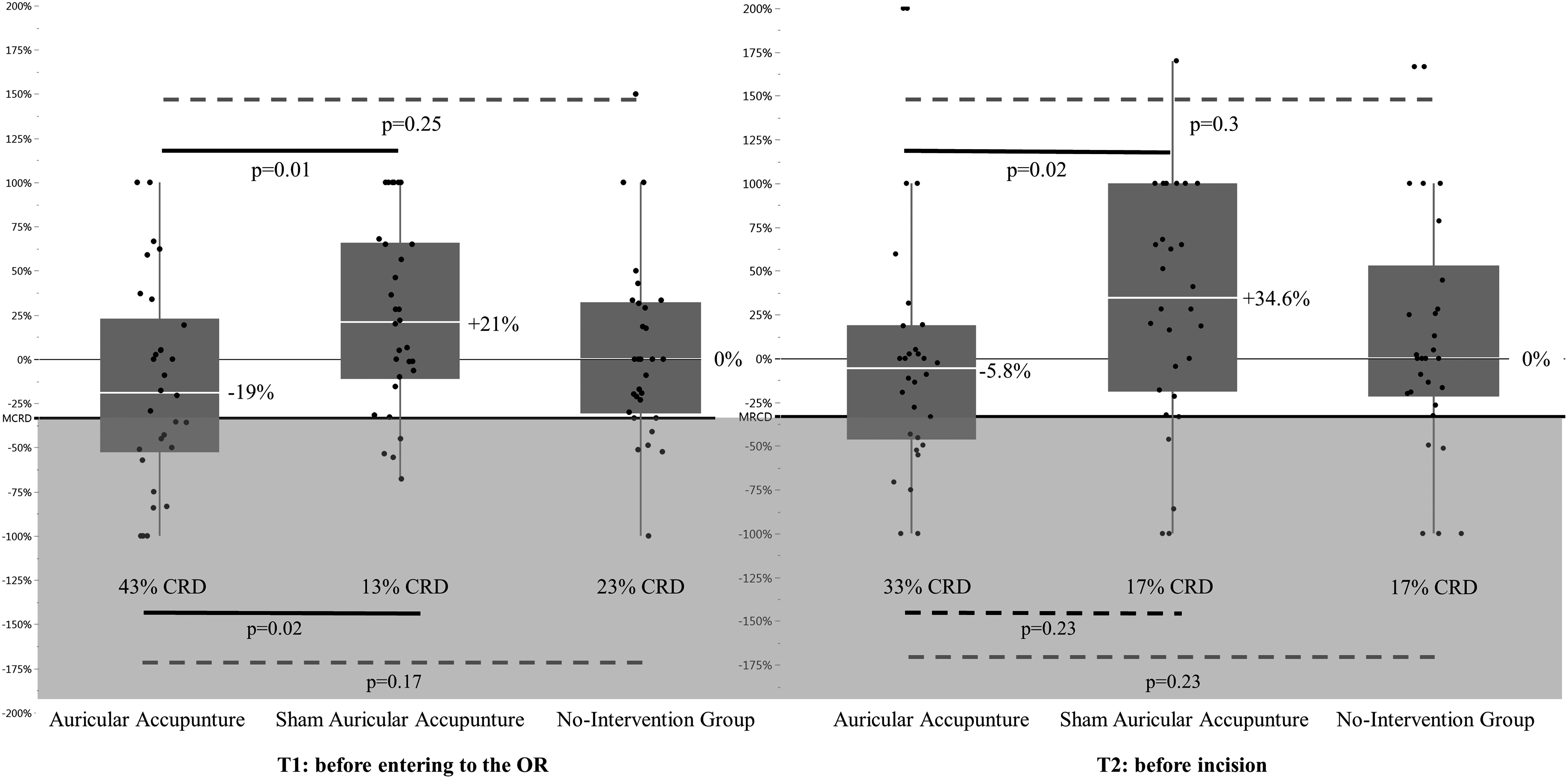
Effect of the intervention on percentage change in anxiety level at T1 (primary outcome) and T2. Plain lines indicate a significant difference. AA, auricular acupuncture; MCRD, minimal clinically relevant decrease threshold, delimited in light gray; n% CRD, proportion of patients reaching clinically relevant decrease in anxiety; NIC, no-intervention control; SAA, Sham auricular acupuncture; T1 and T2, timepoints; Y axis, percentage change in anxiety level at the time point compared with T0.
Secondary Outcomes
A negative value indicates a decrease. A Wilcoxon signed-rank and Fisher Exact test were used for tables A and B; Steel-Dwass method was used for table C (mean difference [z-score] with significance [p-value] shown).
AA, auricular acupuncture; NIC, no-intervention control; SAA, Sham auricular acupuncture; T0, T1, and T2, measurement time points.
The intervention effect on clinically relevant anxiety reduction (≥33% from the initial level) was significantly higher with AA compared with SAA (odds ratio [OR] 3.45 [95% CI 1.19–9.96]) at T1, and non-significant at T2 (OR 2.5 [95% CI 0.74–8.5]). No significant effect was found on comparing AA and NIC either at T1 (OR 2.5 [95% CI 0.8–7.64]) or at T2 (OR 2.5 [95% CI 0.74–8.5]).
Adjusted for the threshold of anxiety at the time of inclusion (VAS-A ≥ 40 at T0), the intervention effect was significant with AA compared with SAA at T1 (OR 5.21 [95% CI 1.43–18.98]), and non-significant at T2. Compared with NIC, the effect of intervention did not reach statistical significance, although a positive trend was observed (OR 2.62 [95% CI 0.85–8.06], p = 0.09) at T1.
The parturient woman's anxious state did not significantly influence the intervention effect at T1 or T2 (Supplementary Appendix Table S1A, B).
The Number Needed to Treat for the AA compared with the sham was 4 (95% CI 1.9–11.8). On comparing AA with NIC, the absolute risk reduction from the intervention is 20% (95% CI −3.31% to 43.31%).
In subgroup analysis, in patients with an initially low anxiety level (VAS-A < 40 at inclusion), a median 15% [IQR −81 to 46] decrease in the AA group and 56% [IQR 28–100] increase in the SAA group were detected for anxiety, and this was statistically significant. Differences for anxiety changes in patients with initially higher anxiety were nonsignificant. The proportion of women reaching a clinically relevant anxiety decrease threshold was significantly higher in the AA group (n = 7, 43.8%) compared with SAA and NIC.
However, for the initial higher anxiety (VAS-A > = 40) subgroup, no significant difference in the proportion of women reaching a clinically relevant anxiety decrease was found, although six patients had a relevant anxiety relief in the AA group (Supplementary Appendix Table S2).
Anxiety reduction, measured with APAIS, was significant in the AA group, compared with both SAA (z-score 2.48, p = 0.0349) and NIC (z-score 3.62, p = 0.0009) (Supplementary Appendix Table S3A, B).
There were no differences detected regarding the effect of AA on parasympathetic tone changes measured with ANI at T0 and T1 (Supplementary Appendix Table S4). No effect on early postoperative pain was captured (Supplementary Appendix Table S5).
We found no significant correlation between ANI and VAS-anxiety at T0 and T1 periods in all groups. Anxiety level, measured with APAIS, had excellent correlation with VAS-A in all groups across T0 and T1 time frames (Supplementary Appendix Tables S6 and S7).
Regarding side effects and adverse events, in all groups there were four cases of maternal hypotension, eight cases of bradycardia, seven cases of nausea/vomiting, seven cases of dizziness, and six cases of drowsiness, which were non-different between groups. There were no AA-specific adverse effects (ear pain, bleeding or bruising at the needling site, skin irritation, allergy, hematoma, or local infection), except one case of skin irritation under the patch in a patient with SAA (Supplementary Appendix Tables S8 and S9).
Discussion
In our randomized controlled and blinded study, we found that AA applied in women scheduled for elective C-section 1 h before the admission to the operating theater results in a significant reduction in anxiety compared with the sham intervention. The proportion of patients reaching a clinically significant anxiety reduction was 2.5 times higher in the AA group compared with the sham; however, no significant differences in anxiety variations were found when compared with the no-intervention group.
Interestingly, in subgroup analysis, although underpowered, this effect was significant in those with an initially low anxiety level (above 40). It was consistently demonstrated that patients with a high acute anxiety level need additional coping strategies (e.g., conversation with staff or distraction), in addition to already implemented anxiolytic intervention. 27 Although the clinical benefit of dividing patients into those with high and low anxiety was found to be questionable, 28 a quick testing with VAS-A scale may help to predict whether another supplementary anxiety coping strategy may be employed to enhance woman's experience through the c-section procedure.
About one in every four patients will benefit from the AA treatment compared with sham. Although non-statistically significant, the AA treatment may still be interpreted as helpful compared with no treatment, as the number needed to obtain a negative result (no clinically relevant decrease) is high—at least 30 patients. 29
Our study demonstrated significant dichotomous changes in anxiety level at time points T1 and T2 between the AA and SAA groups, pointing out the beneficial effect of acupuncture. Women with sham plaster were expecting anxiolysis from the treatment, however there was no perceived relief. This may explain the increase in anxiety, which is not observed in the NIC group. This phenomenon persisted during the T2 time point.
There was a small placebo effect in the SAA group—seven patients had a significant decrease in anxiety level. These findings are in contrast with the already published sham effects from acupuncture studies, 30,31 especially when the target of acupuncture intervention is pain. 32 It has been shown that acupuncture point stimulation altered some of the sex hormone levels during pregnancy in both animal models and humans.
Even sham interventions, associated with gentle stimulations, may alter the activity of oxytocin-sensible neurons, producing various effects, involved in the nociception process, yet not exhaustively studied. 33,34 In our study, in both AA and SAA groups, the same auricular points were stimulated during electrical detection, but the duration was about 1 min. In the SAA arm, plaster, applied on AA points, produced negligible pressure; however, a tactile stimulation persisted through the experiment.
We observed no significant anxiety changes in the NIC group, because these patients had no intervention and they were not expecting any treatment effect for the anxiety.
Acute preoperative anxiety before C-section is prevalent (>70%). 4,35 Pharmacological management of parturient women's anxiety is challenging, because of both caregivers' and patients' reluctance to use medication with trans-placental passage and potential fetal exposure. Although there is no evidence of the association of pharmacological anxiolysis and adverse neonatal outcomes, 36 –39 no improvement in patients' experience was observed while using systematic preoperative anxiolysis in general surgery. 6
Therefore, the interest of nonpharmacological treatment of acute preoperative anxiety in parturient women is important. The beneficial effect of AA was already reported in ambulatory gynecological procedures and in abdominal surgery. 40,41 Regarding specifically C-section, the reduction in acute anxiety scores was demonstrated after acupressure intervention 18,42 ; however the effect was small, and it did not reach a clinically significant difference. To the best of our knowledge, our study is the first in not only reporting median anxiety changes in response to the AA, but also describing the proportion of patients reaching clinically significant relief in anxiety.
We were not able to demonstrate the effect from AA on the parasympathetic tone, measured in our study with ANI. However, ANI was validated for the detection of such changes following classical noxious stimuli under general anesthesia, and it has been never reported as an instrument for objective anxiety-induced changes in parasympathetic tone. Moreover, spinal anesthesia produces considerable changes in sympathetic/parasympathetic balance, probably precluding the precise measurement of parasympathetic tone changes in response to anxiety.
There were no hemodynamic events or other side effects that may be associated with AA intervention, and in all patients the C-section procedure was safe and uneventful. An intrathecal morphine used for spinal anesthesia provides effective postoperative analgesia for more than 24 h after the procedure, but it may also induce nausea and vomiting. This is one of the reasons why no association between AA and pain control in the early post c-section period might be revealed, and the same applies for nausea and vomiting. No AA-specific complications were noted.
The AA is a less costly intervention (0.01€ per patch vs. 0.02€ per a single 0.5 mg alprazolam pill at our institution), non-cumbersome for patients, requiring minimal training, and it is easily applied preoperatively. The effect of AA was sustainable for more than 1 h after the patch placement, which is consistent with the acupuncture principle. The effect of acupressure, studied in the context of acute anxiety, is limited, and it is not sustained 30 min after the release of pressure from the stimulated points. 43
Our study has some limitations. There was no masking in the NIC group, either for patients or for clinicians. An attention bias may be, therefore, present in this group, leading to the mitigation of anxiety. Another possible limitation is that the acupuncture points identification and adhesive sham may probably induce an acupressure effect. However, there was no pressure maintained, and the T1 measurement was remote. Moreover, the importance of point localization and skin penetration in randomized studies assessing the effect of acupuncture was already outlined. 44
We used the VAS scale for the anxiety measurement. Most studies use the Spielberger State Trait Inventory (STAI) to assess the effect of intervention. 45 This 40-item questionnaire is recommended for anxiety measurement, but it is not easy to use in the immediate preoperative period because it takes too much time to be completed. The VAS is validated and correlated to STAI to assess anxiety, 46 and therefore this choice of tool did not affect the internal validity of the study results. Moreover, we found an excellent correlation between VAS-A and APAIS. The latter scale is widely used for selective premedication in general surgery.
We did not analyze either the previous experience of C-section, or indications for the surgery, reported to influence preoperative anxiety 47 ; however, the groups were comparable in terms of previous birthgiving experience.
Patients' anxiety measurements were performed only before the incision, and no further follow-up was continued after the surgery. The level of anxiety was shown to decrease from the preoperative moment to the end of the C-section. 2 . However, the moment of anesthesia procedure for the C-section is a no-return point, seen in psychology as an “irrevocable commitment to action, which was preceded by a period of gradually increasing commitment, […] a fundamental limit on the ability to control thought and action.” 48 For this reason, our primary end-point was measured just before the anesthesia procedure.
Preoperative, especially chronic, anxiety is well known as a risk factor of perioperative adverse effects, but also remote effects such as persistent pain after surgery, or postpartum depression. We did not specifically design our study to measure the postoperative pain after spinal block release, and we did not capture persistent postoperative pain (<3 months postoperatively) and postpartum depression. However, no acute side effects (hemodynamics, early postoperative pain) were noted. The effect on the newborn Apgar score was not studied.
Conclusions
In conclusion, compared with the sham, a 3-points AA significantly reduces preoperative anxiety in pregnant women before C-section, with a trend toward improvement compared with usual care. Less costly, less invasive, and safe in terms of adverse effects, it can be used in routine practice from the moment of the patient's admission. Given a small effect but potentially no harm from the technique, further studies with a cluster-randomized step-wedged design may be conducted and should consider the other than anxiety patient-reported outcomes.
Footnotes
Acknowledgment
The authors thank all the medical and paramedical staff of the Obstetrical Unit (maternité) of the Hôpital de la Croix Rousse for their help and contribution.
Authors' Contributions
V.L., C.H., P.B., and F.A. designed the study; V.L. performed the experiments; P.P., M.D., and M.R. analyzed the data; and J.F.F. and M.D. drafted the article. All the authors have approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by Hospices Civils de Lyon.
Supplementary Material
Supplementary Appendix Figure S1
Supplementary Appendix Figure S2
Supplementary Appendix Table S2
Supplementary Appendix Table S3
Supplementary Appendix Table S4
Supplementary Appendix Table S5
Supplementary Appendix Table S6
Supplementary Appendix Table S7
Supplementary Appendix Table S8
Supplementary Appendix Table S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.