
Abstract
Introduction:
Oligonol, an oligomerized-polyphenol from Litchi chinensis extract, has been shown to alleviate metabolic syndrome. The aim of this study was to evaluate the effects of oligonol in patients with nonalcoholic fatty liver disease (NAFLD).
Methods:
Adult patients with NAFLD defined by magnetic resonance imaging-derived proton density fat fraction (MRI-PDFF) ≥11% were enrolled and then randomly assigned to receive either oligonol or placebo capsules. Primary endpoint was ≥30% reduction in MRI-PDFF at 24 weeks. Secondary outcomes were reductions in bodyweight, waist circumference, alanine transaminase, fasting blood sugar, and lipid profiles at week 24.
Results:
Forty patients were enrolled (n = 20/group). Primary endpoint was achieved in 20% in the oligonol group and 15% in the placebo group (p = 0.50). The authors found a reduction in MRI-PDFF between weeks 0 and 24 in the oligonol group; however, the change was not different from the placebo group. Secondary outcomes were similar between two groups.
Discussion:
Oligonol has not shown a significant therapeutic effect in NAFLD. Future studies with a longer duration of therapy might be needed to achieve the primary endpoint.
Clinical Trial Registration Number:
Thai Clinical Trial Registry identification number: TCTR20200814001.
Introduction
Due to the obesity epidemic, nonalcoholic fatty liver disease (NAFLD) has become the most common liver disease worldwide with an estimated prevalence of 24%. 1 A subset of patients with NAFLD developed nonalcoholic steatohepatitis (NASH), which could lead to fibrosis progression and cirrhosis. 2,3 Currently, there are no Food and Drug Administration-approved medications for the treatment of NASH. Alternative medicines that are safe, effective, and inexpensive are the attractive options for the management of a lifelong disease such as NASH.
Oligonol (Amino Up Co., Ltd., Sapporo, Japan), a standardized oligomerized-polyphenol from Litchi chinensis extract, has been shown in both preclinical and clinical studies to have insulin-sensitizing, lipid-lowering, anti-inflammatory, and weight-loss effects. 4 –6 Previous in vitro and in vivo studies demonstrated that oligonol may alleviate hepatic steatosis. 4,7,8 To date, there is no human study evaluating the therapeutic potential of oligonol in NAFLD patients. Therefore, the aim of this study was to evaluate the antisteatotic effects of oligonol in patients with NAFLD.
Liver biopsy, a gold standard for the diagnosis of NASH, is invasive and subject to sampling errors. With this drawback, several attempts have been made to find serum markers that could aid in the diagnosis and/or prognostication of NAFLD by targeting at one of the pathogenic steps (i.e., fat accumulation, oxidative stress, inflammatory responses, and hepatocyte apoptosis). In this study, potential serum markers were used to monitor changes in oxidative stress (malondialdehyde [MDA]), 9 apoptosis (cytokeratin-18 [CK-18] fragment), 10 and adipokine (leptin) after oligonol treatment.
In this study, the reduction in liver steatosis measured by magnetic resonance imaging-derived proton density fat fraction (MRI-PDFF) was used as a primary endpoint instead of liver histology. MRI-PDFF is a noninvasive tool to assess liver steatosis and has gained its popularity in assessing treatment response in the setting of early-phase clinical trials in NASH in the recent years. 11 Patel et al. performed a comparative analysis of histologic responders, defined as a ≥2-point reduction in the NAFLD Activity Score (NAS) without worsening fibrosis, versus nonresponders, and the corresponding quantitative change in liver fat content measured by MRI-PDFF. The results showed that a relative reduction of 29.3% in liver fat on MRI-PDFF is associated with a histologic response in NASH. 12 As a result of this finding, a cutoff of 30% reduction in liver fat on MRI-PDFF has previously been used in several NASH clinical trials and this particular criterion was used in this study as well.
Materials and Methods
A randomized double-blinded placebo-controlled trial was conducted at the King Chulalongkorn Memorial Hospital, Thailand, from July 1, 2019 to June 30, 2020. The study protocol was approved by the Institutional Review Board (IRB No. 242/62) and conformed to the principles of the Declaration of Helsinki. Informed consent was signed by all participants. Adults aging 18 years and older with the history of NAFLD were enrolled in the study. NAFLD was defined by elevated alanine transaminase (ALT; ≥19 U/L in women and ≥30 U/L in men 13 ) with the presence of hepatic steatosis grade ≥2 (defined as liver fat content ≥11% by MRI-PDFF 14 ). Exclusion criteria are described in Supplementary Data S1.
Participants were randomly assigned to receive either oligonol or placebo by a stratified randomization method based on their age, gender, and body mass index (BMI). Participants, who were assigned to the oligonol group, received 100 mg of oligonol capsules twice a day, whereas the placebo group received identical-appearing placebo capsules twice a day. Both investigators and participants were blinded to the experimental group. The duration of treatment was 24 weeks. Basic demographics and clinical data were gathered using a predefined questionnaire.
Participants were scheduled for interval visits at the beginning of the study (week 0), week 4, week 12, and at the end of the study (week 24). Blood tests and MRI-PDFF were done at weeks 0 and 24. Potential adverse effects were recorded at every visit. Primary outcome was a 30% reduction in MRI-PDFF at 24 weeks. Secondary outcomes were reductions in bodyweight, waist circumference, ALT, fasting blood sugar, homeostatic model assessment for insulin resistance (HOMA-IR), lipid profiles, serum CK-18 fragment, and MDA at 24 weeks. Additional information regarding methods and statistical analysis are described in Supplementary Data S1.
Results
Patient characteristics
A total of 40 patients were enrolled (n = 20 in each group). Mean age of participants were 50.6 ± 12.0 years with 60% male. Fifty percent of participants were overweight (BMI 23.0–27.5 kg/m2) and 50% were obese (BMI ≥27.5 kg/m2). 15 Mean percentage of hepatic fat content measured by MRI-PDFF was 21.8% ± 5.8% at baseline. Ninety percent of participants had insulin resistance by using HOMA-IR threshold of 1.56 for men and 1.64 for women 16 with median HOMA-IR of 2.44. Baseline characteristics were not different between two groups.
Primary and secondary outcomes
Primary outcome was achieved in 20% (4/20) in the oligonol group and 15% (3/20) in the placebo group without being significant (p = 0.50, Fisher's exact test). As shown in Figure 1, a reduction in MRI-PDFF between weeks 0 and 24 was seen more pronouncedly in the oligonol group (mean difference 3.74 ± 4.67%) than in the placebo group (mean difference 2.61 ± 5.87%). The reduction in MRI-PDFF was, however, not different between two groups. Changes in clinical characteristics and biochemical tests between weeks 0 and 24 in each group are presented in Table 1. Although the improvement in secondary outcomes was observed in the oligonol group, changes in bodyweight, waist circumference, ALT, fasting blood sugar, HOMA-IR, lipid profiles, MDA, leptin, and CK-18 between weeks 0 and 24 were not significantly different between two groups (Table 1). No adverse events were reported in either placebo or oligonol groups.
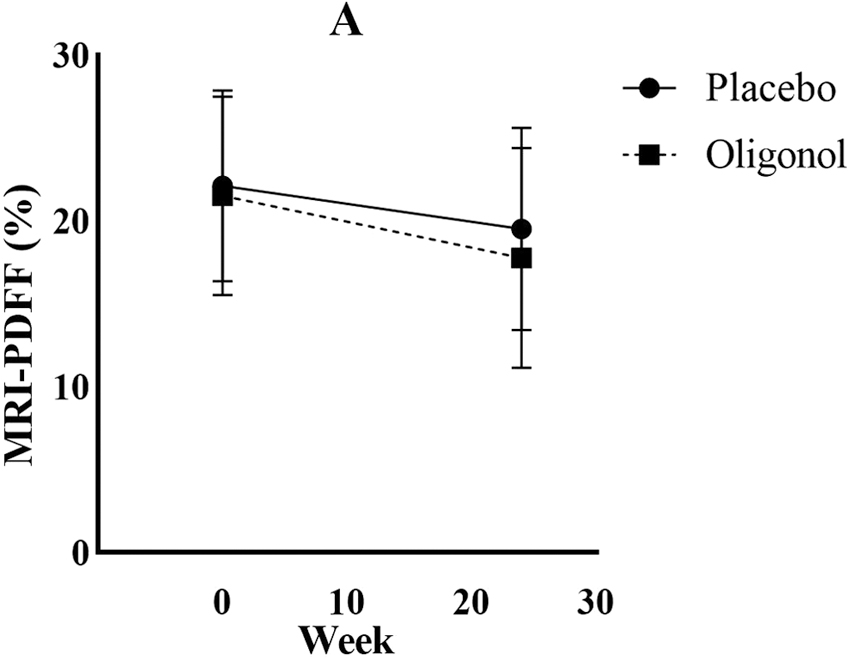
Changes in MRI-PDFF over time in each group. A, p = 0.02; ns = nonsignificant. MRI-PDFF, magnetic resonance imaging-derived proton density fat fraction.
Changes in Clinical Characteristics and Biochemical Tests Between Weeks 0 and 24 in Each Group
Comparisons between groups at week 24 by analysis of covariance.
ALT, alanine transaminase; BMI, body mass index; CK-18, cytokeratin-18; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment for insulin resistance; LDL-C, low-density lipoprotein cholesterol; MDA, malondialdehyde; MRI-PDFF, magnetic resonance imaging-derived proton density fat fraction.
The correlation between new serum markers and hepatic fat content or metabolic parameters
Significant correlations between MDA and bodyweight (r = 0.359, p = 0.02), and waist circumference (r = 0.32, p = 0.04) were noted, but there were no correlations between MDA and hepatic fat content or other parameters. A significant correlation between leptin and bodyweight was observed (r = 0.333, p = 0.04); however, leptin did not significantly correlate with hepatic fat content or other parameters. CK-18 significantly correlated with ALT levels (r = 0.426, p = 0.006) but not with hepatic fat content or other parameters. A significant correlation was seen between leptin and MDA (r = 0.344, p = 0.03).
Discussion
Oligonol is standardized oligomerized-polyphenol from L. chinensis extract and is rich in monomeric Flavan-3-ols and procyanidins. This was the first human study to evaluate the effects of oligonol in NAFLD. Results showed that a 24-week treatment of oligonol reduced percent hepatic fat on MRI-PDFF, bodyweight, waist circumference, ALT and fasting blood sugar. However, the changes were not different from the placebo group. The primary outcome was not achieved in this study possibly due to insignificant anti-NASH effect of oligonol or insufficient duration of treatment or participants' nonadherence to lifestyle modification (Supplementary Data S2).
An in vitro study demonstrated that oligonol reduced triglyceride accumulation in HepG2 cells in a dose-dependent manner through the suppression of lipid synthesis genes, such as acetyl-CoA carboxylase, fatty acid synthase, sterol regulatory element-binding protein-1, and the upregulation of β-oxidation enzymes, such as carnitine palmitoyltransferase 1a. 4 Similarly, Alexander-Aguilera et al. showed that lychee extract reduced serum lipid, abdominal fat, and the severity of hepatic steatosis in metabolic syndrome rats induced by a high fructose diet. 8 Despite positive results in in vitro and animal studies, a significant antisteatotic effect of oligonol was not observed in this human study.
In contrast to the negative results, a randomized double-blinded placebo-controlled trial by Nishihira et al. showed that a 10-week treatment of oligonol led to the reduction in bodyweight, waist circumference, subcutaneous fat area, visceral fat area, and insulin resistance. 5 In this study, although the reduction in fasting blood sugar at week 24 in the oligonol group were more pronounced than in the placebo group, the difference was not statistically significant. It is important to note that despite less adherence to diet control and less physical activities than those in the control group (Supplementary Data S2), patients in the oligonol group still experienced some degree of weight loss suggesting the possible weight-loss effect of oligonol. Further studies with a structured diet and exercise program are needed to confirm this hypothesis.
In this study, the effects of oligonol on various serum markers of NAFLD were also explored. Previous studies showed that serum leptin levels were directly correlated with the severity of hepatic steatosis indicating the role of peripheral leptin resistance in the development of NAFLD. 17 In contrast with previous studies, a significant correlation between serum leptin levels and hepatic fat content by MRI-PDFF or liver chemistries was not seen in this study. However, a significant correlation between serum leptin levels and bodyweight was observed in this study as has previously been shown in other studies. 18 Despite the correlation between serum leptin and bodyweight, oligonol treatment for 24 weeks failed to make a significant impact on serum leptin levels. Similar findings were also seen in a study by Nishihira et al. 5
Mitochondrial dysfunction with subsequent production of reactive oxygen species (ROS) and lipid peroxidation play a major role in NAFLD development. 19 MDA, a product of lipid peroxidation, has been used in preclinical and clinical studies as an oxidative stress marker. Although a 24-week treatment of oligonol reduced serum MDA levels, the changes did not significantly differ from the placebo group. In contrast to the authors' findings, Bak et al. showed that oligonol inhibited ROS production in an in vitro study using ferrous sulfate/hydrogen peroxide-induced lipid peroxidation in rat liver homogenates. They also demonstrated that oligonol treatment significantly reduced hepatic MDA levels and attenuated liver injuries caused by carbon tetrachloride (CCl4) in rats. 20
Hepatocyte apoptosis is believed to play an important role in the development and progression of NAFLD. 21 The stimulation of apoptotic pathways by liver inflammation leads to the activation of caspase cascade and the cleavage of intracellular substrates, such as CK-18, the major cytoskeletal protein in the liver. Plasma CK-18 fragment levels have been shown to be an independent predictor of NASH and are positively correlated with the degree of fibrosis. 10 In this study, a positive correlation between serum CK-18 fragment levels and ALT was observed.
This finding was not surprising given that the higher degree of inflammation would likely induce more apoptosis. Using a rat model of CCl4-induced liver injury, Bhoopat et al. showed that lychee extract significantly reduced the numbers of apoptotic cells in the liver. 22 In contrast to previous animal studies, significant changes in CK-18 fragment levels were not seen after 24 weeks of oligonol treatment in this study. The reason for this discrepancy might be related to the dosage. Animal studies suggested that the anti-inflammatory, antioxidant, and antiapoptotic effects of oligonol were dose dependent. 20,22 It was possible that the dose used in this clinical trial might not be high enough for oligonol to exert its antiapoptotic effect.
In this study, MRI-PDFF was used instead of liver biopsy in the diagnosis of NAFLD and in the determination of treatment response. A paired liver biopsy-MRI-PDFF study showed that using the cutoff value of 11%, MRI-PDFF correctly identified patients with hepatic steatosis grade ≥2 with the area under the receiver operating characteristic value of 0.90. 14 Using a cutoff value at 30% reduction in MRI-PDFF, MRI could predict ≥2-point reduction in NAS with sensitivity of 42% and specificity of 87%. 23 Therefore, the use of 30% reduction in MRI-PDFF as a primary endpoint of this clinical trial was a reasonable alternative to liver biopsy as this was an early study to explore the effect of oligonol in NAFLD.
This study had few limitations. Despite the reduction in hepatic fat content compared with baseline data in the oligonol group, the degree of improvement did not significantly differ from those in the placebo group. The placebo effect could be attributed to lifestyle changes of patients in the placebo group. Future studies with clearly defined dietary and exercise regimens are needed to control for these confounders and to determine the actual efficacy of oligonol. Second, the authors used MRI-PDFF to determine treatment efficacy instead of liver biopsy. Although MRI-PDFF is a reasonable noninvasive alternative to liver biopsy in the diagnosis of NAFLD, the test is imperfect in the determination of treatment response. The 30% reduction in MRI-PDFF that the authors used to signify primary endpoint has high specificity but low sensitivity. Therefore, some patients who actually had histologic response (defined by ≥2-point reduction in NAS without fibrosis progression) might have been mislabeled as nonresponders.
Conclusions
Oligonol has not shown a significant therapeutic effect in NAFLD when compared with the placebo. Further studies are warranted to determine whether the effect of oligonol will be stronger with the longer duration of treatment or with a higher dose, or whether it will have the additive effect when used in combination with lifestyle modification.
Footnotes
Authors' Contributions
M.C. contributed to the conceptualization, methodology, investigation, formal analysis, original draft preparation, and review and editing of the final draft. W.S. contributed to the investigation, data curation, project administration, and review and editing of the final draft. A.C. contributed to the conceptualization, methodology, and review and editing of the final draft. P.T. contributed to the conceptualization, methodology, supervision, and review and editing of the final draft. All authors read and approved the final article.
Data Availability Statement
Data will be available on request due to privacy/ethical restrictions.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
This study was partially funded by the Amino Up Co., Ltd. who produces and distributes oligonol in Thailand. This study was funded by the following funders. All funders provided the funding for the conduct of the study but the study was independent of it. Amino Up Co., Ltd. (Apart from the funding, the company also provided oligonol and placebo capsules for the study). Ratchadapiseksompotch Fund, Chulalongkorn University (Grant No. CU_GR_63_124_30_31). Alternative and Complementary Medicine for Gastrointestinal and Liver Diseases Research Unit, Department of Physiology, Faculty of Medicine, Chulalongkorn University. Center of Excellence in Hepatitis and Liver Cancer, Department of Biochemistry, Faculty of Medicine, Chulalongkorn University.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.