
Abstract
Objective:
To perform a systematic review of the literature regarding scientific reality of hippotherapy in children with cerebral palsy graded according to France HAS (Haute Autorité de Santé) recommendations and applied to the International Classification of Functioning.
Methods:
The research in MEDLINE and Cochrane Library databases was performed using the keywords: “Equestrian therapy,” “Riding for the disabled,” “Hippotherapy,” “Equine-movement therapy,” and “Therapeutic horse (back) riding.” The methodological quality of the articles was assessed using four levels of proof and three guideline grades (A: strong; B: moderate; C: poor).
Results:
Seven prospective, randomized controlled studies and one systematic review confirm the level of proof of hippotherapy in children with cerebral palsy with grade B. Hippotherapy in children with cerebral palsy contributes to improve motor function, symmetry of muscle contraction, spasticity, posture, and walking. Fifty prospective no randomized studies confirm the level with grade C for balance, motor coordination, lumbopelvic mobility, walking speed, functional development, and social behavior.
Conclusions:
Hippotherapy in children with cerebral palsy can be recommended. Regarding the literature data, the level of proof of hippotherapy in children with cerebral palsy is moderate (grade B).
Introduction
A
Cerebral palsy is the leading cause of disability in children. Interruption of oxygen supply to the fetus or brain asphyxia is classically considered the main causal factor explaining later cerebral palsy. It is most often the result of environmental factors, which might interact with genetic vulnerabilities, and could be severe enough to cause the destructive injuries. Cerebral palsy is a group of disorders that affect movement and muscle tone or posture. Signs and symptoms appear during infancy or preschool years.
In general, cerebral palsy causes impaired movement associated with exaggerated reflexes, floppiness or spasticity of the limbs and trunk, unusual posture, involuntary movements, unsteady walking, or some combination of these. It represents a nonprogressive disturbance of motor control, the result of a nonprogressive, permanent cerebral lesion of the developing brain (by agreement before the age of 3). 4 It is the source of impairments and disabilities of very variable levels, which impact on the neurological and functional development of the child. The main impairment is motor, frequently combined with cognitive, social, and communication disorders. 4
Hippotherapy designates treatment delivered on horseback by a health professional (physiotherapist, occupational therapist, speech therapist, psychologist, psychomotor therapist, adapted physical activities instructor, etc.). The movement of the horse is used as a therapeutic intervention or a therapeutic tool by the therapist. During hippotherapy treatment, the therapist identifies the impairments and disabilities of patients and sets the objectives to be achieved. 5 The therapist chooses re-educational methods to stimulate dynamic postural stabilization, recovery following disturbance of balance, and postural control through feedback and anticipation. 6
This practice aims to bring a real change in re-educational treatment in particular with reference to the practice of a physical activity with a substantial recreational element. These hippotherapy programs must be adapted to the capacities of the children, their symptoms, and their demands. It must be within the framework of a personalized treatment plan. That can be modified to accommodate observations and presumed needs, and in accordance with local, family, and institutional possibilities.
More than a quarter of international scientific publications on hippotherapy deal with the treatment of children with cerebral palsy that is what inspires the production of this literature review.
However, it is necessary to clarify the difference between hippotherapy and other equestrian therapeutic activities. There is therapy with the horse and equitherapy.
First, Renée de Lubersac has developed Therapy with the Horse in the 1980s. This corresponded to a publicized psychological treatment via the horse to improve cognitive, social, emotional even physical potential by psychological and physical means without riding. 7 This technique, centered on the psychological dimension, would not be deployed intentionally to target the physical and re-educational benefit of equestrian activity.
Then, there is instructor-led recreational equestrian therapy, which is comparable to equitherapy in France. Nontherapist riding instructors and their assistants conduct that. It is based on their equestrian training, on their knowledge of riders' handicaps, and on methods that allow use of proper safety conditions on appropriately trained horses. The horseback riding therapy therapeutic approach as implemented in the United States comprises procedures, precautions, contraindications, and a complete lesson plan that is followed by the instructors and their assistants. The PATH Intl. (Professional Association of Therapeutic Horsemanship International Center Accreditation) must certify it. The instructor chooses target objectives depending on the physical needs of the rider. These exercises are centered on incremental challenges to a rider's ability to stretch and move while maintaining balance and posture in all body positions while the horse walks slowly and evenly. 8 –12
Hippotherapy seems to be the most scientific and reproducible technique. The horse is used as a rehabilitation tool in an established protocol. The therapist uses the movements of the horse for therapeutic purposes on posture and motor function.
Objective
The principal objective of this work was to determine the level of scientific proof of the efficacy of hippotherapy in the re-educational management of children with cerebral palsy. This work come from data in the literature graded according to France HAS (Haute Autorité de Santé) recommendations and applied to the ICF. The secondary objective was to evaluate the hippotherapy protocols offered in the literature enabling an appropriate average duration of treatment to be proposed.
Materials and Methods
A systematic review of the literature was performed by searching the MEDLINE, Cochrane Library, PEDro, and Web of Science databases for the years 1966 to October 2021 (Fig. 1). References listed in the articles retained were considered, and articles matching the inclusion criteria, but not present in the initial search, were selected. A grey literature search was also performed using Google Scholar, Classic Google, and Abes. The keywords used were “Equestrian therapy,” “Riding for the disabled,” “Hippotherapy,” “Equine-movement therapy,” and “Therapeutic horse (back) riding.”
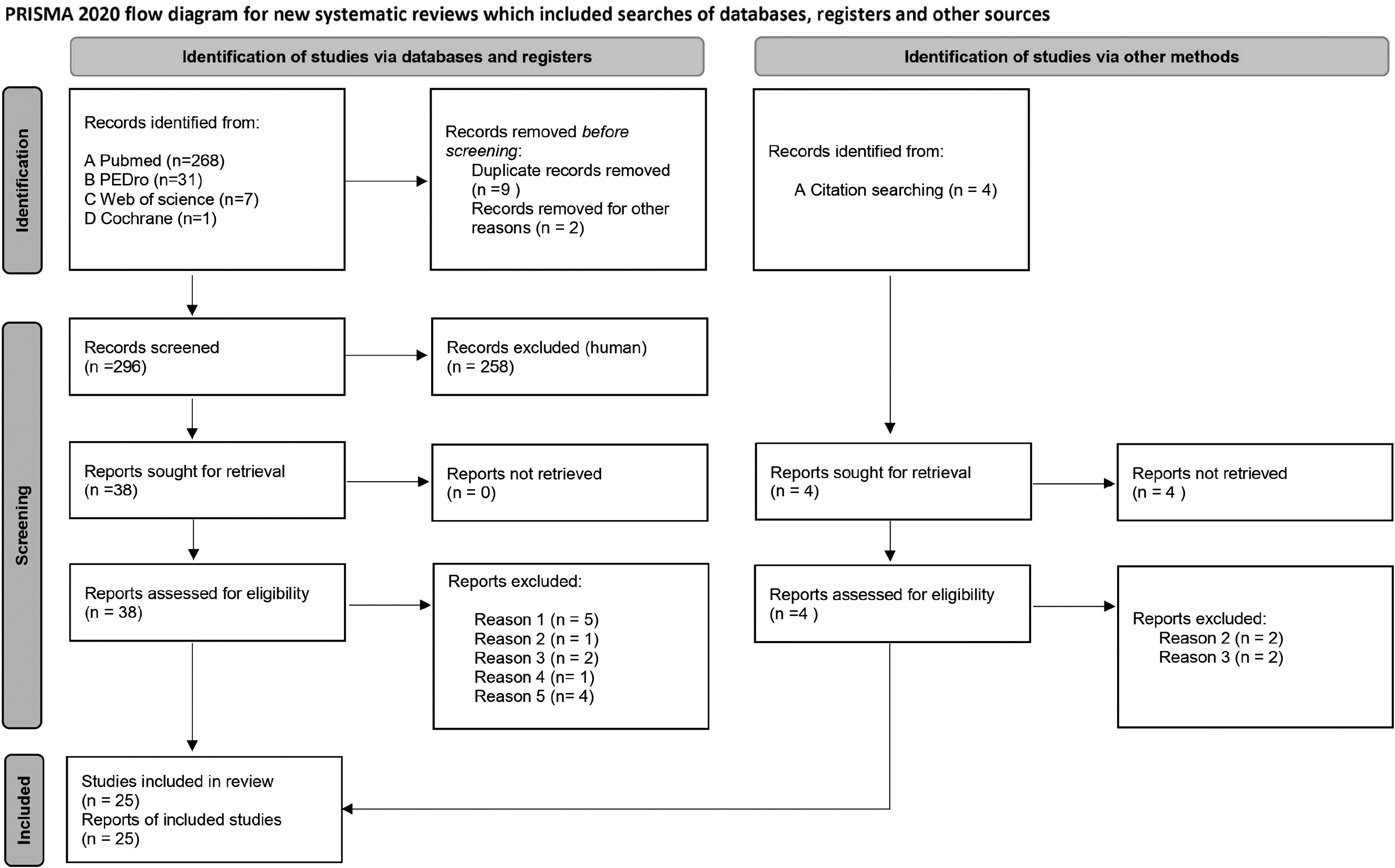
Article selection procedure for the literature review PRISMA 2020 flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
An initial selection of articles was made independently by the author because of abstracts to retain articles dealing with hippotherapy and/or equitherapy for children with cerebral palsy. Once these articles were selected, the whole text was recovered for reading. There was then a first reading, which allowed potential articles that did not deal with the subject directly to be ruled out. The following articles were retained: randomized controlled studies, reviews and recommendations, quantitative prospective and retrospective studies, and descriptive studies in French and English containing at least a connection between hippotherapy/equitherapy and children with cerebral palsy. Qualitative studies and case studies were excluded.
The articles were analyzed in two stages: a first stage devoted to the evaluation of methodology following the HAS (French National Health Authority) recommendations, 13 and then, a second stage devoted to the analysis of writing quality using the Consolidated Standards of Reporting Trials (CONSORT) checklist 14 for the randomized controlled trials and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist 15 for the other nonrandomized controlled trials.
The methodological quality of the articles was therefore evaluated following the good practice recommendations of the HAS of December 2010 in accordance with four levels of proof and three grades (A-B-C). 13 Studies with very poor quality methodology (inadequate, insufficient number of subjects, imprecise intervention) were, however, retained in view of the small number of clinical trials and randomized controlled studies, literature reviews, and recommendations present in the literature. In the absence of levels of proof, information was collected regarding professional practices. A study of methodology was also performed using the CONSORT criteria, 14 which is an international guidance tool intended to be used to evaluate the writing quality of a randomized controlled trial.
A binary score (0 = absent, 1 = present) was used for all criteria with a maximum score of 37. The scoring was performed solely for the prospective randomized studies.
The PRISMA guide was used to study the methodology of the other nonrandomized articles as the authors suggest. 15 A binary score (0 = absent, 1 = present) was used for all the criteria with a maximum score of 27.
The efficacy of the hippotherapy/equitherapy was then described for each HAS grade using the ICF parameters, 13 namely the impact on the impairments, activity limitations, and participation restrictions of children with cerebral palsy.
Results
The keyword search identified 296 articles. The empirical search based on the references listed in retained articles identified four additional articles. A total of 296 articles were listed in this way. The first selection exercise ruled out 258 articles, based on abstract reading, which revealed no elements relating to hippotherapy in children with cerebral palsy.
The reading of the whole text of the 38 remaining articles ruled out 13 additional articles: five dealing with the effect of a horse simulator and not hippotherapy (reason 1, Fig. 1),
16
–20
- one covering global proposals for the treatment of children with cerebral palsy but not specific to hippotherapy (reason 2, Fig. 1),
21
- two setting out the cardiovascular response of children with cerebral palsy during equitherapy sessions (reason 3, Fig. 1),
22,23
- one qualitative study on the parent's perception of their child with cerebral palsy after a hippotherapy session (reason 4, Fig. 1).
24
Four studies were not retained because they did not explore function of child with cerebral palsy (reason 5, Fig. 1). 10,25 –27 Three studies 28 –30 were analyzed but not retained in the literature review, as they were case studies.
Methodological quality
Methodological evaluation according to the HAS criteria
The methodological evaluation of the articles in accordance with France HAS good practice recommendations 13 did not find any established scientific proof (grade A). However, the study found a scientific presumption (grade B) for 10 articles 1,6,31 –38 from the 25 articles (level II) including 1 systematic review 35 (Table 1).
Level of Proof of Articles According to France HAS Grades
HAS, Haute Autorité de Santé.
The remaining 15 articles 39 –52 are evaluated as being studies containing substantial bias that is level IV with a low level of proof (grade C) (Table 1).
Evaluation of the writing quality analysis
Tables 2 and 3 summarize all items defined in the literature as quality criteria for the writing of a clinical study and verify their presence in the different parts of the article.
Methodological Study of the Randomized Controlled Articles Using the Consolidated Standards of Reporting Trials Checklist
Binary score (0 = criterion absent, 1 = criterion present after reading/analysis of the article against the 37 items on the CONSORT checklist); good methodological level for scores ≥22.
CONSORT, Consolidated Standards of Reporting Trials.
Source: Schulz et al. 14
Methodological Study of the Nonrandomized Controlled Articles Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Checklist
Binary score (0 = criterion absent, 1 = criterion present after reading/analysis of the article against the 27 items of the PRISMA checklist); good methodological level for scores ≥17.
PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Source: Page et al. 15
The CONSORT checklist allowed two levels of methodological evaluation to be distinguished for the prospective randomized studies:
First-level score higher than or equal to 22/37: six level II studies 1,33,34,36 –38
Second-level score below 22: one level II study. 47
The PRISMA checklist allowed two levels of methodological evaluation to be distinguished for the no-randomized studies:
Efficacy of hippotherapy and equitherapy
The efficacy of hippotherapy and equitherapy was evaluated in accordance with its impact on the impairments, activity limitations, and participation restrictions of children with cerebral palsy found in the literature (according to the ICF) (Table 4).
Scientific Reality of Hippotherapy in Children with Cerebral Palsy Graded According to France HAS Recommendations and Applied to the International Classification of Functioning
Analysis of the literature suggests a possible efficacy of hippotherapy with respect to the following:
Impairments
Improvement of the motor function of children with cerebral palsy classified as grade B of France HAS recommendations by five level II studies 1,31,34,35,37 and nine level IV studies. 5,6,39,40,43,44,48,49,51
Improvement in the symmetry of the muscular contraction of children with cerebral palsy classified as grade B of France HAS recommendations by two level II studies 31,48 and one level IV study. 49
Improved lumbar pelvic mobility of children with cerebral palsy classified as grade C of France HAS recommendations by a level IV study. 50
Improvement in the spasticity of children with cerebral palsy classified as grade B of France HAS recommendations by a level II study. 31
Activity limitations
Improvement in the walking parameters of children with cerebral palsy classified as grade B of France HAS recommendations by three level II studies, 34,36,37 and improvement in walking speed and cadence stride length classified as grade B of France HAS recommendations by one level II study 37 and two level IV studies. 43,47
Improvement of the posture of children with cerebral palsy classified as grade B of France HAS recommendations by three level II studies 32,46,48 and three level IV studies. 42,45,51
Improvement of the balance and motor coordination of children with cerebral palsy classified as grade B of France HAS recommendations by one level II study 38 and two level IV studies. 41,42
Improvement of the functional development of children with cerebral palsy classified as grade C of France HAS recommendations by a level IV study. 39
Participation restrictions
Trend toward improvement in the quality of life of children with cerebral palsy classified as grade B of France HAS recommendations by two level II studies 33,38 but with no statistically significant difference in one. 33
Three level IV studies 28 –30 were also analyzed but not retained in the literature review because of their very low methodological level (case study). They seem to show a grade C improvement in the social behavior and concentration of children with cerebral palsy, 30 an improvement in academic results, 29 and finally an improvement in communication. 28
Summary of the 25 studies retained dealing with hippotherapy
Table 5 summarizes all the studies in the literature review, with a brief description, and their results classified according to their HAS levels of proof.
Summary of the 25 Studies Retained Dealing Hippotherapy
av., average age; BOT2-SF, Bruininks–Oseretski Motor Proficiency short form; BOTMP, Bruininks–Oseretsky Test of Motor Proficiency; CBCL, Child Behaviors Checklist; CHQ, Child Health Questionnaire; CI, confidence interval; ContG, control group; CP, Cérébral Palsy; CP QoL-Child, The Cerebral Palsy Quality-of-Life Questionnaire for Children; EAPT, Equine Assisted Physiotherapy; EMG, electromyogram; Gait, Gait ride system of walking analysis; GMFCS, Gross Motor Function Classification System; GMFM, Gross Motor Function Measure; GMFM-E, GMFM dimension-E; HPT, Hippotherapy; ICF, International Classification of Functioning; ICF-CY, The International Classification of Functioning, Disability and Health for Children and Youth; IntG, intervention group; mv, millivolt; N, number of children; OR, odds ratio; PBS, Pediatric Balance Scale; PDMS, Peabody Developmental Motor Scale; PEDI, Pediatric Evaluation of Disability Inventory; PSPPYC, Pictorial Self Perception for Young Children; SD, standard deviation; SMD, standardized mean difference; SPPC, Self-Perception Profile for Children; WHOQOL-BREF, World Health Organization Quality of Life.
Protocol and average duration of treatment
The 25 studies included evaluated the efficacy of hippotherapy and equitherapy in 695 children with cerebral palsy. The average duration was 9.65 weeks (between 1 day and 26 weeks) with a follow-up of the children and a delayed evaluation in three studies: at 6 weeks postintervention, 8 at 12 weeks postintervention, 36 and between 12 and 14 weeks postintervention. 52
Few rigorous studies containing a detailed hippotherapy or equitherapy program applied to children with cerebral palsy were found in the literature. They were rather descriptions of tools associated with another therapeutic intervention. The only studies to explain the equitherapy sessions describe the child in a sitting position on the horse walking clockwise in a circle for 4 min and then for 4 min in the anticlockwise direction, with activities of touching different parts of horse's body or objects placed along the route. No detailed protocol of exercises to strengthen specific muscles or to develop proprioceptive function was found in the literature. 31,36
Quality evaluation of studies
Only seven randomized controlled studies 1,33,34,37,38,47,48 were found in this literature review testifying to the overall low scientific level of trials dealing with hippotherapy in children with cerebral palsy.
The numbers studied were also too small to allow results to be generalized. Sixteen studies 5,11,18,31,32,39 –44,46 –49,52 involved a population of <20 patients and therefore have low statistical power.
Finally, the level of the results analysis methodology and study design is unsatisfactory: substantial bias was demonstrated, 18,33 and the use of a nonvalidated “in-house” scale 2,32 does not allow actual effectiveness to be determined. Furthermore, some protocols displayed imprecise methods 28 or the use of a dose effect, which distorts the results.
Discussion
Although the use of hippotherapy for the re-education of children with cerebral palsy is relatively common, the authors note that rigorous studies on the subject are scarce. Their methodologies are debatable, difficult to use, and/or to apply to patients. The various hippotherapy modalities and protocols are not always defined sufficiently to allow generalization and implementation during hospitalization or outpatient care. No level 1 study or grade A recommendation was found.
The literature confirms a level of proof of hippotherapy programs in children with cerebral palsy at HAS grade B based on eight clinical studies. The question now raised is that of the mechanism of action of hippotherapy in the improvement of physiological parameters.
The principle of hippotherapy lies in the continuing generation of disequilibrium, where the horse generates rhythmic stimuli and postural changes, resulting in adjustments secondary to the imbalance. 20,53 The postural interactions dimension of equestrian practice acts as a postural stimulator for patients. It varies their speed and position forcing the riders to displace their center of gravity, working simultaneously on stability, dynamic posture, vestibular balance, and somatosensory reflexes. 48 It is also established that the simple fact of being in the saddle on a walking horse entails the contraction of around 300 muscles. 31 The horse's pendulum-like motion unbalances the rider's seat imposing more than 2000 postural adjustments every half hour. 31
Children with cerebral palsy often have postural disorders related to asymmetric muscle contraction, in particular of the adductor muscles and the spinal muscles. 1,3,36,54 –56 The erector spinae muscles are often active in isolation, which permits the voluntary maintenance of trunk posture by the child. Postural disorders seem to increase during dual task activity that requires particular attention. So postural adjustment, to anticipate the disequilibrium that is induced during the performance of an active movement, does not occur.
The motor impairment of children with cerebral palsy represents an anomaly of the automatic antigravity responses for which these children must compensate by voluntary control, when their neuromuscular potential allows this. 57 This anomaly is also accentuated by the pronounced lack of axial proprioceptive references in children with cerebral palsy. 19 This prevents them from feeling their position in space and therefore from managing the imbalance.
Pérennou et al. 58 demonstrated that muscular tone mainly that of the extensor muscles is the main agent in combating gravity. The mechanisms by which it is distributed (spinal cord and brain stem) are the fundamental mechanisms of postural control making the nervous system the main organ of balance. The integrity of the cerebral structures involved in the control of antigravity orientation is necessary for correct postural orientation. It may therefore be supposed that the topography of cerebral damage in children with cerebral palsy may be reproduced in the disordered perception of the vertical that follows strokes. This may be due to damage to the brain stem, cerebral hemispheres or central and peripheral damage to the gravity sensing, and somatosensory and vestibular pathways. 58
Finally, postural stabilization is the result of a complex physiology requiring the choice of a stabilized frame of reference and involving cerebral control associated with the contribution of sensory afferents. 58 The brain uses a number of limited, tested, stored motor maneuvers in a repertoire that in principle include the response elements appropriate to usual situations. 58 There seems to be some plasticity since new strategies may be learnt, perhaps, for example, by means of hippotherapy, in line with the postural stimulation of children with cerebral palsy.
The aim of the re-educational care of children with cerebral palsy is to improve their independence by optimizing their functional and locomotor capacities. Children with cerebral palsy show abnormal antigravity automatic responses. Hippotherapy appears to improve posture in children by improving muscle tone in the extensor muscles.
The hypothesis can then be advanced that hippotherapy will improve the functional independence of children with cerebral palsy by optimizing their walking ability 6 through an improved representation of the environment with better control of postural stabilization. This may be made possible by restoring the balance between the contraction of agonists and antagonists (extensors/flexors) allowing the extensor muscles to fulfill their role in combating gravity. Furthermore, the symmetrical left–right walking motion of the horse will repeatedly displace the child on either side of the midline causing continuous proprioceptive and vestibular stimulation, which will increase awareness of the body. Thus, these repeated postural adjustments will help the child to create a more “normative” perception of the midline and of the symmetry of loading. 36
The choice of horse will also have an impact on the functional result. The principle of hippotherapy is to use equine biomechanics on the biomechanics of the child with cerebral palsy to fight against harmful motor patterns. A precise and objective analysis of the gait of the child and the horse is mandatory to find a pair to improve the functions of children with cerebral palsy.
The performance of high-powered randomized clinical studies is thus necessary to demonstrate the efficacy of hippotherapy in children with cerebral palsy. The objective will be to show the superiority of hippotherapy over conventional treatment in the functional independence of children with cerebral palsy. These studies will perhaps result in hippotherapy being viewed as a real re-educational resource that may lead to treatment being funded by social security, as is already the case in Sweden, Norway, and Switzerland, 59 allowing it to be used by the majority of patients.
Conclusions
There is no proof of the efficacy of hippotherapy in the re-education of children with cerebral palsy. However, literature on the subject is scarce, and from the data currently available, it is possible to suggest that hippotherapy could form an integral part of the treatment of children with cerebral palsy. Further work is necessary to better specify the content of hippotherapy programs and protocols, alone or associated with other therapies (multisensory stimulation methods …) and their medical–economic impact. In particular, it seems essential to validate the content of sessions supporting this practice and to develop evaluation tools specific to hippotherapy. This is why a survey of good practices and a “state of the art” is necessary to prove the effectiveness of hippotherapy, to standardize practices and programs, and to promote their recognition by health authorities.
Footnotes
Authors' Contributions
E.P.: writing review. P.F. and D.V. proofreading and correction.
Author Disclosure Statement
The authors do not report any potential conflicts of interest.
Funding Information
No funding was received for this article.