
Abstract
Objective:
Music listening interventions are utilized in a wide variety of clinical settings to help patients manage stress, anxiety, pain, discomfort, as well as attendant influences on sedative exposure, delirium, and cognitive functioning. While the body of research regarding the use of music-based listening interventions continues to grow, there is a paucity of information in the literature about specific music used for listening interventions. The purpose of this secondary analysis is to examine the music that study participants identified as their preferred music and listened to during the study.
Design:
This secondary analysis is based on data from a parent study, which was a three-arm randomized controlled trial attesting a patient-directed music (PDM) listening protocol to manage the psychophysiological symptom of anxiety.
Setting:
Twelve intensive care units in a major metropolitan area in the United States.
Subjects:
Participants included the 126 mechanically ventilated patients enrolled and randomized to the PDM listening arm of the study.
Results:
Data presented in this study include playlists from the 12 genres patients self-identified as preferred with specific groups and artists requested for music listening during the study. Discographies of the playlists are also included.
Conclusions:
The efficacy of interventions is impacted by the design of the intervention and the selection of music utilized. Implications of this analysis further explore the role of a board-certified music therapist (MT-BC) in designing and implementing a music listening intervention. The specialized knowledge on the therapeutic use and benefits of music that an MT-BC possesses supports the development of quality study intervention and appropriate implementation. The review of the music utilized in the parent study provides detailed information about the music utilized to inform future research focused on music listening interventions to effectively build on previous studies.
Clinical Trial Registration:
Introduction
The research surrounding the use of music listening during mechanical ventilation (MV) has increased over the past two decades. As clinicians and researchers collaborate to examine nonpharmacological interventions to help patients manage the stress and anxiety experienced during MV, music has emerged as an ideal option given its effect on the sympathetic nervous system by decreasing heart rate, respiratory rate, blood pressure, improving sleep, and decreasing sedative exposure. 1 –12 Due to the critical health status and limited energy of MV patients, listening to music is an appropriate intervention as it requires little of the patient. 13 –17 The accessible nature of music through streaming platforms and mobile devices allows patients to easily engage in listening to music. 14,15,18 Additionally, while music listening interventions are addressing a multiplicity of symptoms across patient populations, listening to music can also help to manage different symptoms simultaneously. 4,14,19 –28 Music listening is also a desirable nonpharmacological approach due to the lack of negative side effects. 8,14,15,18,29 –31
These myriad benefits of music listening are further supported by patients and family member accounts from listening to their preferred music that is comforting and they were grateful to have their music to use during their MV. 8,17 Assessment and implementation of music listening with preferred music contribute to effective outcomes. However, there is often an absence of information and clarity regarding the music utilized for the intervention, despite the existence of reporting guidelines. 32 –36 Specific descriptions about each facet of the music intervention contributes to reporting transparency that provides other researchers with accurate knowledge of the intervention and the specific music utilized. Providing clear and detailed information indicates why and how music was selected for the study, fosters replicability, as well as translation of the intervention into clinical practice. Therefore, the purpose of this study was to provide an in-depth analysis of the preferred music of mechanically ventilated intensive care unit (ICU) patients enrolled in a randomized controlled trial.
Materials and Methods
Overview of the parent study
The data included in this secondary analysis is from a parent study in which the primary aim was to evaluate whether a patient-directed music (PDM) listening intervention was effective in decreasing anxiety and reducing exposure to potent sedative medications in patients receiving mechanical ventilatory support. 4,16 The parent study was reviewed and approved by the Institutional Review Board at the University of Minnesota.
This three-group randomized controlled trial recruited patients from 12 ICUs in the Minneapolis-St. Paul metropolitan area. Patients were randomized to (1) PDM, involving patients listening to their preferred music whenever they choose for as long as they wanted to listen. Music was delivered through noise-canceling headphones, (2) active control conditions included the use of noise-canceling headphones only, whenever they wanted to for as long as they wanted, or (3) the control group received usual ICU care typical of the respective unit. Details from the parent study are available in previous publications. 4,7,13,16,17,31
Description of PDM listening protocol
The PDM listening intervention for the study involved the use of patient-preferred music between 60 and 80 beats per minute. 4 The PDM protocol was designed to empower patients not only to identify their preferred music but to also determine the frequency and length of time they wanted to listen to music. Patients were able to select music from any genre and were not limited with regard to their music preferences. 16
When a patient was enrolled into the study and randomized to the music group, they were immediately provided with an MP3 player and a set of five compact discs (CDs) of relaxing music preselected by the board-certified music therapist (MT-BC). These CDs were selected for the starter set to provide an array of music that includes a variety of instrumentation of piano, guitar, Native American flute, harp, and guitar and flute combined. This allowed patients the opportunity to begin listening to music immediately upon enrollment and to exert the power of choice in their listening. Table 1 includes a listing of the starter set CDs selected. They all included music between 60 and 80 beats per minute. The variety of instrumentation allowed patients to select what they wanted to listen to based on their preferences, and it allowed patients to begin listening to music immediately. 16,17
Start Compact Disc Set
Assessment of music preferences
The MT-BC met with patients within 24 h of randomization to the PDM group. During the music preferences assessment, the MT-BC utilized the Music Assessment Tool (MAT) to determine the patient's preferred music. 7 Patient-preferred refers to music from any genre that the participant identifies as music they would like to have provided. Patients were asked to identify genres of music, groups, artists, and instrumentation they like, as well as any groups, artists, and instrumentation they did not like. 13 Fifteen broad genre categories were included on the MAT form: alternative rock, blues, classical, country, heavy metal, hip hop, jazz, new age, oldies (rock and roll, doo-wop, and surf music from the second half of the 20th century), popular, reggae, rhythm and blues, religious/sacred, rap, rock, and world music. Discerning these preferences ensured the MT-BC could provide music the patient wanted to listen to and would best be able to utilize.
Compiling and providing patient-preferred music
The MT-BC then compiled the patient's preferred music purchasing it in CD and/or digital format and uploading it onto the research computer. In compliance with copyright laws, the music was then burned onto CDs and delivered to the patient, which patients returned at the end of enrollment. Throughout the study, patients in the PDM group met with the MT-BC daily throughout the study to ensure music preferences were assessed continually and to allow the patient to identify and request new or different music they wanted. This allowed patients to request music to address different needs such as providing distraction or improving mood, and to continue to be tailored to their individual preferences and provide more music for their listening options. These daily visits also allowed the MT-BC to engage in regular follow-up with the patient's nurse. The MT-BC performed equipment checks to ensure the MP3 player and headphones were functioning properly and that the equipment was accessible to patients. This clinical trial was conducted from 2006 to 2011 and while the technology utilized for the study is now obsolete, the PDM listening protocol is applicable to current technology.
The MT-BC was responsible for locating and purchasing music that fit the parameters of 60–80 beats per minute and patients' preferred music. Additionally, the MT-BC burned the music onto CDs, delivered the music to the patient, and maintained documentation of the music data. The MT’-BC's specialized knowledge of music, music genres, and the effects of music helped to support the process of patients identifying receiving their preferred music, even as they were challenged in communicating. This expertise also contributed to maintaining treatment fidelity of the study protocol and detailed reporting of music and CDs distributed by genre. 16
Patients' preferred music selections were documented by genre and instrumentation on the MAT form. Additional information and music requests that patients provided following the initial assessment were recorded throughout their enrollment in the study and included details, including artists, groups, albums, and songs. The MT-BC also ensured that each piece of song and music met the 60–80 beat per minute to maintain the integrity of the PDM protocol.
Analysis
Descriptive statistics were used to summarize the data to address the study purpose. Specifically, responses to the MAT were analyzed descriptively by the frequency of the different ways that patients reported engaging in music listening, and the genres identified as preferred throughout enrollment in the study were summarized. A description of sample playlists is provided as well as a summary of music provided that was requested by patients from each of the different genres.
Results
Music listening engagement inclusive of when and reasons for listening, and music from 15 broad genre categories were included on the MAT form. 7,16 There were 126 patients randomized to the experimental PDM group, with a mean age of 59 (SD14). 4 Figure 1 illustrates the type of music listening engagement, including the percentage of patients that reported they listen to music during mealtimes, to manage stress, to relax, and for enjoyment. Patients reported listening to music most frequently for enjoyment and to manage stress. It is important to recognize that a patient may listen to music for multiple reasons.

Music listening engagement.
Patients reported their music preferences based on genres. Figure 2 details the percentage of patients who selected the different genres of music. Patients could identify and request music from as many genres as they preferred. The most frequently identified music preferences included classical (75%), jazz (60%), and oldies (41%).
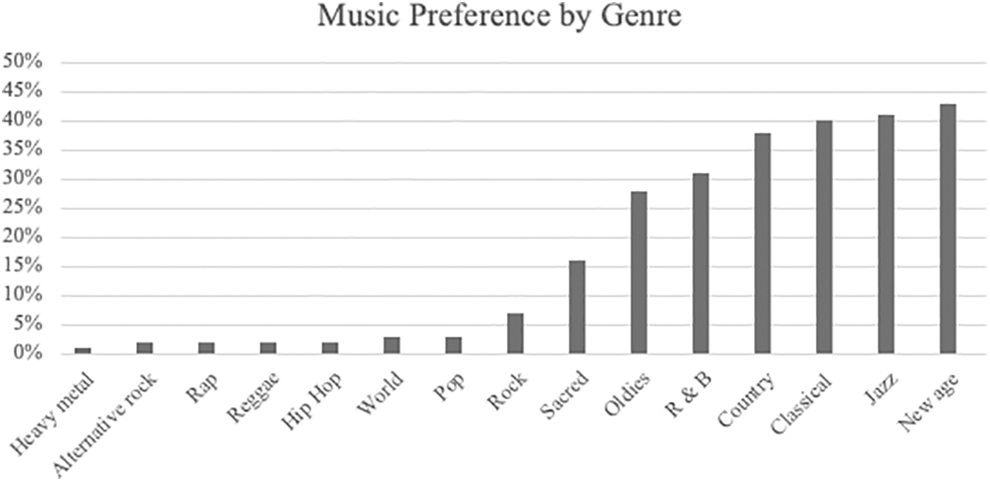
Music preferences by genre.
Overall, patients requested music from 12 distinct genres for their preferred music listening. 16 Over the course of the clinical trial, a total of 1580 CDs of music were distributed to the participants in the PDM group. 16 Each CD was personalized by the MT-BC based on the specific music preferences of each participant. While it is not feasible to provide a full review of all the music utilized in the study, sample playlists are included to illustrate specific music utilized from each requested genre. Patients randomized to the PDM group received a starter set of CDs to allow them to begin to listen to music immediately (previously listed in Table 1). Tables 2 –13 delineate the music and various artists and groups that participants specifically requested. Appendix A1 includes the discographies for each of the sample playlists.
Blues
Classical
Country
Jazz
New Age
Oldies (1940–1970)
Popular
Rhythm and Blues
Reggae
Sacred
Rock
World Music
The music included in each of the sample playlists meets the a priori conceptualization of 60–80 beats per minute. Sample playlists are included from 12 of the 15 genres. The sample playlists include 15 songs or pieces of music from each genre to provide an overview of the music and to provide more detail regarding the variety and scope of music utilized in the study. The sample playlists provided illustrate some of the artists whom patients requested, and the music from these artists that met the study criteria. These sample playlists provide transparency in reporting the music utilized in the PDM listening study intervention. 32 –36
Discussion
Music listening is an intervention that has been implemented in a wide array of health care settings, including surgical and procedural areas to help manage the symptoms patients may experience. 2,37 –40 While research findings report significant reductions in symptoms of anxiety, pain, discomfort, 21,41,42 and to promote MV weaning, 43 these outcomes are reported from studies that have provided patients with limited choice regarding the music to which they will listen. The majority of study protocols provided music from a predetermined and often limited list of music the researcher has selected 11,12 and most studies do not draw upon the expertise of a music therapist. Systematic reviews of have reported that in the majority of research protocols include only music preselected by the investigators(s) which limits patient choice limitations. 21,41,42 In fact, research protocols that promote patients using their own music or allow to select preferred music from a full range of genres are quite limited. 4,42
It is a minomer to refer to investigator-selected music for intervention testing as “patient-preferred” music interventions. The experimental PDM intervention implemented and tested in the parent clinical trial was unique in that patients were not limited in the music they could request as they were active participants in the research protocol. This ensured they could select their preferred music from multiple genres and feel confident that indeed this music would be provided by the MT-BC.
It is important to consider that the music a patient chooses may change over time. For example, a patient may select one genre or piece of music to foster relaxation and later may select music from a different genre to foster distraction to manage anxiety or pain. Providing patients the power of choice allows them to determine what music is preferred based on individual needs or symptoms. This is further reinforced by patients' requests for more music in music intervention studies. It is recommended that researchers consider the dynamic nature of patient music preferences to foster patient-centered care 44 and patient satisfaction. 45,46
Knowledge of music, music genres, its therapeutic uses, and cultural considerations related to music is a specialized area. The vast majority of music listening research has not included a music therapist as an integral member of the research team. To implement a broader scope of music and to select music within the 60–80 beats per minute it is imperative to collaborate with a music therapist to ensure the music is carefully and properly selected. A music therapist is skilled in compiling music from a wide variety of genres to ensure the proper and safe implementation of music to address hypothesized outcomes. 16,41
Previous research implementing music-based listening interventions have lacked building on the previous research, 41 due to the fact that much of the literature included a limited description of the music utilized. Typically, the focus of the music-based research article is on the outcomes of the listening intervention. Researchers may report a genre(s), but specific details regarding the aspects of music are not included. As a result, future research studies cannot build on previous findings. Detailed and specific information about the music and music listening protocol is vital given the music is the intervention being tested and warrants full description in the article.
The increasing body of literature indicates the growing use of music listening in patient care. It is often described as a cost-effective intervention because it allows the patient to self-manage symptoms and may reduce symptomology. However, there has been limited exploration of the cost/benefit analysis of music listening. While a recent article reported the cost-effectiveness of a PDM listening protocol among critically ill mechanically ventilated patients, 31 more research is needed to evaluate this in addition to salient patient-reported outcomes.
The research surrounding music listening has focused on the symptomology of anxiety, stress, pain, and discomfort. There is potential to move the research to evaluate the effect of music listening on other patient symptoms that may complicate the treatment process. A recent study explored the use of music listening with complex, critically ill patients to reduce delirium. 45,46 The potential to bring music listening into new areas to improve patient care is considerable. This potential may best be achieved through interdisciplinary collaborative practice and research. Music therapists possess unique knowledge of music and its impact on health, healing, and wellbeing. Research testing music listening interventions in the care of patients with complex health care needs, including management of chronic conditions, would benefit from the expertise of a music therapist to inform the protocol and the music selected for intervention.
Additionally, to effectively advance the understanding of music-listening interventions, researchers must report detailed information regarding all aspects of the music intervention. Clear and transparent reporting regarding music preference assessment and utilization of those findings to fully inform music-listening interventions will ensure that study protocols can be replicated and eventually integrated into the clinical practice environment.
Conclusion
Music listening interventions are increasingly being implemented in a wide array of procedures and patient care environments. While this body of research has been increasing over the past two decades, there is often a lack of information and clarity about the music intervention protocol as well as the music selected and utilized for intervention. There have been recent calls for clear and transparent reporting of music-based interventions to ensure they conform to Consolidated Standards of Reporting Trials (CONSORT). 47 Researchers are urged to provide detailed descriptions of the music-based interventions to ensure that future research can be clearly informed about the music to effectively build upon the research evidence.
The cost-effectiveness and accessible nature of music listening have made it a viable intervention even with critically ill patients. The complex needs of critically ill patients and the various symptoms that music listening can address, suggest that a clinician trained and knowledgeable in the therapeutic use of music should be in charge of designing the music-based intervention. As in any type of intervention study, the design of the intervention is guided by a clinician with the area of expertise. The expertise that an MT-BC can provide in designing music-based interventions is evident in methods and models that program music for therapeutic use by analyzing specific elements of the music and utilizing a systematic approach to curating music for music-listening interventions can have greater efficacy. 48,49
The clarity in reporting all aspects of a music-listening intervention, as well as integrating the expertise of a music therapist in designing the intervention are essential in moving these types of interventions into new areas of patient care and to addressing new and different symptoms. This collaborative and targeted approach to implementing music-listening interventions will help to propel and advance this body of research and literature.
Footnotes
Authors' Contributions
A.H. as the lead author took the lead on writing and preparing the article. She created the figures with music engagement data and music genre data. She also reviewed the tables and playlists discographies. K.J. collated all the secondary data, preparing it for presentation in the article. She created the tables for the music playlists from the original data from the parent study and gathered the information for the discographies for each playlist as well. L.C. contributed to writing the introduction of the article and provided feedback and critical edits on the article as a whole.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research or the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The project described was supported by Grant Number R01NR009295 from the National Institute of Nursing Research, National Institutes of Health (L.C., Principal Investigator). The study sponsor had no role in the design, collection, analysis, or interpretation of the data; in writing of the article; or in the decision to submit the article for publication. This work was completed while L.C. was at the University of Minnesota, School of Nursing.