
Abstract
Background:
Complementary medicine (CM) is often used as an opportunity for preventive health measures and supportive self-care practices. This study aimed to explore the use of self-care practices and preventive health strategies and the aspects of the experienced emotions during the COVID-19 pandemic in a population with an affinity for CM.
Methods:
The authors conducted an exploratory cross-sectional study using an anonymous 41-item online survey in the German language. The survey respondents were recruited among adults with an affinity for CM (e.g., as targeted through their memberships in CM associations) from September 2020 to February 2021. A selection of self-care methods, mainly from CM, was presented in the questionnaire. Numerical rating scales (NRSs), ranging from 0 = minimum to 10 = maximum, were used to measure the intensity of different emotions experienced during the pandemic. Statistical analysis was carried out descriptively.
Results:
A total of 1605 participants (80.6% female; mean age: 55.4 ± 12.6 [SD] years; 43.9% holding a university degree) were included. The use of self-care methods for health promotion during the pandemic was reported by 86.8% of the respondents. Respondents favored staying in nature (85.6%), healthy nutrition (85.6%), and physical activities (83.6%). More than 60% of the respondents made use of vitamin C and/or D, herbal medicines, nutritional supplements, relaxation techniques, breathing exercises, homeopathy, or meditation for health promotion. The analysis of emotional status by NRS (0–10) revealed the lowest mean ± SD (standard deviation) for “feeling lonely” (2.6 ± 2.9) and “feeling anxious” (2.8 ± 2.6), and the highest mean for “feeling connected to others” (6.2 ± 2.5) and “well-being” (5.8 ± 2.4).
Conclusions:
Participants used a wide variety of self-care methods and prevention strategies to promote their health during the COVID-19 pandemic and showed, overall, a balanced emotional status. Further research should include a control group representative of the general population, to investigate the possible impact of self-care strategies.
Clinical Trial Registration Number:
“Deutsches Register Klinischer Studien” (German Clinical Trial Register); registration number: DRKS00022909.
Introduction
The World Health Organization declared the coronavirus disease 2019 (COVID-19) outbreak, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a pandemic on March 11, 2020. 1 Infections can be asymptomatic or can present with mild symptoms (mostly cough, fever, cold, and loss of smell and taste), but can also lead to severe pneumonia and multiorgan failure resulting in death. 2,3 In Germany, cumulative data showed that 10% of SARS-CoV-2-infected people needed to be hospitalized, and the lethality rate was 1.8% (as of November 23, 2021). 3
At the time the authors designed this study in April 2020, vaccines were still not available, and the treatment options for COVID-19 were insufficient. Nonpharmaceutical interventions (NPIs), such as face masks, social distancing, lockdowns, quarantine, and isolation, were implemented to contain the pandemic. 4,5 Several studies ascertained the presence of psychological distress and mental health issues in the general population during the pandemic. 6,7 Due to a lack of scientific evidence at this time, no other preventive measures, for example, those regarding a healthy lifestyle, have been recommended by the health authorities in Germany thus far.
However, a health-promoting lifestyle consisting of physical activity, healthy nutrition patterns, mind–body therapies, and mental well-being/wellness as a self-empowering strategy for disease prevention, along with specific treatments and therapeutic interventions, is considered an important component of complementary/traditional whole medicine systems. 8 –10 Thus, the use of health-promoting methods is assumed to be popular among people who are in favor of complementary medicine (CM). 11
Surveys conducted among the general population in the Netherlands (NL), Norway (NOR), and Sweden (SWE) investigated the use of self-management strategies from the field of CM for the prevention and treatment of COVID-19-related symptoms: 30.3% of the respondents made use of self-help techniques, but only a few respondents used them specifically to prevent (4.4%) or to treat (0.4%) COVID-19. Yoga, meditation/mindfulness, and relaxation techniques were the most commonly practiced health-promoting methods. 12
An early systematic review of clinical studies on CM in the treatment of COVID-19 patients published until July 2020 indicated that a variety of treatments, mainly Chinese Medicine (qigong, acupuncture, Chinese herbal Medicine, relaxation techniques), were studied. The authors observed an improvement in psychological symptoms (e.g., depression, anxiety, stress, negative emotions) and physical symptoms (e.g., inflammatory factors, physical activity). 13
CM has a long tradition in Germany and is popular not least because of large lay associations, such as Kneipp-Bund e.V. (Kneipp Association) and Natur und Medizin e.V. (Nature and Medicine), with tens of thousands of members. 11,14 They support the dissemination of information on CM principles among their members; thus, their members are supposed to be more health conscious than the general population, and they are supposed to have own concepts of how to prevent diseases and foster health. 15 However, the extent of implementation of self-care methods during the pandemic among people with an affinity for CM in Germany remains unclear.
This cross-sectional study aimed to evaluate the types and use of self-care methods and prevention strategies used and the emotional status among people with an affinity for CM during the COVID-19 pandemic.
Materials and Methods
Study design and setting
This explorative cross-sectional study was performed between September 18, 2020, and February 1, 2021. People who were familiar with and in favor of CM were asked to participate in an anonymous online survey in the German language.
The study was conducted by the Institute of Social Medicine, Epidemiology and Health Economics of the Charité–Universitätsmedizin Berlin and approved by the University Ethics Committee (EA2/127/20, July 07, 2020, Berlin). The study was registered in the “Deutsches Register Klinischer Studien” (German Clinical Trial Register).
Participants and recruitment
Having internet access was a precondition to participate. The inclusion criteria were the provision of signed informed consent for data analyses and confirmation of age ≥18 years. The authors addressed the questionnaire to adults who considered themselves to have a relationship with CM (e.g., through a membership in a CM association). Participants were mainly recruited through the nonprofit CM associations Kneipp-Bund e.V. and Natur und Medizin e.V. They promoted the study in the member magazines and through social media (e.g., Twitter, Facebook, online newsletters). Furthermore, the authors promoted the study through the Charité Outpatient Department for Complementary and Integrative Medicine and on the website of the patient and citizens' initiative “Weil's hilft!” (Because it helps!) and Gesundheit aktiv e.V. (Health active e.V.).
Outcome measurement and data collection
The questionnaire was implemented using the SoSci Survey software (Leiner, 2020)
16
and was made available to participants at
The authors prospectively collected sociodemographic data such as age, sex, household size, postal code, and full-day childcare responsibility. They asked about school education, highest vocational qualification, employment status, and, if employed, about essential worker status and the possibility of working from home. The authors inquired about memberships to CM associations (Kneipp-Bund e.V., Natur und Medizin e.V., others, none).
Furthermore, they asked about chronic diseases and risk factors for a severe course of COVID-19 (diabetes mellitus, chronic lung disease, chronic liver disease, heart disease, hypertension, obesity, immunodeficiency, smoking, cancer) and about the use of officially recommended NPIs (handwashing, hand disinfectant, facemasks, cough and sneeze etiquette, physical distancing, and reduction of direct social contacts). 17
The frequency of the use of (1) general health-promoting measures and (2) CM during the 12 months before the pandemic was captured with the help of a 4-point or 5-point Likert scale. To determine the self-care methods used for health promotion in the prevention or treatment of COVID-19, a selection of 17 popular CM measures was presented (physical activity, staying in nature, hydrotherapy, relaxation techniques, meditation, breathing exercises, healthy nutrition, nutritional supplements, vitamin C and/or D, other vitamins, herbal medicines, homeopathy, Anthroposophic medicine, Ayurveda, Chinese Medicine, nasal rinses, yoga, others). The measures were not further specified, and so, it was up to the respondents to define their nutrition as healthy or their techniques as relaxing. Free text boxes in “other” could be used to enter other applied measures. Participants were asked to rate the success of the CM methods used (strong, medium, low, don't know).
The authors also captured data on SARS-CoV-2 infections that had occurred (sickness severity, location of treatment, number of illness days) as well as whether there was contact with people with COVID-19 and personal knowledge of persons who died from COVID-19.
To capture the current emotional status during the pandemic, nine different questions about being stressed out, being relaxed, feeling anxious, worrying, feeling sad, well-being, feeling lonely, feeling connected to others, and missing physical contact with others were evaluated with a numerical rating scale (NRS) ranging from 0 to 10 points (0 = minimum to 10 = maximum). The questions used to capture emotional status considered anxiety and worries to be basic emotions 18 ; perceived stress, relaxation, and well-being were considered important determinants for the state of mind and life satisfaction 19 ; and belongingness and feeling connected to others constituted a basic psychological need, 20 while perceived loneliness was an impairment to fulfilling this basic need. The authors decided to inquire about these aspects because they assumed they would be influenced by living conditions and changes in social life during the pandemic, and they used the NRS because it elicits quick and intuitive responses.
Furthermore, the authors asked if social contact in general had intensified (yes; no). Employees were asked about worries regarding their professional lives (no; yes, but not so many; yes, a lot).
As an option, respondents could enter their e-mail address voluntarily and separate from other data to obtain a chance to receive 1 of 50 books about CM as an incentive prize that was to be randomly drawn after ending the study in February.
Statistical analysis
Statistical analysis was carried out descriptively using IBM SPSS Statistics (version 26). As this was an explorative study, no sample size calculation was performed, but the authors aimed to include ∼2000 participants. The quantitative descriptive analysis reports mean values, medians, standard deviations (SDs), interquartile ranges (IQRs), and absolute and relative frequencies (valid percentages). For graphical presentation of the results, MS Excel (version 2110 Build 16.0.14527.20270) was used.
Subgroups
The authors compared females with males and different age categories (18–30, 31–50, 51–70, >70 years old). To explore whether the emotional status was related to specific characteristics, they compared participants who reported being in a more “positive” emotional status with those who reported being in a more “negative” emotional status. To define positive and negative emotional status, the values of the seven items related to emotions (stressed, anxious, sad, worried, lonely, relaxed, and well-being) were added for a total score ranging between 0 and 70 points. The items “being relaxed” and “well-being” needed to be recoded inversely for this procedure.
Instead of a cutoff value, the authors decided to consider participants who had 0–21 points (on average 0–3 points per question) to have a rather “positive emotional status” and those who had 49–70 points (on average 7–10 points per question) to have a rather “negative emotional status” and included them for this analysis.
Results
Sociodemographic data
A total of 1605 people participated in the survey and consented to the data protection statement. Recruitment was stopped in February 2021. However, the questionnaire was incompletely answered by 226 participants for unclear reasons (Fig. 1 and Supplementary Material S3). Each answered question was included in the analysis.
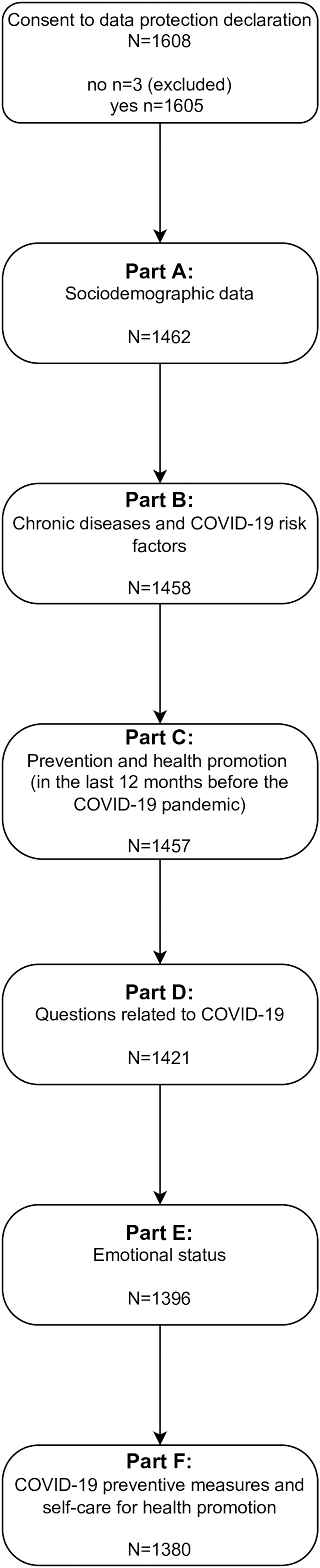
Number of responses per questionnaire part.
Participants were mainly female (80.6%; n = 1178) and middle-aged (55.4 ± 12.6 years) and had a high level of education. More than two-thirds (69.1%; n = 1009) had a higher education entrance qualification (“Abitur”). A total of 43.9% (n = 640) of the respondents had a university degree. One-fifth (20.2%; n = 294) had completed an apprenticeship. Most frequently, participants had employee status (38.5%; n = 561). A quarter were self-employed (28.4%; n = 415), and another quarter (25.1%; n = 366) had already retired. Approximately one-third (31.5%; n = 301) were working from home during the pandemic. A fifth (20.4%; n = 296) reported responsibility for full-day childcare at home, and a fifth (21.0%; n = 306) reported living alone.
There were differences in the size and characteristics of the subgroups.
Males more often reported CM association memberships (58.5%; n = 162) than females (50.1%, n = 590). The number of CM association memberships increased with age, from 17.9% (n = 7) among 18- to 30-year olds to 82.6% (n = 142) among >70-year olds. More than half of the participants (52.7%, n = 784) reported membership in at least one CM association.
Participants with a “negative emotional status” were less likely to have a membership (39.5%, n = 30) than participants with a “positive emotional status” (59.4%, n = 314) (Table 1).
Sociodemographic Data and Membership in a Complementary Medicine Association
Figures report n and % (if not specified).
CM, complementary medicine; SD, standard deviation.
Chronic diseases and risk factors for a severe course of COVID-19
Approximately one-third of the respondents declared that they suffered from chronic diseases (34.6%; n = 504). More than a quarter answered affirmatively to having COVID-19 risk factors for a severe course. Hypertension, immunodeficiency, and chronic lung conditions were most frequently indicated.
More females than males reported the presence of chronic diseases, but, aside from that, females reported fewer risk factors than males. The prevalence of chronic diseases and risk factors increased with age, but decreased with a “positive emotional status.” Even when people with a “positive emotional status” had an older mean age, this group reported fewer chronic diseases and fewer risk factors than people with a “negative emotional status.” More than half of the participants with a “negative emotional status” reported the presence of a chronic disease, which was +23.5% (in relative numbers) greater than that reported by participants with a “positive emotional status” (Table 2).
Presence of Chronic Diseases and COVID-19 Risk Factors for a Severe Course of COVID-19
Figures report n and %.
Most participants (75.9%; n = 1047) reported making use of NPIs. Most of the NPI users reported practicing of handwashing (96.7%; n = 1012), facemasks (88.3%; n = 925), cough and sneeze etiquette (85.8%; n = 898), and physical distancing (84.5%; n = 885). A majority reduced direct social contacts (71.5%; n = 749) and used hand disinfectant (68.5%; n = 717).
Use of self-care methods before and during the COVID-19 pandemic
In the 12 months before the pandemic, 98.4% of the respondents made use of general health-promoting and prevention strategies such as physical activity, healthy nutrition, or relaxation techniques. A total of 87.0% made use of these prevention strategies at least once a week, and 36.5% made use of them daily. The proportion of daily users was highest among the subgroups with “positive emotional status,” “age 51–70 years,” and “female” (Supplementary Material S4).
In the last 12 months before the pandemic, 85.9% made use of specific methods from the field of CM at least rarely. Three-quarters of the respondents were using it at least sometimes, and approximately half of the respondents were using CM regularly. A total of 14.1% did not use CM. The highest percentage of regular users was found among the subgroups “negative emotional status,” “female,” and “age 51–70 years.” The highest rate of nonusers was among the subgroups “age 18–30 years,” “male,” and “>70 years” (Supplementary Material S4).
During the pandemic, 86.8% of the participants made use of self-care methods for health promotion, especially with the goal of strengthening their health. Self-care users favored staying in nature, healthy nutrition, and physical activity. The listed self-care methods were mainly rated as successful measures for health promotion and illness prevention. The proportion of self-care users who rated the health-promoting effect of the method as medium or strong ranged from 54.3% (n = 188) for Ayurveda to 97.6% (n = 1152) for healthy nutrition (Fig. 2).
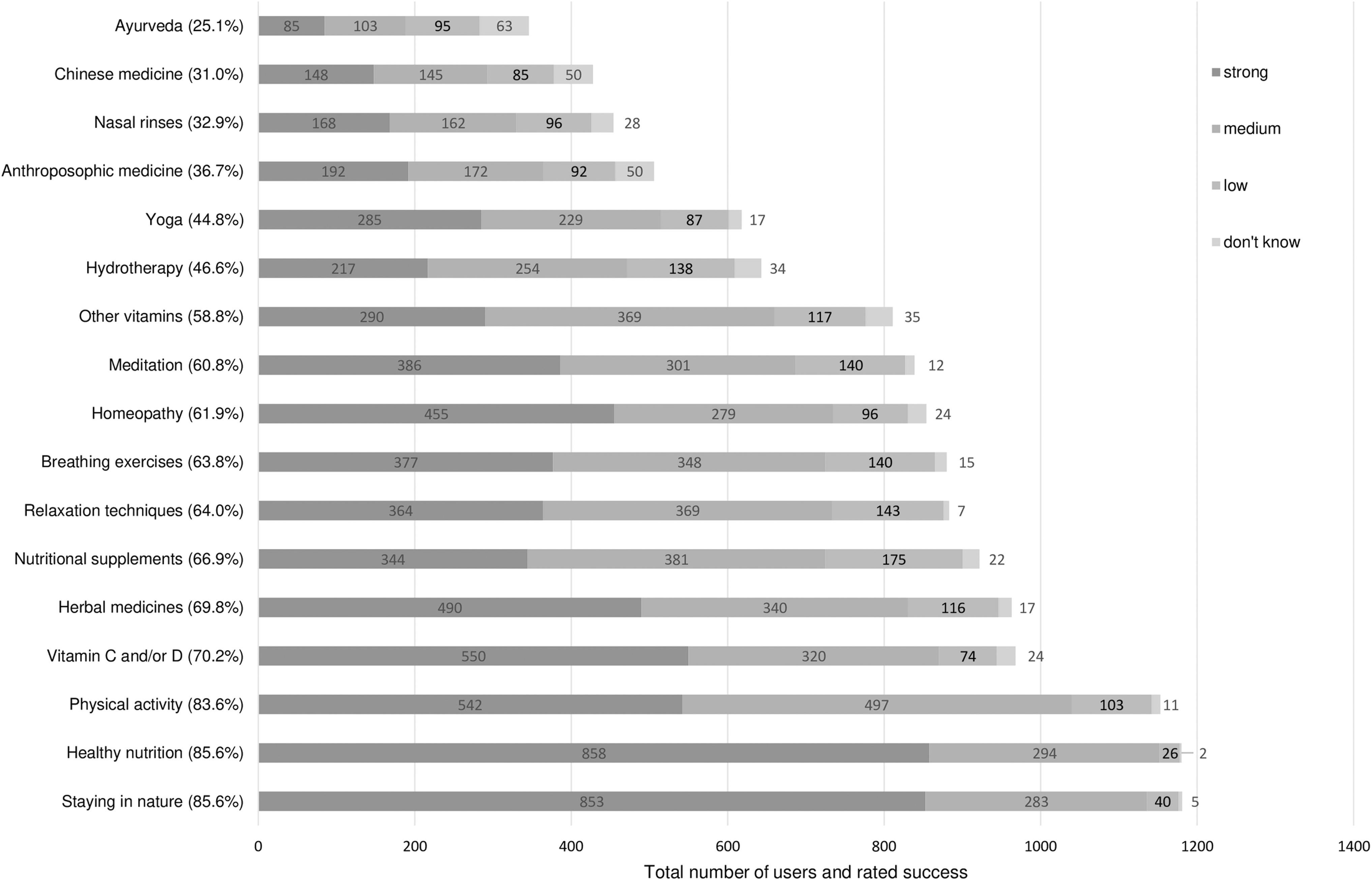
Use of self-care methods and rated success. Percentages in parentheses present the proportion of the users compared with all respondents.
Every listed method was used more often by females than by males, especially yoga (+16.1%) and homeopathy (+14.7%). There were some differences noted in the use of self-care methods during the pandemic when comparing the emotional status and the sex of participants. On the one hand, 86.7% of the respondents from each of the categories “positive emotional status” and “negative emotional status” made use of health-promoting methods during the pandemic. On the other hand, a relatively greater proportion of participants with a “positive emotional status” made use of relaxation techniques (+10.8%) and yoga (+14.3%), whereas participants with a “negative emotional status” more often used CM methods such as nutrition/supplements (vitamin C and/or D + 11.4%; other vitamins +17.9%; nutritional supplement +14.4%) and Anthroposophic medicine (+11.9%) (Supplementary Material S5).
A quarter of the participants (25.7%; n = 413) used the free text boxes to describe the self-care methods they used for health promotion during the pandemic. In particular, qigong and aromatherapy were mentioned frequently (Fig. 3).

Treemap chart of self-care methods for health promotion during the COVID-19 pandemic. Methods were listed when there were n ≥ 5 mentions in the free text boxes of the survey instrument. Sorted by major topic (large font). Only absolute numbers are reported.
Impacted by COVID-19
Approximately 10% (n = 147) of the respondents reported having had contact with people with COVID-19, and 8.5% (n = 121) had lost a personal acquaintance who had died from COVID-19. Only 16 participants (1.2%) reported having had a SARS-CoV-2 infection themselves. They mainly described mild (n = 8) or moderate (n = 6) symptom severity. One person reported severe symptoms, and another person reported no symptoms. Ten of the respondents did not need treatment for their SARS-CoV-2 infection, five were treated as outpatients, and one was treated as an inpatient. The number of days of sickness ranged from 0 to 30.
Fourteen of the individuals with COVID-19 used the listed methods of self-care or prescribed treatment during the course of their illness, especially healthy nutrition (n = 12), staying in nature (n = 11), vitamin C and/or D (n = 11), other vitamins (n = 8), nutritional supplements (n = 8), herbal medicines (n = 8), physical activity (n = 8), and breathing exercises (n = 8). They made use of homeopathy (n = 7), hydrotherapy (n = 6), meditation (n = 6), relaxation techniques (n = 5), yoga (n = 3), nasal rinses (n = 2), Anthroposophic medicine (n = 1), Ayurveda (n = 1), and Chinese Medicine (n = 1).
They named other measures used in free text boxes, which are frequently used in respiratory tract infections in Germany (Angocin®, containing nasturtium and horseradish, essential oils, preparations from Cistus [English: rockrose], zinc, Sinupret®, containing cowslip, gentian, sorrel, elderberry, and verbena, rest/calm, sleep, fresh fruit). In addition, O2/O3 or alkaline or multivitamin infusion, green tea, and grapefruit seed extract were used.
Emotional status during the pandemic
Most respondents reported low values for feeling lonely (mean ± SD: 2.6 ± 2.9), anxious (2.8 ± 2.6), or sad (3.3 ± 2.8), representing a low manifestation of negative emotions. The highest means were reached for feeling connected to others (6.2 ± 2.5) and well-being (5.8 ± 2.4). Boxplots with IQRs and medians are presented in Figure 4, and means and SDs are presented in Supplementary Material S6.
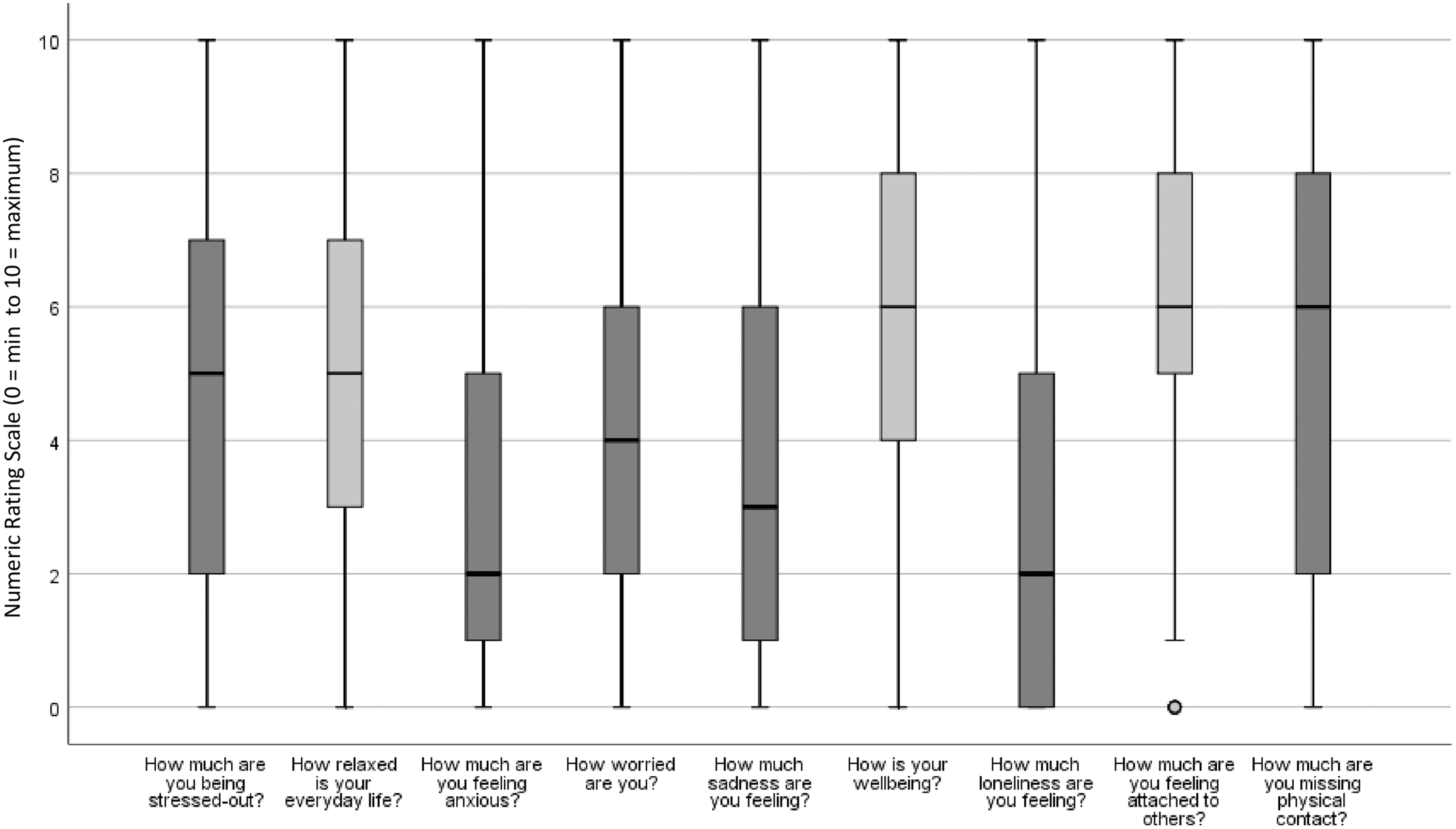
Intensity of different aspects of emotional status on an NRS. Boxplots report medians (black bold line) and quartiles of results from an NRS ranging from 0 to 10 points (0 = minimum to 10 = maximum). Dark grey: rather negative emotions, Light grey: rather positive emotions. NRS, numerical rating scale.
None of the 1393 respondents stated that he or she had intensified social contacts; nevertheless, the values for feeling connected to others were high. Half of the 1011 working participants (56.3%; n = 574) had no worries about their professional lives, while 14.7% (n = 149) were worrying a lot.
Based on the emotional status responses, 37.9% (n = 529) of the respondents were allocated to the subgroup “positive emotional status” and 5.4% (n = 76) to the subgroup “negative emotional status” for further analysis of their characteristics.
The following differences in sex and age groups were observed: male respondents showed slightly lower levels, on average, for all negative emotions than females showed. People younger than 51 years stated that they were more stressed out (18–30 years: 5.1 ± 2.8; 31–50 years: 5.4 ± 2.6) than elderly people (51–70 years: 4.6 ± 2.8; >70 years 2.9 ± 2.4). Participants older than 70 years showed the lowest levels for all negative emotions and the highest for all positive emotions in the questionnaire (Supplementary Material S6).
Discussion
To the authors' knowledge, this study is the first to investigate self-care methods and strategies used during the COVID-19 pandemic among persons with a preference for CM in Germany. Respondents were mainly female and middle-aged and had higher levels of education. More than one in four persons indicated having risk factors for developing a severe course of COVID-19. The use of health-promoting and CM methods among the study population had already been high before the pandemic and remained high during the pandemic. Respondents used a broad variety of self-care methods in addition to generally recommended NPIs. A combination of measures was used, including self-characterized healthy nutrition, physical activity, and staying in nature; these were favored as strategies for health promotion and were mainly rated as having a medium to strong effect. Only 16 participants reported having had COVID-19. On average, negative emotions were not very pronounced, especially feeling lonely, anxious, or sad.
Strengths and limitations of the study
To the best of knowledge, this is the largest study on self-care methods among people with CM affinity in Germany, with 1379 respondents who completed the survey. The study captured the start of a second increase in infection rates (“second wave”) of the COVID-19 pandemic in Germany. As the study was performed online, the authors had a wide reach and asked a wide range of questions (e.g., emotional status, free text boxes). The questionnaire was written to be quick to read and easy to understand.
The authors used the NRS to assess the intensity of certain aspects that influenced emotional status during the pandemic. This is rather unusual except in ratings for pain 21 or anxiety. 22 They used this innovative form to increase compliance because the NRS could be answered quickly, spontaneously, and intuitively. Furthermore, the construction of the dichotomous subgroups “positive emotional status” and “negative emotional status” was an attempt to combine and summarize data on emotional aspects and predictors. However, this procedure is not validated so far.
This cross-sectional study can only represent a certain moment of the pandemic. The prevalence rate for COVID-19 was variable over the 4-month-long recruiting period, 23 and this may have had an impact on the internal validity. Because this was an anonymous online survey, the authors could not externally validate the characteristics reported by the participants, and they could not determine if the questionnaire was answered more than once per person.
Taken together, the results of this study must be interpreted carefully and should not be generalized to the German population, as this study population might be different from the general German population.
Comparison with other studies
Sociodemographic characteristics (mainly female, higher education, middle-aged) are in line with other studies exploring the characteristics of CM users 24 –27 in the general population. This study population appears to be healthier and more health-conscious than the general German population, in which 16% (instead of 5.4% of the general population) suffer from obesity and more than 20% (instead of 3.6% of the general population) are smokers. 28,29
In the NL, NOR, and SWE, 2494 subjects from the general population were surveyed on their use of CM self-management strategies during the first 3 months of the pandemic. 12 The use of self-help techniques amounted to 30.3% (NL: 31.7%, NOR: 27.4%, SWE: 33.2%), but only a few people intended to prevent (4.4%) or treat (0.4%) COVID-19 with these techniques. In comparison, 86.8% of the German respondents with a specific connection to CM reported the use of self-care methods for health promotion during the COVID-19 pandemic.
Respondents from the NL, NOR, and SWE favored yoga (11.4%), meditation/mindfulness (11.0%), and relaxation techniques (8.6%) across all countries. Breathing therapy (13.0%) was the method used most often in SWE, but it was not captured in the data from the NL and NOR. In contrast, a greater proportion of these respondents made use of yoga (44.8%), meditation (60.8%), relaxation techniques (64.0%), and breathing exercises (63.8%). Regarding the use of natural remedies, vitamins, minerals, and dietary supplements, a majority (62.8%) of the respondents from the NL, NOR, and SWE made use of these measures, but only 3.4% did so to prevent SARS-CoV-2 infection, and only 0.24% did so to treat COVID-19 infection. Almost half of the respondents (49.9%) used vitamins/minerals. They made use of dietary supplements (29.2%), herbs (18.2%), and homeopathic remedies (4.7%).
Compared with the use rates in the NL, NOR, and SWE, a study of 1222 people from the Republic in Bangladesh in mid-2020 reported a less frequent use of vitamin supplements (27.1%) and mineral supplements (19.9%), but a more frequent use of herbal products (57.6%) and homeopathy, especially the homeopathic drug Arsenicum album (30.4%), to reduce the risk of infection. 30 Lifestyle components such as whole food diet and physical activity seem to influence the risk and severity of COVID-19. 31,32 It is assumed that due to different and restricted social and economic conditions in Bangladesh, NPIs such as social distancing and lockdowns are practically not feasible. 33 Thus, Bangladeshis might have been influenced by the Ministry of Ayurveda, Yoga & Naturopathy, Unani, Siddha, and Homoeopathy from neighboring India that recommended Arsenicum album as a homeopathic remedy along with other CM methods. 30,34
This study population showed a frequent use of vitamin C and/or D (70.2%), other vitamins (58.8%), and nutritional supplements (66.9%). Herbal medicines (69.2%) and homeopathy (61.9%) were used by many respondents. A cohort study among hospitalized COVID-19 patients showed that vitamin D deficiency was associated with a higher risk of a severe course of COVID-19. 35
The mentioned studies differ from this study. In SWE, NOR, and the NL, the study respondents were a population-representative group, and the Bangladesh study aimed to address the general public as well. The assumption that respondents who are in favor of CM report a higher use of self-care strategies than respondents from a sample from the general population was confirmed.
In this study, the membership of a CM association was associated with better mental health and well-being (Table 1). However, due to the cross-sectional study design, the authors could not answer the question if being in such an organization increases the likelihood of mental well-being or if the mentally well are more likely to join these organizations.
A study from the NL, NOR, and SWE found that respondents who used self-management strategies to prevent COVID-19 were more likely to be worried. 12 Respondents to this study with a “positive emotional status” or a “negative emotional status” did not differ regarding the proportion of self-care users (86.7% each), but they differed in the type of self-care methods they used during the pandemic. Participants with a “positive emotional status” used relaxation techniques and yoga more often, and participants with a “negative emotional status” preferred healthy nutrition and supplements and Anthroposophic medicine (Supplementary Material S5). The size and characteristics of the subgroups (e.g., age, retirement, chronic diseases) can be considered factors that influence the results of used self-care methods.
Respondents showed a similar compliance to NPIs compared with a sample from the general German population: in September 2020, 87.6% of the general German population reported wearing a face mask, 89% obeyed rules on coughing hygiene, and 67% reduced social contacts 36 compared with 88.3%, 85.8%, and 71.5% in this study, respectively.
A frequently pursued strategy among respondents in this study seemed to be a combination of NPI use and the use of a variety of self-care methods, mainly physical activity, healthy nutrition, and staying in nature, as a health promotion and prevention strategy.
Several studies highlight a connection between the COVID-19 pandemic and mental health problems such as affective disorders and perceived stress. 6,7,37 –39 Authors of a systematic review of 19 studies in 8 different countries found the prevalence rates of anxiety (6.33%–50.9% in 11 studies), psychological distress (34.43%–38% in 2 studies), and stress (8.1%–81.9% in 4 studies) to be rather high among the general population. 6 The range of prevalences may be explained by different ways of data collection by a broad variety of validated questionnaires.
A meta-analysis that included 17 studies found the prevalence of anxiety to be 31.9% (17 studies) and that of stress to be 29.6% (5 studies) in the general population. 7 Another meta-analysis that included 55 studies found the prevalence of anxiety to be 15.15% (54 studies) and that of psychological distress to be 13.29% (19 studies) in different types of populations. 37 However, the way governments managed COVID-19 and communicated about it varied from country to country and also changed within individual countries during the course of the pandemic. This is likely to have had a significant impact on the public's perception of the pandemic and thus on their responses to it.
Surprisingly, in this study, levels for feeling anxious were rather low, with a median of 2 (NRS 0–10 points). Levels for being stressed out were higher, with a median of 5. It needs to be noted that a quarter of the respondents were in the range from 5 to 10 on the NRS for feeling anxious. A quarter reached 7 to 10 points on the NRS for being stressed out. Males and elderly people showed lower values regarding anxiousness and distress than females and those in younger age groups. These observations have also been made in other studies. Lower stress was associated with male gender, older age, mindfulness, 38,39 social support, and higher levels of education. 38
Mindfulness was not surveyed directly but can be assumed to be higher among this study population than in the general population because it comprises the meditation, breathing exercises, and relaxation techniques that were used by more than 60% of the respondents. Mindfulness, higher education, and higher age are protective factors 38,39 with a higher prevalence in this study population, and it might also be a reason for a generally more balanced emotional status.
Nature stays could also be an important reason for the rather balanced emotional status. A position article on human–nature interaction concepts hypothesized that social connectedness and connectedness to nature are based on the same general psychological mechanisms. 40 The authors summarize that the natural environment can give rise to spiritual feelings of peace or love and increased well-being, while stress-related symptoms are reduced. Most respondents made use of staying in nature and perceived it as an effective measure. Perhaps nature stays are a viable substitute to human contact in periods when physical human-to-human contact needs to be reduced to avoid infections.
Chronic diseases were correlated with more symptoms of anxiety and stress. 6 This can be confirmed by this study. Respondents who were allocated to the “negative emotional status” group reported a greater number of chronic diseases.
Conclusions
Self-care strategies, including generally healthy lifestyle elements such as spending time in nature, healthy nutrition or exercise and herbal medicine, relaxation techniques, breathing exercises, homeopathy, and meditation were practiced frequently in addition to NPIs by the respondents of this study. The sample was predominantly female, middle-aged, and had achieved higher levels of education. Respondents were in a rather good emotional condition at the start of the second COVID-19 wave.
Further research, preferably studies including a control group representative of the general population and using validated instruments, should investigate the use and impact of self-care strategies on the health and emotional status during the pandemic crisis, as their research results may have public health implications for the future.
Footnotes
Acknowledgments
The authors gratefully thank their study secretary Margit Cree for her contribution to the study's administration. Furthermore, they gratefully thank Caroline Geiser from the Kneipp Bund e.V. and Dorothee Schimpf from Natur und Medizin e. V. for supporting them by informing their members about the study in their newsletters and on their associations' websites. The authors also thank Weronica Grabowska for the linguistic check of the figures' text.
Authors' Contributions
M.O., B.B., B.S., G.R., M.T., S.B., and T.T.-D. participated in developing the study design and protocol. Specific tasks and responsibilities: project administration (M.O. and B.B.); methodology (M.O., B.B., G.R., B.S., M.T., and S.B.); data curation (S.B. and L.J.); formal analysis (L.J., S.B., and T.T.-D.); drafting of the article (L.J., M.O., B.B., S.B., and G.R.); visualization (L.J.); supervision (M.O. and B.B.); and funding acquisition (B.B.). All authors read and approved the final article.
Data Availability Statement
The original raw data of this study will be made available on request from the corresponding author. The data are not publicly available due to information that could compromise the privacy of the research participants.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors sincerely thank the investigator (institute for social medicine) and Komitee Forschung Naturmedizin e.V. (KFN) for funding this study.
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
Supplementary Material S4
Supplementary Material S5
Supplementary Material S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.