
Abstract
Introduction:
Multiple sclerosis (MS) is a progressive disease of the central nervous system that can result in highly variable effects on mobility and sensorimotor function. Persons with MS (pwMS) often use complementary and alternative approaches, such as acupuncture, to address these symptoms. However, studies of acupuncture on these symptoms have been hindered by methodologic flaws, which have limited the ability to draw conclusions about its efficacy. The purpose of this study was to examine the feasibility of an acupuncture intervention on a wide range of sensorimotor and mobility measurements in pwMS.
Methods:
Using a randomized crossover design, subjects experienced acupuncture or a no treatment control condition twice weekly for 4 weeks, followed by a 4-week washout period, and then crossed over to the other condition for 4 weeks. Strength, sensation, spasticity, gait, and balance were measured for all subjects, both before and after each condition.
Results:
Seven of the 12 subjects who started the program completed all phases. No subjects experienced adverse effects. No statistically significant changes were observed in the gait or balance measures. Small statistically significant changes were observed in upper extremity strength. Sensation and spasticity were unaffected.
Discussion:
The variability of MS suggests that a wide array of testing procedures be utilized, however, this may have led to difficulty with completing all phases of the study. Acupuncture did not result in changes in mobility in pwMS. Some improvements in upper extremity strength were observed. It is unclear whether these changes represent the effect of acupuncture or the inherent variability of MS.
Introduction
Multiple sclerosis (MS) is a progressive disease of the central nervous system (CNS) that can result in a multifactorial and highly variable impact on physical and cognitive function. Allopathic medical management has greatly improved over the last several years, leading to the slowing of disease progression. However, the lack of effective management of the myriad of impairments and functional limitations that lead to disability continues to have a catastrophic impact on persons suffering from MS. The relative dearth of effective biomedical interventions to address the symptoms of MS has led many people with the disease to examine the use of complementary and alternative medicines as a means of addressing the signs and symptoms that they may feel are not adequately addressed by standard biomedical management. This is evidenced by the fact that persons with MS (pwMS) report a relatively high usage of acupuncture. 1 –3 However, although there is an extensive history of acupuncture usage, there is little bioscience evidence to support its effectiveness in addressing the signs and symptoms of the disease.
A recent review of the literature 4 presented evidence that the few studies that have investigated the use of acupuncture to treat the signs and symptoms of pwMS have been limited by poor study design, limited or absent statistical analysis, and poor description of the sample. The combination of high usage with little supporting evidence creates a problem for health care practitioners who work with pwMS; health care practitioners need to be able to advise their patients appropriately when making clinical decisions using the best available evidence.
Although MS is traditionally thought of as a disease that is caused by CNS demyelination and inflammation, it can also be considered a disease of mobility. Difficulty with aspects of mobility such as walking, balance, transfers, and bed mobility are some of the most common complaints of pwMS. 5 Although allopathic medicine is used to treat the pathology of the disease, mobility issues are customarily treated with rehabilitation such as physical and occupational therapy. Despite the high reported usage of acupuncture in pwMS, few studies have examined its use in terms of mobility.
To our knowledge, the only study examining the use of acupuncture to treat mobility in pwMS was published by Criado et al, 6 who found improvements in 25-foot walk test (25FWT) performance following acupuncture treatment (AT), although other aspects of MS mobility were not examined and the level of severity of the participants was not specified. The mobility deficits in MS are multifactorial and diverse. Limitations in walking or balance in pwMS can be due to limitations in strength, motor control, sensation, flexibility, cognition, and behavior. Given the variable nature of MS, these deficits can occur singly or in various interacting combinations with variations in intensity and duration. Examination of mobility deficits in pwMS must therefore include multiple systems. A comprehensive assessment of multiple aspects of mobility must be conducted to accurately assess the effects of acupuncture on mobility in pwMS.
Given the high reported rate of acupuncture usage by pwMS, in contrast to the limited bioscience evidence for its effectiveness, health care practitioners who educate MS patients regarding their health care choices would benefit from research examining the efficacy of acupuncture in addressing MS deficits. Specific examination of the effects of acupuncture on aspects of mobility rather than disease activity will more accurately address the question of whether acupuncture has an impact on physical function in patients with MS. However, the absence of high-quality evidence limits the ability of clinicians who treat pwMS to make accurate judgments regarding whether acupuncture can be recommended.
Therefore, the purpose of this pilot study was to examine the feasibility of testing the effects of an acupuncture intervention on sensorimotor function and mobility on a sample of patients with MS using a randomized crossover design. It was hypothesized that the acupuncture intervention and the sensorimotor and functional evaluation measures would be well tolerated by the participants and could provide a useful framework for future research. If this hypothesis was correct, it would suggest that this protocol could be used in larger scale efficacy studies to determine if acupuncture is an effective intervention for treating MS. A secondary hypothesis for this study was that the acupuncture intervention will result in an improvement in mobility and sensorimotor function. If this hypothesis was correct, it would further suggest that a larger scale trial is appropriate.
Methods
A randomized crossover design was used in this study (Fig. 1). Participants were recruited through flyers from local MS centers. Potential participants would contact the primary author (H.K.) who would assess their appropriateness for the study through phone interview. Inclusion criteria included definitive diagnosis of MS; Expanded Disability Status Scale (EDSS) of 2.5–6.5, as determined by a neurologist; ability to walk unaided for 6 min with or without an assistive device; and ability to read, understand, and sign an informed consent document. Exclusion criteria included bleeding precautions, trypanophobia (defined as an extreme fear of medical procedures involving injections or hypodermic needles), inability to lie still for 30 min, active cancer, current exacerbation, and history of AT. All participants provided written informed consent, which was approved by the Institutional Review Board of Hunter College, City University of New York.

Consolidated Standards of Reporting Trials (CONSORT) diagram.
Participant characteristics, including age, type of MS as determined by a neurologist, years since diagnosis, EDSS score, and use of assistive devices, were collected. Baseline measurements for gait and balance included the 6-minute walk test (6MWT), 25FWT, and Mini-Balance Evaluation System Test (MBT). The EDSS is the most widely used measurement tool to describe disease progression in patients with MS and to assess the effectiveness of therapeutic interventions in clinical trials. In the 6MWT, subjects were asked to walk at their fastest comfortable pace for 6 continuous minutes, and the total distance covered during this time was recorded. In addition, the distance covered every minute was measured to determine whether the subject maintained a steady pace or slowed over time, which is considered to be a sign of motor fatigability, a common MS finding.
These tests have been found to be reliable and valid for measuring mobility in MS, 7 –9 and are capable of capturing a wide array of mobility attributes. Upper and lower extremity strength testing was performed using a handheld dynamometer (HHD), and sensory testing was performed using a biothesiometer. HHD and biothesiometry were used rather than the more commonly used manual muscle testing and standard sensory testing, as they can deliver more reliable as well as continuous data (as opposed to categorical data). 10,11 Spasticity testing was performed using the modified Ashworth scale (MAS). The sensorimotor and functional testing evaluations were developed and performed by Physical Therapist with more than 15 years of experience, each in working with pwMS.
Following the collection of baseline data, subjects were randomized into the AT and control (C) groups. AT sessions began with 10 min of intake and patient preparation. The acupuncture protocol design, patient assessment, and needle application were performed by a licensed acupuncturist and naturopathic doctor (second author, B.S.-B.) with more than 20 years of clinical, academic, and research experience and a specialization in treating pwMS. The AT protocol comprises two sets of points. The first set consisted of core point selection, used in an MS Standard of Care (SOC). 12 The SOC protocol had 10 fixed needle insertions; Du-20 and Yin Tang were in the midline (1 needle) and the other 4 points LI4, LV3, ST36, and SP6 were bilateral, therefore incorporating 8 point insertions. SOC treatment was based on the Traditional Chinese Medicine (TCM) interpretation of the four phases of MS. 13 Similar groups of points have been used in previously published trials. 14
Several point combinations were common in each of the four phases. Using the SOC resulted in bilateral needling of 6 point combinations. The second set of points was individualized to the patient's needs as determined by the acupuncturist, and depended on the particular presentation of each patient in the session and allowed for variability in the patient presentation. The assessment was performed through the TCM tongue and pulse diagnostics by a licensed acupuncturist and consisted of two to four patient individualized point combinations. The acupuncturist was able to include up to four other individualized points (a total of eight additional needles).
Most subjects had up to 18 needle insertions, with the most common additions being GB34, ST40, Shen Men, and SP9. Depending on the specific indications, needles were inserted between 2 mm and 2.5 cm. The depth of insertion was calculated to prevent injury to the adjacent areas or organs. The needles were “Spring 10” by DBC, 0.20 × 30 mm, single used, and were disposed of in a sharps container.
For the (C) group, subjects lay supine in a darkened room in the acupuncturist's office and experienced the exact conditions than the AT group received, except for the AT itself. In other words, subjects during the control condition did not undergo acupuncture. Subjects were made aware that this was the control condition. All participants were asked to hold all medications and exercise regimens constant during the study period. The authors chose not to perform sham acupuncture in the control sessions because the use of sham acupuncture using “fake points” or sham needles has been found to have an effect as well, referred to as the needle effect. 14
After 4 weeks, the groups were crossed over, with the initial treatment group undergoing a 4-week detraining period to minimize any effects of the acupuncture, as well as learning effects from the mobility testing, to be followed by a 4-week period where they received the same experience as the control group. The initial control group also underwent a 4-week washout period before experiencing the 4-week AT.
Mobility and sensorimotor measurements were taken immediately before the first AT or C session and once a week immediately following every two sessions. The evaluators were blinded to the group allocation, and follow-up sessions were performed weekly for 4 weeks after the final acupuncture or control session to assess the long-term effect of treatment. Follow-up retention, as well as all other planning and organizational factors, was administered by the clinical study coordinator.
Data analysis
Statistical analyses were performed using SPSS (version 24). The authors used generalized estimating equations (GEEs) to analyze the effect of the condition (pretest, control, acupuncture, and post-test sessions) on all outcome measures. They chose a GEE approach rather than an analysis of variance because participants contributed to different numbers of observations and a GEE can account for the unbalanced data set. Based on the goodness-of-fit statistics (QIC), the authors chose an identity link function and exchangeable covariance structure to best fit this model. They performed follow-up paired t tests if the overall Wald test was significant, and used the Sidak method to control for multiple comparisons.
Results
Table 1 lists the conditions for each participant. All 12 participants contributed to the baseline measurements, but only 8 contributed to both the control treatment (CT) and AT conditions. Of the five subjects who did not complete both conditions, none experienced any adverse reactions to AT. Seven of the eight participants who underwent both treatments were measured again during the follow-up session. All missing sessions occurred because of scheduling difficulties associated with the institution where the study was performed.
Subject Characteristics and Conditions Contributed by Each Participant
EDSS, Expanded Disability Status Scale; PP, primary progressive; RR, relapsing remitting; SP, secondary progressive.
As shown in Table 2, the GEEs showed significant differences among conditions for spasticity (MAS of right hip flexors), sensory testing (biothesiometry of the big toe pulp, right plantar metatarsal phalanx, right medial and lateral malleolus, and left side of C5), strength scores (HHD of left hip flexion, left knee flexion, right knee flexion, right elbow flexion, right elbow extension, right wrist flexion, left wrist extension, and right wrist extension), and balance scores (anticipatory and sensory orientation domains of the MBT), Wald χ 2 s ≥ 8.93, ps ≤ 0.03. The highlighted rows in Table 2 indicate the outcome measures with significant differences among pairwise comparisons. Although scores after AT were not significantly different from pretest scores, AT outperformed CT in HHD scores (left hip flexion, right elbow flexion, right wrist flexion, and right wrist extension) and biothesiometry scores (right lateral malleolus; ps ≤ 0.025).
Wald Tests for All Outcome Measures. Means, and Standard Deviations for Scores During Pre- and Post-Tests, and for Average Scores After Control Treatment and Acupuncture Treatment
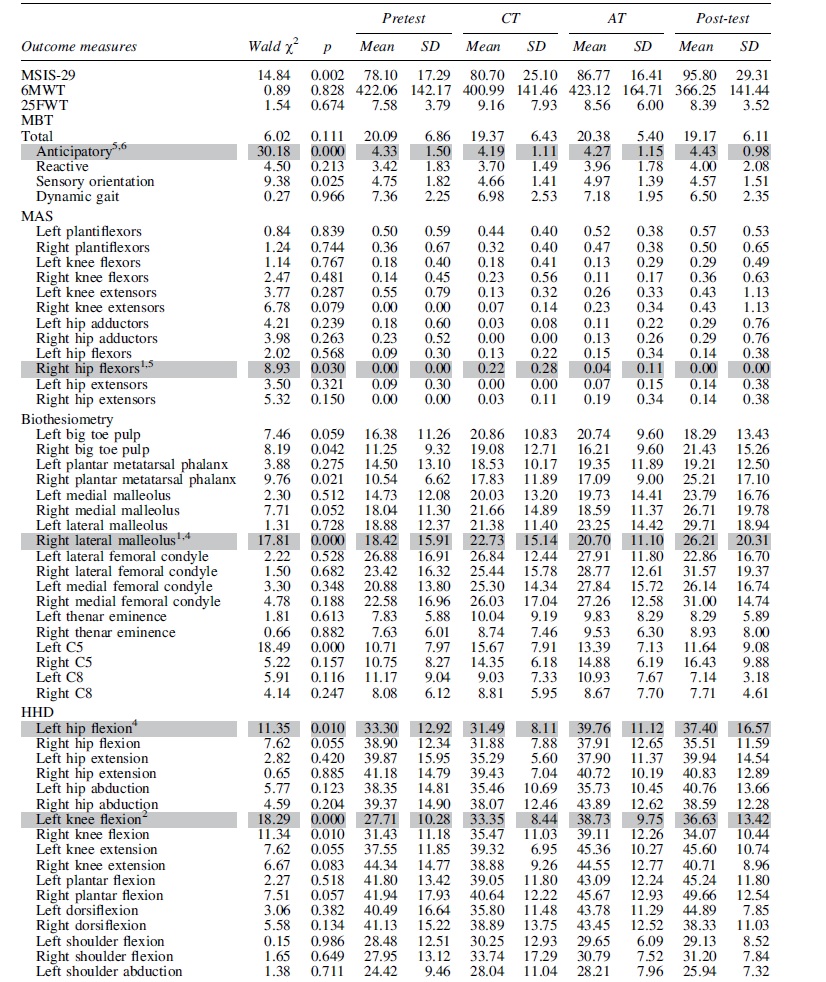

The HDD score for left knee flexion was better after AT than during the pretest (p = 0.004), but differences between AT and CT did not reach significance. The scores of the anticipatory domain of the MBT were slightly worse after CT and AT than during the post-test (ps ≤ 0.014). All other significant pairwise comparisons were among the CT, pre-, and post-tests, ps ≤ 0.048.
Discussion
In this study, the authors investigated the use of a protocol and its feasibility for performing an acupuncture intervention on specific aspects of mobility and sensorimotor function in pwMS. They performed this study because of the relatively high use of acupuncture in pwMS and the lack of evidence supporting its use. Previous studies of MS and acupuncture have been limited by numerous methodological issues, and so, a primary goal was to investigate a protocol for both acupuncture intervention and sensorimotor and mobility outcome measures in the MS population. It was hoped by presenting evidence of the utility and feasibility of a protocol such as this that future research could conduct the larger scale projects needed to accurately assess the efficacy of acupuncture in addressing MS signs and symptoms.
Cramer 15 suggested several areas of assessing feasibility that apply to this study. Recruitment of a sufficient number of patients and the patients' willingness to be randomized are important indices of study feasibility. In this study, the authors were obligated to cease recruitment due to COVID restrictions thereby limiting the number of participants. This was somewhat mitigated by the choice of using a crossover design so that all participants in the study received both the experimental and control conditions. The crossover design also limited any dissatisfaction that participants might have felt from being randomized into a nonintervention group. Although not all subjects completed the entire protocol, none of the subjects dropped out due to complications related to the intervention itself. The dropouts primarily occurred for three reasons: personal issues (death in family), unrelated MS exacerbation, and unrelated medical complications.
It is possible that the length of the protocol may have contributed to the dropout rate as a shorter protocol would have less time for complications to occur. MS is well known to be a progressive and variable condition, and therefore, the longer the length of the protocol the greater the risk for complications to occur. However, a shorter protocol may not have been sufficient to detect meaningful clinical changes. The sensorimotor and mobility assessments were performed weekly and lasted approximately an hour each. Although none of the participants claimed that he or she found the assessments difficult, future studies might consider a reduced frequency of assessments.
Because MS can affect individuals in an extremely diverse and individual manner, the authors used a relatively large number of outcome measures with the goal of capturing as wide an array as possible of clinical change. Although this may have added to the overall time and energy commitments experienced by the participants, they felt that this was necessary to provide proper attention to the heterogeneity of the population. MS lesions can potentially present at any time and location in the CNS and this underscores a principal issue with studying the effects of interventions; patients can be at similar levels of disability but this can be due to involvements of different areas of the CNS. Therefore, it is important that investigators “cast a wide net” to have sufficient sensitivity to clinical change.
In this study, the authors considered acupuncture as a modality as opposed to a technique as by utilizing highly experienced acupuncturists with extensive experience in MS as opposed to a PT who has experience in “needling techniques.” Acupuncture represents a practice with thousands of years of history treating an extremely wide range of conditions. Using skilled and experienced acupuncturists ensured that the intervention provided to these subjects was authentic. The acupuncture that was provided was individualized through the use of 10 questions, tongue and pulse diagnosis, and objective observation. The “Ten Questions” refers to a series of questions utilized by a Chinese medicine practitioner to establish a TCM differential diagnosis. 16 During the interview the practitioner will ask about the following: hot, cold and fever, chills; sweat; head and face; pain; urine, stool; thirst, appetite, taste; sleep; thorax, abdomen; gynecological/male and medical history.
This information will be interpreted and translated into a Chinese diagnosis pattern using the eight principles (yin/yang, hot/cold, internal/external, and excess/deficient). The eight principles provide a framework to interpret the answers to the 10 questions and the practitioner's objective observations during the tongue and pulse diagnosis. This analysis provides a way to describe the patient's pathology in TCM terms to design an appropriate and unique protocol.
The authors supported their individualized treatments with four fixed points that are used in most MS treatments. In most cases, the TCM diagnostics would have warranted using those same points as well. According to Matos et al, 17 TCM is defined as “a systematic healthcare system developed from clinical experience based on a scientific model of regulation.” TCM relies on unique theories and practices to treat diseases and enhance health. The practices of TCM include Chinese herbal, dietetics, acupuncture, moxibustion, manual therapy (Tuina), and exercises, such as qigong and “Taijiquan.”
In this study, the authors utilized both an SOC approach and individualized treatment as they felt that this best represented acupuncture that would be delivered to address the unique and specific needs of pwMS. The authors individualized part of the treatment utilizing TCM diagnostic patterns. To generate what is called Eight Principles Syndrome Differentiation, they utilized a tongue and pulse diagnosis, and looked at the patient's complexion, movement, and speech. The authors also inquired about past history and present symptoms. The individualized point selection part of the treatment in this study came from all these diagnostic evaluations as a whole. From the perspective of TCM practitioners, both syndromes and diseases should be diagnosed upon the patients' symptoms and signs.
While TCM has many ways of identifying illness, its eight principles, abstracted from the individual characteristics of specific syndromes, provide a guideline check for (1) exterior and interior syndromes, (2) cold and heat syndromes, (3) deficiency and (4) excess syndromes, and yin and yang syndromes. During the diagnosis, different patterns of differentiation were seen in the participating subjects. The differentiation patterns were highly varied and the authors therefore did not analyze the frequency of each of the presenting differentials. They did observe many a preponderance of Kidney Yin/Qi deficiency presenting subjects and several Spleen Q deficient individuals leading to damp accumulation.
Although the small size of this study limited the ability to draw useful information regarding effectiveness, the authors hypothesized that persons who received acupuncture would demonstrate significant improvements in these outcome measures compared with the control condition. The data collected and analyzed in this study did not support this hypothesis. Although there were a few isolated areas where the data reflected significant improvements following AT, it is difficult to make the case that such improvements are evidence that the treatment was causative, and may instead have represented some of the normal variability that occurs in MS.
The greatest amount of change occurred during strength testing. To measure changes in strength, the authors used handheld dynamometry as it results in more objective data points than the more commonly used manual muscle test. Thirteen separate movements were tested on each side, for a total of 26 measurements. Significant improvements following the use of acupuncture occurred in 5 of the 26 measurements (left hip and knee flexion, right elbow flexion, right wrist flexion, and extension). Whether these improvements were due to acupuncture or normal MS variability is not known, although it is noteworthy that significant improvements also occurred for left wrist extension and right elbow flexion in the control group.
Spasticity was assessed using the modified Ashworth Scale. Twelve different lower extremity areas were tested on the left and right sides for a total of 24 measurement areas. A significant difference was found for the control condition of the right hip flexors. AT had no significant effect on spasticity. It is possible that the relatively mild nature of MS in this subject pool (EDSS 3.5) resulted in mild, if any, spasticity. More severely impaired patients exhibiting greater spasticity might have had different findings.
Biothesiometry testing of the patients' vibratory thresholds was performed at nine discrete points on the left and right sides of the body. The only area that showed a significant improvement with AT relative to the control was the right lateral malleolus. Although biothesiometry attempts to limit some of the subjective nature of sensory testing using ratio levels of measurement, the perception of vibratory stimulation is still a subjective phenomenon, and as a result, these outcomes may not accurately reflect changes in sensory function. No significant changes were observed in gait, balance, or quality of life.
The relative absence of clinical changes following AT when compared with control patients does not necessarily suggest that pwMS or the clinicians who treat them should exercise caution regarding the use of AT. The acupuncture protocol that the authors used was specifically developed for use with pwMS and administered by trained practitioners with many years of experience working with pwMS. However, the relatively modest gains that were observed cannot be considered evidence supporting its use in this population and may represent the variability that is common in this disease. Further evidence of the changes being due to variability rather than the AT is the fact that there were several instances where significant improvement was seen in the control group, but not in the acupuncture group. Day-to-day and even within-day variability is a hallmark of MS, 18,19 and therefore makes single measurements unreliable indicators of the patients' true status.
The authors tried to address this by having multiple points of measurement over time, but due to the small sample size, they still cannot rule out that the changes that they saw were due to variability as opposed to treatment effects. Future studies should consider including assessing for this characteristic when taking the subjects' history.
Another topic in this protocol to be considered was the length of the acupuncture intervention; MS is a chronic disease that these subjects had experienced for many years. It may be that the “dosage” of the acupuncture may not have been sufficient to produce a detectable change. However, the authors chose the shorter period due to the fact that MS is also known to be a progressive disease and therefore longer intervention periods run the risk of subjects encountering an exacerbation during the course of the experiment, thereby obscuring any treatment effects.
The overarching purpose of this study was to examine the feasibility of a specific protocol for studying the effects of acupuncture on mobility in pwMS. To perform studies that can accurately ascertain the effectiveness of acupuncture on MS mobility, a specific protocol needs to be enacted. Although the authors utilized a protocol that they felt effectively captured the heterogeneity that is the hallmark of MS, this study had many limitations that should be seriously considered in future investigations. This sample size was quite small, and with a larger sample size, greater evidence for the statistical significance of acupuncture may have been found. Similarly, this sample was predominantly composed of individuals with relatively mild disabilities. It may be that pwMS with moderate or severe disability may have responded differently than in this sample.
Although this study did not find that acupuncture resulted in changes in mobility or sensorimotor function, the authors cannot rule out the possibility that acupuncture resulted in changes that were not captured by the tests that they used. The authors used a comprehensive battery of physical therapy measures to capture the impact of acupuncture, but did not use self-report/qualitative measures. Many of the subjects stated that after AT, they felt stronger, more energized, and more motivated. Although the placebo effect cannot be ruled out, it may also be the case that these subjective self-reports may reflect actual changes that these tests were not sensitive enough to capture. Alternatively, it may be the case that the effects of acupuncture were relatively short-lived and the positive effects of the treatment may have dissipated before measurement had occurred.
The use of self-report measures, both immediately after the AT and during regular testing periods, may have added useful data, and future studies should consider their use.
In this study, the use of a “no acupuncture” control condition as opposed to a “sham acupuncture” control condition was carefully considered. The authors chose to use the former because of the evidence presented in the acupuncture Effective Guidelines, 20 a Cochrane systematic review, 21 and a meta-analysis of the control group influence, 22 suggesting that it is not always preferable to use sham needle interventions in controlled trials. Depending on the “n” and the question asked, sham needles, either penetrating or nonpenetrating, may lead to a placebo effect and diminish the effect size. Although acupuncture in general has been proven superior to all categories of control groups, trials that use sham-penetrating needles have a smaller effect size than trials with nonsham controls. 23
The authors therefore chose the control group methodology that was driven by the question “is acupuncture superior to no acupuncture in improving mobility and sensorimotor function in pwMS?” It is possible that the authors used sham acupuncture and double-blinding, which may have resulted in different results. However, given that the protocol used resulted in a very small number of significant differences between groups, it seems unlikely that larger effect sizes between conditions would have been found.
Conclusion
In this pilot study, acupuncture did not lead to improvements in mobility, sensorimotor function, or quality of life in pwMS when compared with a no-treatment control. Future studies should consider larger sample sizes as well as other possible outcome measures, as the impact of acupuncture may not have been accurately detected by the tools used in this study.
Footnotes
Authors' Contributions
H.K. and B.S.-B. conceived and planned the project. H.K., B.S.-B., and Z.L. conducted the experiments. H.K., J.R., and B.S.-B. were responsible for writing the article. J.R. performed all the statistical analyses. S.W. was responsible for the project management. All authors discussed the results and contributed to the final article.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This project was partially funded by a National Multiple Sclerosis Society Pilot Research Grant (Grant No. PP1807-32188).