
Abstract
Introduction:
Active duty (AD) women suffer with chronic pelvic pain (CPP) while providers tackle diagnoses and treatments to keep them functional without contributing to the opioid epidemic. The purpose of this randomized trial was to determine the effectiveness of noninvasive, self-explanatory mindfulness-based stress reduction (MBSR) or self-paced healthy lifestyle (HL) interventions on CPP in AD women.
Methods:
A 6-week, interventional prospective study with AD women aged 21–55 years at Mountain Home (MTHM), Idaho, was conducted. Women were randomly assigned to MBSR (N = 21) or HL (N = 20) interventions. The primary outcome was pain perception. The secondary outcomes were depression and circulating cytokine levels.
Results:
Women in the MBSR group exhibited reduced pain interference (p < 0.01) and depression (p < 0.05) alongside decreased interleukin (IL)-4 (p < 0.05), IL-6 (p < 0.05), eotaxin (p < 0.05), monocyte chemoattractant protein-1 (p = 0.06), and interleukin-1 receptor antagonist (IL-1ra) (p < 0.01) and increased vascular endothelial growth factor (p < 0.05). Women in the HL group did not have changes in pain; however, they did exhibit reduced depression (p < 0.05) alongside decreased granulocyte–macrophage colony-stimulating factor (p < 0.05) and increased tumor necrosis factor alpha (p < 0.05), stromal cell-derived factor-1 (p < 0.01), and IL-1ra (p < 0.01).
Conclusions:
AD women receiving MBSR or HL had reduced depression scores and altered circulating cytokine levels; however, only those receiving MBSR had reduced pain perception. Findings support MBSR as an effective and viable behavioral treatment for AD women suffering from CPP and provide premise for larger randomized controlled studies.
Clinical Trial Registration:
MOCHI—An RCT of mindfulness as a treatment for CPP in AD Women NCT04104542 (September 26, 2019).
Introduction
Chronic pelvic pain (CPP) is defined as noncyclic pain in the lower abdomen, back, or buttocks, which is severe enough to require medical attention and is present for at least 6 months without successful treatment and expected to be lifelong. 1 CPP is associated with a variety of gynecologic (e.g., endometriosis), gastrointestinal (e.g., irritable bowel syndrome), urological (e.g., interstitial cystitis), musculoskeletal (e.g., pelvic floor dysfunction), and body-wide (e.g., fibromyalgia) conditions that may have unique or common etiologies. CPP is common, affecting 15% of the U.S. population 2 and negatively impact women's quality of life (QOL), including physical functioning, psychological well-being, and interpersonal relationships. 2 Additionally, CPP is often elusive and difficult for providers to diagnose. 2,3 Up to 55% of women continue to experience pain without obvious pathology even after surgical interventions. 4 These women become frustrated with persistent symptoms and lack of improvement. 3,5
As of July 2017, 15% of U.S. military are women. 6 These active duty (AD) women became combat deployable in 2016 after the U.S. military officially lifted the ban on female soldiers serving in combat roles. 7 While CPP in AD women has rarely been studied, one retrospective chart review of 1,737 deployed AD women reported 14% of female soldiers were seen for poorly managed CPP during Operation Iraqi Freedom and Operation Enduring Freedom. 8 Compared with civilians, AD women are at greater risk for hysterectomy for their CPP, and for hysterectomy at an earlier age (35 years vs. 43 years, p < 0.0001). 9
Female veterans disproportionately suffer from CPP at an estimated prevalence of 30% and are more likely than male veterans to receive opioids for this pain. 10,11 This is concerning with the epidemic of opioid use disorders affecting an estimated 2 million Americans, and this rate is increasing across all populations (SAMHSA, 2019). 12,13 Generally, women with CPP report a 45% rate of reduced productivity, 14 a deficit detrimental in a combat zone. The Veteran Administration screens veterans for military sexual trauma (MST), and national data from their program reveal one in four women respond affirmatively to history of MST, which can contribute to CPP and mental health conditions such as depression, anxiety, or post traumatic stress disorder (cck-law.com/blog/military-sexual-trauma-mst-statistics).
Due to comorbidities associated with pain syndromes and mental health illness, it is recommended to screen for psychiatric disorders in any female veteran with unexplained pain. 15 The American College of Obstetricians and Gynecologists (ACOG) considered awareness of female veterans' unique health care needs as essential to practice nationwide. 16 It is imperative that the authors identify treatment approaches that are safe and effective for AD women with CPP.
The U.S. Veterans Health Administration (VA) supports a biopsychosocial model assuming that pain is influenced by a variety of different physical, pathological, psychological, social, and environmental factors. 15 Female veterans with CPP screened positive for comorbid mood disorders at a rate of 31%, had lower healthy physical functioning scores, more medical symptoms, and higher numbers of sick days at the VA. 15,17 A large body of work suggests a role for proinflammatory cytokines in the pathophysiology of CPP, 18 –22 perceived stress, 23 and mood disorders 24 that often accompany CPP.
Alternative nonpharmacological treatments such as mindfulness-based stress reduction (MBSR) or healthy lifestyle (HL) modifications including nutrition and exercise have been shown to reduce proinflammatory cytokine levels 22,23 and are recommended for CPP. 24 These treatments can lead to positive reappraisal, decrease biological stress pathways, and lower nociceptive excitability, thus breaking the self-sustaining cycle of pain and neurogenic inflammation. 25 MBSR, a complementary treatment with an emphasis on cultivating a focused, contemplative self-awareness, can help patients obtain self-regulation for health improvement in positive reappraisal coping. 26
The classic in-person MBSR class includes a live interactive group session where individuals learn from each other and support each other's learning in addition to the homework sessions and journaling but is not always feasible. However, these interventions have yet to be studied in the context of CPP in AD women. Thus, the purpose of the present pilot study was to investigate the putative beneficial effects of noninvasive MBSR and HL interventions, found online for ease of access during deployments with AD women with CPP, on pain perception, depression, and circulating cytokine levels.
Materials and Methods
This interventional prospective study was approved by the University of Missouri-Kansas City Institutional Review Board, the TriService Nursing Research Program Human Research Protection Office (HRPO), and the Wilford Hall HRPO office. All research was performed in accordance with relevant guidelines and regulations provided by these governing bodies, and informed consent was obtained from all participants. Records of participant participation followed regulatory guidance including Federal Privacy Act, 5 USC 522a and its implementing regulations, the Health Insurance Portability and Accountability Act of 1996(HIPAA), and 45 code of federal regulations Parts 160 and 164.
Additionally, all regulatory criteria met an additional ethics review at the Mountain Home (MTHM) Air Force Base (AFB) to assure that proper protocol was adhered to with minimal concern for coercion. This study was registered with the grant in
Participants were recruited from outpatient clinics in an United States Air Force (USAF) military treatment facility (MTF) at MTHM AFB, Idaho. The MTF at MTHM has family practice, mental health, and women's health specialists who were able to assist with recruitment.
AD women with CPP, pain in the lower abdomen/back for greater than 6 months, were recruited through the Wilford Hall HRPO and the TriService Nursing Research Program HRPO at MTHM from June to August 2019 after assuring for participant protection. After referral of the prospective participant with inclusive CPP diagnosis confirmed, a preliminary eligibility assessment of interested participants was conducted via a telephone interview. A positive response to any of the following criteria in the initial interview led to exclusion: (1) age <21 years or age >50 years; (2) menopausal, pregnant, or breastfeeding; (3) pelvic/abdominal surgery within 6 months; (4) vaginal/pelvic infection at time of enrollment (as potential confounder of cytokines drawn), underlying diseases (cancer, diabetes, autoimmune); (5) unavailable to commit 3 months to study; and (6) no access to computer or inability to get online.
Initially, the list of participants came from the group practice managers and local women's health and family practice providers who agreed to help with recruitment of women with specific ICD-10 codes for general CPP or more specific CPP conditions, including irritable bowel syndrome, bladder pain syndrome, vestibulodynia, low-back pain, from their practice. A few women self-identified directly from flyers and a poster used for recruitment, and all participants approved the primary investigator access to record review to confirm a history of diagnosis meeting criteria.
Once consent was signed and diagnosis confirmed, participants were asked to complete valid and reliable questionnaires, including a demographics questionnaire, a pain questionnaire (the Brief Pain Inventory [BPI]), a depression questionnaire (the Patient Health Questionnaire [PHQ]-9), and a mindfulness questionnaire (the Five Facets of Mindfulness Questionnaire [FFMQ]), sent through the Research Electronic Data Capture (REDCap). These data were collected at baseline before beginning either intervention and again at 6 weeks postintervention. Through REDCap, data were managed securely with an infrastructure programming allowing for the blinded assignment of these AD women with CPP to either the MBSR or the HL interventions. Once assigned, only the primary investigator (PI) had oversight to manage the database.
For this study, MBSR online-training consisted of classic journal and written guidance with YouTube videos found on
The HL group had access to weekly voice-over slides that guided them in nutrition and exercise choices with a different focus each week (Supplementary Appendix SA). It was modeled after the Group Lifestyle Balance course found at USAF bases used by Nutritional Medicine to work with patients with diabetes or weight concerns. This group was required to journal at least 5 days weekly entering their workouts and meals with a specific target goal to meet by the end of the study. The PI was able to monitor daily journaling in the fitness tracker and send weekly reminders. Each member documented in MyFitnessPal and shared their diary with one of the authors (C.D.C.). This free site helped the HL participant journal their diet and exercise daily and track their goals.
All AD members have access to a certified nutritionist trained in telephone coaching, and these women were informed that this was still available if desired to help guide them. Many of the HL group (those with irritable bowel syndrome) were advised to use the fermentable oligo-, di-, mono-saccharides and polyols (FODMAP diet) due to their specific type of CPP. All slides were forwarded to the HL participants and they could elect to watch them asynchronously.
Mindfulness was measured among participants in both the MBSR and HL groups. To measure mindfulness, a multifaceted construct characterized by a shift in attention resulting in observation of each moment experience without interpretation, elaboration, or analysis of that experience as an intentional and nonjudgmental awareness, the FFMQ was used. 27 The FFMQ consists of subscales that measure the five facets of mindfulness: observe, describe, act with awareness, nonreactivity, and nonjudging, with 39 statements on a 5-point Likert-type scale ranging from 1 to 5. 27 Facet scores range from 8 to 40, except for the nonreactivity facet, which ranges from 7 to 35 (See Supplementary Table S2).
Pain perception (intensity and interference) was measured using the BPI. The intensity of pain is measured by 4 items (current as well as worst, least, and average in the past week) on 0 “no pain” to 10 “worst pain imagined” for the numerical scales. Seven activities describe the interference and include general activity, mood, walking, work, relations with others, sleep, and enjoyment of life, where 0 refers to “no interference” and 10 “complete interference.” 28 It is used in the military and can be completed in less than 5 min. It has established reliability (Cronbach's alpha ranges: 0.77–0.91), internal consistency, good to excellent test–retest values (intraclass correlation coefficient 0.84–0.90), and construct validity α > 0.70 in seven of nine studies documenting pain in cancer patients, lower back pain, range of motion, and muscle tenderness. 28
Depression was measured using the PHQ-9, a 9-item, Likert-type, self-assessment nominal screening and diagnostic tool used in primary care clinics in the Department of Defense (DOD) and VA routinely for somatic symptoms in depression. The PHQ-9 scores each item from 0 to 3 providing a severity score ranging between 0 and 27. The scores 0, 1, 2, and 3 are assigned to the response categories referring to frequency of a particular symptom over the last 2 weeks with “not at all,” “several days,” “more than half the days,” and “nearly every day,” respectively. 29 The severity of depression scores is graded as none/minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27).
The PHQ-9 has a sensitivity of 51%, a specificity of 94%, and high validity (area under the receiver operating characteristic curve 0.85, 95% confidence interval [CI] 0.82–0.88). 29 The PHQ-9 has been used internationally as a criterion-based diagnosis of mental disorders translated in 25 languages with adequate reliability, and construct and criterion validity in diverse samples. The DOD used the PHQ-9 in veterans and found adequate internal consistency (Cronbach's α = 0.92, 95% CI = 1.86–19.13) and test–retest (0.84). 30
Blood draws were collected at baseline before beginning either intervention and at 6 weeks (postintervention). They were not standardized by time of day or menstrual cycles due to the limitations in laboratory personnel, and access for participants during their duty day. Cytokine concentrations in plasma were measured using a multiplex electrochemiluminescence immunoassay kit developed by Meso Scale Discovery (MSD).
The customized U-PLEX (Cat. No. K15054D) assay consisted of the following analytes: granulocyte–macrophage colony-stimulating factor (GM-CSF), IFNg, interleukin (IL)-2, IL-4, IL-6, IL-8, IL-10, IL-17A, tumor necrosis factor alpha (TNFα), interleukin-1 receptor antagonist (IL-1Ra), monocyte chemoattractant protein (MCP)-1, stromal cell-derived factor (SDF)-1, and vascular endothelial growth factor (VEGF)α. The assay was carried out according to the manufacturer's instructions. Frozen plasma samples were thawed on ice, then diluted fourfold, run in duplicate, and analyzed using Discovery Workbench 4.0.12 software (MSD). Calibrators supplied by MSD were used to create standard curves and extrapolate sample concentration.
The collected data stored on REDCap were transferred to R version 3.5.0 for statistical analyses. Next, data were described using standard statistical methods such as frequency distribution, graphical displays of data, and application of the appropriate descriptive statistics to determine each variable's central tendency, distribution, and variability. Descriptive statistics were provided for subject characteristics and can be found in Table 1. Categorical variables are reported with counts and percentages, whereas continuous variables are reported as medians and interquartile ranges. The primary outcome was considered change in scores on the BPI, and the secondary outcomes were change in scores for FFMQ and PHQ-9 questionnaires. An a priori power analysis found that a sample size of N = 100 would be required to achieve a statistical power of 0.8, for an alpha level of 0.05 and an effect size of 0.5. Although underpowered with a sample size of N = 27, an alpha level of 0.05 was maintained to determine an effect size of 0.5, which is considered moderate to large.
Study Population Demographics
Data missing for one patient in each group.
GED, General Education Development.
The Mann–Whitney U (Wilcoxon signed rank) test was used to compare within-group differences for changes (pre- to postintervention) in mindfulness facets, pain scores, depression scores, and cytokine levels. For cytokines, outliers (detected using the Robust regression & OUTlier method) and undetermined values (below that of the lowest standard) were not included in the analysis. Statistical significance was defined as p < 0.05. Due to the exploratory nature of cytokine analyses, no adjustment was made for multiple comparisons, although adjusted means determined using the Bonferroni–Holm method are reported in Supplementary Table S1.
Results
The analysis included 41 eligible evaluable participants (MBSR = 21, HL = 20) from MTHM. A high attrition was projected for the “online” treatments, but the last-minute deployment contributed to even higher attrition (30% vs. 10%) for personal or professional obligations. The final completion total for both the groups was N = 28, including 14 participants from each group and plasma samples from 13 participants in the MBSR group and 12 in the HL group at baseline before the intervention and at 6 weeks following the intervention (see Supplementary Fig. S1 and Supplementary Data S1). The demographic characteristics of participants in the MBSR and HL groups are shown in Table 1. Of note, no participants reported any adverse events related to the interventions, although one participant in the HL group reported a broken arm due to a skiing accident in week 5.
Postintervention comparisons on the FFMQ demonstrated significant improvements for the MBSR group for all mindfulness facets except describe. No significant changes in mindfulness were found for the HL group. This demonstrated fidelity for the MBSR group along with assuring that the HL group was still “novice” to MBSR by comparison.
The effectiveness of MBSR and HL on pain was evaluated. Of the 28 participants who completed the study, 27 completed the BPI at both time points. At 6 weeks postintervention, women in the MBSR group exhibited significant reductions in pain interference (p < 0.01), over time, whereas those in the HL group did not (p ≤ 0.51; Fig. 1).
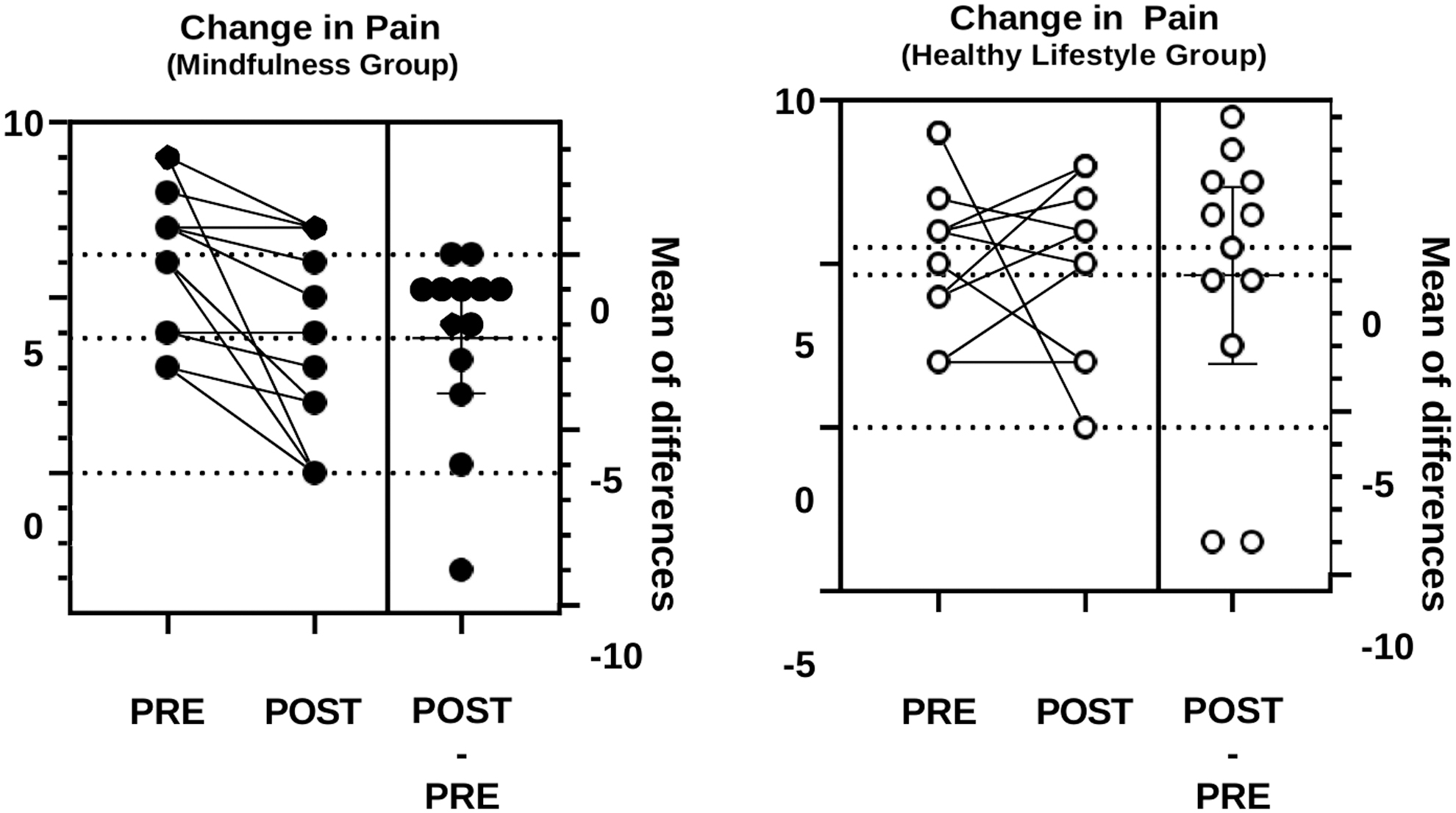
This figure demonstrates the changes in pain scores for both the MBSR group and the HL group from before the intervention to after each intervention. The mean scores of differences are in the figure. HL, healthy lifestyle; MBSR, mindfulness-based stress reduction.
The effectiveness of MBSR and HL on depression scores was also evaluated. Women in both the MBSR (p < 0.05) and HL (p < 0.05) groups had an overall significant reduction in depression score over time measured with the Total PHQ-9 (Fig. 2).
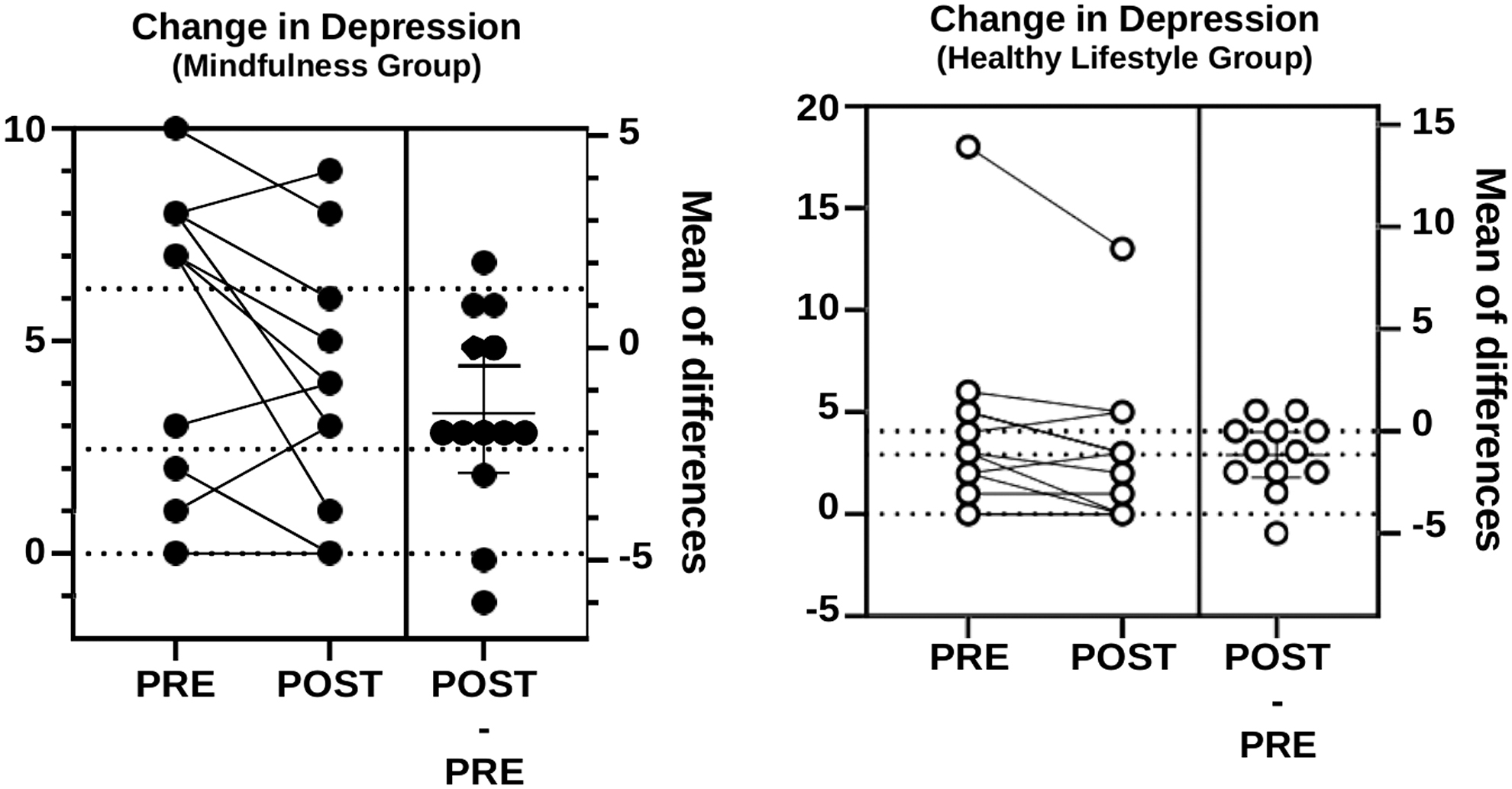
This figure demonstrates the mean differences in depression for both the groups. Note that the MBSR group had more notable changes to depression scores compared with the HL group.
Finally, the effects of MBSR and HL on plasma levels of proinflammatory and anti-inflammatory cytokines were evaluated. As shown in Figure 3, the MBSR group had decreased levels of IL-4 (p < 0.05), IL-6 (p < 0.05), eotaxin (p < 0.05), MCP-1 (p = 0.06), and IL-1ra (p < 0.01) with increased levels of VEGF (p < 0.05) over time (pre- to postintervention) measured. As shown in Figure 4, the HL group had decreased levels of GM-CSF (p < 0.05) and increased levels of TNFα (p < 0.05), SDF-1 (p < 0.01), and IL-1ra (p < 0.01).
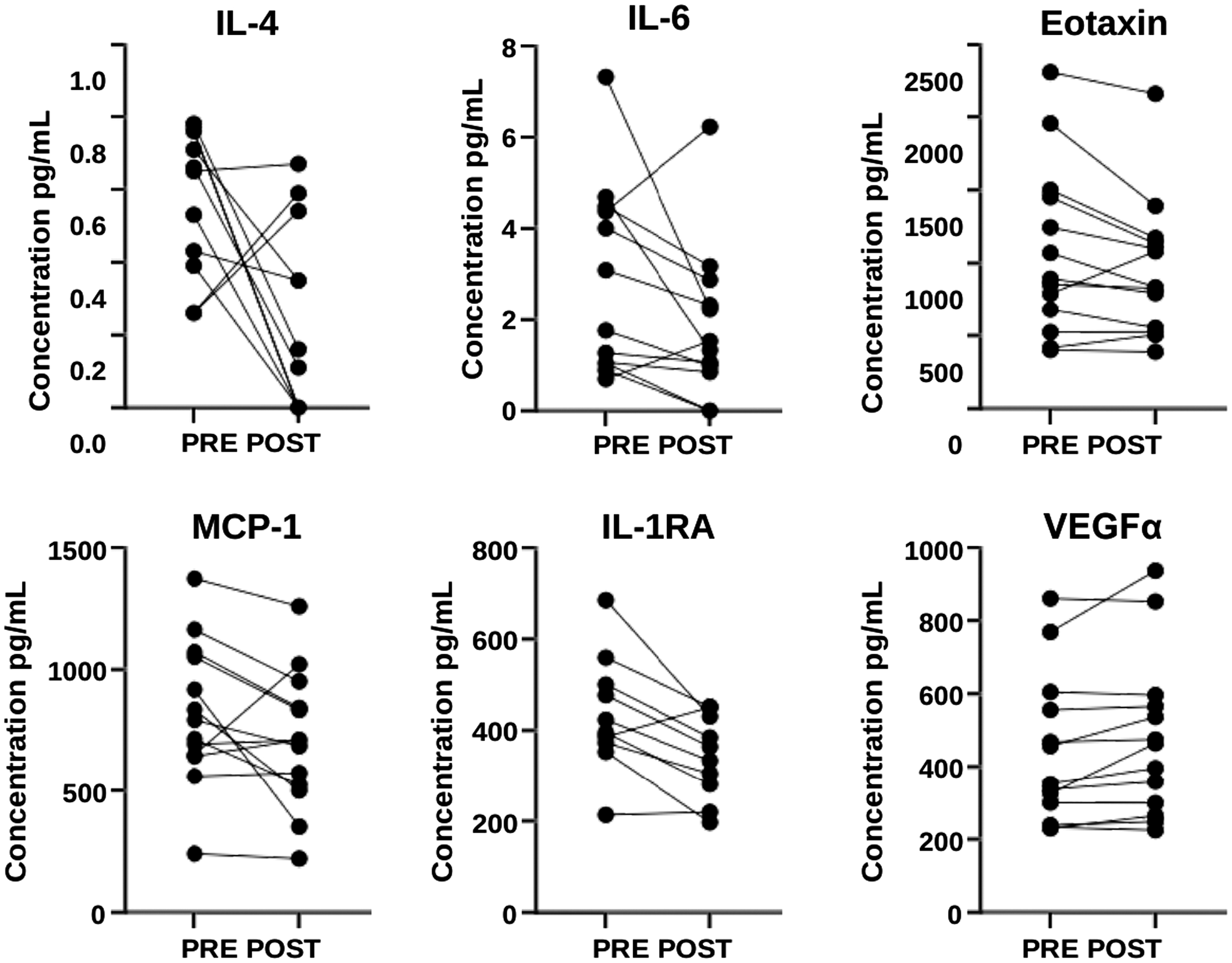
This figure shows the changes in cytokine levels for the MBSR group from before to after the intervention. These include both proinflammatory and anti-inflammatory cytokines.

This figure shows the changes in cytokine levels for the HL group from before to after the intervention.
Discussion
This study was designed to evaluate the effectiveness of a noninvasive, self-explanatory online MBSR or self-paced HL intervention on CPP, depression, and inflammation among AD women. The authors found that AD women receiving the MBSR intervention had significant reductions in CPP. Furthermore, women receiving either intervention had significant reductions in depression alongside plasma cytokine levels. While prior research has found MBSR and HL interventions effective for the management of related pain and health conditions, the results of this study are the first to demonstrate the benefit of MBSR and HL in a population of AD women with CPP.
The MBSR training significantly improved mindful actions for the MBSR group, with a 24% reduction in pain interference scores and a 15% reduction in depression scores postintervention. This is in line with published reports demonstrating that MBSR training improves pain and depression among patients with CPP. 22,31 –34
Accumulating evidence suggests that MBSR has multimodal effects on convergent pathways that regulate pain, mood, and inflammation. For example, MBSR treatment has been shown to reduce proinflammatory cytokine levels in patients with chronic pain conditions. 33 –35 Furthermore, it reduces stress hormones and activates descending pain inhibitory pathways. Women in the MBSR group also exhibited changes in cytokine expression levels. Specifically, levels of IL-4, IL-6, eotaxin, MCP-1, and IL-1ra were decreased and levels of VEGF were increased. Cytokines are small intracellular regulatory proteins secreted by immune cells in the periphery and neurons and glia in the central nervous system. 21
Proinflammatory cytokines increase the activity of nociceptors by direct receptor-mediated actions as well as by inducing the transcription of pain-relevant genes that promote long-term synaptic plasticity. 18 Meanwhile, anti-inflammatory cytokines negatively regulate proinflammatory cytokine expression and signaling to resolve inflammation and reduce pain. 36 IL-6, eotaxin, and MCP-1 are proinflammatory cytokines whose levels are elevated in patients with CPP 33,34,37,38 such that higher levels are associated with greater pain. 39 Additionally, elevated levels of these cytokines are correlated with depressed mood, 40 –43 which often accompanies CPP. The finding that expression levels of these cytokines were reduced following MBSR suggests that mindfulness may reduce pain and improve mood through normalizing cytokine signaling.
IL-4 and IL-1ra are anti-inflammatory cytokines well known to have analgesic effects, 36 and MBSR interventions that improve QOL, mood, and stress have been shown to increase their levels. 44 Thus, the finding that IL-4 and IL-1ra levels were decreased following MBSR was surprising, although in line with data from a study where plasma levels of IL-4 were elevated in endometriosis patients. 45 The finding that VEGF levels were increased following MBSR was also unexpected, as VEGF regulates angiogenesis and pain 46 and increased levels have been observed in patients with CPP. 47 Notably, the resolution of inflammation is an active process characterized by cyclical fluctuations in cytokines and growth factors released by immune and other cells to regain physiological homeostasis. 35 Thus, measurement of cytokines at multiple time points following MBSR may be required to understand the impact of this intervention on regulating proinflammatory versus anti-inflammatory cytokines.
While women in the HL group did not have significant reductions in pain scores, they did exhibit a 12% reduction in depression scores at the completion of the intervention. This finding is like others demonstrating the positive impact of HL interventions on mood. Specifically, a diet high in fruits, vegetables, whole grains, and antioxidants and low intake of animal foods has been associated with a decreased risk of depression. 48 Additional evidence demonstrates that exercise reduces depressive symptoms and improves QOL and physical function, independent of factors such as education or physical health. 49 –51 The HL women also exhibited significant changes in cytokine expression levels.
Specifically, levels of GM-CSF decreased and levels of TNFα, SDF-1, and IL-1ra increased. GM-CSF is an important hematopoietic factor that can promote macrophage migration from the bone marrow, contributing to the inflammatory process observed in depressive disorders. 52 Antidepressants, such as fluoxetine, have been found to reduce plasma levels of GM-CSF associated with improved mood. 52,53 IL-1ra is a member of the IL-1 cytokine family that serves as an endogenous negative-feedback regulator to control potentially pathological inflammatory events. 54 In addition to alleviating pain, IL-1ra improves mood in patients with depression and has been an important therapeutic target. 54 Thus, HL training may improve mood in women with CPP through normalizing GM-CSF and IL-1ra signaling.
Intervention-dependent increases in levels of the proinflammatory cytokines TNFα and SDF-1 were also observed. TNFα is a key regulator of immune function implicated in numerous health problems of immune origin, including CPP 55 and depression. 56 SDF-1 is emerging as an important contributor to pelvic inflammatory diseases 57 and depressive mood disorders. 58 Long-lasting increases in TNFα and SDF-1 are maladaptive; however, transient increases following HL interventions such as exercise may be vital for adaptive responses to training that ultimately have beneficial effects on mood.
Acute release of TNFα after exercise is necessary to induce anti-inflammatory cytokines (e.g., IL-1ra) promoting resolution of inflammation, tissue repair, and improved mood. 59 Acute increases in SDF-1 following exercise training augment the function of myocytes, 60 leading to regeneration of skeletal muscle and vascular tissues, respectively. While there is a gap in the understanding of specific mechanisms whereby combined exercise and nutrition training improve depression, the findings of this study together with published results suggest that a HL stimulates immune, muscle, and other cells to secrete proinflammatory and anti-inflammatory cytokines influencing mood-relevant pathways.
The online MBSR and HL interventions allowed for self-care in a military setting with widest dissemination for training at the participant's own time even during deployments. Using a web-based survey had several advantages, including population accessibility, time savings, and reduced cost. Online resources can potentially reach more AD members. Professional demands in the military can be overwhelming for many and having a resource that is easily accessible to them anywhere can be life changing. Active participation in an online MBSR program can potentially lead to less physiological reactivity in response to stressors, improving morbidity.
However, this study had several limitations. First, participants had to have access to emails and capability to open attached links. The amount of surveys using web-based systems invariantly led to respondent fatigue and unwillingness to participate by some. The loss of participants for this longitudinal study was projected as it was online, although the time interval between pre (baseline) and post (6-week) follow-up was short. Compensation is minimal with military members, and they were required to be self-driven to complete the online trainings. Second, although the demographics at MTHM were comparative to the USAF demographics, the sample size was small, increasing the chance of a type I error, and was restricted to MTHM, which may limit generalizability. Third, nutrition and exercise were not monitored for the MBSR group. Fourth, monitoring for major life events was not included. Fifth, in the absence of a no-treatment control group, the authors cannot rule out effects of other factors on improving pain- and inflammation-related outcomes. Thus, within-group comparisons are exploratory and must be interpreted with caution.
Future research should include comparisons using alternative MBSR trainings (classic vs. online-only MBSR) along with monitoring training for HL activities. Furthermore, a larger study focusing on the combined effects of MBSR and HL with a control arm measuring results over an extended period (6 months) would help understand sustainability and continued impact of the interventions. Discovering interventions beneficial in improving coping with chronic pain is relevant and necessary to future studies.
In summary, results from this interventional prospective study demonstrated that MBSR improved pain and related depression symptoms. Although HL did not have significant effect on pain, it did reduce comorbid depression and, thus, may have added benefit when used in combination with MBSR. These results support the need for larger randomized controlled studies to test the safety, efficacy, and feasibility of the MBSR and HL for AD women with CPP.
Footnotes
Acknowledgments
The authors thank the TriService Nursing Research Program support staff especially Kemia Duncan, Shannon Sarino, and Kesha Chandler. The authors thank the leadership team, Family Health, Women's Health, Flight Medicine, and laboratory for assistance at Mountain Home Air Force Base. The authors acknowledge Xin Zhang and Yaomin Wang at Duke University for assistance in analysis of samples.
Authors' Contributions
C.D.C. designed the study, wrote the article, and prepared the table. A.G.N. performed laboratory experiments, prepared figures, and wrote the article. E.A. had oversite and contributed to the writing of the article. R.B. and M.F. performed analysis and prepared the figures. All authors contributed to the interpretation of results and reviewed the contents of the article.
Disclaimer
The content and conclusions do not necessarily represent the official position or policy of, nor should any official endorsement be inferred by, the TriService Nursing Research Program, Uniformed Services University of the Health Sciences, the DOD, or the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was sponsored by the TriService Nursing Research Program (TSNRP), Uniformed Services University of the Health Sciences (USU Grant No. HU0001-1920057, Project No. N18-C03) to C.D.C.
Supplementary Material
Supplementary Figure S1
Supplementary Data S1
Supplementary Appendix SA
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.