
Abstract
Objectives:
Hot flashes are unpleasant long-term complications of breast cancer. This study aimed to evaluate the effects of a traditional Persian medicine containing extracts of Cichorium intybus L. (chicory) and Fumaria parviflora L. (Fumitory) extract syrup (CFS) compared with placebo when used as intended.
Design:
Randomized, double-blind, placebo-controlled clinical trial.
Setting/Location:
The Oncology Ward of Shahid Modarres Hospital (Tehran, Iran).
Subjects:
Breast cancer survivors undergoing hormone deprivation therapy.
Interventions:
Patients were randomly allocated to receive 5 mL CFS or placebo syrup three times a day, for 4 weeks.
Outcome measures:
The co-primary outcomes were self-reported daily hot flashes frequency and severity scores assessed using self-reported daily dairies, including 1 week of baseline data.
Results:
Of the 148 patients screened, 137 were eligible, and 96 were randomly allocated to receive either CFS (n = 48) or placebo (n = 48). All participants who returned their dairies were compliant and analyzed as randomized in the a priori per-protocol analysis. After 4 weeks of treatment, both the mean daily hot flashes frequency and severity score had reduced by 57% in the CFS group and 10% in the placebo group. The overall weekly mean daily hot flashes frequency (effect size ηp 2 0.221, p < 0.001, n = 66) and severity scores (effect size ηp 2 0.160, p = 0.001, n = 66) were significantly lower in the CFS group compared with the placebo group (one-within one-between repeated-measures analysis of variance adjusted for baseline). CFS was well tolerated, with similar proportions of serious and nonserious adverse events occurring in both groups.
Conclusions:
This is the first study to report the effects of chicory or fumitory for the treatment of hot flashes. The findings provide preliminary evidence that CFS can improve hot flashes in breast cancer survivors undergoing hormone deprivation therapy. More research is warranted to confirm its effectiveness, safety, and mechanisms of action.
Clinical Trial Registration:
IRCT20210226050506N1.
Introduction
Vasomotor hot flashes are the most common complications experienced by female breast cancer survivors following chemotherapy and while on estrogen deprivation treatment. 1 The condition causes daily dysfunction, sleep disorders, sexual problems, and diminished quality of life. 2,3 In the general menopausal population, the maximum incidence of hot flashes is 34%, whereas for breast cancer survivors, it is reported to be above 46%. 2 This complication has led to numerous breast cancer survivors not following their treatment plan and even refusing to continue cancer treatment, 3,4 which in turn can negatively impact their prognosis and survival. 5
Management options for breast cancer survivors suffering from hot flashes are limited, as hormone replacement therapy is contraindicated due to the increased risks of cancer recurrence, along with other complications such as deep vein thrombosis. 6 –8 Recommended non-estrogen synthetic pharmaceuticals include selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), and gabapentin. 6,7 However, side effects such as insomnia, dizziness, weight gain, dry mouth, headache, and constipation often limit acceptability and tolerance. 6
Unpleasant side effects of cancer treatments are common motivating factors for traditional, complementary, and integrative medicine (TCIM) use. 9 Most of the high-quality evidence in the support of TCIM for breast cancer survivors are for mental health and quality-of-life outcomes rather than for the management of hot flashes. 10 –13 For instance, there is emerging evidence that some traditional Chinese herbal medicines may be effective for improving other menopausal symptoms and quality of life in breast cancer survivors, but their effects on hot flashes are uncertain. 12,14 Cimicifuga racemosa (black cohosh) is probably effective for general menopausal populations, yet the results are mixed for breast cancer survivors. 15 –17
Other herbs, including Hypericum perforatum (St. John's wort), Humulus lupulus L. (hops), and Valeriana officinalis (valerian), have also demonstrated efficacy for general menopausal populations; however, they are yet to be evaluated in breast cancer populations. 14,18 –20 Soy phytoestrogens are unlikely to be effective. 10,14 Acupuncture may alleviate general menopausal symptoms in breast cancer survivors; however, it also appears to have little effect on hot flashes. 13 It should be noted that many of the phytotherapies commonly used to manage menopausal symptoms have phytoestrogens that are estrogen-like structures, 20 and the safety of their long-term use by breast cancer survivors continues to be debated. 16,17,21,22
Persian medicine (PM), with a long and prolific traditional history, introduces many recommendations for managing hot flashes. Cichorium intybus L. (chicory) and Fumaria parviflora Lam. (fumitory) are among the medicinal plants frequently used and were selected for this study. The synergistic effects of combining these medicinal plants in syrup dosage form are cited in the most important PM textbooks: the Al-Qanun fi al-Tibb and Makhzan ol-Adviya. 23,24 PM scholars believe that oral consumption of these herbal medicines could cool down the body, remove the fever, alleviate the severity of hot-quality humors (bile and blood), and eject the scorched waste material through urinary and alimentary gateways. 23,24
The scientific mechanisms of action of the two herbs for hot flashes are yet to be elucidated, as there is no direct preclinical or clinical research evaluating the herbs in the context of hot flashes. However, the extracts used (chicory seed and fumitory aerial parts extracted with hot water infusion) have low amounts of phytoestrogens making them suitable for breast cancer survivors undergoing hormone deprivation therapy. 25,26
The two plants are widely cultivated across Asia and Europe. 27,28 In vitro and preclinical studies have mostly focused on their antipyretic, antioxidant, analgesic, anti-inflammatory, antispasmodic, anti-infective, and pro-testosterone effects with potential clinical indications for diarrhea, jaundice, immune stimulation, liver toxicity, diabetes, and even male infertility. 27,29 There is also emerging preclinical evidence to suggest that the two herbs may have various neurological effects. 30 –32 Clinical studies have evaluated the effects of F. parviflora L. extract on chronic hand eczema 33 and uremic pruritus in hemodialysis patients, 34 and C. intybus L. root extract for osteoarthritis of the hip or knee 35 and its antiplatelet effects in healthy adults. 36 The two herbs were well tolerated in these clinical trials, and there were no serious adverse events.
Despite their traditional use in PM, the efficacy of either herb for the management of hot flashes is yet to be evaluated in a clinical trial. The aim of this study was to evaluate the effects of a C. intybus L. (chicory) and F. parviflora L. (fumitory) extract syrup (CFS) compared with placebo syrup, when used as intended, on the severity and frequency of hot flashes in breast cancer survivors undergoing estrogen deprivation treatment.
Materials and Methods
Study design
This study was a single-center, randomized, double-blind, parallel, placebo-controlled clinical trial. Eligible participants were randomized in equal proportions to receive CFS or placebo syrup for 4 weeks. The trial protocol was registered in the Iranian Registry of Clinical Trials. No changes to the protocol were made after trial commencement.
Participants
Study participants were outpatients who had been referred to the Oncology Ward of Shahid Modarres Hospital (Tehran, Iran). The recruitment period was February 2021 to October 2021. An oncologist identified and screened potentially eligible patients with confirmed breast cancer diagnosis (confirmed by a certified pathology report) and invited them to participate in the trial if they met the following inclusion/exclusion criteria.
The included study participants were females, aged 18–65 years, with a diagnosis of breast cancer (stage 0–3), who had previously undergone chemotherapy, surgery, or radiotherapy, and at the beginning of the enrollment, at least 4 weeks had elapsed since commencing an estrogen deprivation treatment, such as oophorectomy, tamoxifen, luteinizing hormone-releasing hormone agonists, aromatase inhibitors, or Herceptin, and without any dose modification. The minimum required hot flashes criteria were at least two hot flashes in 24 h.
Patients were excluded if they were currently using, or had used in the last 4 weeks, any of the following: acupuncture, vitamin E, omega-3, phytoestrogen supplements, high-phytoestrogen diets, hypnosis, psychosomatic therapies, antidepressants (e.g., venlafaxine, bupropion, fluoxetine, paroxetine, citalopram, sertraline), anxiolytics or sedatives (e.g., diazepam, temazepam), gabapentin, pregabalin, clonidine, or aspirin, or if there was a history of hypersensitivity to chicory, fumitory, or additives to the syrups. Patients with cardiac, hepatobiliary, renal, or endocrine including diabetes mellitus comorbidities were also excluded.
Intervention
Participants were given three identical 150 mL bottles of CFS or placebo syrup that were matched for color and appearance. They were instructed by the research assistant to self-dispense 5 mL of syrup, 1 h before meals, three times a day (breakfast, lunch, and dinner) for 4 weeks.
To prepare the CFS product, the dried limbs of C. intybus L. and F. parviflora Lam. were purchased from one of the most reputable perfumeries in Tehran; they were then approved and registered by the pharmacist of medicinal plants in the herbarium of the Tehran University of Medical Sciences, School of Pharmacy, who prepared the CFS and placebo interventions. The codes of chicory and fumitory herbarium are TUH-1762 and TUH-2317, respectively. The plants were cleaned and washed, and then dried. The chicory seeds and fumitory aerial parts were then collected and grounded separately.
Twenty grams of chicory seeds and 10 g of fumitory aerial part were boiled in 150 mL of water for 25 min and strained. From which, 70 mL was combined with 35 g of sugar and 20 mL of vinegar. To prepare the placebo syrup, 1000 g of sugar was added to 500 mL of water and 250 mL of vinegar and heated to achieve the desired consistency. A natural edible color (Sirang, Khorasan) was then added to appropriate it to the color of the CFS product. The two products were bottled and coded in three identical bottles each with a capacity of 150 mL.
The spectrophotometric method used to analyze the total amount of phenolic compounds in the CFS extract was based on the Folin–Ciocalteu method. 37 For this purpose, 1 mL of the extract was poured into a test tube, and 5 mL of Folin–Ciocalteu solution diluted in distilled water in a ratio of 1–10 was added to it and kept away from light. After 10 min, 4 mL of 75 mg/mL sodium bicarbonate solution prepared with distilled water was added to the solution and incubated for 30 min away from light at room temperature. After this time, the absorbance of the sample was measured at 765 nm. 38 The amount of total phenol measured in the extract based on gallic acid was equivalent to 6.58 ± 0.15 mg GAE/mL.
The microbial stability of the product, total counting tests of aerobic microorganisms, and the total count of total mold and yeast were performed, and the presence of Escherichia coli and Salmonella spp. in the extract was examined. The total aerobic microbial count and the total yeasts/molds count were within the normal range according to acceptable U.S. pharmaceutical criteria. 39 In addition, two samples were negative for E. coli and Salmonella spp.
Primary outcomes
The weekly mean daily frequency of hot flashes and the weekly mean daily hot flashes severity score across the 4 weeks of treatment after adjusting for baseline frequency or severity were the primary outcome measures. Participants were asked to fill out daily in their diary the number of hot flashes they experienced and the overall daily severity (rated on a 1- to 4-point scale of mild, moderate, severe, or very severe) (Supplementary Appendix SA1). 40
Safety assessment
Any reported adverse event was considered a secondary outcome. Participants were followed up by a researcher every 2 weeks to identify possible side effects from the intervention. Additionally, participants were requested to inform the researchers of any unusual symptoms they experienced at any time and record them in their diary (Supplementary Appendix SA1). They were also advised to call their physician if experienced any adverse event in study period.
Other assessments and procedures
Participant data were collected at enrolment. Baseline data included age, height, weight, current and past breast cancer treatments, menopausal history, marital and occupational status, and 1 week of daily hot flashes frequency and severity. Participants were asked to visit their physician on a weekly basis. They completed the dairies daily and handed them in their last visit to the physician.
The CFS and placebo bottles were collected at the final visit to check compliance. Whenever possible, the reason for participant withdrawal from the trial was recorded. Adequacy of blinding was not assessed.
Randomization and allocation concealment
A research assistant who was not involved in the eligibility assessment and was blinded to the intervention codes randomly assigned participants and dispensed the study interventions. Participants were randomization with an allocation ratio of 1:1 with no block randomization that was performed using Randomizer software (Saghaei M. [2004], Random Allocation Software [Version 1.0]).
Only the pharmacist had access to the intervention codes, which were concealed from the researchers until after the database was locked. If a serious adverse event was reported, the allocation could be immediately decoded by the main researcher and the participant would be withdrawn from the study. Otherwise, intervention allocation was decoded at the end of the study by the main researcher.
Sample size
Based on the expected difference of 2.8 in the hot flashes score between the two groups according to a previous study, 2 the sample size was calculated at 40 patients in each group with a two-sided significance level of 0.05 and power of 90%. Considering the possibility of failure to follow-up and participant non-compliance, the sample size was set at 48 patients per group.
Statistical methods
Since the efficacy of CFS was yet to be evaluated in a clinical trial, the treatment effect of greatest interest was the effect of CFS when used as intended. Therefore, the statistical analysis plan was according to a per-protocol analysis that was written before database lock and unblinding (Supplementary Appendix SB1). Only participants who completed the 5-week trial and consumed at least 30% of the prescribed total amount (≥136 mL) would be included in the analysis. The weekly mean daily frequency of hot flashes was calculated by dividing the total number of hot flashes by the number of days. The daily hot flashes severity score was calculated as the hot flashes frequency multiplied by the severity rating of mild, moderate, severe, or very severe on a 1- to 4-point rating scale. 40 The weekly mean daily hot flashes severity score was calculated in the same manner as the weekly mean of daily frequency of hot flashes. Missing items from the daily dairy entries were interpolated by trend analysis. 41 Data are described as mean ± standard deviation or counts with percentage.
One-within one-between repeated-measures analysis of variance (ANOVA) adjusted for baseline was used to compare the weekly mean daily frequency of hot flashes and the weekly mean daily severity scores between the two groups across the 4 weeks of treatment. This was followed by repeated-measures ANOVA post hoc testing with the two-sided, independent samples t test and analysis of covariance to adjust for baseline differences and to compare the weekly mean differences between the two groups at weeks 2, 3, 4 and 5.
Statistical significance was set at 0.05. The conservative Bonferroni method was used to control the type I error rate from multiple comparisons. 42 Partial eta squared (ηp 2 ) was used as the measure of effect size with 0.01 considered small, 0.06 medium, and 0.14 large. All the data were analyzed using Statistical Package for the Social Sciences software, version 15 (IBM SPSS, Chicago, IL). (See CONSORT herbal medicine extension as Supplementary Appendix SC1).
Ethical considerations
The study was performed in compliance with the guidelines of the Declaration of Helsinki. This study was approved by the ethics committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.MSP.REC.1398.125). All the participants willingly signed the informed consent form before participating in the study. Participants received no financial reimbursements.
Results
Participants' enrollment
In this clinical trial, 148 patients with hot flashes were screened, from which 137 were eligible and 96 participants were enrolled and randomly allocated to either the CFS group (n = 48) or the placebo group (n = 48). Thirty-two participants in the CFS group and 34 in the placebo group completed the trial and were included in the per-protocol analysis (Fig. 1). All participants who returned their diary were administered the correct intervention and were compliant. Therefore, all participants were analyzed according to the group they were randomly allocated. Missing data items were imputed for 3.1% of frequency items and 3.1% of severity items in the CFS group and 0% of frequency items and 2.9% of severity items in the placebo group.
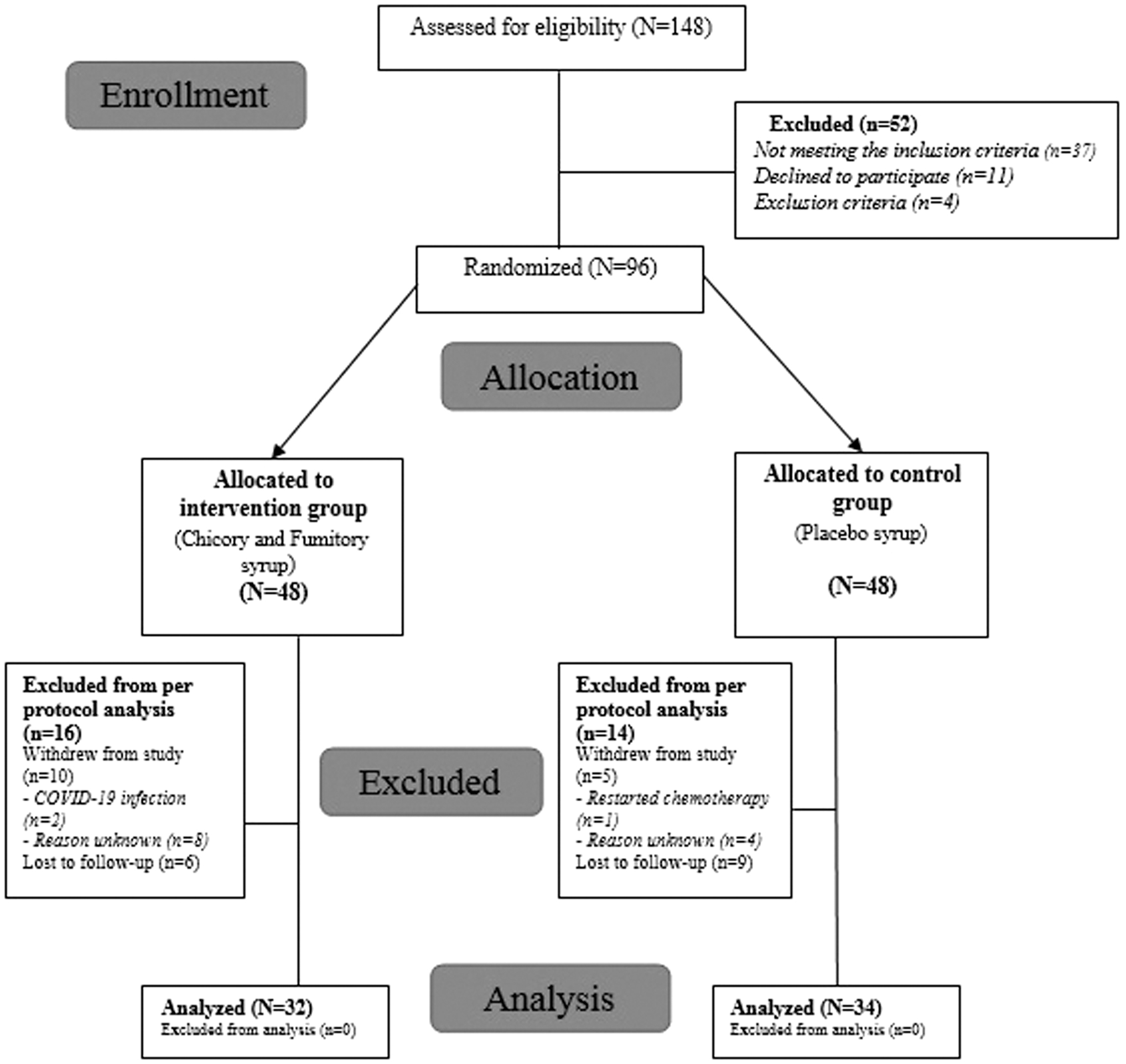
The consolidated standards of reporting trials (CONSORT) flow diagram.
Baseline characteristics
The baseline demographic and clinical characteristics of the 96 participants enrolled and the 66 participants included in the analysis are shown in Table 1. The mean age was 52 ± 7.21 and 52 ± 6.35 years, respectively, in the intervention group and 48 ± 7.42 and 49 ± 8.31 years, respectively, in the placebo group.
Baseline Characteristics of the Participants
BMI, body mass index; CFS, cichorium intybus L. (chicory) and Fumaria parviflora L. (fumitory) extract syrup; SD, standard deviation.
Hot flashes frequency
From baseline (week 1) to week 5, the hot flashes frequency in the CFS group had significantly reduced by 57.3% (mean difference −1.37, 95% confidence interval [CI]: −1.74 to 0.99, p < 0.001) compared with a nonsignificant reduction of 9.8% in the placebo group (mean difference −0.21, 95% CI: −0.42 to 0.0, p = 0.524). After adjusting for baseline frequency, the overall weekly mean daily frequency of hot flashes was significantly lower in the CFS group than in the placebo group (effect size ηp 2 0.221, p < 0.001) (Table 2).
Hot Flashes Frequency and Severity Scores Among Breast Cancer Survivors
Adjusted for baseline frequency or severity score.
Bonferroni corrected p-values for two pairwise comparisons two-sided, independent samples t test.
Bonferroni corrected p-values for two pairwise comparisons ANCOVA adjusted for baseline.
One-within repeated-measures ANOVA adjusted for baseline.
One-within one-between repeated-measures ANOVA adjusted for baseline.
ANCOVA, analysis of covariance; ANOVA, analysis of variance; CFS, cichorium intybus L. (chicory) and Fumaria parviflora L. (fumitory) extract syrup; CI, confidence interval; MD, mean difference; SD, standard deviation.
Weekly comparisons found that the differences between the groups started to become apparent at week 4, but only after adjusting for baseline frequency (Table 2). By the last week of the intervention (week 5), the differences between the two groups were significant both with and without adjusting for baseline frequency. Participants in the CFS group experienced an average of around one less hot flash daily than the placebo group (mean difference: −0.92, 95% CI: −1.59 to −0.24, p = 0.009; adjusted mean difference: −1.14, 95% CI: −1.57 to −0.72, effect size ηp 2 0.320, p < 0.001; Table 2 and Fig. 2).
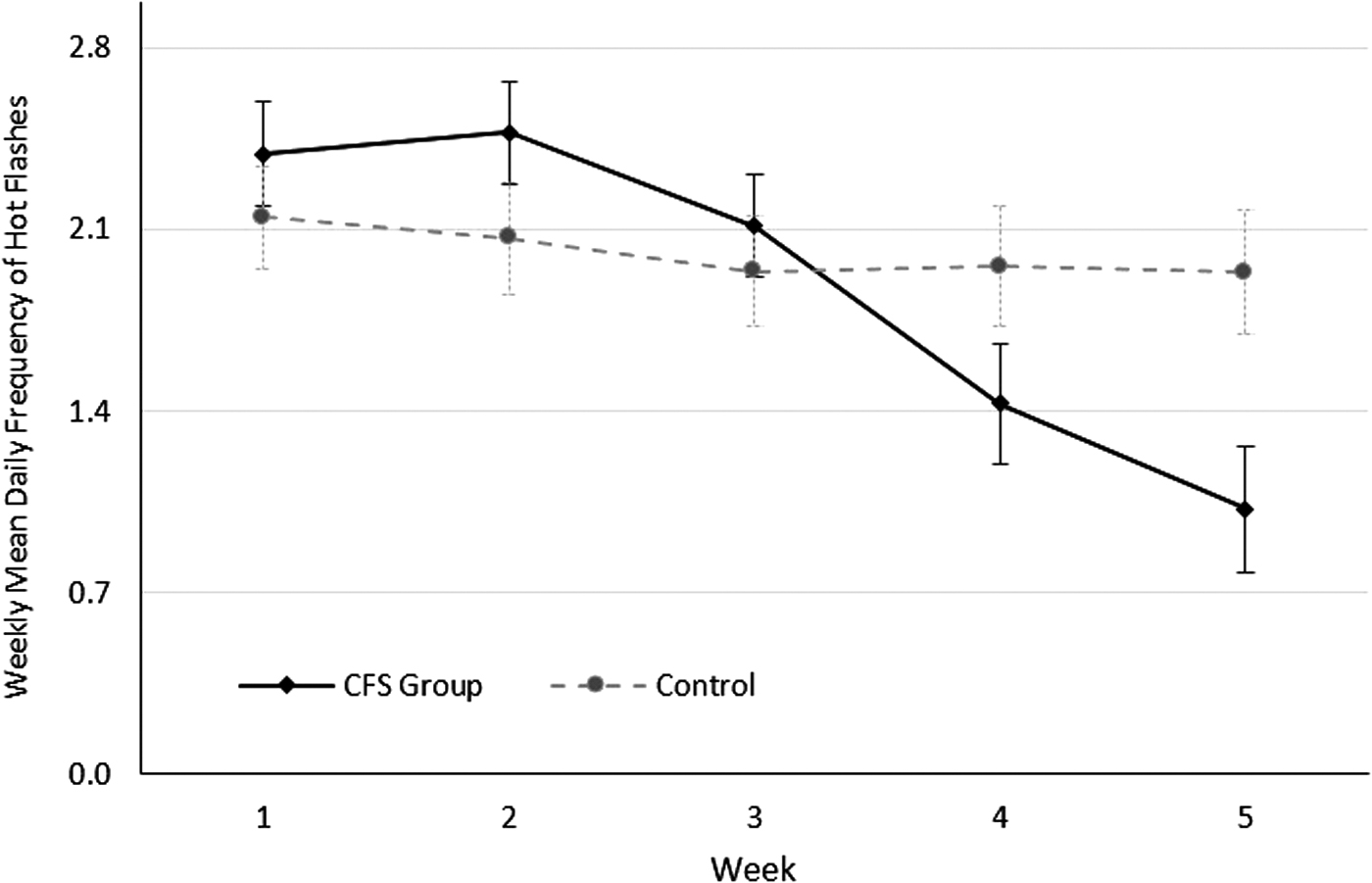
Weekly mean daily frequency of hot flashes with standard error bars.
Hot flashes severity score
From baseline (week 1) to week 5, the weekly mean hot flashes severity score in the CFS group had significantly reduced by 56.6% (mean difference 2.434, 95% CI: −3.42 to −1.46, p < 0.001) compared with a nonsignificant reduction of 9.8% in the placebo group (mean difference −0.26, 95% CI: −0.58 to 0.06, p = 0.112). After adjusting for baseline severity, the overall weekly mean hot flashes severity scores were significantly lower in the CFS group compared with the placebo group (effect size ηp 2 0.160, p = 0.001) (Table 2).
Again, weekly comparisons found that the differences between the groups started to become apparent at week 4, but only after adjusting for baseline severity (Table 2). By week 5, the differences were significant both with and without adjusting for baseline severity (mean difference: −1.32, 95% CI: −2.87 to 0.23, p = 0.094; adjusted mean difference: −2.01, 95% CI: −2.97 to −1.06, p < 0.001, effect size ηp 2 0.219; Table 2 and Fig. 3).

Weekly mean daily hot flashes severity scores with standard error bars.
Adverse events
Two participants in the CFS group withdrew from the study due COVID-19 infections, and one participant in the placebo group withdrew due to cancer recurrence requiring chemotherapy. In the per-protocol data set, the proportions of participants in each group who experienced a nonserious adverse event were similar. In the CFS group, one participant had a headache, one participant felt cold in her hands and feet, and one participant complained of increased pain in her hands and feet. In the placebo group, two participants had headache, two participants complained of cold in their hands and feet, and one participant suffered from fatigue.
Discussion
This is the first study to report the effects of chicory and fumitory syrup on hot flashes in breast cancer survivors undergoing hormone deprivation therapy. It is also the first to evaluate the effects of either herb in any menopausal population. The results showed that CFS significantly alleviated both the hot flashes frequency and severity scores across the 4 weeks of treatment and the effect sizes were large. At the end of the study, both the weekly mean hot flashes frequency and severity scores were 57% lower in the CFS group, whereas only 10% reductions were observed in the placebo group. Comparisons of the weekly mean differences revealed that the effects of CFS started to become apparent after 3 weeks of treatment (week 4) and were statistically and clinically significant by the end of the study (week 5). CFS was well tolerated, with similar proportions of serious and nonserious adverse events occurring in both the groups.
Based on the finding of this study, CFS may be a suitable alternative to clinically proven nonhormonal synthetic pharmaceutical options. 6 –8 Indeed, the percentage improvements from baseline in both the frequency and severity scores are comparable. 43 It is worth noting, however, that the baseline hot flashes frequency and severity scores tended to be higher in the randomized controlled trials (RCTs) evaluating these pharmaceuticals. 43 Future research is therefore required to confirm the CFS efficacy in populations with more severe symptoms and compare its efficacy to these recommended pharmaceuticals.
The results from this double-blind placebo-controlled RCT are among the first to demonstrate the efficacy of a phytotherapy for hot flashes in breast cancer survivors. 10,11,16 For instance, the findings are mixed for commonly used herbs such C. racemosa (black cohosh); only nonrandomized studies of interventions and open-label RCTs have reported benefit, whereas a double-blind, randomized, placebo-controlled crossover trial did not. 16,44,45 Benefits have also been reported for various traditional Chinese herbal medicine formulations; however, these RCTs were all open-label with no placebo or active control. 14
The potential mechanisms of action of the chicory and fumitory extracts for relieving hot flashes are yet to be determined, as are any synergistic, antagonistic, or antitoxic effects from combining the two extracts. The pharmaceutical actions commonly reported in the literature tend to focus on their beneficial effects on liver toxicity and anti-inflammatory, antipyretic, and antioxidant properties. 25,29,46,47 This property might be attributed to aforementioned medicinal drugs components' ability to decrease proinflammatory factors such as interleukin levels. 47 Yet, these actions do not provide a satisfactory explanation on their own, as hot flash is a disorder of temperature regulation that involves hypothalamic thermoregulatory instability following estrogen withdrawal. 6,7
There is emerging research to suggest that both herbs may also have neurological effects. The glycosides and triterpenoids in chicory have been found to inhibit glutamatergic transmission and enhance GABAergic transmission, 30 and the seeds, which was the part used in the CFS product, contain numerous amino acids that are precursors for neurotransmitters. 47 Fumitory may have diverse effects on the nervous system, including potential anxiolytic and pro-cognitive effects that have been attributed to protopine and other psychoactive alkaloids in the herb, 31 with some postulating that fumitory may be a functionally novel type of anxiolytic through the inhibition of cytokine expression in the nervous system. 32
These findings are noteworthy given that there are numerous neurologically active pharmaceuticals that can alleviate hot flashes. 6,7 Therefore, along with elucidating CFSs potential mechanisms of action, given the potential multisystem effects of CFS, future clinical trials should also consider evaluating its effect on other symptoms that are known to impact the mental health and quality of life of breast cancer survivors. 48
The decision to investigate CFS was inspired by traditional PM. 23,24 The use of ethnopharmacology, ethnomedicine, and reverse pharmacology to discover new compounds and medicines is nothing new. 49 Typically, in vitro bioassays and other analytical technologies are applied in a logical sequence to screen for pharmacological activity and identify new compounds, that is followed by in vivo preclinical studies, and eventually clinical trials. 50,51 Unfortunately, the yield is very low. It has therefore been argued that this target-based approach is inefficient due to the complexity of natural products and failure to fully harness the holistic wisdom of traditional medicine. 51,52
Indeed, this present study is a good example. Based on the preclinical research to date, it is highly unlikely that this herbal formulation would be identified as a candidate for treating hot flashes. Hence, an alternate strategy is proposed. After identifying and understanding the traditional medicine context, paradigm, philosophy, and utilization, safety is then confirmed, followed by controlled studies involving humans to confirm effectiveness and efficacy, and finally, the pharmacological mechanisms of action are investigated. 53
This study is not without limitations, and further clinical research is required to confirm the results. There was substantial missing participant data due to study withdrawals and lost to follow-up (31%, n = 30/96) that could bias the results. For example, participants missing from the placebo group may have had higher frequency and severity scores that led them to leave the study due to perceived ineffectiveness, while participants in the CFS group may have left due to more nonserious adverse events including taste aversion. Reassuringly, the proportion missing from both the groups and baseline characteristics was similar.
However, there was only a limited amount of data available about the reason for withdrawal and none of these participants returned their diaries. Therefore, there were no outcome data, including daily hot flashes frequency and severity during week 1 (baseline) that could be used to conduct a sensitivity analysis to evaluate the robustness of the results. As this was the first study to evaluate CFS for hot flashes, a per-protocol analysis was conducted to evaluate whether the formulation was likely to be efficacious when used as intended. However, the analysis also ended up adhering to an intention-to-treat (ITT) analysis. All 66 participants who returned their daily dairy were compliant; therefore, they were analyzed according to the group they were randomly assigned and none of the data collected were excluded from the analysis.
Despite using a valid measure in this study and blinding the participants and researchers, there was not an objective outcome measure. This raises some concerns about outcome measurement bias, as the placebo was not matched for taste and the adequacy of blinding was not assessed. The limited sample size, which was underpowered due to a large dropout rate, and lack of long-term follow-up are some other limitations of the study. Finally, there is limited generalizability to other populations, with and without a diagnosis of breast cancer and with higher hot flashes frequency and severity. Prescription of CFS with different dosages should be taken into consideration by future studies.
Conclusions
This study presented the first evidence on the potential efficacy and safety of a combination herbal medicine extract of C. intybus L. (chicory) seeds and F. parviflora L. (fumitory) aerial parts. According to the results, daily consumption of CFS for 4 weeks can significantly reduce hot flashes frequency and severity in breast cancer survivors using estrogen deprivation therapy. Future studies using an ITT analysis, with adequate power, and a longer follow-up are necessary before drawing any definite conclusions. Finding the proper dose of the preparations also requires further investigatory attempts, and the mechanisms of action are yet to be elucidated.
Authors' Confirmation Statement
All the authors declare that they are employed at an academic or research institution as researchers or faculty members where research or education is the primary function of the entity.
Authorship Statement
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Footnotes
Acknowledgments
The authors would like to be grateful to the patients participated in this research.
Authors' Contributions
Conception and designing of study (N.R., M.P., G.H.); data collection (A.K., M.M.A., F.H., G.H.); data analysis (M.P., J.H., G.H.); article drafting (A.K., M.M.A., F.H., M.P., G.H.); critical revision (N.R., M.P., J.H., G.H.); supervision (N.R., G.H.); all the authors read and approved the final version of the article.
Author Disclosure Statement
The authors declare that there is no competing interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix A1
Supplementary Appendix B1
Supplementary Appendix C1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.