
Abstract
Introduction:
It is recommended that users of complementary and alternative medicine (CAM) also seek conventional medical care to prevent the loss of access to appropriate medical care. However, the status of such use is unknown. The aim of this study was to examine the time trends in the proportion of CAM users who also receive conventional medical care for the same symptoms.
Methods:
This is a repeated cross-sectional study. Of data for 753,978 respondents to the Comprehensive Survey of Living Conditions, which was conducted seven times between 1995 and 2013, data from 17,707 individuals who used acupuncture, moxibustion, anma-massage-shiatsu, or judo therapy were analyzed. Cross-classified multilevel logistic regression models with individuals as level 1 and survey year and cohort as level 2 were used to calculate odds ratios (ORs) and 95% credible intervals (CIs) for combined use of CAM and conventional medical care. Age was entered as an individual-level variable. The period effect after 2003 was entered as a survey year-level variable because the number of eligible persons providing CAM treatments has increased since 2003.
Results:
Among the 17,707 CAM users, 11,567 (65.3%) were women. When age was entered as an explanatory variable, the results showed that both older men and women tended to receive conventional medical care (women, OR: 1.04, 95% CI: 1.03–1.04; men, OR: 1.03, 95% CI: 1.02–1.04). Additional examination of the possible period effect after 2003 showed a positive (although nonsignificant) association (women, OR: 1.36, 95% CI: 0.89–1.99; men, OR: 1.37, 95% CI: 0.94–1.91).
Conclusions:
As patient age increased, patients combined CAM use with conventional medicine. The findings also suggested that the combined use of CAM and conventional medicine has increased since 2003.
Introduction
Complementary and alternative medicine (CAM) is used worldwide. According to a survey conducted in 2003–2015, >70% of the general population in North America has tried CAM at least once, 1 whereas a survey in 2014 reported that 25.9% of the general population in Europe had used CAM in the past 12 months. 2 A 2016 survey in Japan found that 12.8% of the population had used CAM at least once per year. 3 Among patients in Japan who have chronic disease and have used CAM, massage was the second most used CAM modality, and the fifth most used was acupuncture and moxibustion. 4
As has been widely noted, it is important to differentiate the terms “complementary” and “alternative” regarding the use of CAM. According to the National Center for Complementary and Integrative Health (NCCIH), “complementary” medicine use is use of a nonmainstream approach together with conventional medicine. In contrast, “alternative” medicine use is use of a nonmainstream treatment modality in place of conventional medicine. 5 Some previous studies have reported the potential adverse health effects of alternative medicine use (e.g., delay or loss of access to appropriate medical care). 6,7
In this regard, the NCCIH emphasizes the importance of “integrative” health, which brings conventional and complementary approaches together in a coordinated way, recommending scientific research on “complementary and integrative” health approaches. 5,8 In line with this, the World Health Organization (WHO) also promotes the strategy of closer integration of CAM into the health care system. 9 Despite some concerns about appropriate CAM use, few studies have examined evidence for the integrative use of CAM among the general population.
Accordingly, the aim of this study was to examine time trends in the proportion of acupuncture, moxibustion, anma, massage, shiatsu, and judo therapy users who use these treatment modalities integrally (i.e., in combination with conventional medicine) in Japan from 1995 to 2013. Age–period–cohort (APC) analysis was conducted using a repeated cross-sectional survey of a nationally representative sample of Japanese people.
Ethical approval
This study was approved by the institutional review board of Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences and Okayama University Hospital Ethics Committee (No. K2103-001).
Methods
Participants
The study data were obtained from the Comprehensive Survey of Living Conditions (CSLC), which was conducted by the Japanese Ministry of Health, Labour and Welfare. This is a nationwide cross-sectional survey that has been conducted every year since 1986 to obtain basic data on household structure. To obtain detailed information on living conditions, including health care, medical services, welfare, and pensions, a large-scale CSLC survey is conducted every 3 years. For example, in the CSLC survey conducted in 2013, complete households and household members living in 5530 randomly selected area units were sampled in the CSLC survey conducted in 2013, in which trained surveyors visited each household, and distributed and collected self-administered questionnaires.
Permission was obtained from the Ministry of Health, Labour and Welfare to use anonymized CSLC data from 1995 to 2013, which was the latest data available as of March 2021. The CSLC response rates were 91.0% in 1995, 89.7% in 1998, 87.4% in 2001, 79.9% in 2004, 80.1% in 2007, 79.4% in 2010, and 79.6% in 2013. Note that there is a possibility that the same person responded more than once.
The questions used to determine eligibility included skip patterns. First, individuals in hospital or using a long-term care insurance facility were excluded (question 2). Second, individuals with no subjective symptoms over a period of several days were excluded (question 3). Individuals with subjective symptoms were then asked to select subjective symptoms from multiple options and then select the one symptom that they found most worrisome (supplementary question 3–1). Those who selected their most worrisome symptom were then asked to report their use of the following treatment options: attending a hospital or clinic; attending an anma-massage-shiatsu, acupuncture, moxibustion, or judo therapy session; using over-the-counter drugs; using other treatments, or no treatment (supplementary question 3–2).
Of the 753,978 participants from 1995 to 2013, 234,437 participants who identified their most worrisome symptom and who selected anma-massage-shiatsu, acupuncture, moxibustion, or judo therapy as their chosen treatment method for their most worrisome symptom were defined as CAM users. Data for these individuals were used in this study.
CAM situation in Japan
In Japan, there are several types of CAM practitioners, including acupuncturists, moxibustion therapists, anma-massage-shiatsu therapists (anma and shiatsu are Japanese-style massage), and judo therapists (this type of therapy originated in first aid for judo injuries). Despite being CAM modalities, acupuncture, moxibustion, anma-massage-shiatsu, and judo therapy are partly covered by national health insurance (NHI) and are, therefore, partly integrated into the NHI system. However, under the NHI, the combined use of CAM and treatment at a conventional medical institution is not permitted.
Furthermore, because only 36% of acupuncturists and moxibustion therapists provide NHI treatment, most users of these modalities receive non-NHI treatment. 10 Thus, it was not possible to fully investigate the use of CAM in Japan using only data obtained from the NHI system. The use of the CSLC surveys permitted assessment of CAM use regardless of NHI use.
Exposure variables
Age was categorized into the following 18 groups; the median value was used for each group: 2.5 (0–5), 8.5 (6–11), 13 (12–14), 17 (15–19), 22 (20–24), 27 (25–29), 32 (30–34), 37 (35–39), 42 (40–44), 47 (45–49), 52 (50–54), 57 (55–59), 62 (60–64), 67 (65–69), 72 (70–74), 77 (75–79), 82 (80–84), and 87 (85 or older) years. In the survey, the information about age was collected in these categories. Period was categorized into 7 survey years. Cohort was categorized into twelve 10-year birth cohorts (from the 1900s to the 2010s).
The number of acupuncturists, moxibustion therapists, and judo therapists has increased in Japan since 2003; therefore, there has been an increase in the number of nationally licensed CAM providers. 11 This may affect the status of CAM provision in Japan. Therefore, differences between the period up and including 2002 and the period after and including 2003 were examined.
Outcome variable
On the questionnaire, participants were asked whether they had received any treatment for their primary symptom. Participants could select 37–45 symptom items, which differed depending on the year of the survey. The 2013 survey contained the following 43 symptoms: fever, dullness, insomnia, annoyance, forgetfulness, headache, dizziness, partial blindness, vision difficulties, tinnitus, hearing difficulties, palpitations, dyspnea, chest pain, cough, nasal congestion, breathing difficulties, sour stomach, diarrhea, constipation, anorexia, stomachache, hemorrhoids, toothache, swollen gums, difficulty chewing, rash, itching, stiff shoulder, low back pain, limb joint pain, poor movement of limbs, numbness, cold limbs, swollen legs, difficult urination, frequent urination, urinary incontinence, menstrual pain, fracture sprain, cuts or scalds, other, and unknown.
Because the symptoms on the questionnaire differed slightly between survey years, symptoms were categorized into 13 symptom groups (systemic, eye, ear, chest, respiratory, digestive, teeth, skin, muscles, limbs, urology, other, and unknown).
In this study, participants who had these symptoms and chose to go to a hospital/clinic in conjunction with CAM use were defined as “integrative” users, although “complementary” and “integrative” are often used interchangeably in the context of CAM use. Note that whether the participants accessed integrative care or simply accessed multiple modalities in this study cannot be confirmed.
Statistical analysis
The data had a multilevel structure that comprised individuals at level 1, and period and cohort at level 2. 12 An APC analysis was conducted using cross-classified multilevel logistic models, sometimes called a hierarchical APC modeling approach. 13
After examining the period- and cohort-level variances excluding any explanatory variables (empty model), age was entered as a level 1 explanatory variable to examine the relationship between age and outcome (model 1). Then, “2003 and after” was additionally included as a level 2 explanatory variable (model 2). All the analyses were stratified by sex. A sensitivity analysis was performed by including only musculoskeletal symptoms, which were the most frequently reported symptoms. 4
Bayesian inference was applied to estimate the parameters, using Markov chain Monte Carlo methods (burn-in 2500, Markov chain Monte Carlo sample size 10,000). Odds ratios (ORs) and 95% credible intervals (CIs) were obtained for each variable. Regarding period- and cohort-level variances, median ORs (MORs) were calculated. 14 If the MOR is 1, there is no variation between periods or cohorts. If there is considerable between-period variation or between-cohort variation, the MORs will be large. The measure is directly comparable with fixed-effects ORs. The deviance information criterion was used to compare the goodness-of-fit of each model. 15
All statistical analyses were performed using Stata version 16 (StataCorp LLC, College Station, TX).
Results
Of the total 753,978 participants, 17,707 CAM users (2.3%) were included in the analysis (Fig. 1). Table 1 gives the characteristics of the participants. Of the 17,707 CAM users, 11,567 (65.3%) were women, and the proportions of integrative use were 28.8% in 1995, 38.3% in 1998, 36.3% in 2001, 38.5% in 2004, 41.8% in 2007, 42.7% in 2010, and 40.8% in 2013. The most frequently reported symptom for which CAM treatment was sought was musculoskeletal problems, which accounted for half or more than half the cases in all survey years.
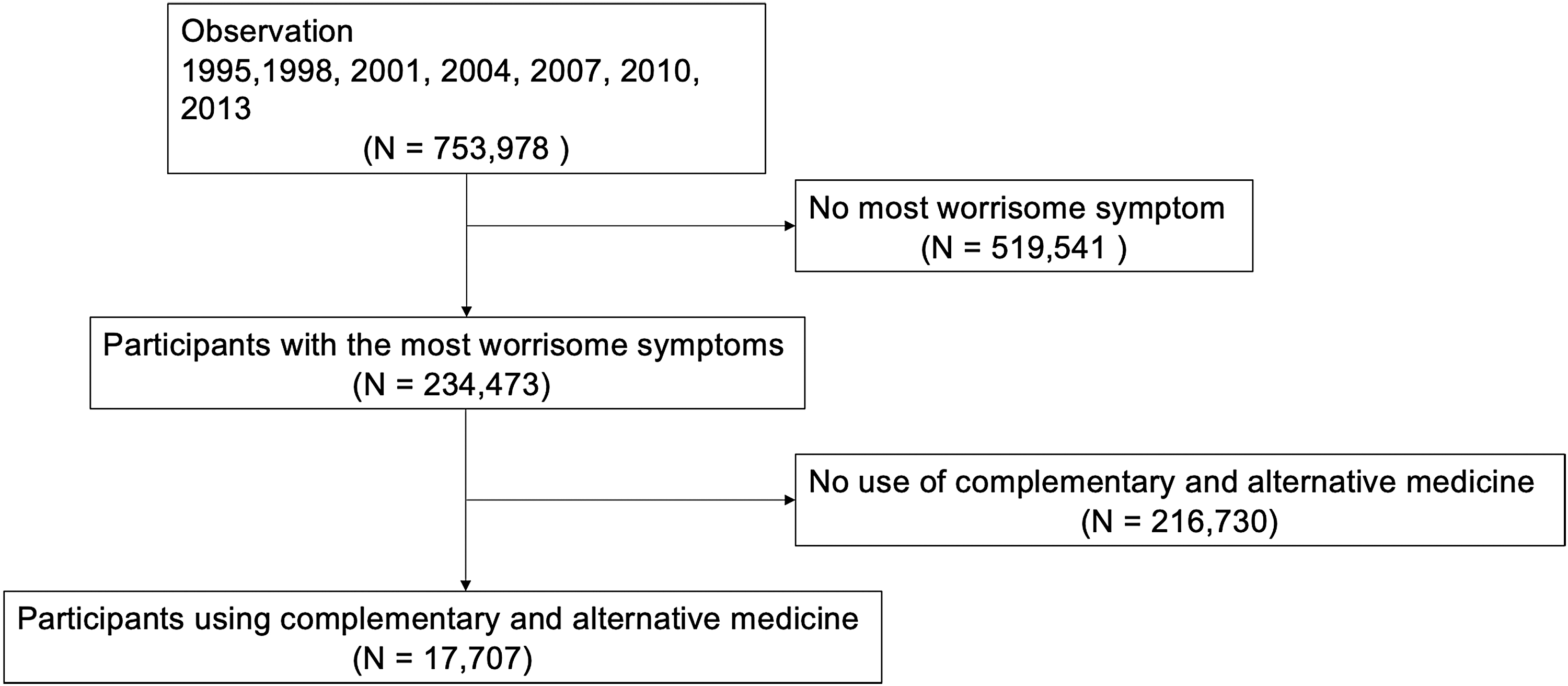
Participant flow.
Characteristics of Complementary and Alternative Medicine Users Between 1995 and 2013
CAM, complementary and alternative medicine.
The time trends of the proportion of integrative medicine use are shown in Figure 2a; there were no substantial changes during the study period. In both sexes, the proportions of integrative use tended to increase among older participants (Fig. 2b), whereas the proportions of integrative use decreased among the younger cohorts (Fig. 2c).
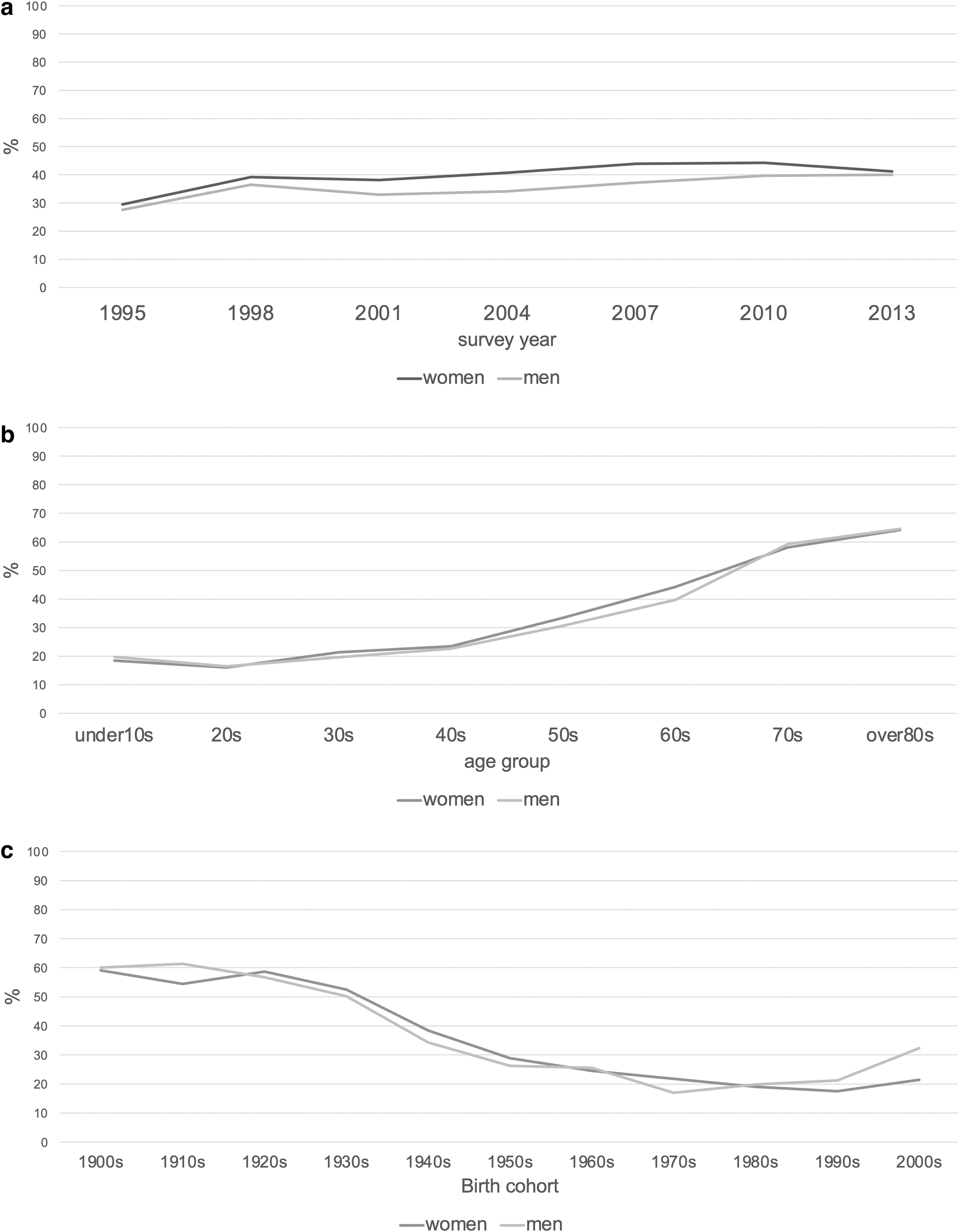
Prevalence of integrative CAM use.
Table 2 shows the ORs and 95% CIs for the association between integrative use and age, period, and cohort. In the empty model, the MORs for period and cohort were 1.60 (95% CI: 1.28–2.32) and 2.83 (95% CI: 1.9–4.93), respectively, among women. The corresponding MORs among men were 1.58 (95% CI: 1.26–2.28) and 2.61 (95% CI: 1.77–4.70). When age was entered as an explanatory variable (model 1), the ORs were 1.04 (95% CI: 1.03–1.04) for women and 1.03 (95% CI: 1.02–1.04) for men. Finally, when the possible period effect for 2003 and after was additionally examined (model 2), the ORs were 1.36 (95% CI: 0.89–1.99) for women and 1.37 (95% CI: 0.94–1.91) for men.
The Odds Ratios for Integrative Use with Age, Period, and Cohort Effects
CI, credible interval; MOR, median odds ratio; OR, odds ratio; SD, standard deviation.
When only the most frequently reported (musculoskeletal) symptoms were included (Table 3), the OR for 2003 and after was significant for men (OR: 1.32, 95% CI: 1.00–1.83), but was slightly attenuated for women (OR: 1.14, 95% CI: 0.88–1.52).
The Odds Ratios for Integrative Use for Musculoskeletal Problems with Age, Period, and Cohort Effects
The deviance information criterion values were almost the same in the three models for both women and men.
Discussion
The present findings suggest that the integrative use of CAM in Japan increased in both men and women during the study period, which is consistent with the NCCIH and WHO strategies. Given that integrative use is a safe and effective way to use CAM, the present findings have important implications for CAM use in Japan. For both women and men, integrative CAM use increased with age. In particular, electroacupuncture reportedly has better cost–utility results than nonsteroidal anti-inflammatory drugs, 16 and its integrative use may help to reduce health care costs. Further research is needed on this issue.
A previous study reported that 12.8% of Japanese used CAM in the past 12 months in 2016. 3 By contrast, of the 753,978 subjects in this survey, only 17,707 (i.e., 2.3%) were CAM users. One possible reason of this discrepancy may be the different age structure; this survey was conducted for all ages, whereas the previous study was conducted for ages 20 years and older. In addition, the questionnaire used in this study asked “attending an anma-massage-shiatsu, acupuncture, moxibustion, or judo therapy session” as CAM. Thus, there is a possibility that other CAM users were not included in the sample, which may well explain the low proportion in this study.
As mentioned in the Methods section, the number of people who have obtained national certification in CAM has increased since 2003, which may have led to a decline in the quality of certified personnel. 11 However, the present findings suggest that integrative CAM use increased after 2003 in both women and men (ORs, 1.36 and 1.37, respectively); this may suggest that owing to the greater number of CAM-certified personnel, CAM accessibility improved, especially among more health-conscious individuals.
Furthermore, the findings may be interpreted a posteriori from a medical practice perspective; for example, some CAM-certified personnel may have recommended that their patients visit a hospital/clinic, whereas some medical doctors may have recommended that their patients use integrative CAM. Some practitioners may consider this type of referral exchange to be beneficial for their business. In either case, the possibility that the increased number of CAM-certified personnel led to lower CAM quality cannot be excluded, and further studies are warranted to examine the quality of CAM-certified personnel.
A sensitivity analysis was also performed to examine the associations, including only the most frequently reported symptoms (musculoskeletal symptoms) (Table 3). The fact that judo therapists are only qualified to treat musculoskeletal symptoms may have affected the results. However, acupuncture and moxibustion are most frequently used to treat musculoskeletal symptoms in Japan; 10 therefore, these results are probably representative of CAM users in general.
This study featured anonymous data derived from a nationwide survey in Japan, which is a strength of the study. Very few studies have examined integrative CAM use, and there are few large-scale studies with samples representative of the whole country. Given the growing interest in integrative health and CAM use, it is important to examine the time trends in other countries in future studies.
There are several study limitations. First, because a single question was used to assess the use of acupuncturists, moxibustion therapists, anma-massage-shiatsu therapists, and judo therapists, these CAM modalities could not be evaluated separately. Separate analyses of the use of these modalities are needed because they may be used for different reasons. Second, this study investigated the use of CAM in combination with conventional medicine for the same symptoms. Respondents were asked to report multiple subjective symptoms and to report which type of medical treatment they had sought for the symptom that was most worrisome.
However, it is possible that participants with many subjective symptoms (e.g., older people) selected conventional medicine if they were already using this for another symptom. This may have led to differential misclassification and the overestimation of integrative use. Third, no adjustment was made for education or income, which have been considered to be potential confounders in previous studies. 2,3 Data on education are only available after 2010, and information about annual income was not used owing to the small sample size.
In addition, the possibility of unmeasured confounding cannot be excluded. Finally, it has been argued that APC analysis using cross-classified multilevel models does not solve the identification problem. 17,18 Therefore, it is conceivable that the present APC analysis may be characterized by identification problems.
Conclusions
The integrative use of CAM in Japan increased from 1995 to 2013, which is consistent with the NCCIH and the WHO strategies. For both sexes, older people tended to use integrative CAM. Despite some previous concerns, the increase in the number of national CAM certifications since 2003 was associated with more integrative CAM use, although a concern about the low quality of CAM personnel remains. The results did not substantially change when the analysis included only participants with musculoskeletal symptoms as the main complaint for which CAM was used. Because CAM systems vary widely from country to country, further studies are warranted to examine integrative CAM use in other countries.
Footnotes
Acknowledgments
The authors are grateful to Saori Irie for her valuable support in collecting data. The authors thank Diane Williams, PhD, from Edanz for editing a draft of this article.
Authors' Contributions
N.M. contributed to conceptualization, formal analysis, writing—original draft, and funding acquisition. E.S. was involved in methodology and writing—review and editing. T.M. was in charge of software and writing—review and editing. S.T. took charge of writing—review and editing. T.Y. was responsible for writing—review and editing, data curation, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Okayama Medical Research Association grant R02-01.