
Abstract
Objectives:
The aim of this study was to evaluate the impact of acupuncture on hot flashes in breast cancer patients taking tamoxifen as an adjuvant antiestrogen therapy in Korea.
Design:
This trial was a randomized, no-treatment-controlled, single-blind, multi-center trial. Participants were randomized 1:1 into the acupuncture group or into the no-treatment control group.
Location:
This trial was conducted at Daegu Catholic University Hospital and Daegu Haany University Korean Medicine Hospital in Daegu, Republic of Korea.
Participants:
Patients with moderate to severe symptoms of hot flashes while receiving adjuvant antiestrogen therapy using tamoxifen after surgery for breast cancer were included.
Interventions:
In the acupuncture group, acupuncture was performed three times a week for 4 consecutive weeks at five predetermined points. The control group received no treatment during the study period.
Study Outcome Measures:
As a primary outcome, the severity of hot flashes was measured on the visual analogue scale (VAS) and total hot flash score. In addition, the quality of life (QoL) of participants was assessed as a secondary outcome.
Results:
A total of 30 patients were included in this study, 15 each in the acupuncture group and the control group. The participants in the acupuncture group significantly decreased the severity of hot flashes evaluated with both VAS and total hot flash scores compared with participants in the control group. Also, the acupuncture group showed improved score of a global health status/QoL scale and functional scales assessed with the European Organisation for Research and Treatment of Cancer QoL questionnaire—core questionnaire, compared with those in the control group. This trend was maintained 4 weeks after acupuncture treatment. No adverse events have been reported in this study.
Conclusions:
Acupuncture was effective and safe in improving hot flashes in Korean breast cancer patients receiving adjuvant antiestrogen therapy with tamoxifen, and it improved the QoL.
Clinical Trial Registration:
KCT0007829.
Introduction
Breast cancer is the most common cancer in Korea and worldwide in women. 1,2 Treatment of breast cancer is determined based on clinicopathologic characteristics and biologic factors. In particular, antiestrogen therapy, including tamoxifen, is recognized as the standard treatment for hormone receptor-positive breast cancer. 3 Tamoxifen helps reduce breast cancer recurrence and mortality in hormone receptor-positive breast cancer, but it has several side effects. 4
Among the side effects of tamoxifen, hot flashes are the most common. Hot flashes are a sudden, intense sensation of body warmth or heat on face and can be accompanied by sweating. 5 Hot flashes can cause poor sleep quality, mood change, and increased fatigue, and affect quality of life (QoL). 6,7 Hormone replacement therapy (HRT) is one of the methods to alleviate hot flashes in healthy postmenopausal women, but breast cancer patients are prohibited due to the risk of tumor recurrence. 8,9
Several non-hormonal strategies including the complementary and alternative medicine (CAM) have been evaluated to manage hot flashes in breast cancer patients. 10 However, these drugs are also associated with several side effects. In addition, there is a lack of research on the effectiveness of CAM on hot flashes other than acupuncture. 10
Previous studies have shown that acupuncture improves hot flashes in healthy women. 11,12 In addition, several studies have suggested the effect of acupuncture on hot flashes of breast cancer patients. 13,14 Our previous pilot study also showed the feasibility of acupuncture to alleviate hot flashes in breast cancer receiving antiestrogen therapy. 15
Nevertheless, recent studies have not yet provided convincing evidence to support the effect of acupuncture on hot flashes in breast cancer patients, and further studies are needed. 16,17 The aim of this study was to evaluate the impact of acupuncture on hot flashes in breast cancer patients receiving adjuvant antiestrogen therapy with tamoxifen in Korea.
Materials and Methods
Trial design
This trial was a randomized, no-treatment-controlled, single-blind, multi-center trial. The study was conducted at Daegu Catholic University Hospital and Daegu Haany University Korean Medicine Hospital in Daegu, Republic of Korea. Ethical approval for this study was obtained from the Institutional Review Board of each institution. The study protocol included 12 acupuncture sessions over 4 weeks, at five predetermined points in the acupuncture group. The control group received no treatment during the study period.
The severity of hot flashes was measured as a primary outcome, and the QoL was measured as a secondary outcome. The protocol has been registered with the Korea Clinical Research Information Service (Registration number: KCT0007829; URL:
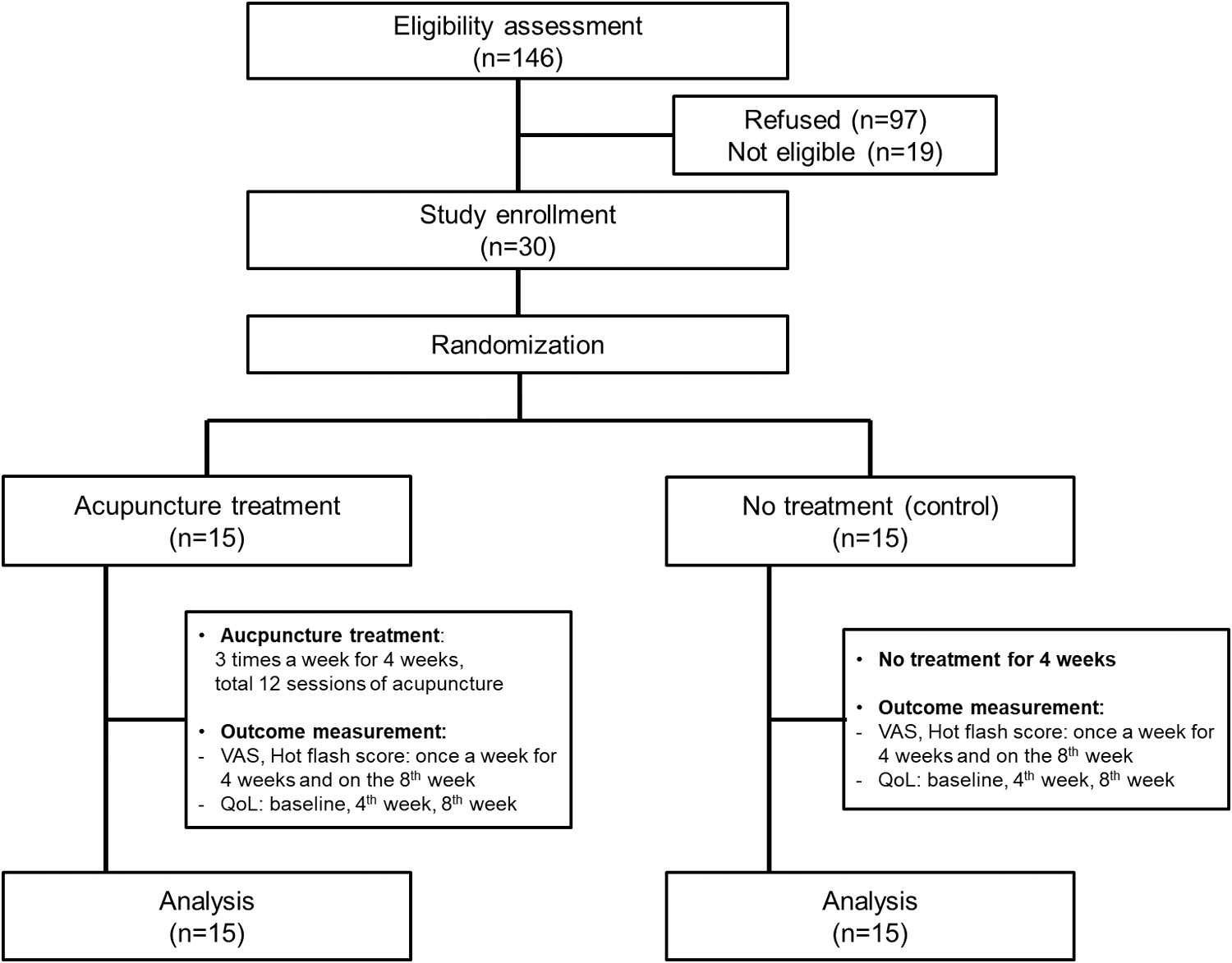
A study design and participant flow. VAS, visual analogue scale.
Participants
Written informed consent was obtained from all patients before participant registration in accordance with the clinical trial protocol. The recruitment of subjects was conducted from April 2017 to June 2017, and investigators from two institutions registered a total of 30 patients. Participants from each of the two institutions were randomized 1:1 into the acupuncture group or into a no-treatment control group. The random sequence was generated based on the permutation blocking technique by a statistician of School of Medicine, Daegu Catholic University.
The allocation code was placed in opaque envelopes numbered sequentially by the statistician and sealed. Each study participant was blinded and assigned to a corresponding group according to the results of randomization. The inclusion criteria were as follows: (1) adjuvant antiestrogen therapy using tamoxifen after surgery for breast cancer; (2) moderate to severe symptoms of hot flashes defined in the Food and Drug Administration; (3) 3 or more hot flashes during the week before screening; (4) voluntary participation; (5) Karnofsky performance status score of >60; (6) follow-up is possible during the study period; and (7) discontinuation of HRT or other pharmacological or alternative treatments for hot flashes at least 4 weeks before screening. 15,18
The criteria for exclusion were as follows: (1) other pharmacological or alternative treatment for hot flashes during the study period; (2) severe medical or psychiatric conditions that make participation in the trial inappropriate; and (3) hot flashes due to menopause, not antiestrogen therapy.
In the acupuncture group, acupuncture was performed three times a week for 4 consecutive weeks at five predetermined points. The control group received no treatment during the study period.
Interventions
In the acupuncture group, acupuncture was performed three times a week for 4 consecutive weeks. Acupuncture was performed by government-registered acupuncture specialists, traditional Korean medicine (TKM) physicians. Acupuncture points were selected according to the recommendations of TKM clinical experts and standard acupuncture textbooks 19 –23 (Table 1).
Acupuncture Points Prescriptions and Their Anatomical Position
The acupuncture treatment time was about 25 min for each treatment. We used a total of 8 sterile disposable stainless-steel needles for each acupuncture treatment. Before each acupuncture, the skin was cleaned and disinfected with an alcohol preparation pad. The acupuncture method was the same as in previous studies. 24 –26 Briefly, the needles were inserted into the skin at a depth of 5–10 mm at the predetermined acupuncture points and the needles were manually manipulated to obtain de qi. 24 –26
Ten minutes after initial insertion of the needles, the acupuncturist manipulated the needles using techniques, including rotating, lifting, and thrusting without evoking needle sensation to maintain the intensity of the de qi (obtaining qi) sensations.
The control group only performed the usual care for breast cancer during the study period and received no other treatment for hot flashes.
Study outcome measures
As a primary outcome, the severity of hot flashes was measured on the visual analogue scale (VAS) and total hot flash score. The VAS and total hot flash score were evaluated once before acupuncture treatment, once every week for 4 weeks during acupuncture treatment, and once after acupuncture treatment, a total of 6 times. The control group was evaluated before the start of the study, once every week for the first 4 weeks after participation in the study, and once on the 8th week. Participants used VAS to record the average hot flash severity over the past week. The VAS results recorded by participants were converted to scores between 0 and 100, as described in our previous study. 15
The secondary outcome measure was the QoL of the participants. To evaluate QoL, the European Organisation for Research and Treatment of Cancer (EORTC) QoL questionnaire—core questionnaire (EORTC QLQ-C30) version 3.0 27,28 and breast cancer module (EORTC QLQ-BR23) were used as tools. The survey using these questionnaires were conducted a total of three times before the start of the study, at the 4th week after participation in the study, and at the 8th week.
The EORTC QLQ-C30 version 3.0 incorporates 30items, including functional scales, symptom scales, a global health status/QoL scale, and six single items. 29 The EORTC QLQ-BR23 is a module of 23 questions to evaluate symptoms of breast cancer, breast cancer treatment-related symptoms, and additional QoL domains affected by breast cancer or treatment. 30 All responses were analyzed for each item after calculating the score according to the manual. 31
Statistical analysis
Sample-size calculations were based on previous pilot studies. 15,32 We assumed an intervention effect difference on hot flash score of 2.11 and a standard deviation of 1.92. The power of the study was 80%, and the significant level of two-sided Type I error was set at 5%. Assuming a 10% loss of the participants, a sample size of 30 participants was calculated. This study used an intention-to-treat analysis to analyze the results.
The change in the severity of hot flash was analyzed using the repeated-measures one-factor analysis. For each participant, the average daily VAS value and total hot flash score were calculated for 14 days of visit using student t-tests or Mann–Whitney U test. A repeated-measures analysis of variance was used to analyze the overall changes in the VAS values, total hot flash scores over time, and participants' QoL changes.
To analyze the outcomes of acupuncture treatment, differences between groups, differences between time points, and changes according to time points between groups were compared. In this study, the SPSS statistical package, version 21.0 (SPSS Inc., Chicago, IL) was used for statistical analysis. Since there were two primary outcomes in this study, the p-value of <0.025 was designated as significant in comparing the primary outcomes between the two groups to protect against a Type I statistical error. For other results, the p-value of <0.05 was analyzed to be statistically significant.
Results
Baseline characteristics
A total of 30 subjects were registered from two institutions for this study. All participants completed the trial, and there was no dropout. The mean age was 47.5 ± 5.7 years (range, 29–56) for all participants. Although the mean age of the participants was younger than 50 years, the proportion of postmenopausal status was relatively high because amenorrhea was induced by chemotherapy in most of premenopausal women. Table 2 showed the demographic characteristics and clinical findings of the participants.
Demographic and Clinical Characteristics at Baseline
BMI, body mass index; SD, standard deviation.
Impacts of acupuncture on the severity of hot flashes in participants
The primary end point was the severity of hot flashes. All participants completed the outcomes measures during the study periods, and there were no missing values to be handled. Both the VAS value and total hot flash score of the acupuncture group measured at the end of acupuncture treatment were significantly reduced compared with the control group (p < 0.001 and p = 0.008, respectively), showing a significant decrease in the severity of hot flashes, which was the primary endpoint.
When analyzed only in the acupuncture group, the mean VAS value decreased significantly over time (p < 0.001), but no interval change of total hot flash score was observed over time (p = 0.978). Even after 4 weeks after completion of acupuncture in the acupuncture group, the improved hot flashes did not worsen again and was maintained in the acupuncture group. Table 3 and Figure 2 showed the changes in the average VAS value and total hot flash score of the participants during the study period.
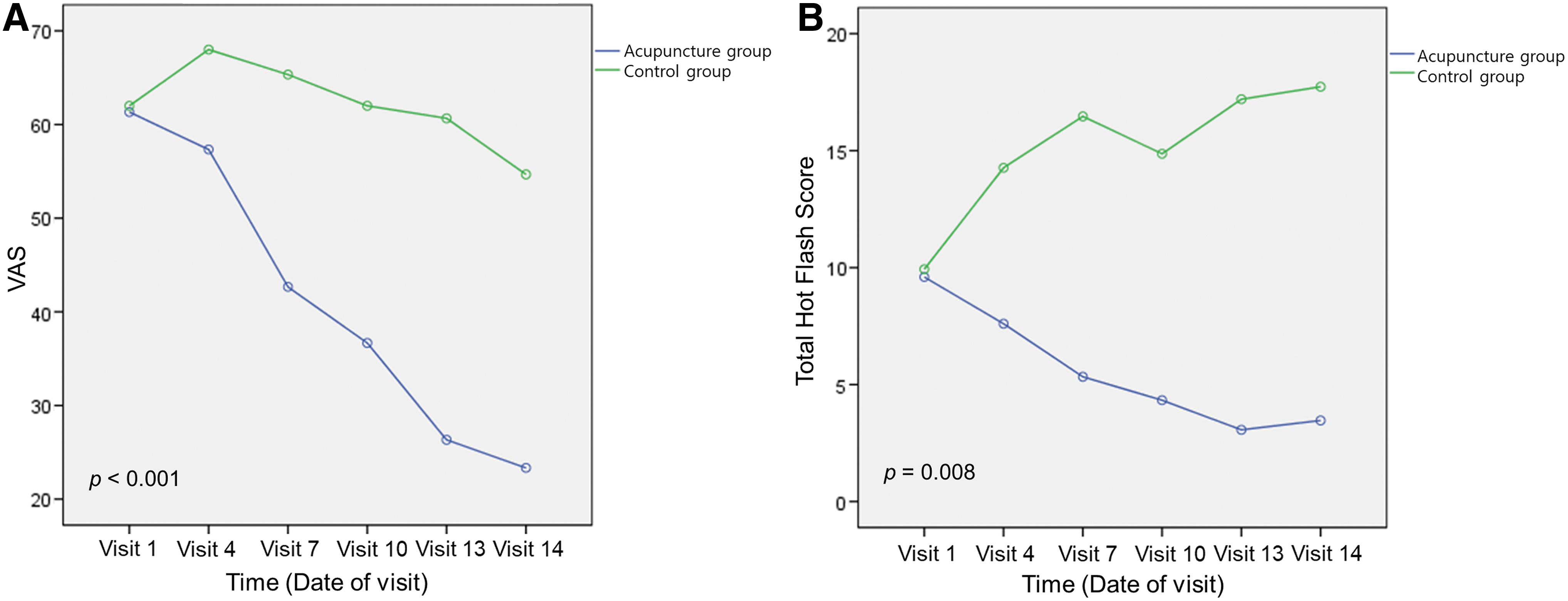
Changes in mean VAS and total hot flash score from baseline to 4 weeks after the final acupuncture session.
Mean Values of Visual Analogue Scale and Total Hot Flash Scores from Baseline to 4 Weeks After the Final Acupuncture Session
Statistically significant with p < 0.025.
Multiple comparison result by contrast
Visit 1 > Visit 4, Visit 7, Visit 10, Visit 13, Visit 14.
Visit1 ≠ Visit 4, Visit 7, Visit 10, Visit 13, Visit 14.
SD, standard deviation; VAS, visual analogue scale.
Impact of acupuncture on the participants' QoL
The secondary endpoint, QoL of the participants was analyzed using the EORTC QLQ-C30 and the EORTC QLQ-BR23 questionnaire. The acupuncture group demonstrated improved scores on the functional scales as well as the global health status/QoL scale in the evaluation using the EORTC QLQ-C30 questionnaire, compared with the control arm (p = 0.004 and p = 0.027, respectively) (Table 4; Fig. 3).
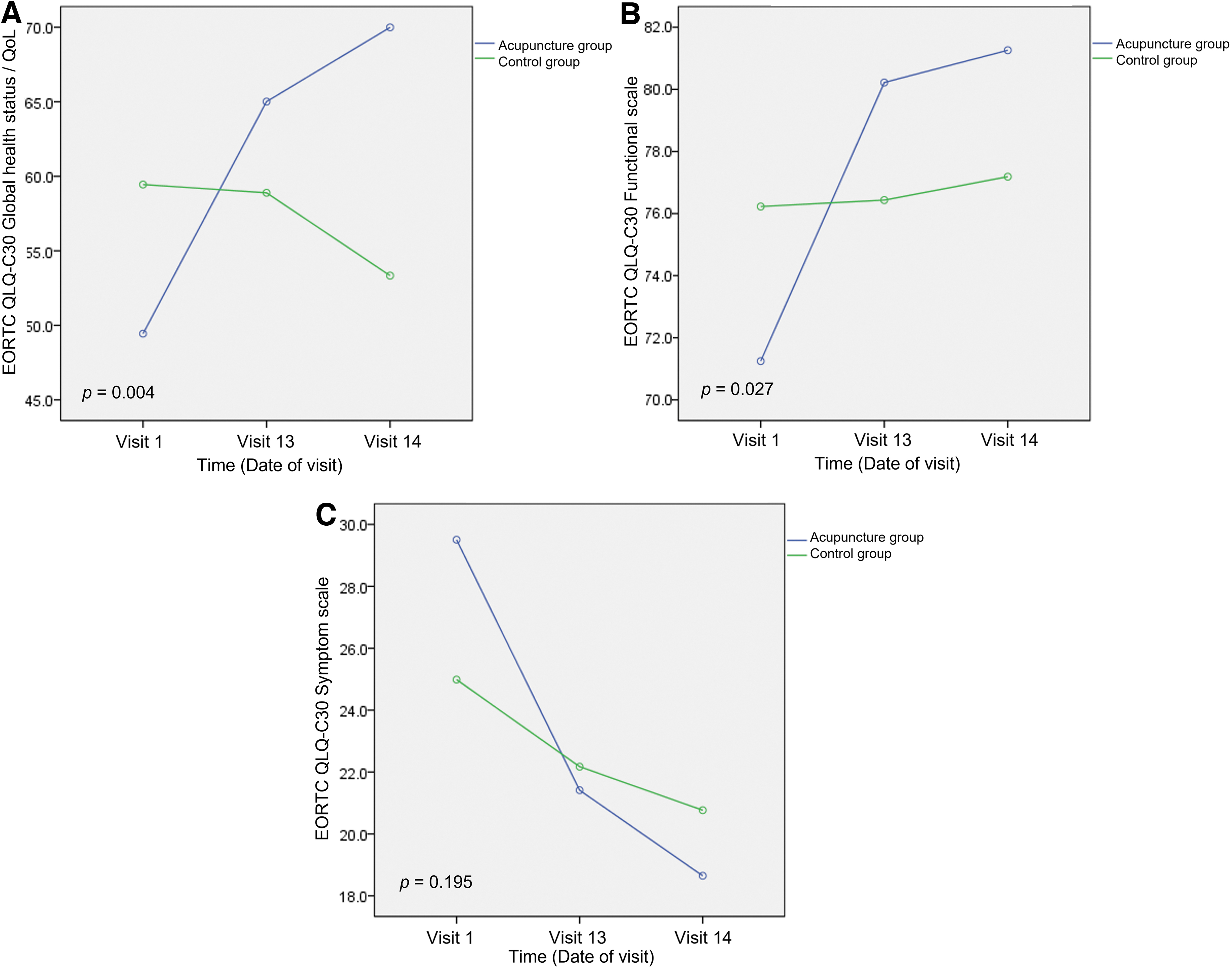
Changes in mean scores of the EORTC QLQ-C30 over time.
Quality of Life of Breast Cancer Patients Assessed with the EORTC QLQ-C30 Questionnaire from Baseline to 4 Weeks After the Final Acupuncture Session
Statistically significant with p < 0.05.
Multiple comparison result by contrast.
Visit 1 ≠ Visit 13, Visit 14.
Visit 1 < Visit 13, Visit 14.
Visit 1 > Visit 13 > Visit 14.
QoL, quality of life; SD, standard deviation.
However, there was no significant difference in the change in the EORTC QLQ-BR23 score over time between the two groups (Table 5). As a result of repeated-measures ANOVA performed alone in the acupuncture group, the functional scales and symptom scales of the EORTC QLQ-C30 showed significant improvement over time (p = 0.009 and p = 0.001, respectively). In addition, the functional scales and symptom scales of the EORTC QLQ-BR23 showed significant improvement in the acupuncture group alone (p = 0.036 and p = 0.001, respectively).
Quality of Life of Breast Cancer Patients Assessed with the EORTC QLQ-BR23 Questionnaire from Baseline to 4 Weeks After the Final Acupuncture Session
Statistically significant with p < 0.05.
Multiple comparison result by contrast.
Visit 1 > Visit 13 > Visit 14.
Visit 1 > Visit 13, Visit 14.
SD, standard deviation.
Safety
In the study participants, the compliance rate was good at 100%. Acupuncture was well tolerated with any side effects. During the study periods, neither serious nor non-severe adverse events were noted in all participants.
Discussion
In this randomized, no-treatment-controlled, single-blind, multi-center trial, we observed that acupuncture treatment significantly reduced the severity of hot flashes in patients with breast cancer taking tamoxifen as an adjuvant antiestrogen therapy. This result confirms the feasibility of acupuncture in improving hot flashes in breast cancer patients shown in our previous single-arm pilot study. 15 In addition, as shown in previous studies, 14,33 –37 acupuncture significantly improved QoL in breast cancer patients receiving adjuvant antiestrogen therapy in this study.
Recently, several studies have investigated the effects of acupuncture on breast cancer-related symptoms. Especially, there are randomized controlled trials (RCTs) that showed the effect of acupuncture on reducing hot flashes in breast cancer patients (Table 6). 13,14,33 –44 A meta-analysis, including 11 RCTs, demonstrated that the hot flashes score in the acupuncture group differed significantly compared with the control groups (p = 0.04). 45
Overview of Randomized, Controlled Trials of Acupuncture for the Treatment of Hot Flashes in Breast Cancer Patients
BDI-PC, Beck Depression Inventory-Primary Care; CESD, Center for Epidemiological Studies Depression; EA, electroacupuncture; EORTC QLQ-BR23, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire—Breast cancer module; EORTC QLQ-C30, European Organisation For Research and Treatment of Cancer Quality of Life Questionnaire—Core questionnaire; EuroQoL, European quality-of-life survey; GCS, Greene Climacteric Scale; HADS, Hospital Anxiety and Depression Scale; HFCS, hot flash composites score; HFRDI, Hot Flash Related Daily Interference; KI, Kupperman index; MenQoL, Menopause Quality of Life; NA, not assessed; NSABP, National Surgical Adjuvant Breast and Bowel Project; PGWB, Psychological and General Well-Being Index; PSQI, Pittsburgh Sleep Quality Index; QoL, quality of life; SA, sham acupuncture; SF-12, Short Form-12 Item Survey; TA, traditional acupuncture; VAS, Visual Analog Scale; WHQ, Women's Health Questionnaire.
Another meta-analysis showed that acupuncture did not significantly reduce the frequency or the severity of hot flashes (p = 0.34 and p = 0.33, respectively). 16 Nevertheless, there was considerable heterogeneity among these studies and the effects of acupuncture on the hot flashes remain controversial. 16 In several RCTs, sham acupuncture was applied as a control and no significant difference was shown in the hot flashes changes between each groups, although acupuncture improved hot flashes. 38 –40,42
Nevertheless, there were very few no-treatment controlled RCTs. In this regard, we used a no-treatment control to clearly compare the effects of acupuncture. In our study, acupuncture treatment significantly improved hot flashes, whereas there was no change in the control group.
Hot flashes affect the QoL of women with breast cancer compared with the absence of hot flashes. 33 Several RCTs investigated the impact of acupuncture on the QoL in breast cancer patients who suffered from hot flashes and showed improved QoL after acupuncture treatment. 14,33 –37 Zhang et al meta-analyzed RCTs and showed that they significantly improved QoL after acupuncture. 45 Meanwhile, Bao et al found no significant change of QoL after acupuncture in these patients, whereas there were significant changes of QoL in the sham acupuncture group. 38
The authors explained that the small number of subjects included in the trial may have made it difficult to find between-group differences. 38 As most studies have shown, our study also showed that acupuncture helps to improve the QoL. In particular, in the acupuncture group, the global health status/QoL scale and functional scales of the EORTC QLQ-C30, and the symptom scales of the EORTC QLQ-BR23 were significantly improved.
Our findings suggest that acupuncture not only improves the QoL by reducing hot flashes in breast cancer patients suffering from hot flashes, but also acupuncture itself can help directly improve the QoL.
The mechanisms for how acupuncture improves hot flashes and QoL in breast cancer patients are not well established. As suggested in previous studies, one mechanism may be that acupuncture treatment can mediate the modulation of autonomic nerve system and anti-inflammatory effects by regulating inflammatory cytokines. 46,47 Inflammation has been recognized as being involved in tumorigenesis by regulation of cytokines. 48
In addition, it has been suggested that hot flashes are associated with inflammation. 49 Thus, we hypothesized that acupuncture may modulate inflammation and improve hot flashes severity as well as QoL in breast cancer patients. To clarify this mechanism, it is necessary to study the relationship between changes in inflammatory cytokines after acupuncture and improvement of hot flashes and QoL in breast cancer patients.
In acupuncture studies, participant compliance may vary depending on the protocol, including acupuncture treatment periods. In previous studies, acupuncture treatment periods varied from 4 to 12 weeks, and most of the acupuncture treatments were performed 1–2 times a week (Table 6). Participants' compliance was 82%–94% in the RCTs with acupuncture for 12 weeks, and 88%–100% in the RCTs with a shorter period of acupuncture.
Deng et al showed that hot flashes decreased even after acupuncture treatment for 4 weeks, with good compliance at 97%. 40 In our study, acupuncture was administered for a total of 4 weeks with the same protocol as our previous study, to determine the effectiveness of short-term treatment and increase patient compliance. As a result of the study, 4 weeks of acupuncture were also effective in hot flashes and the compliance was excellent at 100%.
In addition, we noticed the effect of maintaining up to 4 weeks after the end of treatment, indicating that the impact of acupuncture treatment is not only temporary during treatment. Our findings support that short-term acupuncture can be applied in patients to improve hot flashes even if the acupuncture period is not long, and the shorter duration provides good compliance, making it suitable for clinical application.
Acupuncture has been reported to be safe in previous studies. Mild side effects, including minor bleeding on the acupuncture site, bruising, muscle pain, headache, fatigue, pruritus, and nausea, were reported in several studies, and there were no serious side effects reported. 33,40,42 In our study, no side effects were noted after acupuncture, suggesting that acupuncture can be safely applied in breast cancer patients.
There are several limitations in our study that need to be acknowledged. First, this study has a limitation in generalizing the results of the study because the number of participants was small, and it was conducted with single blinds. To overcome this limitation, large double-blind RCTs will be needed. Second, the follow-up period after completion of acupuncture treatment is as short as 4 weeks, so there is a limit to confirm the long-term effect of acupuncture.
In general, anti-estrogen therapy for breast cancer requires 5 to 10 years. Therefore, it is important to analyze the duration of the improvement of hot flashes after acupuncture in these patients, and it is necessary to conduct long-term follow-up studies. Third, although hot flashes are generally evaluated using subjective symptoms, objective tools for evaluating hot flashes were not included and the placebo effect of acupuncture cannot be excluded.
Further studies using validated objective measures are needed to more reliably analyze the impact of acupuncture. Fourth, the participants included in this study are all Korean women. To determine the impact of acupuncture, it is necessary to analyze the difference in the effects of acupuncture treatment according to racial and cultural differences through a large-scale multinational study. Nevertheless, to the best of our knowledge, this study is the first RCT to demonstrate the effect of a short period of acupuncture treatment of 4 weeks on hot flashes and the QoL in breast cancer patients taking tamoxifen.
Conclusions
Our results demonstrated that acupuncture not only effectively reduces hot flashes in breast cancer patients receiving adjuvant antiestrogen therapy with tamoxifen, but also helps improve QoL. Acupuncture can be clinically recommended for improving hot flashes and QoL in patients with breast cancer. In addition, it is also suggested that 12 acupuncture treatments over 4 weeks, the protocol of this study, can be used as a practical approach.
To confirm the impact of acupuncture on hot flashes and to determine a standardized acupuncture protocol in patients with breast cancer, further studies are needed to include sufficient subjects, compare various protocols, and follow up for a long time.
Footnotes
Acknowledgments
The authors thank Dr. Min Ah Kwak for helpful discussions regarding study design and valuable advice, Drs. Yuri Lee and Seo Young Park for the acupuncture treatment and practical assistance.
Authors' Contributions
All authors contributed to the article and approved the submitted version. Y.J.J.: Conceptualization, data curation, investigation, resources, validation, visualization, and writing—original draft (lead). H.R.C.: Data curation, investigation, resources, visualization, and writing—original draft (supporting). K.-S.K.: Conceptualization, data curation, funding acquisition, investigation, methodology, resources, and writing—review and editing (equal). I.H.S.: Conceptualization, formal analysis, funding acquisition, methodology, project administration, validation, and writing—review and editing (equal). S.H.P.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, and writing—review and editing (equal).
Protocol Availability
The full trial protocol for access is available at the Comprehensive and Integrative Medicine Institute data archive.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This study was supported by a grant of the Ministry of Health and Welfare, Republic of Korea (Project No: 090-091-3000-3038-301-320-01).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.