
Abstract
Background:
Despite the reported benefits of evidence-based practice (EBP), there are concerns that some practitioners, including naturopathic doctors (NDs), may be cautious about its use. The objective of this study was to explore Canadian ND perceptions, preparedness, and engagement in EBP, and the barriers and enablers to EBP uptake.
Methods:
The study was a national cross-sectional survey. NDs practicing in Canada were invited to complete the validated 84-item Evidence-Based Practice Attitudes and Utilization Survey between February and May 2020.
Results:
A total of 252 Canadian NDs were recruited. Participant attitudes toward EBP were predominantly positive, with three-quarters of participants indicating that >50% of their practice was informed by clinical research evidence. One-half of participants self-reported a medium-high to high level of skill across most EBP-related activities. Notable barriers to EBP uptake were lack of clinical evidence in naturopathy, and lack of time. Access to the internet and online databases were identified as useful enablers to improving EBP engagement.
Conclusions:
By shedding light on Canadian ND engagement with, preparedness for, and perceptions of EBP, the findings will help guide the development of strategies to support EBP uptake in NDs with the expectation of improving quality of care.
Introduction
Evidence-based practice (EBP) emerged from growing concerns that research evidence was not influencing clinical decision-making in a timely and consistent manner. The EBP framework, which was designed to foster the delivery of best practice care, 1 expanded the type of knowledge used in clinical encounters to include three tenets: use of the “best available” research evidence in combination with clinical expertise and patient preferences. 1 EBP also encouraged a shift away from being dependent on anecdotal accounts, traditional knowledge/practices, and theoretical reasoning, to placing greater emphasis on the use of evidence from high-quality studies when the latter reflects the “best available” evidence. 2
There is mounting evidence to suggest that the adoption of EBPs is associated with improvements in health outcomes, patient satisfaction, and health care expenditure. 3,4 Despite these reported advantages, many groups of health professionals have been resistant to adopting EBP, expressing concerns that EBP devalues clinician experience, and fails to consider the difficulties in translating research findings into complex, real-world situations. 2 Conversely, several studies have shown members of some professions to be largely supportive of EBP, including chiropractic, 5,6 osteopathy, 7,8 medicine, 9 and physiotherapy. 10 That said, little is known about the attitudes of naturopathic doctors (NDs) toward EBP. Understanding the EBP landscape in naturopathic medicine (NM) is an important first step to recognizing what, if any, EBP skills and behaviors require attention in this profession. 11,12
NM is an eclectic health discipline that blends traditional and natural therapeutic strategies with contemporary scientific knowledge to support the prevention and management of diverse health conditions. The practice is underpinned by a set of principles that aim to create a coherent approach to care, including treating the whole person, treating the underlying cause of illness, and supporting the body's self-healing processes. 13 The critical analysis of accumulated knowledge is a more recently proposed principle of NM, 14 yet there are some indications that NDs may be cautious about embracing EBP. In Australia, some naturopathic practitioners have branded EBP as a threat to the integrity of naturopathic practice, 15 and in North America, NDs have expressed concern that EBP may be used as a tool to discredit naturopathic practices. 16
Notwithstanding, a qualitative study of North American NDs suggests that these attitudes may be in flux, with perceptions of EBP possibly shifting from one of hesitancy to one of cautious embrace. 16
In Canada, NM is regulated in six provinces. 17 To be registered as an ND in Canada, an individual must complete an undergraduate degree as well as a 4-year naturopathic medical program at an accredited institution. These programs typically include training in basic science, diagnosis, and naturopathic and conventional treatment approaches. 14 To practice as an ND in Canada, graduates must also successfully complete licensing and provincial board examinations. Given the duration and scientific content of Canadian ND training, and the licensure requirements to practice NM in Canada, one might assume that Canadian NDs would be adequately prepared for, and supportive of, EBP.
The only known study to explore Canadian ND perceptions of EBP is a survey conducted in 2018, 18 which sought to explore the capacity and needs of the profession in relation to research participation. Participants reported a high level of agreement (84%–100%) with statements related to the importance of critical evaluation, defining outcomes and using evidence to improve clinical care. Participants also rated highly their confidence in formulating a research question, performing a literature review and appraising research evidence. Notwithstanding, the primary objective of this earlier study was to explore ND interest in participating in research, thus disregarding the other tenets of EBP (i.e., clinical expertise and patient preference). As such, no previous study has been undertaken with the primary aim of capturing Canadian ND perceptions, preparedness, and engagement with EBP.
Methods
Design
The project was a national cross-sectional survey of self-selected Canadian NDs. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 19
Objectives
The objectives of this project were to examine Canadian ND (1) engagement in EBP activities, (2) preparedness for EBP, (3) perceptions of EBP, (4) barriers and enablers of EBP uptake, and (5) the association between Canadian ND demographic/practice variables, and EBP engagement, preparedness, and perceptions.
Participants
All NDs practicing in Canada, who were fluent in the English language, were eligible to participate in the survey. Based on a 6% margin of error with 95% confidence for any individual item on the survey, and a target population of 2400 Canadian NDs, 20 the project required a sample size of at least 241 participants.
Methods
The Evidence-Based practice Attitude and utilization Survey (EBASE) is an 84-item self-administered instrument designed to assess 6 constructs related to EBP: use [engagement] of EBP (19 items), skills [preparedness] in EBP (13 items), attitude [perceptions] toward EBP (10 items), training in EBP-related areas (5 items), barriers to EBP uptake (13 items), and enablers of EBP uptake (10 items). 21 The remaining items measure the demographic/practice characteristics of participants. Three subscores can be generated from the use, skills and attitude items. Details of the scoring and parameters of these subscores have been previously reported. 6
The psychometric properties of EBASE have been published elsewhere. 21,22 Briefly, EBASE has demonstrated good internal consistency (Cronbach's alpha = 0.84), good construct and content validity (Content Validity Index = 0.899), and acceptable test–retest reliability (Intraclass Correlation Coefficient = 0.578–0.986). In addition, EBASE has been administered to a broad range of clinical disciplines (including osteopaths, 7,8,23,24 chiropractors, 5,6,25,26 nursing students, 27 herbalists, 28,29 homeopaths, 28 yoga therapists, 30 and Traditional Chinese Medicine practitioners 28 ) and across multiple countries (including Australia, 7,27,28 Canada, 25 the United Kingdom, 8 Spain, 23 Sweden, 24,26 and the United States 5,6,29,30 ).
As EBASE was originally developed for an Australian complementary medicine (CM) audience, some survey items required minor modification to ensure applicability to Canadian NDs. These changes included replacing the term CM with NM, and amending regionally specific demographic items (e.g., Canadian provinces, treatments typically provided in the first consultation). These amendments did not alter the meaning of the survey items.
Data collection
The survey was pilot tested by a convenience sample of five Canadian NDs with varying levels of academic and clinical experience. The aim of the pilot was to establish whether the language of the survey was appropriate to the Canadian NM context, and to confirm survey completion time. Pilot participants recommended minor changes to some terminology to improve the clarity of these items. These recommendations were deliberated by the research team, and implemented if consensus of agreement was reached. The average completion time of the survey was 10–15 min.
Participant recruitment was undertaken between February and May 2020. The survey was promoted using a multimodal approach to maximize reach and diversity of responses, and to reduce the risk of undercoverage and recruitment bias. This included the use of regular social media posts, and recurrent participant invitations in newsletters of the Canadian Association of Naturopathic Doctors, provincial naturopathic associations in British Columbia, Nova Scotia, Alberta, and Saskatchewan, the alumni newsletter for the Canadian College of Naturopathic Medicine, and the Interdisciplinary Network of Complementary and Alternative Medicine. All recruitment media directed potential participants to the online survey (hosted by SurveyMonkey™), where further information about the study was provided. The participant's IP address was recorded to check for duplicate entries from the same device throughout the duration of the survey.
Participants were required to read the participant information sheet before commencing the survey. As an incentive, participants could choose to enter a lottery to win one of three prizes.
Data analysis
Data were imported into IBM SPSS Statistics v.25.0 (IBM Corp., Armonk, NY) for analysis. The deduplication procedure for online surveys was applied to exclude multiple responses from single participants. 31 Surveys containing >80% unanswered items (due to early participant dropout) were excluded from the analysis [30]. Missing data were described as missing. Categorical data were reported as frequency distributions and percentages, and non-normally distributed data as medians and interquartile ranges (IQRs). Associations between nominal-level variables were tested using Cramer's V. Kendall's tau correlation coefficient was used to test for associations between ordinal-level variables. Coefficients were interpreted as follows: 0.10–0.29 (weak association), 0.30–0.49 (moderate association), and 0.50–1.00 (strong association). 32 The level of significance was set at p < 0.05.
Results
A total of 252 Canadian NDs agreed to participate in the survey, of which 240 completed the first item (participation rate: 95.2%), and 176 completed the last item (completion rate: 69.8%). The analyzable sample (i.e., number of survey responses >20% complete) was 234. As the reach of the survey could not be quantified, it was not possible to calculate a survey response rate.
Participant demographics
More than two-thirds of participating NDs were female (70.5%) and aged between 30 and 49 years (70.1%) (Table 1). The majority of participants held a postgraduate qualification (70.5%), with most completing their highest qualification within the past 10 years (56.8%). Two-thirds of NDs worked part-time in clinical practice (i.e., 69.2% worked 1–30 h in practice), and participated in research 1–15 h/week (62.8%). Most (61.1%) participants did not work in a teaching role in the higher education sector. Participants largely practiced in the city or inner-city suburbs (56.0%), within the provinces of Ontario and British Columbia (70.5%). Almost one-half (49.1%) of the participants worked in a clinical setting alongside other complementary medicine (CM) providers.
Demographic and Practice Characteristics of Participants (n = 234)
CM, complementary medicine.
EBP engagement
The median EBP use subscore (13; IQR 8, 20.5; range 1–24) revealed moderate/high-level engagement in EBP-related activities among NDs. Highest levels of engagement were reported for online search engines and online databases, which NDs used ≥6 times in the previous month (71.3% and 65.3%, respectively) to search for practice-related literature/research (Table 2). By contrast, only 20.1% of the participants referred to lay literature ≥6 times in the past month to assist their clinical decision-making. Most (i.e., 63.3%–77.4%) NDs engaged in the remaining EBP-related activities between 1 and 15 times in the previous month.
Participating Naturopathic Doctor's Engagement in Evidence-Based Practice Activities in the Previous Month (n = 234)
Response categories with the highest number of responses have been bolded for each item.
IQR, interquartile range.
A weak positive association was found between use subscore (categorized by quartiles) and highest qualification (Ƭ = 0.126, p = 0.011) and hours in clinical practice (Ƭ = 0.155, p = 0.004). Use subscore was also moderately positively associated with hours participating in research (Ƭ = 0.331, p < 0.001). There were no statistically significant associations between use subscore and other demographic/practice variables. Use subscore (noncategorized) was weakly positively associated with the attitude subscore (Ƭ = 0.213, p < 0.001), and moderately positively associated with skill subscore (Ƭ = 0.399, p < 0.001).
Two-thirds of NDs used traditional knowledge (69.2%), published clinical evidence (i.e., clinical trials; 70.5%), clinical practice guidelines (68.4%), fellow clinicians/experts (65.0%), and patient preference (62.8%), a moderate-large extent of the time to inform clinical decision-making (Table 3). The remaining five information sources were used by 63.6%–73.0% of participants, a small-moderate extent of the time, to inform clinical decision-making.
Information Sources Used by Participating Naturopathic Doctors to Inform Their Clinical Decision-Making (n = 234)
Response categories with the highest number of responses have been bolded for each item.
IQR, interquartile range.
When participants were asked to estimate the percentage of their clinical practice that was based on evidence from clinical research, most (70.9%) indicated that a moderate to large proportion of their practice (or 51%–99% of practice) was based on such evidence (Fig. 1).
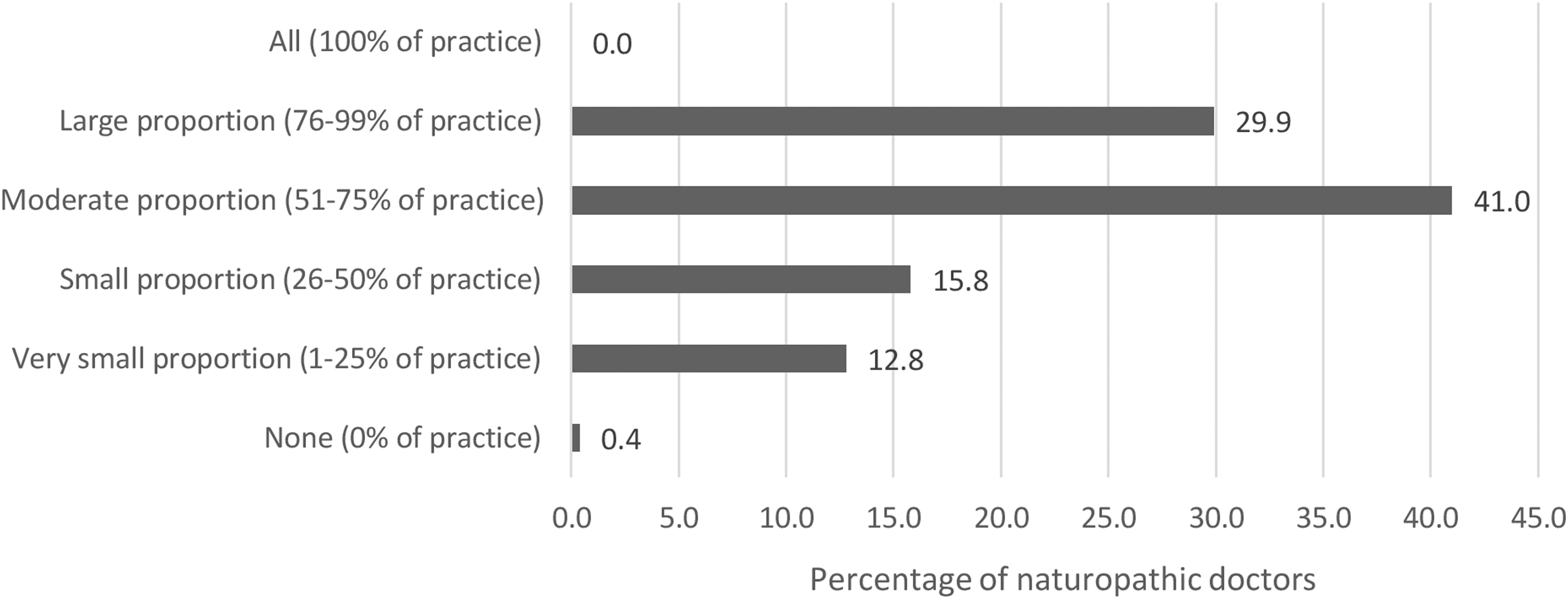
Percentage of participating naturopathic doctors' clinical practice based on evidence from clinical research (n = 234).
Preparedness for EBP
Median skill subscore (44.5; IQR 39, 52; range 19–65) pointed to moderate-level EBP-related skill among NDs. Highest self-reported skill levels related to “acquisition” activities of the EBP process, with two-thirds of NDs rating their ability to search online databases (75.7%), locate professional literature (67.1%), and retrieve evidence (65.4%) as moderate-high to high (Table 4). By contrast, the majority of participants reported a low/low-moderate skill level in conducting systematic reviews (64.5%) and clinical research (78.6%). Most (i.e., 64.1%–78.6%) participants rated their skill level as moderate/moderate-high for the remaining eight skills.
Self-Reported Skill Level in Evidence-Based Practice Among Participating Naturopathic Doctors (n = 234)
Response categories with the highest number of responses have been bolded for each item.
IQR, interquartile range.
Skill subscore (categorized by quartiles) was weakly positively associated with hours per week participating in research (Ƭ = 0.296, p < 0.001) and teaching in the higher education sector (Ƭ = 0.178, p = 0.003). There was also a weak positive association between skill subscore and gender (with male participants reporting higher skill levels; V = 0.296, p < 0.001) and practice setting (with higher skill levels reported among participants practicing in educational institutions or with CM and conventional medical/allied providers; V = 0.191, p = 0.021). Skill subscore (noncategorized) was weakly positively associated with attitude subscore (Ƭ = 0.234, p < 0.001). There were no statistically significant associations between skill subscore and other demographic/practice variables.
Most NDs reported undertaking some form of training in EBP (91.9%), evidence application (90.2%), critical analysis/thinking (88.0%), and to a lesser degree, the conduct of systematic reviews and meta-analyses (56.8%). Less than one-half (49.6%) of participants completed any training in conducting clinical research. Participants completed training across these five areas largely as a minor (20.1%–29.9%) or major (5.6%–38.0%) component of a study program.
Perceptions of EBP
Median attitude subscore (34; IQR 31, 37; range 8–40) signified a largely favorable attitude toward EBP among NDs (scores ranging between 32.0 and 40.0 are indicative of predominantly agree to strongly agree responses). Most participants agreed or strongly agreed that professional literature/research findings were useful in their day-to-day practice (93.5%), EBP was necessary in the practice of NM (92.4%), EBP assisted them in making decisions about patient care (95.8%), and they wanted to learn/improve the skills necessary to incorporate EBP into their practice (93.2%) (Table 5). At least one-half of NDs disagreed or strongly disagreed that the adoption of EBP placed an unreasonable demand on their practice (77.3%), and there was a lack of evidence from clinical trials to support most of the treatments used in practice (50.0%).
Perceptions of Evidence-Based Practice Among Participating Naturopathic Doctors (n = 234)
Response categories with the highest number of responses have been bolded for each item.
Reverse scored item.
EBP, evidence-based practice; IQR, interquartile range.
A weak negative association was evident between attitude subscore and participant age (Ƭ = −0.156, p = 0.014). Associations between attitude subscore and other demographic/practice variables were not statistically significant.
Barriers and enablers to EBP uptake
Participants were asked to indicate the extent to which 13 factors acted as barriers to EBP uptake. Most participants indicated lack of time (67.1%), lack of clinical research evidence in naturopathy (67.1%), patient preference for a particular treatment (61.9%), lack of resources (46.2%), and insufficient skills in locating (47.1%), interpreting (53.4%), and appraising (54.7%) research were minor/moderate barriers to the uptake of EBP. The majority of NDs did not perceive the following factors to be barriers to EBP uptake: lack of interest in EBP (71.8%), lack of colleague support for EBP (64.5%), lack of incentive to participate in EBP (60.7%), and insufficient skills in applying research findings to clinical practice (52.1%).
Participants were divided as to whether a lack of relevance to NM practice (44.4% stating it is not a barrier vs. 50.0% stating it is a barrier) and a lack of industry support (48.3% stating it is not a barrier vs. 46.2% stating it is a barrier) were barriers to EBP uptake.
Of the 10 enabling factors listed in the survey, most participants reported these as moderately/very useful, including access to the following: the internet in the workplace (90.6%), free online databases in the workplace (90.2%), free online databases that require license fees (82.9%), full-text journal articles (88.0%), online EBP education materials (86.3%), critical reviews of research evidence relevant to naturopathy (83.7%), critically appraised topics relevant to naturopathy (74.3%), tools to assist the critical appraisal of research evidence (71.8%), research rating tools to facilitate critical appraisal of single research articles (65.8%), and online tools to conduct critical appraisals of multiple research articles related to a single topic (59.8%).
Discussion
This is the first study to assess the engagement, preparedness, and perceptions of EBP among Canadian NDs. The findings indicate that Canadian NDs have a generally positive attitude toward EBP, and moderate-level skill and moderate/high-level engagement with EBP. Participating NDs incorporated information from a wide range of sources to inform their clinical decision-making, but appear to be constrained from using certain types of evidence due to limited time, resources, and skills. The implications of these findings are discussed below.
Attitudes toward EBP were largely positive among Canadian NDs. This finding corroborates the attitudes expressed by North American and New Zealand naturopaths 33 in previous surveys, 16,18 as well as that reported by other CM professions in North America, 6,29,30 Australia, 7,28 Sweden, 24,26 and the United Kingdom. 8 The weak negative association between attitude and participant age also aligns with the view that the continuum of attitudes toward EBP is generationally specific. 16 The amount of time since graduation is an important consideration as the inclusion of research and EBP in naturopathic curriculum has changed over time, as has institutional culture, with recent graduates being exposed to more opportunities to develop EBP competencies compared with the 36% of respondents who completed their training over a decade ago.
In addition to the positive attitudes toward EBP, Canadian NDs reported a reasonable level of EBP engagement. However, the degree of EBP engagement reported in this survey is higher than the levels reported previously by other CM professions, including chiropractors, 6,25 osteopaths, 7,8 herbalists, 29 and yoga therapists. 30 This finding appears to align with the proportion of ND practice that is based on clinical research evidence, which is similarly higher than that reported by other CM professions. 5,7,8,29,30
The information sources NDs used to inform their clinical decision-making were diverse, although there was a stronger preference for traditional knowledge, clinical research evidence, and patient preference. The preference for traditional knowledge is similar to that reported by New Zealand naturopaths 33 and other CM professions, including chiropractors, 5,6 osteopaths, 7,8 herbalists, 29 and yoga therapists. 30 This act of combining different sources of information is consistent with the definition of EBP and might support the view that Canadian NDs have a suitable understanding, and application of EBP. Indeed, most participating NDs agreed that EBP considers clinical experience and patient preference, suggesting that participants may be cognizant of the various tenets of the EBP framework. 1
With respect to preparedness for using EBP, Canadian NDs reported high-level skill in identifying clinical questions or knowledge gaps, and steps in the acquisition of such knowledge. Participants reported that their weakest EBP-related skills were the conduct of clinical research and systematic reviews. This finding is similar to other surveys of CM providers, which consist largely of individuals working in clinical practice rather than individuals participating in the generation of research. 6 While skills related to the conduct of research may strengthen a clinician's skills in other EBP-related areas, such as critical appraisal and interpretation, they are arguably not necessary for the provision of evidence-based care.
A correlation was observed between EBP utilization and hours participating in research. This finding suggests that increased opportunities to participate in research (e.g., interrogating literature, collecting/analyzing research data) may foster increased EBP uptake. Similarly, a correlation was observed between EBP skill and hours participating in research and teaching in the higher education sector. This might again suggest a potential benefit of practitioners engaging in research and academic teaching opportunities to improve EBP skill development. Indeed, studies in other disciplines indicate that exposure to research training/activities may promote EBP uptake in clinicians. 27,33 –35
Participants pointed to several barriers to EBP uptake, with most participants reporting lack of time and lack of clinical research evidence in naturopathy as minor to moderate barriers. These barriers to EBP uptake are consistent with those reported by other CM professions, 5 –8,25,33 suggesting that systemic factors may be at play. Indeed, the lack of investment in naturopathic research (required for evidence generation 36 ), and the notable absence of naturopathic interventions in most clinical guidelines (as a means of facilitating evidence application 37 ) are well documented, and essential to overcome to improve EBP uptake in NM.
Other commonly reported enablers of EBP uptake were improving access to the internet, online databases, and full-text publications, particularly in the workplace. Access to these resources is essential to implementing most stages of the EBP process, including the acquisition, appraisal, and application of evidence. 38 Correspondingly, the absence of these resources was reported by participants as a notable barrier to EBP engagement. Similarly, and as reported by other CM professions, 6,25 a lack of skills in performing these tasks was viewed as an obstacle to EBP uptake. An overwhelming majority of participating NDs indicated that they were interested in learning or improving skills for EBP use.
This interest in continued education suggests that practitioners may have insight into, and an interest in correcting, their skills deficits. High-level interest in developing these skills further suggests that additional training within the naturopathic curriculum or continuing education opportunities are warranted and likely to be well-received by this professional group.
A strength of this study was the use of a validated and well-utilized instrument, 21 which allowed for direct comparison between different professions and geographic locations. There were some limitations to the study also. The use of nonprobability self-selection sampling increases the risk of self-selection bias. For instance, NDs holding strong opinions about EBP may have been more inclined to participate in the study; although, the reasons for nonparticipation are not known. The use of a multimodal recruitment approach aimed to mitigate this risk. Another consideration is that the analyzed sample was somewhat short of the required sample size, meaning that the study findings may have a slightly higher margin of error.
As there are limited publicly accessible, nationally representative and comprehensive demographic data on the Canadian ND workforce, it is difficult to assess the representativeness of this study sample. Notwithstanding, the age, sex, and geographical distribution of this sample closely approximated that of Canadian NDs reported in other surveys. 18,38 As with all self-reported surveys, there is a risk of cognitive bias; thus, it is possible that the self-reporting of EBP skill level may not directly correlate with a participant's actual skill level (as might be determined through a quiz).
Conclusions
Despite previously reported concerns of hesitancy, the present research suggests that Canadian NDs are generally supportive of EBP, and embrace the three tenets of the EBP framework. Participating NDs were also moderately prepared for, and moderately to highly engaged in EBP-related activities. A number of barriers and enablers to EBP uptake were also identified, which will help inform the development of future strategies to improve EBP engagement among NDs, with the expectation of improving quality of care and patient outcomes.
Footnotes
Ethical Approval
The study was reviewed and approved by the University of South Australia Human Research Ethics Committee (App. ID. 202745) and the Canadian College of Naturopathic Medicine Research Ethics Board.
Informed Consent
Informed consent to participate was implied based on completion of the survey.
Acknowledgments
The authors wish to thank the Canadian NDs who completed the survey, and the various associations that promoted the study, all of whom made this research possible.
Authors' Contributions
ML: Conceptualization, methodology, investigation, formal analysis, visualization, writing—original draft, writing—review and editing, and project administration. MA: Methodology, visualization, writing—original draft, and writing—review and editing. KC: Methodology, visualization, writing—original draft, and writing—review and editing.
Author Disclosure Statement
The authors state no conflict of interest.
Funding Information
The authors received no specific funding for this research.