
Abstract
Objectives:
The objective of this study was to investigate the effect of acupressure on fatigue severity, sleep quality, and psychological status in patients with end-stage renal disease (ESRD) receiving hemodialysis (HD) treatment.
Design:
A single-blinded parallel-group randomized controlled trial.
Settings/Location:
A medical center in central Java, Indonesia.
Subjects:
One hundred and six patients who had been receiving HD for at least 3 months were enrolled in this study and randomly assigned to two groups.
Interventions:
The experimental group received acupressure at K1, ST36, and SP6 acupoints. In contrast, the control group received sham acupressure at 1 cun from these three acupoints. Subjects received acupressure thrice per week for 4 weeks, and pressure on each acupoint was applied for 3 min bilaterally.
Outcome measures:
The primary outcome was fatigue severity, while sleep quality and psychological status (depression/anxiety) were evaluated as secondary outcomes. Outcomes were assessed using the Brief Fatigue Inventory, Pittsburgh Sleep Quality Index, and Hospital Anxiety and Depression Scale.
Results:
Acupressure induced a significant medium to large effect on improvement in fatigue (b = −1.71, confidence interval [95% CI]: −1.90 to −1.51, ΔR 2 = 0.744), sleep quality (b = −5.81, 95% CI: −6.80 to −4.81, ΔR 2 = 0.525), and anxiety (Estimate = −3.213, 95% CI: −4.238 to −2.188, pseudo R 2 = 0.292)/depression (Estimate = −3.378, 95% CI: −4.432 to −2.325, pseudo R 2 = 0.268) in experimental group patients compared to controls. No adverse events of acupressure were reported during the study process.
Conclusions:
Acupressure significantly and independently improved fatigue, depression/anxiety, and sleep quality in ESRD patients receiving HD.
Clinical Trial Registration:
NCT05571007
Introduction
End-stage renal disease (ESRD) is a progressive and irreversible impairment in kidney function that prevents the maintenance of mineral and waste product homeostasis. 1 Globally, ESRD is one of the most common chronic diseases with an incidence of 3 million in 2014 and has increased annually. 2 –4 In addition, it is one of the top 10 diseases in Indonesia that have significantly contributed to economic and health problems. 5 Patients require dialysis therapy or kidney replacement such as hemodialysis (HD), peritoneal dialysis (PD), and kidney transplants. 2 –4 Furthermore, 87.9%, 9.3%, and 2.6% of patients were, respectively, reported to have received HD, PD, and kidney transplants according to 2014 registry data. 1
Fatigue is a subjective feeling of tiredness, weakness, or lack of energy that interferes with normal activities, quality of life, and sleep. This feeling cannot be relieved by rest 6 –8 since it is a complex, multidimensional, and multifactorial phenomenon in ESRD patients receiving HD with a frequency ranging from 42% to 89%. 2,9 –13 Furthermore, it is strongly associated with chronic inflammation and severely affects the patient's treatment outcomes. 14 –16 It increases the risk of mortality and cardiac complications, highlighting its importance in ESRD patients. 15,16
Currently, fatigue management continues to focus on pharmacologic interventions, including growth hormone administration, antidepressants, antianxiety medications, levocarnitine, and erythropoietin-stimulating hormone. 15,16 However, these interventions favor renal burden and potentially increase side effects. Therefore, nonpharmacologic options such as nutritional intervention, exercise, health education, and acupressure are increasingly considered in managing fatigue. 15,16
Acupressure is a nonpharmacologic intervention of Traditional Chinese Medicine (TCM) performed by pressing or massaging acupoints to stimulate nerve endings and induce endorphin production, leading to muscle relaxation, pain relief, and improved comfort. 17 Furthermore, it has been tested as an alternative treatment in various conditions, such as sleep disorder, fatigue, pain, depression, and anxiety, 17 –19 especially among patients undergoing HD. 20 –22 Several studies have proven its effect on fatigue management using different acupoints, such as K1, GB34, ST36, SP6, BL23, LI4, and HT7. 23 Because acupressure is noninvasive, easy to learn, and applicable to individuals with proper training, it should be considered a safe intervention in fatigue management. Unfortunately, this intervention has not been used to manage fatigue in Indonesia. Therefore, this study aimed to investigate its effects on fatigue in ESRD patients who have been receiving HD. Sleep quality and psychological status were also assessed.
Materials and Methods
Study design
This was a single-blinded parallel-group randomized controlled trial (RCT) in which subjects did not know their group allocation. The primary outcome was the severity of fatigue in ESRD patients. Sleep quality, depression, and anxiety were evaluated as secondary outcomes due to their close association with fatigue. Subjects who fulfilled the inclusion criteria and completed informed consent were individually assigned to two groups using a random number table at a 1:1 ratio (simple randomization). Data were collected from a hospital in Indonesia from July to November 2019. This RCT is registered on
Participants
Inclusion criteria included aged ≥18 years, HD for at least 3 months, fatigue severity ≥4 (using a single item indicator of fatigue, ranging from 0 to 10 points), absence of lower limb wounds, did not receive any complementary treatments, and willingness to participate. Patients were excluded if they were diagnosed with major depression or psychiatric disorders, wound or amputation of the lower extremities, rheumatoid arthritis, or fracture of the limbs.
Intervention
The intervention was performed by the first author, also the principal investigator (PI), alone. The PI received training from a Traditional Chinese Physician (TCP), who is a clinical practitioner and associate professor of TCM, on how to find acupoints (K1, ST36, and SP6) and how to perform acupressure accurately.
The PI developed an acupressure protocol (Supplementary Data S1) and chose three acupoints (K1, ST36, and SP6) based on a literature review. 23 –27 In addition, the intervention dose was designed based on previous RCTs in terms of acupressure for fatigue management in HD patients. 24 –29 Most studies designed the frequency, duration, and intensity of acupressure as thrice a week for 4 weeks 24 –29 with a pressure application of 3 min per acupoint. 24 –27,29 The above studies found a small to large effect on reducing fatigue severity (Cohen's d = 0.02–1.6) 24 –27, and sleep quality (Cohen's d = 0.4–1.2), 26,29 and a small effect on psychological status (Cohen's d = 0.11–0.2). 26,28 The acupressure protocol was reviewed by three licensed TCPs with >20 years' clinical experience. To increase the internal validity of the study, the PI performed acupressure for all subjects individually and manually by following the established protocol, with no adverse events observed during the study process.
The PI manually applied thumb pressure to the three acupoints (K1, ST36, and SP6) at the rate of two rotations per second for 3 min at each acupoint. Acupressure was performed thrice per week for 4 weeks. Because these acupoints are located bilaterally in the lower extremities, 18 min were spent on each subject. The control group received acupressure at the sham acupoints using the same acupressure protocol, but the pressure was applied at 1 cun from K1, ST36, and SP6.
It is very important to locate and stimulate the acupoint to induce “de-qi” (thumb pressure at which the subject feels a sensation of a dull ache, tingling, and soreness). If the subject experienced “de-qi” when the PI stimulated the acupoint, the true point was considered to have been located. However, when the PI stimulated the sham acupoint, “de-qi” was not elicited in the subjects; thus, it did not evoke the effect of acupressure on symptom management. 30 The points were held with a depth of pressure described by the subject as the feeling of “de-qi.” Acupressure was performed in both groups within the first 2 h of the HD session. No participant experienced adverse events from acupressure during the study process.
Outcomes and data collection
Data were collected at two time points: before the intervention (baseline, T0) and after completion of the 4-week intervention (post-test, T1). The PI collected outcome variables 30 min after acupressure at T1. All questionnaires were completed by the subjects with the assistance of the PI. Thus, there were no missing data in this study. To avoid reporting bias, the PI collected data neutrally without guiding patients' answers and reminded patients that participation in the study would not affect their right to receive medical treatment at the hospital. Furthermore, the PI is not a health care provider at the study site; therefore, patients may likely feel free to provide answers without hesitation.
The Brief Fatigue Inventory (BFI) was used to measure the severity of fatigue in the past 24 h. This 9-item self-reported questionnaire is scored on a 0–10 numerical rating scale, where 0 and 10 reflect absence and the highest severity of fatigue. The BFI score is classified into mild (1–3 points), moderate (4–6 points), and severe fatigue (7–10 points). 31 In addition, BFI was tested in ESRD patients and showed good reliability with a Cronbach α of 0.96, 32,33 while its internal consistency reliability was 0.89 in this study.
Pittsburgh Sleep Quality Index (PSQI) was used to measure sleep quality. 34 This 19-item self-reported questionnaire is combined to form seven component scores (e.g., subjective sleep quality, latency, duration, habit efficiency, disturbances, medication, and daytime dysfunction), each of which has a range of 0–3 points added to yield a global score, with a range of 0–21. A global score higher than 5 points indicates poor sleep quality. 34 The Indonesian version of PSQI has good reliability with a Cronbach α of 0.89, 11,34 while its internal consistency reliability was 0.80 in this study.
The Hospital Anxiety and Depression Scale (HADS) was used to measure psychological status. This 14-item questionnaire has two subscales: anxiety (seven items) and depression (seven items). It is measured on a 4-point Likert scale, ranging from 0 (not at all) to 3 (very often) with higher scores indicating an increased level of anxiety/depression. 35 The HADS score is classified as severe (16–21 points), moderate (11–15 points), mild (8–10 points), and no anxiety or depression (≤7 points). 35 It is a valid, trustworthy, and easy measurement tool used by health care providers to identify and quantify anxiety and depression. 35,36 It demonstrates good reliability with a Cronbach α of 0.70, 36 while its internal consistency reliability was 0.91 in this study.
Statistical analysis
Data were coded and analyzed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). Data were analyzed individually using an intention-to-treat approach, which analyzes results based on the experimental group to which subjects were initially randomly assigned, regardless of whether they completed the intervention. 37 Multiple regression was used to analyze group differences in BFI and PSQI, while ordinal logistic regression was used to analyze the subscales of HADS. A p-value <0.05 was considered statistically significant. The sample size was estimated using G-power 3.0.10, with type II error = 0.8, α = 0.05, and effect size = 0.61, which was based on a similar study by Tsay 26 and Sabouhi et al. 25 Therefore, the estimated sample size for this study was 88 (44 subjects per group).
Ethical considerations
The study was approved by the Institutional Review Board of the Jenderal Soedirman University Research Ethics Committee (No. 3010/KEPK/VII/2019). The PI presented the study proposal to physicians and nursing staff at the study site to obtain their support. After receiving referrals from the health care providers at the study site, the PI met potential subjects and explained the purpose and procedure of the study to them. Informed consent was obtained before data were collected.
Results
A total of 114 patients fulfilled the sampling criteria. After exclusion of eight patients for various reasons, 106 patients were enrolled and randomly assigned to the experimental and control groups. However, 10 subjects were lost to follow-up due to the following reasons: did not participate in the intervention for 1 week (changed schedule) (n = 3), died (n = 3), refused to participate in the entire program (n = 1), and transferred to another hospital for HIV/AIDS treatment (n = 3). Finally, 96 subjects completed the study, with 49 in the experimental group and 47 in the control group (Fig. 1). Since no significant differences in baseline were found between attrition subjects and subjects who completed the study, an intention-to-treat approach was chosen to analyze the data. Moreover, no participants in the experimental group reported unintended effects due to acupressure (e.g., dizziness or pain).
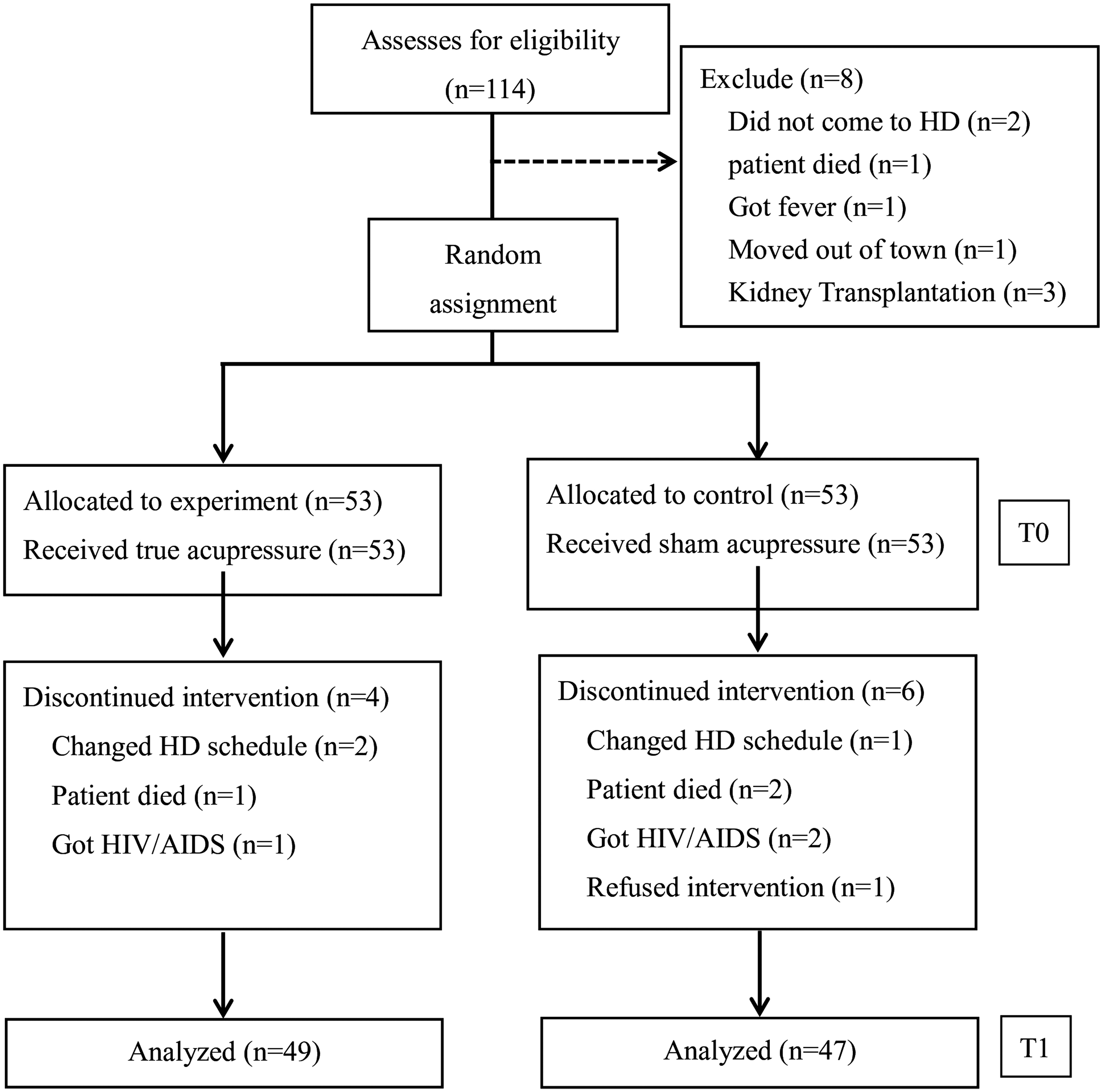
CONSORT flow diagram.
Most patients aged 36–65 years had an education level above senior high school, were married, and had been on dialysis for at least 2 years (Table 1). In laboratory findings, all participants had anemia (low Hb and Hct), hypoalbuminemia, hypercholesterolemia, and hyperglycemia (Table 2).
Demographic Characteristics of the Study Groups (N = 106)
CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HD, hemodialysis; TB, tuberculosis.
Baseline Laboratory Value of the Study Subjects (N = 106)
BUN, blood urea nitrogen; HbA1c, glycated hemoglobin; HBC, hemoglobin cell; HCT, hematocrit; PLT, platelet; SD, standard deviation; WBC, white blood cell.
The mean baseline BFI and PSQI scores in the experimental group were slightly higher than those in the control group (BFI: 6.14 ± 0.66 vs. 5.79 ± 0.52; PSQI: 13.91 ± 2.61 vs. 13.17 ± 3.36). However, the mean baseline scores for the HADS anxiety and depression subscales in the experimental group were slightly lower than those in the control group (anxiety: 12.40 ± 3.35 vs. 14.81 ± 5.15; depression: 12.42 ± 3.12 vs. 15.13 ± 4.58) (Table 3).
The Comparison of Brief Fatigue Inventory, Pittsburgh Sleep Quality Index, Hospital Anxiety and Depression Scale Between Groups at Baseline (N = 106).
BFI, Brief Fatigue Inventory; HADS, Hospital Anxiety and Depression Scale; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation.
Using multiple regression and controlling the pretest scores of BFI and PSQI, the authors found that after 4 weeks of intervention, the experimental group had statistically significantly lower fatigue (b = −1.71, confidence interval [95% CI]: −1.90 to −1.51, ΔR 2 = 0.744) and better sleep quality (b = −5.81, 95% CI: −6.80 to −4.81, ΔR 2 = 0.525) than the control group (Table 4). In addition, the authors used a cutoff score for HADS, 35 dividing subjects into four groups (no anxiety or depression, mild, moderate, and severe), and performed ordinal logistic regression to analyze group differences. This study found that the experimental group had statistically significantly lower anxiety (Estimate = −3.213, 95% CI: −4.238 to −2.188, pseudo R 2 = 0.292) and depression (Estimate = −3.378, 95% CI: −4.432 to −2.325, pseudo R 2 = 0.268) than the control group (Table 5).
Multiple Regression for the Group Difference in Post-Test of Brief Fatigue Inventory and Pittsburgh Sleep Quality Index (N = 106)
Control group as reference group. Adjust: pretest of BFI and PSQI.
BFI, Brief Fatigue Inventory; CI, confidence interval; PSQI, Pittsburgh Sleep Quality Index.
Ordinal Logistic Regression for Subscales of Hospital Anxiety and Depression Scale (N = 106)
Reference group. Adjust: pretest of HADS.
CI, confidence interval; HADS, Hospital Anxiety and Depression Scale.
Discussion
Fatigue is a common symptom in ESRD patients undergoing HD 10,12 and is considered a significant predictor of treatment outcome. 11,13 Therefore, health care providers should pay more attention to its management. This study showed significantly lower fatigue severity in HD patients in the experimental group than those in the control group. This result was similar to those of previous studies testing the effectiveness of acupressure on fatigue in ESRD patients in Taiwan, 26,38 United States, 24 and Iran. 25 However, in Indonesia, only one study has been conducted in which acupressure was used to improve the complications of diabetes mellitus. 39 The present study is the first to investigate the effect of acupressure on improving fatigue in Indonesian patients with ESRD.
Regarding the effect of acupressure on fatigue management in HD patients, this study showed a large effect size (ΔR 2 = 0.744), which is similar to results of other studies reporting a medium to large effect. 24,25,40 However, one study showed a small effect 26 in which the method, sample size, number of acupoints, and dose of acupressure were all similar to those used in this study; the only difference was the measurement tool. This study used BFI to measure fatigue, while Tsay's study 26 used the Piper Scale, which was originally developed for cancer patients. The Piper Scale may not be sensitive in ESRD patients. Further studies are suggested to test the effect of acupressure on fatigue using the same instrument.
All ESRD studies used the same dose of acupressure (acupressure applied thrice per week for 4 weeks). However, regarding the number of acupoints, this study adopted three (K1, ST36, and SP6), while some used four (K1, ST36, SP6, and GB34) 24,26 or five (K1, BL23, SP6, GB34, and HT7) acupoints. 25 Only one study chose a single acupoint (K13) 40 ; regardless of the number of acupoints used, all show a significant benefit of acupressure on fatigue, including when only one acupoint was adopted. 40 However, Tsay 40 provided a 3-min foot massage before acupressure; therefore, the large positive effect obtained needs further investigation due to the possibility of an additional effect.
Furthermore, this study showed a significantly lower HADS score (pseudo-R 2 = 0.268–0.292, a large effect) and better sleep quality (ΔR 2 = 0.525, a large effect) in HD patients in the experimental group than in those in the control group. The obtained result was similar to those of previous studies testing the effectiveness of acupressure on anxiety, 22,28,41 depression, 21,22,28,41 and sleep quality 11,20,26,40 with ESRD patients undergoing HD in different countries. A study from Iran showed a large positive effect (Cohen's d = 1.60) on anxiety and depression despite acupressure being applied at a single point (P6). 41 Another study from Malaysia 28 showed that acupressure significantly improved depression, anxiety, and general psychological stress with application on GV29, HT7, and K13. 28
The impact of acupressure was similar to that reported in previous studies investigating its effects on sleep quality in ESRD patients undergoing HD. 11,20,26,40 However, Arab et al reported a significant large effect (Cohen's d = 1.45) by applying acupressure to only one acupoint (HT7) and providing weekly exercise two to three times during implementation. 11 To examine whether this effect is due to acupressure or from exercise requires further testing.
In addition to the statistical significance of the effectiveness of acupressure on important outcomes, its clinical significance is supported by minimal clinically important difference (MCID). MCID is the smallest change in a treatment outcome that would be perceived as clinically meaningful. 42 Since there are no MCIDs available to detect the effectiveness of acupressure in patients with HD using BFI, PSQI, and HADS, the literature search was extended to other interventions with different populations. Although MCID for BFI is still unknown, MCIDs for PSQI and HADS are 4.4 and 1.7 points, respectively. 43,44 MCIDs in this study were calculated using a distribution-based approach with the effect size method suggested by the literature. 45,46 MCIDs of 4.77, 4.37, 2.59, and 2.81 points were obtained for BFI, PSQI, HADS-anxiety, and HADS-depression, respectively, which can be interpreted as clinically meaningful.
Some studies tested the benefit of acupressure in other populations, such as patients with late-stage lung cancer 47 and pregnant women, 48 and detected a significant medium effect (Cohen's d = 0.43–0.73) on sleep quality. Since acupressure has worked on patients with serious illnesses, such as advanced cancer, it should be applied to other populations with different chronic illnesses (e.g., chronic obstructive pulmonary disease, congestive heart failure, and elderly with chronic illnesses).
Limitations
Although this study had academic and clinical significance, there were some limitations. First was the short follow-up period after the intervention. The outcome variables were only once obtained 4 weeks after acupressure. Since its long-term effect is unknown, further research could determine the long-term benefit of acupressure on fatigue, sleep quality, and anxiety/depression.
The second limitation was that since all subjects were from one dialysis center, their characteristics may not be generalizable; therefore, external validity may be influenced. Therefore, recruitment from different hospitals is recommended to increase the study generalizability of future studies.
The third limitation was that fatigue severity was measured only through structured questionnaires. There was a lack of objective data at the post-test to prove the effectiveness of acupressure on fatigue management. Therefore, the inclusion of objective data, such as data from wrist actigraphy, in post-test assessments is suggested. Researchers have used wrist actigraphy and found lower rest-activity cycles in patients with fatigue. 49 In addition, wrist actigraphy can detect patients' sleep quality in mood disorders. 50,51 The objective data can be incorporated into future studies to increase the internal validity of acupressure research.
The fourth limitation was that the PI administered the questionnaire and the intervention. Even though the PI was not a health care provider at the study site, patients may have given biased answers. It is recommended to use a blind outcome assessor in future studies to prevent bias during data collection. Finally, the last limitation was the proximity of the sham acupoints to the true acupoints. Future studies may consider choosing sham acupoints that are on the bone prominences, which have no acupoints and are in a different dermatome region, to avoid inadvertently evoking the same effect as true acupoints.
Conclusions
This study showed a significant benefit of acupressure on fatigue, sleep quality, and psychological status in ESRD patients undergoing HD. This 18-min evidence-based acupressure intervention can be administered satisfactorily in a dialysis unit without adverse events. Although acupressure was performed by the PI in this study, patients or family members can perform this intervention, with little training, to control unpleasant symptoms. Since acupressure is noninvasive and easy to learn, it is recommended that this complementary therapeutic approach be included in continuing education to increase nurses' ability to manage symptoms in patients with various chronic illnesses.
Footnotes
Acknowledgments
Special thanks to all the ESRD patients and the staff members from Prof. Dr. Margono Soekardjo hospital who participated in this project.
Authors' Contributions
Conceptualization and Design: All authors. Methodology, Investigation, Data collection, and Formal analysis: M.S., Y.F.T., and P.K.T. Visualization and Writing—Original draft preparation: M.S., S.Y.C., W.R.T. Supervision and Writing—Reviewing and Editing: M.S., S.Y.C., W.R.T., L.C.W., S.H.Y., and J.T.F. All authors have read and approved the final version of the article and agree with the order in which the authors are listed.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.