
Abstract
Background:
Chemotherapy-induced nausea and vomiting (CINV) is one of the most distressing side effects associated with deterioration in the quality of life. This study aimed to assess the clinical value of Huoxiang Zhengqi (HXZQ) oral liquid, a Chinese patent medicine, in combination with 5-HT3 receptor antagonists (RAs) and dexamethasone, in preventing CINV in patients receiving multiday cisplatin-based chemotherapy.
Methods:
In this multicenter, exploratory randomized clinical trial, the authors compared the efficacy of HXZQ oral liquid against a control group receiving a placebo, in combination with 5-HT3 RAs and dexamethasone, in preventing CINV in chemotherapy-naive patients receiving a multiday cisplatin-based regimen between January 2021 and September 2021. The primary endpoint was the complete response (CR) rate. The secondary endpoints included days with no CINV, the incidence of CINV, and life function.
Results:
Sixty patients were randomized into two groups and included in the study. The CR rate was significantly improved by HXZQ oral liquid in acute CINV (63.33% vs. 33.33%, p = 0.020) and CINV beyond the risk phase (96.67% vs. 46.67%, p = 0.000). The number of days with no CINV was significantly more in the HXZQ group compared with the control group in the overall phase (18.10 ± 3.64 vs. 12.13 ± 7.63, p = 0.002). Significantly higher Functional Living Index-Emesis total and domain scores were observed in the HXZQ group.
Conclusions:
HXZQ oral liquid combined with 5-HT3 RAs and dexamethasone is a feasible and safe approach to prevent CINV in patients receiving multiday cisplatin-based chemotherapy who cannot use neurokinin 1 RAs.
Clinical Trial Registration:
ChiCTR2000040123
Introduction
Chemotherapy-induced nausea and vomiting (CINV) is perceived by cancer survivors as one of the most distressing side effects associated with deterioration in quality of life (QoL), and is undesirable for patients treated with chemotherapy and can even compromises patient's receptiveness to treatment. 1,2 The international guidelines recommend a combination of corticosteroids, 5-HT3 receptor antagonists (RAs), and neurokinin 1 (NK1) RAs as antiemetic prophylaxis, with the intent to prevent both acute and delayed CINV, in patients receiving highly emetogenic chemotherapy (HEC). 3 However, 30% of patients still develop CINV after a prophylactic antiemetic regimen intervention during HEC. 3 In addition, the previous real-world study revealed that 36% of patients suffer from CINV beyond the risk period during moderately to HEC. 4 Therefore, CINV remains a concern for clinicians and patients.
In addition, the guideline compliance rate is still unsatisfactory among different countries, which is mainly due to the unavailability of NK-1 RA and glucocorticoids. 5 Therefore, the accessibility, which may be affected by economic constrains, 4 to NK-1 RA is.
Therefore, an affordable and accessible treatment regimen for patients living in developing regions, such as the Sichuan Province of China, who receive HEC, is an unmet need. Emerging clinical evidence seems to favor Chinese herbal medicine for the prevention and treatment of CINV. 6 Based on the Chinese Traditional Medicine theory, damage to the stomach and spleen leads to upward Qi flow, triggering vomiting. 7 Chemotherapy, an exogenous pathologic factor, can injure the stomach and spleen and negatively influence their transportation abilities. 6 Huoxiang Zhengqi (HXZQ) oral liquid, a Chinese patent medicine, can regulate gastrointestinal motility from an immune regulation perspective and alleviate visceral hypersensitivity, and has been commonly used for the treatment of gastrointestinal diseases such as diarrhea and nausea in China. 8 The main components in the HXZQ oral liquid eliminate dampness and regulate the flow of Qi to improve spleen function. 6
Modern medicine attributed the development of CINV to various pathophysiologies. Stimuli transmitted with 5-HT3 and substance P, as well as stimulation from other neurotransmitters, such as dopamine and histamine, interact with the chemoreceptor zone and vomiting center, resulting in CINV. 9 The mechanism of antiemesis in HXZQ oral liquid might be related to the regulation of 5-HT levels, the downregulation of 5-HT (3A) receptor mRNA expression, and the reduction of 5-HT (3A) receptor activity. 10 Based on this, the authors hypothesized that the HXZQ oral liquid may have a potential clinical value in managing CINV. Herein, they conducted this multicenter, exploratory, randomized controlled trial to evaluate the feasibility and safety of HXZQ oral liquid on CINV in chemotherapy-naive patients who received multiday cisplatin treatment.
Materials and Methods
Patients
This multicenter, double-blind, exploratory randomized controlled trial evaluated the safety and efficacy of HXZQ oral liquid against a control group receiving indistinguishable placebo, combined with 5-HT3 RA and dexamethasone, as prophylactic antiemetic regimens for chemotherapy-naive patients receiving multiday cisplatin-based treatment at five cancer centers in Sichuan Province, China. This study followed the design of an exploratory randomized controlled trial (phase IIb). Considering that there were no prior data about HXZQ in CINV controls, the authors chose a relatively small sample size to carry out the initial study. Assuming that the complete response (CR) rate of the HXZQ oral liquid group in the acute phase was 70% and that of the placebo group was 35%, a superiority test was used. Alpha was set to 0.025, the test power was 80%, and the ratio of the HXZQ oral liquid group to the placebo group was 1:1. Each group included 27 eligible patients. A total of 54 cases were thus needed. Considering a 10% dropout rate, 60 cases were required for the total study.
This prospective study was conducted at five cancer centers: at the West China Hospital of Sichuan University, Yingshan Hospital of West China Hospital of Sichuan University, 903 Hospital of Jiangyou, Yibin Second Hospital of West China Hospital of Sichuan University, and Yibin Hospital of Traditional Chinese Medicine. This study was approved by the Ethics Committee of the West China Hospital of Sichuan University. Written informed consent was obtained from all the eligible patients. This prospective study was registered with the Chinese Clinical Trial Registry (ChiCTR2000040123).
Patients who met the following inclusion criteria were enrolled: histopathologically diagnosed malignant tumor, aged 18 years or older, chemotherapy-naive, scheduled to receive multiday cisplatin-based regimens (3-week regimen), without a history of chronic gastrointestinal diseases (such as chronic gastritis), chronic nausea and vomiting, and refusal to NK-1 RA administration. The exclusion criteria were as follows: (1) uncontrolled cancer pain and the need for titration or adjustment of the dose of opioid analgesics, or uncontrolled digestive reactions to opioid drugs; (2) long-term corticosteroid treatment; (3) nausea and vomiting for any reason 3 days before treatment; and (4) history of active peptic ulcer and gastrointestinal bleeding within 1 year.
A computer-generated procedure was used to create a randomization schedule. Before enrollment, 60 random study identification numbers were generated using a computer-generated procedure and randomly assigned to the HXZQ oral liquid group or placebo control group. The grouping results were kept confidential from all researchers. Once the patients were enrolled, the computer-generated procedure assigned them an available study identification number according to the enrollment order. The participants were assigned to the corresponding treatment groups based on the study identification number. The above process was conducted by the Cancer Psychology and Health Management Committee of the Sichuan Cancer Society and was double blind for both subjects and researchers. Based on the computer-generated program, enrolled patients were randomly assigned (1:1) to either the HXZQ oral liquid group (5-HT3 RA + dexamethasone + HXZQ oral liquid) or the placebo control group (5-HT3 RA + dexamethasone + placebo).
Treatment
All participants were administered 5-HT3 RA and dexamethasone. All eligible patients were offered a standardized dose of HXZQ oral liquid or placebo orally. The Cancer Psychology and Health Management Committee of the Sichuan Cancer Society purchased HXZQ oral liquid (Approval number: Z50020409, Lot number: 20112313) and placebo (Lot number: L20112313) from the Taiji Group Chongqing Fuling Pharmaceutical Co., Ltd. (Chongqing, China). The investigational products of the two groups were uniformly packaged. According to the grouping results of the computer-generated procedure, HXZQ oral liquid and placebo were randomly marked with study identification numbers and indicated on the package. The study identification number of medicines is consistent with the study identification number of patients. The above process was conducted by the Cancer Psychology and Health Management Committee of the Sichuan Cancer Society and was double blind for both subjects and researchers.
The HXZQ oral liquid consists of the extractive of 10 herbs. The quantification of ingredients of HXZQ oral liquid refers to the dry weight of the starting material that was used to produce 1025 mL of HXZQ oral liquid.
The starting materials including 80 g Atractylodis Rhizoma (Atractylodes lancea [Thunb.] DC. or Atractylodes chinensis [DC.] Koidz.) rhizome aqueous extract, 80 g Citri Reticulatae Pericarpium (Citrus reticulata Blanco) pericarp aqueous extract, 80 g Magnoliae Officinalis Cortex (Magnolia officinalis
HXZQ oral liquid was approved by the China Food and Drug Administration and produced by Taiji Group Chongqing Fuling Pharmaceutical Co., Ltd. in compliance with the monograph of the Pharmacopoeia of the People's Republic of China 2020. The placebo is a compound comprising six ingredients: Ginger (Zingiber officinale Roscoe) essence (powder) (1 g/L), ginger essence (liquid) (1 mL/L), steviosin (a glycoside derived from Stevia rebaudiana [Bertoni] Bertoni) (1.54 g/L), sucrose octaacetate (0.2 g/L), caramel colors (2.5 g/L), and piperine (an alkaloid obtained from Piper nigrum L.) (0.05 g/L). The researchers evaluated both liquids and found that they have similar taste and appearance. The dosage of HXZQ oral liquid or placebo was 30 mL every day with 10 mL taken orally thrice per day. Patients received the first dose of study medications 1 day before the beginning of chemotherapy until the next cycle of chemotherapy (3-week regimen).
Outcome measurement and follow-up
Baseline demographic characteristics such as age, sex, type of cancer, stage, history of surgery, performance status, smoking status and history, history of alcoholism, history of motion sickness, initial treatment or relapse, asymptomatic brain metastases before chemotherapy, chemotherapy status, use of dopamine RAs, and use of other antiemetic medications (tranquillizers, etc.) were collected. Enrolled patients were evaluated for only one chemotherapy cycle.
Nausea and emesis were measured using the patients' diaries designed and used in the previous real-world study. 4 Patients' diary [designed based on the MASCC Antiemesis Tool (MAT)], a patient's self-recorded diary, recorded the times of daily vomiting, severity of daily nausea, and daily conditions of salvage therapy on days 1–21 of chemotherapy. Nausea severity was evaluated using a visual analog scale (0 = no nausea, 10 = worst). Physicians provided patients' diaries to patients 1 day before the initiation of chemotherapy until the next cycle of chemotherapy with the intent of recording nausea and emesis, and supervised the accomplishment of diaries through daily call follow-up.
QoL was evaluated using the Functional Living Index-Emesis (FLIE), which is a validated questionnaire comprising two domains (nausea and emesis), with nine items in each. 11,12 Each item was evaluated using a seven-point visual analog scale (1 = a great deal, 7 = not at all). Each item in the different domains was summed to obtain a domain score. The total score on the FLIE questionnaire was determined using the nausea and vomiting domain scores. Higher scores corresponded to a favorable QoL and were more likely to maintain daily life. An average item score of >6 (total score >108) was defined as “no impact on daily life.” Patients completed the FILE questionnaire on days 7 and 21 to record the influence of CINV on QoL from days 1 to 7 and days 8 to 21, respectively.
The primary endpoint was to explore the CR rate of HEC in the acute phase (days 1–3 if cisplatin-treated for 3 days), delayed phase (days 4–7 if cisplatin-treated for 3 days), and beyond the risk period (days 8–21 if cisplatin-treated for 3 days). 4 The CR was defined as no vomiting and no salvage therapy, with a grade of nausea of <2.5. The risk phase was defined as the acute phase combined with the delayed phase, and the acute phase, delayed phase, and beyond the risk period were summed to create the overall phase of treatment.
The secondary outcomes included no CINV days, the incidence of CINV, and QoL. The no CINV days were defined as the number of days without emesis, nausea, or rescue therapy.
Experienced clinicians assessed the patients' adverse events according to the National Cancer Institute Common Toxicity Criteria Version 4.0.
Statistical analysis
The SAS 9.4 was performed to analyze data, in which the Mann–Whitney U test or independent-sample t-test was used for continuous variables between the two groups, while the chi-square test was performed for categorical variables between groups. A two-sided p-value <0.05 was deemed as having a statistical significance.
Results
Patient demographics and adherence
From January 2021 to September 2021, 60 eligible patients were enrolled in this study from five cancer centers in Sichuan Province, China (Fig. 1). All patients adhered to taking medications and completed the questionnaires based on daily assessment calls. No medication reduction or interruption due to poor drug tolerance occurred. No significant difference was observed in the patients' demographic characteristics at baseline between the two groups (Table 1).

The participant flowchart. 5-HT3 RA, 5-HT3 receptor antagonist; HXZQ, Huoxiang Zhengqi.
Baseline Demographic Characteristics of Enrolled Patients
HXZQ, Huoxiang Zhengqi; SD, standard deviation.
The incidence of CINV
Of the 30 patients, 12 (40.00%) in the HXZQ oral liquid group and 21 (70.00%) in the placebo group experienced nausea during the acute phase (p = 0.020). There was no significant difference between the HXZQ oral liquid and placebo groups in terms of the prevalence of delayed nausea [17 (56.67%) vs. 21 (70.00%), p = 0.284]. Beyond the risk period, the proportion of patients who experienced nausea was significantly greater in the placebo group compared with that in the HXZQ oral liquid group [16 (53.33%) vs. 3 (10.00%), p = 0.000]. Figure 2a shows the incidence of nausea between the two groups during the different periods.
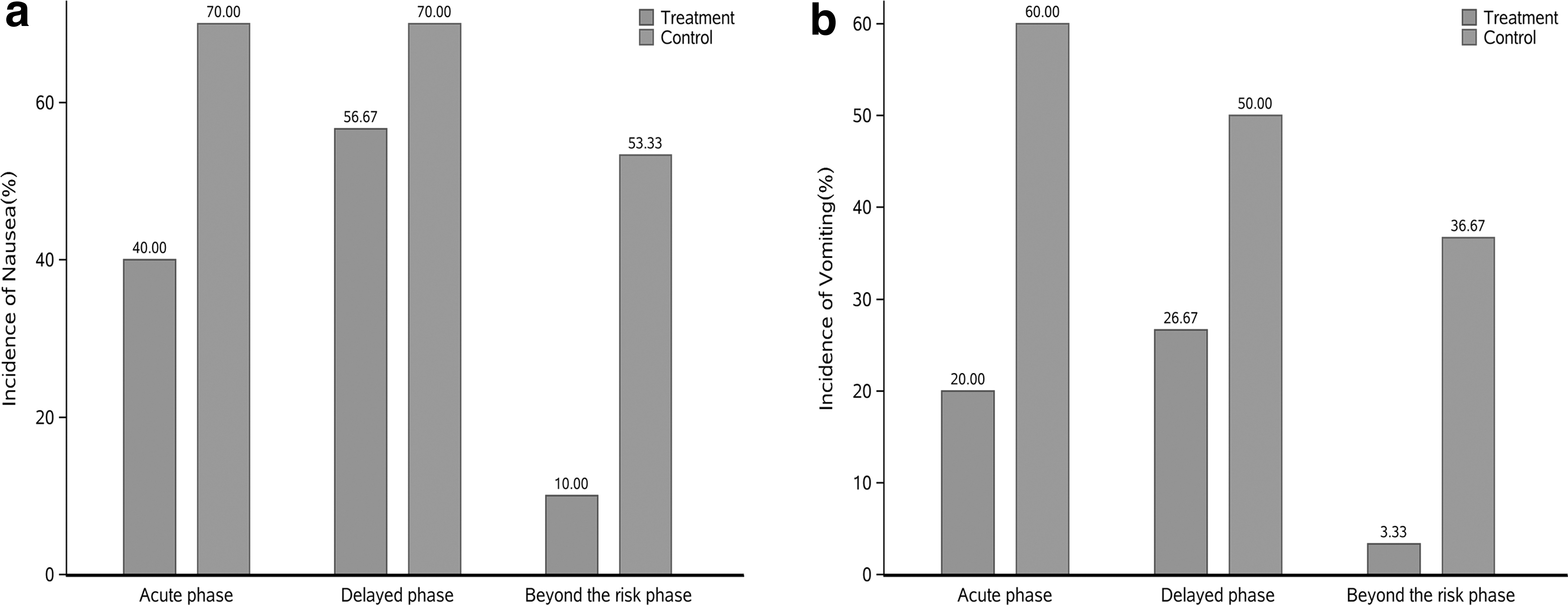
The incidence of chemotherapy-induced nausea and vomiting for the Huoxiang Zhengqi oral liquid (Treatment group) versus placebo (Control group): acute phase, delayed phase, and beyond the risk phase.
The proportion of participants administered the HXZQ oral liquid who had emesis is shown in Figure 2b.
Rate of CR
Participants with CR treated with the HXZQ oral liquid were more common than those who received placebo at any time, except for the delayed period. During the acute, delayed, and beyond risk periods, the rate of CR was 63.33% (19) versus 33.33% (10) (p = 0.020), 50.00% (15) versus 33.33% (10) (p = 0.190), 96.67% (29), and 46.67% (14) (p = 0.000), respectively. The differences in CR between the two groups were as follows: acute period, 30.00 (95% confidence interval [CI], 5.88 to 54.12); delayed period, 16.67 (95% CI, −7.92 to 41.26); and beyond the risk period, 50.00 (95% CI, 31.03 to 68.97) (Fig. 3).
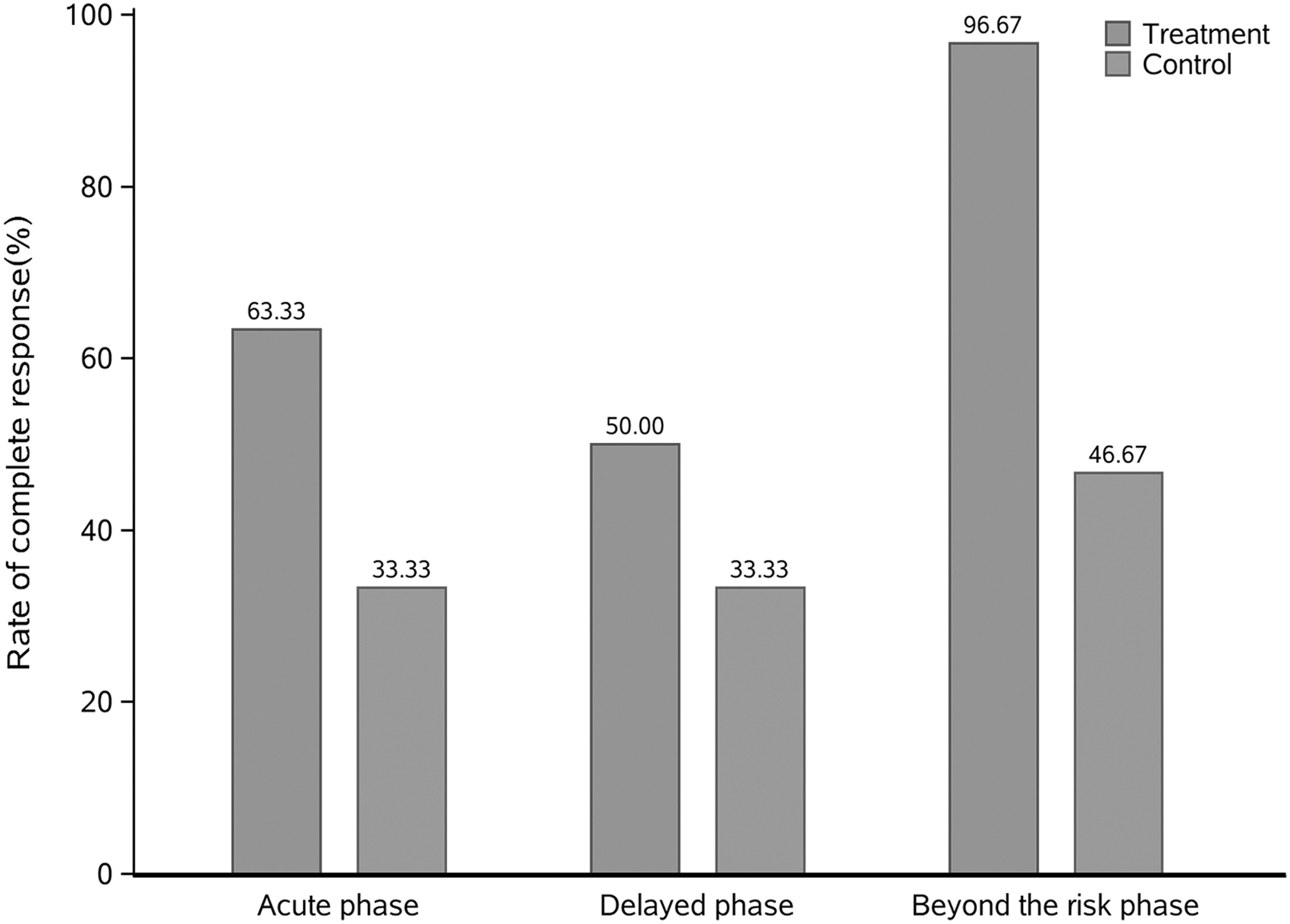
Proportion of patients achieving a complete response for the Huoxiang Zhengqi oral liquid (Treatment group) versus placebo (Control group): acute phase, delayed phase, and beyond the risk phase.
No CINV days
Throughout the diverse periods, the mean (standard deviation) days of no CINV were longer in patients receiving the HXZQ oral liquid compared with the placebo, 2.07 ± 1.14 versus 1.40 ± 1.19 in the acute period (p = 0.031), 2.37 ± 1.61 versus 1.53 ± 1.76 in the delayed period (p = 0.060), 4.43 ± 2.56 versus 2.93 ± 2.72 in the risk period (p = 0.032), 13.43 ± 1.92 versus 9.20 ± 5.37 beyond the risk period (p = 0.000), and 18.10 ± 3.64 versus 12.13 ± 7.63 in the overall phases (p = 0.002). However, there was no significant difference between the two groups in terms of the number of no CINV days in the delayed period (p = 0.060) (Fig. 4).
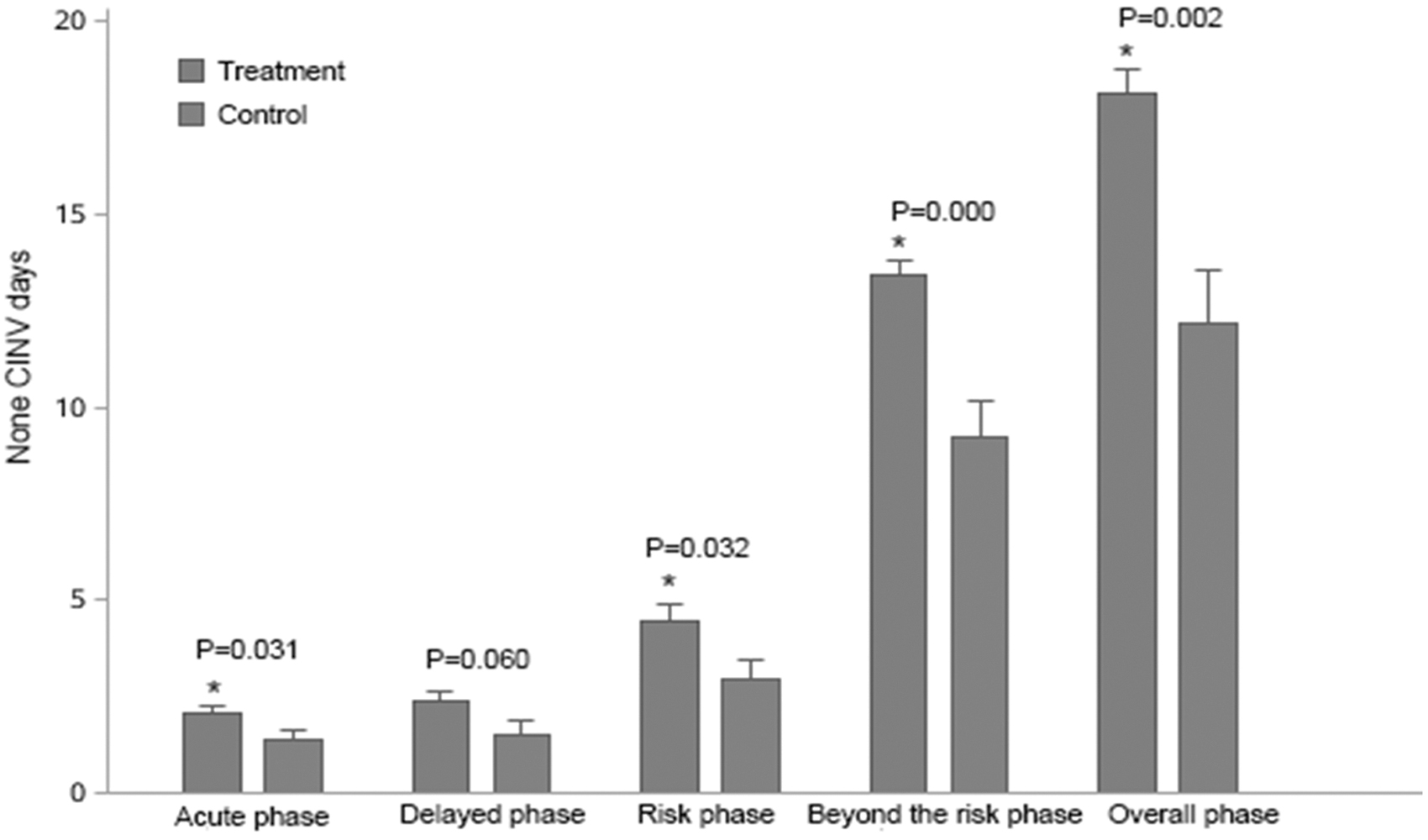
No CINV days. *Statistically significant difference versus placebo. CINV, chemotherapy-induced nausea and vomiting; HXZQ, Huoxiang Zhengqi; Treatment group, HXZQ oral liquid group; Control group, placebo group.
Quality of life
A significantly higher FLIE total score was observed in the HXZQ oral liquid group relative to the placebo group on days 1–7 (109.33 ± 20.52 vs. 87.60 ± 26.35, p = 0.001), as well as on days 8–21 (119.80 ± 18.39 vs. 110.83 ± 19.18, p = 0.009). The scores of the nausea domain were significantly higher in the HXZQ oral liquid group during days 1–7 or days 8–21 compared with the placebo group (53.63 ± 11.16 vs. 41.77 ± 14.48, p = 0.001; 59.07 ± 9.71 vs. 54.70 ± 9.53, p = 0.012, respectively).
The scores of the vomiting domain were more in the HXZQ oral liquid group compared with the placebo group during the days 1–7 as well as days 8–21 (55.70 ± 11.55 vs. 45.83 ± 15.68, p = 0.006; 60.73 ± 9.48 vs. 56.13 ± 11.13, p = 0.013). Moreover, the proportion of patients with total scores >108 was higher in the HXZQ oral liquid group than in the placebo group on days 1–7 and days 8–21 (70.00% vs. 26.70%, p = 0.001; 90.00% vs. 66.70%, p = 0.028) (Fig. 5).
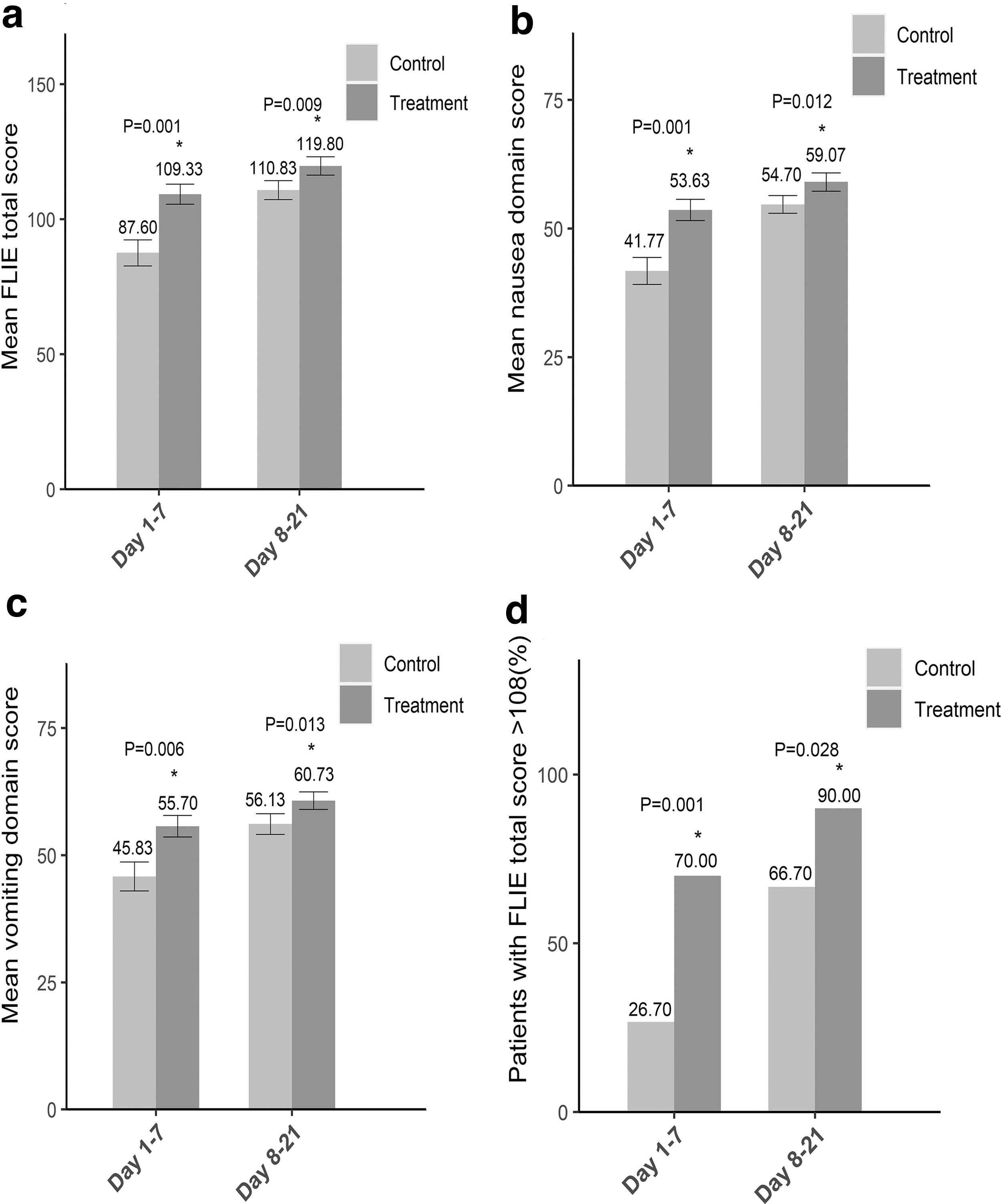
The scores of the FLIE questionnaire on days 1–7 and days 8–21.
Safety
No severe adverse events (grade 3) were observed. No differences in the occurrence rate of adverse events were observed between the two groups (Table 2).
Adverse Effects
HXZQ, Huoxiang Zhengqi.
Discussion
While the current antiemetic guidelines offer the potential to prevent CINV in most patients undergoing HEC, the unsatisfactory compliance of guidelines weakened the control of CINV in clinical practice due to economic constraints and medical insurance policy for developing areas. Therefore, seeking an affordable regimen may be appealing to patients in the developing regions. To the authors' knowledge, only a few studies have used the HXZQ oral liquid to prevent CINV in patients receiving HEC. This study primarily assessed the feasibility and safety of HXZQ oral liquid in addition to 5-HT3 RA and dexamethasone as an antiemetic prophylaxis in cancer patients undergoing HEC.
In this report, the HXZQ oral liquid combined with 5-HT3 RA and dexamethasone was shown to be efficacious in preventing CINV in HEC-treated patients. A higher CR rate was observed across the acute period and beyond the risk period in the HXZQ oral liquid group compared with that in the placebo control group (63.33% vs. 33.33% and 96.67% vs. 46.67%). In addition, no CINV days in the HXZQ oral liquid group versus the placebo control group were 2.07 ± 1.14 versus 1.40 ± 1.19, 4.43 ± 2.56 versus 2.93 ± 2.72, 13.43 ± 1.92 versus 9.20 ± 5.37, and 18.10 ± 3.64 versus 12.13 ± 7.63 in the acute, risk, beyond the risk, and overall phases, respectively. These results also showed that HXZQ oral liquid taken daily significantly reduced the incidence of CINV in the acute period and beyond the risk period for patients with HEC compared with the placebo.
Interestingly, the authors found that the HXZQ oral liquid had the potential to improve and maintain the QoL of patients undergoing HEC, which would not deteriorate after relatively long-term administration. Overall, 70% of the patients in the HXZQ oral liquid group on days 1–7 who received HEC could avoid the impact of CINV on daily life, and 90.00% of the patients did not have CINV, which could have negatively influenced their daily lives on days 8–21. The proportion of patients in the HXZQ oral liquid group who suffered the unfavorable influence of CINV during the risk period was 30%. This percentage was similar to other studies reporting that 33%, 26.8%, and 22.9% of patients who received guideline-consistent CINV prophylaxis undergoing either HEC or moderately emetogenic chemotherapy had a total FLIE <108. 12 –14
Based on this scenario, the authors can assume that HXZQ oral liquid can improve CINV and maintain QoL in patients receiving HEC. They found that outside the risk period, the proportion of patients in the placebo group with FLIE questionnaire scores >108 increased relative to the risk period. However, 1/3 of the patients in the placebo group suffered a negative impact from CINV in their daily lives outside the risk phase, compared with only 10% of the patients who received relatively long-term HXZQ oral liquid. Current research rarely focuses on CINV outside the risk period, but this study found that it could harm patients' QoL, and CINV outside the risk phase needs sufficient attention in future research. In this study, the authors also found that HXZQ oral liquid is capable of improving CINV and maintaining QoL outside the risk period; however, this requires further research.
In China, Traditional Chinese Medicines are widely used as adjuvant treatments for anticancer-related symptoms such as gastrointestinal adverse events. 15 Recently, some clinical trials have evaluated the efficacy of Traditional Chinese Medicines in alleviating chemotherapy- or radiotherapy-related gastrointestinal negative side effects. 15 Guo et al. showed that Astragalus polysaccharide might improve QoL and relieve nausea and vomiting in patients with nonsmall-cell lung cancer treated with vinorelbine and cisplatin. 16 A systematic review performed by Chen et al. 17 assessed the efficacy of herbal medicine in patients with colorectal cancer with chemotherapy-induced gastrointestinal side effects. They found that traditional herbal medications improved chemotherapy-induced gastrointestinal side effects, including nausea and vomiting.
In addition, they also demonstrated that five herbs were associated with improving chemotherapy-induced gastrointestinal toxicities, including Glycyrrhiza uralensis Fisch, Atractylodes macrocephala Koidz, Astragalus membranaceus (Fisch.) Bge, Codonopsis pilosula (branch.) Nannf, and pericarp of Citrus reticulata Blanco. Atractylodis Rhizoma, Citri Reticulatae Pericarpium, and liquorice extract were also essential elements of the HXZQ oral liquid, 8 which indicates that the HXZQ oral liquid might be related to the amelioration of CINV. Some ingredients of HXZQ oral liquid, including Pinellia, Pericarpium citri reticulatae, and Poria, have been shown to improve vomiting. 10 Xiao-Ban-Xia-Tang, composed of ginger and Pinellia, is notably efficacious for treating CINV by inhibiting the central or peripheral increase of the NK1 receptor. 18 Rhizoma Pinelliae was found to have the ability of antiemetic effects on cisplatin-induced emesis model in minks, with possible association with its property to inhibit the central nervous system.
An animal study also illustrated that Rhizoma Pinelliae blocks 5-HT3 and NK1 receptors in isolated guinea pig ileum, which may be a potential mechanism for managing CINV. 19 The pericarpium Citri reticulatae can relieve the contraction spasm of the intestinal smooth muscle caused by 5-HT, histamine, or acetylcholine. 6 Triterpenoids, compounds produced with Poria, can also regulate the expression of 5-HT (3A) receptors in Xenopus oocytes. 20 Lv et al. 6 retrospected 92 clinical studies illustrating that Pinellia Rhizoma, Glycyrrhizae Radix et Rhizoma, Poria, and Atractylodis macrocephalae Rhizoma were the most frequently administered drugs for the control of CINV. This study also found that Chinese herbal medicines are effective in preventing CINV. Based on this, the critical components of the HXZQ oral liquid seemed to have a potential clinical value in preventing and controlling CINV, which offers primary theoretical support for clinical implementation, but further research is needed.
Limitations to this clinical study include its exploratory nature, given that it is a relatively small sample prospective study, and the lack of other studies exploring the clinical value of HXZQ oral liquid in managing CINV. Owing to its exploratory nature, a relatively small sample study cannot lead to a convincing conclusion. However, this study found that HXZQ oral liquid can bring significant clinical benefits to patients with HEC by efficiently preventing and controlling CINV during and outside the risk phase. Larger clinical studies are needed to assess the clinical value of HXZQ oral liquid, 5-HT3 RA, and dexamethasone in preventing CINV in developing areas. The underlying mechanism of HXZQ oral liquid in controlling CINV has not yet been elucidated.
The authors speculated that HXZQ oral liquid might play a potential regulatory role in the 5-HT3-induced CINV pathway, which is a theory supported by some preclinical trials. 10 However, the involvement of other mechanisms remains to be explored. To the authors' knowledge, the NK-1 emetic mechanism is thought to be predominantly involved in delayed CINV. 21 Future studies should explore whether HXZQ oral liquid can prevent delayed CINV by regulating the NK-1 emetic mechanism. The authors will further study the potential mechanism by which HXZQ oral liquid prevents CINV to improve this research direction.
Conclusions
The HXZQ oral liquid, in addition to 5-HT3 RAs and dexamethasone, is a feasible and safe approach to prevent CINV in patients receiving multiday cisplatin-based chemotherapy who cannot use NK-1 RAs.
Footnotes
Acknowledgments
The authors are thankful for the guidance of the Cancer Psychology and Health Management Committee of Sichuan Cancer Society (S.C.S.). They would like to thank Editage (
Authors' Contributions
H.W.: Data curation, formal analysis, investigation, visualization, and original draft. Y.S. and L.X.: Data curation, formal analysis, investigation, methodology, and validation. Y.J.: Formal analysis, resources, and software. J.H., X.D., W.H., and Y.H.: Resources and validation. J.Z.: Conceptualization, project administration, resources, supervision, review, and editing.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.