
Abstract
Introduction:
Complementary and integrative health (CIH) therapies refers to massage therapy, acupuncture, aromatherapy, and guided imagery. These therapies have gained increased attention in recent years, particularly for their potential to help manage chronic pain and other conditions. National organizations not only recommend the use of CIH therapies but also the documentation of these therapies within electronic health records (EHRs). Yet, how CIH therapies are documented in the EHR is not well understood. The purpose of this scoping review of the literature was to examine and describe research that focused on CIH therapy clinical documentation in the EHR.
Methods:
The authors conducted a literature search using six electronic databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Ovid MEDLINE, Scopus, Google Scholar, Embase, and PubMed. Predefined search terms included “informatics,” “documentation,” “complementary and integrative health therapies,” “non-pharmacological approaches,” and “electronic health records” using AND/OR statements. No restrictions were placed on publication date. The inclusion criteria were as follows: (1) Original peer-reviewed full article in English, (2) focus on CIH therapies, and (3) CIH therapy documentation practice used in the research.
Results:
The authors identified 1684 articles, of which 33 met the criteria for a full review. A majority of the studies were conducted in the United States (20) and hospitals (19). The most common study design was retrospective (9), and 26 studies used EHR data as a data source for analysis. Documentation practices varied widely across all studies, ranging from the feasibility of documenting integrative therapies (i.e., homeopathy) to create changes in the EHR to support documentation (i.e., flowsheet).
Discussion:
This scoping review identified varying EHR clinical documentation trends for CIH therapies. Pain was the most frequent reason for use of CIH therapies across all included studies and a broad range of CIH therapies were used. Data standards and templates were suggested as informatics methods to support CIH documentation. A systems approach is needed to enhance and support the current technology infrastructure that will enable consistent CIH therapy documentation in EHRs.
Introduction
Complementary and integrative health (CIH) therapies, also called non-pharmacological therapies, continue to increase in use for management of an array of health conditions and also for health and wellness among the general population. 1,2 CIH therapies include, but are not limited to, massage therapy, Reiki, aromatherapy, acupuncture, and natural supplements. 1,3 In the United States, ∼33% of adults and 12% of children use complementary health approaches. 2 The current opioid epidemic has further increased attention on the use of CIH therapies as part of comprehensive pain management. Several national clinical guidelines support the use of CIH as a first-line therapy for pain management.
These guidelines also require documentation of CIH therapy use in the electronic health record (EHR). 4 –6 EHRs are the main platform for health provider documentation of clinical care and are increasingly used for quality improvement, outcome measurement, and comparative effectiveness research. 7,8 However, the literature reveals that EHR data lack standardization and contain data quality issues, such as data inconsistencies or incompleteness. Furthermore, knowledge of the current EHR documentation practices related to CIH therapies is limited.
Previous evidence suggests that there is high variability in CIH therapy documentation in EHR. 2,9 This variability can be attributed to lack of health provider knowledge related to documentation, poor patient disclosure of use, and limited provider inquiry into the use of CIH therapies. 2 The inconsistent documentation practices raises concerns for patient safety, quality care, and care coordination. Furthermore, the lack of documentation of CIH therapy has implications for research and clinical practice. For example, high variability in EHR data may not be representative of actual clinical use and, therefore, poses challenges on conducting comparative effectiveness research using EHR data and limitations on the generalizability of the research. Improving knowledge related to CIH documentation supports the design of informatics solutions that can aid in building the informatics infrastructure needed to support CIH use in clinical practice and outcomes research. 7,8
Informatics solutions, such as standardized terminologies, have the potential to provide structure to the data. Structured data are standardized and contain uniform elements that enable shareable and comparable data across institutions and platforms. 10 –12 The use of standardized terminologies, such as Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT), provides structure to the data and enables implementation of data standards. SNOMED CT, a comprehensive multilingual clinical health care terminology, is mapped to other international standards, and contains validated clinical concepts to enable consistent representation of clinical content. 13
Additional coding systems such as Current Procedural Terminology (CPT) is another terminology that can play an important role in harmonizing CIH data across the health system. 14 Such data standards across institutions can contribute to a learning health system through use of accessible and shareable data. 12,15 Furthermore, national organizations and initiatives, such as National Institutes of Health, Bridge2AI, recommend the use of data standards to improve interoperability across institutions and provide the infrastructure needed for research to advance analytical methods, such as machine learning (ML) and artificial intelligence (AI). 16
The purpose of this scoping review of the literature was to examine and describe research that focused on CIH therapy clinical documentation in the EHR. The authors selected a scoping review due to the complexity of the body of literature and the need to synthesize evidence across the various heterogeneous domains (i.e., CIH and Informatics). 17
Materials and Methods
The authors followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) to enable a comprehensive systematic scoping review of the literature. 17 They conducted a structured literature search using the following six electronic databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), Ovid MEDLINE, Scopus, Google Scholar, Embase, and PubMed. They consulted with a health science librarian at the University of Minnesota Biomedical Library and categorized a set of predefined concepts terms into five categories (“electronic health records,” “documentation,” “nursing records,” “flowsheet,” “complementary and integrative health therapies,” and “non-pharmacological approaches”) to provide organization when combining terms during the search process (Table 1). After finalizing the included articles, the authors conducted a manual search using the reference lists of the identified studies.
Example Keywords and Search Strategy for Ovid MEDLINE
No restrictions were placed on the publication date. The inclusion criteria were (1) original peer-reviewed full article in English, (2) focus on CIH therapies, and (3) CIH therapy documentation practice used in the research. Exclusion criteria were (1) did not include a description of CIH therapy documentation practice; (2) published as review articles, comments, book chapters, conference abstracts, editorial articles, theses, or dissertations; and (3) non-English.
Based on the eligibility criteria, two reviewers (R.R.A. and S.-C.L.) independently scanned the study titles and abstracts to identify relevant studies. Four reviewers (R.R.A., S.-C.L., R.J., and S.P.) independently performed full-text screening of the studies identified in the title and abstract screen to finalize the inclusion studies. In both title, abstract, and full-text screens, they used the first 10% of the studies to ensure good inter-rater reliability.
For data extraction, the authors developed a data extraction tool using Excel for the purpose of this study. Four researchers (R.R.A., S.-C.L., R.J., and S.P.) independently extracted data from the included studies using the extraction tool. They developed a data extraction protocol to train and guide reviewers to maintain good inter-rater reliability.
The authors used a descriptive summary method to summarize the included articles and provide an overview of the current state and focus of the literature. They thematically organized the studies using different types of informatics approaches and types of CIH therapy identified in the study. This study was non-human subjects research from the Institutional Review Board.
Results
The authors identified 1658 articles and included 33 articles in the final analysis. The majority of the studies were excluded from the final analysis because there was no discussion of CIH therapy clinical documentation (76) (Fig. 1).
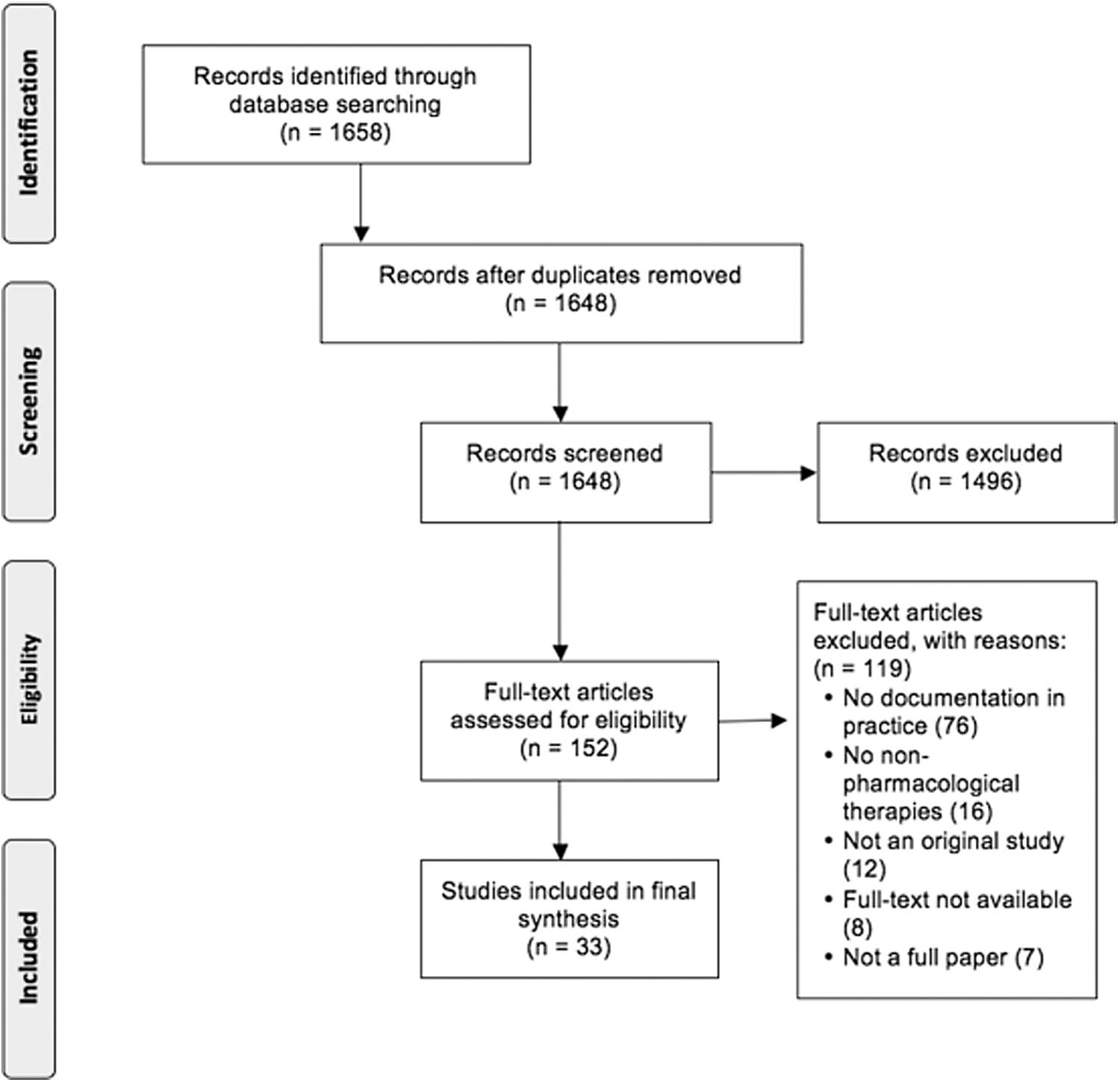
PRISMA-ScR flowchart. PRISMA-ScR, Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews.
Studies ranged from 2002 to 2021, and were conducted in the United States (20) and in a hospital setting (19). Most of the included studies had a retrospective design (9), and over half of the studies (26) used EHR data as a source for data analysis (Table 2).
Description of Included Studies
VHA, Veterans Health Administration.
The main target of CIH therapies for the majority of studies was pain or pain management (14), followed by a reason (not specified) (12), or radiation or cancer treatment side effects (4). About one third included studies did not specify the purpose of CIH therapies provision, reflecting unstandardized reporting, incompleteness CIH therapy documentation, or both. There were 34 different CIH therapies identified in the literature, with acupuncture (12) the most common modality, followed by therapy “Not specified” (9) and massage (8) (Fig. 2). Many frequently used modalities, such as nutritional supplements, Traditional Chinese Medicine, and energy therapies, were mentioned in only few studies. The documentation of art therapy, animal therapy, journaling, and many other CIH therapies that have been shown effective on management of many symptoms, such as pain, were not discussed in any included studies.
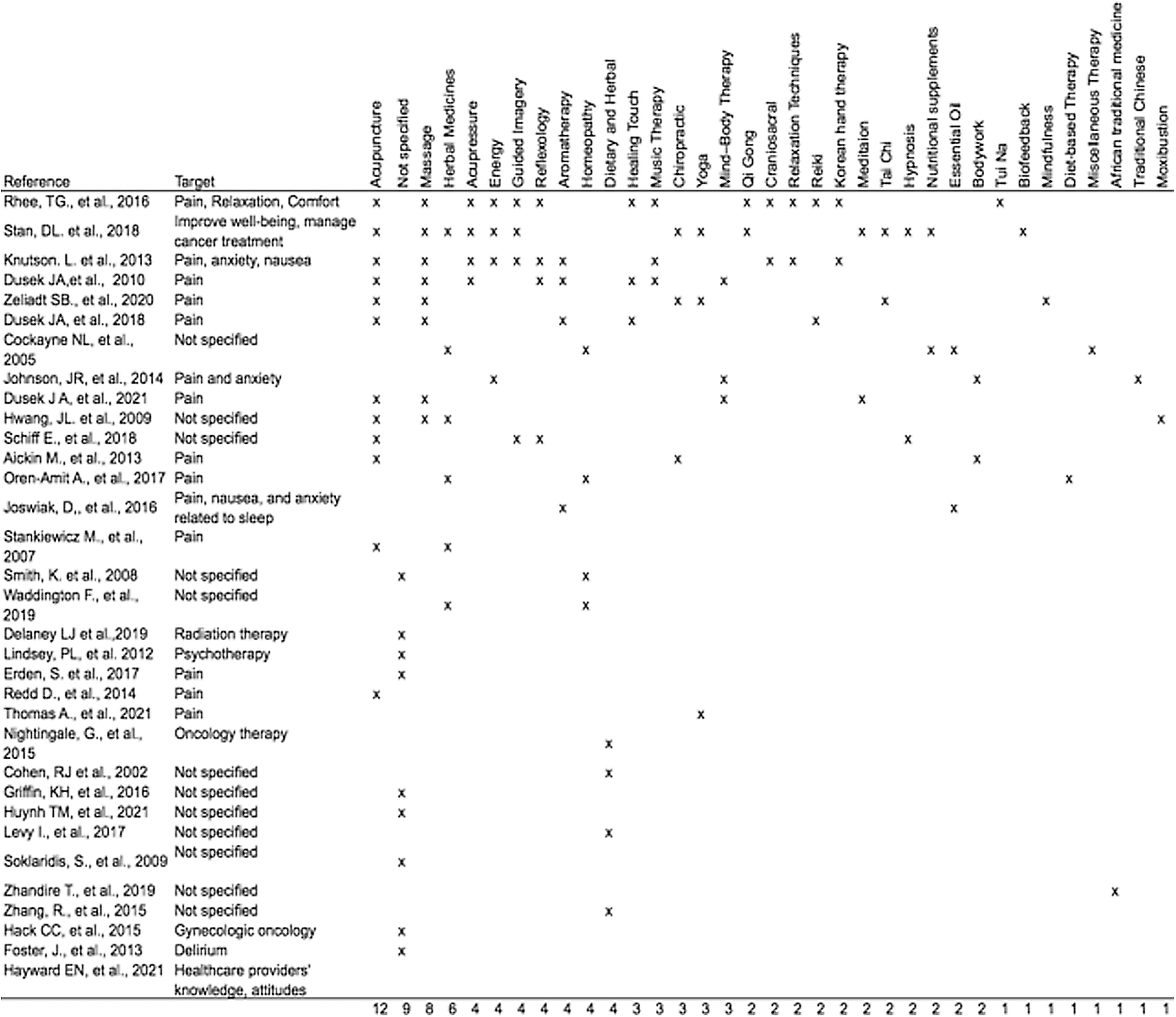
Summary of therapies from included studies.
The authors identified informatics approaches used in the included studies. The most frequent approach was data standards and templates (19), followed by education and training (13), and workflow (13) (Table 3).
Informatics Approaches Identified in the Included Studies
Data standards and templates
Standardization tools (e.g., standardized terminologies or templates) can help facilitate CIH therapy documentation. For example, implementation of standardized tools (e.g., standardized CIH assessment forms) and standardized templates may reduce barriers to CIH therapy documentation. 18 –20 Challenges noted with data standards and templates was use of these tools is not consistent across units nor with all health professionals. 20,21 A system-wide implementation strategy may facilitate consistent use.
Education and training
Proper training of nurses and providers is needed to document CIH therapies as a strategy to reduce missing or incomplete documentation. For example, continuing education or professional development training related to nursing or provider inquiry into CIH patient use. 2,9,20,22,23 Specific challenge related to education and training was there is limited training on CIH documentation within the EHR and if there is training it may not be the same across all units (e.g., emergency room vs. medical/surgical). 23,24
Workflow
Established workflow within the clinical setting can enhance the interprofessional team-based care referral process for CIH therapies, and nurses are the primary drivers of this referral process. 23,24 For example, improving CIH documentation within the context of a complex workflow has the potential to improve patient-centered care. 2 Developing efficient clinical workflows are challenging and require continued iterations to ensure the processes meet the needs of the interprofessional team. 22,25
Discussion
This scoping review provide an overview of research related to CIH therapy clinical documentation in EHRs. A majority of the studies used EHR data as a data source for analysis. The most frequent reason for the use of CIH therapies was pain, and a wide variety of types of CIH therapies were used. Documentation approaches, such as data standards and templates, may support CIH therapy documentation. A whole-systems approach, including documentation policy changes and development of core CIH data standards, can optimize existing electronic documentation infrastructure to support data quality and interoperability.
A majority of articles included in this study (78.8%) used EHR data for analysis. This is not too surprising given the nature of this scoping review. However, this suggests that the EHR is an important data source for analyzing the use of CIH therapies in clinical practice. This is consistent with the existing literature and shows increased use of EHR data for secondary data analysis. 10,26 A caveat (or caution) is reported to be inconsistent or missing documentation of integrative therapies from the EHR for a variety of reasons (e.g., patient nondisclosure or lack of patient/provider communication). 2,9 Inconsistent data may lead to misrepresentation of clinical practices and may not be indicative of real-world practice; thus, caution should be used when analyzing results. 9,20
Pain was the most frequent reason for the use of CIH therapies, and a wide variety of CIH therapies were used in the reviewed studies. This suggests that there is broad use of CIH therapies in clinical practice and aligns with national recommendations for the use of nonpharmacological therapies as first-line therapies to address pain management. 5,6 Current research shows that nurses are frequent users of integrative therapies; this suggests that nurses are in a prime position to lead system-wide efforts to improve CIH therapy documentation practices. 21,25
In addition, this has implications for nurse informaticians to develop recommendations to guide practice documentation changes and build the data infrastructure needed to support CIH therapy documentation. 27 –29 Future study should focus on the expansion of current CIH therapy documentation policies beyond pain management to other conditions, such as sleep disturbances, nausea, or anxiety. 4,27 This may provide additional guidance for EHR documentation and needed incentives required to support the data infrastructure for such documentation.
The finding that the most frequent documentation approach was data standards and templates suggests that the use of informatics methodologies should be further explored and implemented for CIH therapies. 18,24 This is consistent with previous literature recommending that data management and informatics infrastructure is needed to support documentation of CIH therapies. 30 –32 The development of CIH data standards, such as a core data set, can guide clinicians about what to document, foster continuity of care, and enhance the efficiency of health information exchange, which can optimize comparative effectiveness research. 5,18 CIH data standards are a primary prerequisite for realizing data-driven knowledge discovery, such as ML and AI techniques, and have potential to contribute to big data science. 33
A systems approach is needed to develop and optimize the current technology infrastructure needed for consistent CIH therapy documentation in EHRs. 28 This aligns with current frameworks developed to support a whole-systems approach and underscores the need for intentional system design. 24,30 A systems approach will require high-level conceptualization to recognize the interconnectedness between the “systems” across health care (e.g., quality improvement, systems analysts, informaticians, and clinicians).
For example, optimizing or enhancing existing infrastructure such as CIH therapy education and training, adjusting complex clinical workflow, and optimizing documentation (e.g., use of templates), can enhance CIH therapy care delivery. 24,29 Furthermore, the interconnected infrastructure of the EHR system has the potential to support interprofessional research, education, and clinical practice that will contribute to a Learning Health System. 34,35 Future research should examine the best practices needed to optimize a systematic approach to support the use and clinical documentation of CIH therapies. 13
Limitations
The limitations of this review include a scoping review by nature, which is narrow in focus and thus may not capture all current literature. A larger systematic review is needed to compare these findings. This scoping review focused on the published literature and may not be indicative of current clinical practices. An empirical analysis would be beneficial for examining real-world CIH therapy documentation practices in the clinical environment.
Conclusion
This scoping review identified trends in CIH therapy documentation within EHRs. EHR data are a growing data source for analyzing CIH therapies in clinical practice. Informatics approaches, such as data standards, can enhance documentation and enable data reuse for knowledge discovery and program evaluation. A systems approach that includes an interprofessional team (e.g., clinicians, nurses, informaticians, and researchers) is needed to advance CIH therapy use and representation in EHRs. This study is foundational to the development of a data management infrastructure to support CIH therapy documentation across care settings and enable data-driven approaches to facilitate CIH therapy knowledge generation.
Footnotes
Authors' Contributions
R.R.A., S.-C.L., R.J., and E.G.-S. contributed to the design and implementation of the research. R.R.A., S.-C.L., R.J., E.G.-S., M.K., M.J.K., and C.W.D. contributed to the analysis of the results and to the writing of the article. R.R.A. conceived the original and supervised the project.
Ethical Compliance
This study was deemed exempt from review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.