
Abstract
Introduction:
A previous 6-month report showed that adjunctive auricular acupoint stimulation (AAS) slowed myopia progression compared with 0.01% atropine (0.01% A) alone. This 12-month report was to determine whether the antimyopic effect of AAS, when added to 0.01% A, continued beyond treatment cessation, and explore the mode of action of AAS from the accommodative response.
Design and Interventions:
One hundred four children were randomly assigned to either a 0.01% A group or a 0.01% A + AAS group. Participants in the 0.01% A + AAS group received AAS in addition to 0.01% A for 6 months, and then kept using 0.01% A for the following 6 months. Participants in the 0.01% A group only used 0.01% A. The primary outcome was the difference in the mean cycloplegic spherical equivalent refraction (SER) from the baseline to the 12-month visit. Secondary outcomes included axial length (AL) and accommodative lag assessments.
Results:
The adjusted mean change from baseline to month 12 in the SER was −0.62 D for 0.01% A and −0.46 D for 0.01% A + AAS (difference, 0.16 D; p = 0.01), with a respective mean increase of 0.37 and 0.31 mm in AL (difference, −0.05 mm; p = 0.05). For the 5D near target, there was a reduction in the accommodative lag in children receiving add-on AAS relative to 0.01% A alone at 1 and 6 months (both p = 0.002).
Conclusions:
AAS treatment produced additional benefits >0.01% A in slowing myopia progression over the 12-month period, where the efficacy was sustained after the cessation of AAS. An effect of add-on AAS on reducing accommodative lag in response to 5D stimulus was found, but its role in mediating therapeutic response remained unclear.
Chinese Clinical Trial Registry number:
ChiCTR1900021316
Introduction
An alarming increase in the prevalence of juvenile myopia, particularly in educationally developed areas of East Asia, 1,2 has spurred research in the control of myopic progression. In the Atropine for the Treatment of Myopia (ATOM) study, 3 0.01% atropine eye drops (0.01% A) were considered the optimal concentration in slowing myopia progression with fewer side effects compared with higher concentrations of atropine (0.5%, 0.1%). Based on these findings, atropine has gained popularity among myopic children for the control of myopia progression. 4 In the subsequent Low-concentration Atropine for Myopia Progression (LAMP) study, 5 the efficacy of 0.05% atropine on myopia control was twice that of 0.01% atropine and well tolerated without apparent visual adverse effects. However, this formulation is not yet commonplace in worldwide clinical practice. 6 Auricular acupoint stimulation (AAS), an important part of Traditional Chinese Medicine, has been shown to enhance the effect of higher concentration atropine (0.25%, 7 0.125% 8 ) on myopia control. In the first 6-month (phase 1) results of the present study, 9 adjunctive AAS slowed myopia progression by 0.13 D compared with 0.01% A alone in Chinese children, demonstrating an additive effect. Of note, AAS's washout benefits have yet not been accounted for, even though its immediate benefits may be achievable. From the principle of evidence-based conservativism, rebound effects for myopia control treatments should be assumed until proven otherwise. 10 Investigating whether the benefits of AAS continue beyond treatment cessation in the second 6-month period (phase 2) would be more indicative of its ability to prevent myopia progression. 11
A core idea of AAS to treat human diseases in Traditional Chinese Medicine is that stimulation at specific auricular regions can modulate body physiology. 12 To understand the antimyopic effect of AAS within the framework of modern medicine, randomized clinical trials were conducted to observe its efficacy, and evaluate its influence on the accommodative response and choroidal thickness, which were generally assumed to influence the development of myopia. 13 The choroidal thickness change did not differ between groups in phase 1 study, 9 so considering it unlikely to be a major driver of the additive effect of AAS in slowing myopia progression. In contrast, the impact of AAS on the accommodative response was found in the early treatment period, and the whole 12-month outcomes were presented here.
We aimed to answer the following questions in this report: (1) whether the antimyopic benefits of adjunctive AAS remain upon completion of the intervention; (2) if benefits are linked to the change in accommodative response (thereby retinal defocus during near work).
Design and Interventions
Participants
The eligibility criteria had been described previously. 9 Enrolled children aged 7–12 years had myopic refraction between +0.50 D and −6.00 D, astigmatism <1.50 D in both eyes, and anisometropia <1.50 D as measured by cycloplegic autorefraction. In addition, those underwent any myopia control treatment before enrollment or with an allergy to atropine were excluded.
Study design
This was an open-label, randomized, assessor- and statistician-masked, controlled trial adhered to the CONSORT statement (Supplementary File S1). In phase 1, the participants were randomly assigned to receive 0.01% A + AAS or 0.01% A for 6 months, with follow-up at 1, 3, and 6 months. For the current phase 2 study, add-on AAS treatment was stopped, and all participants kept receiving 0.01% A for another 6 months. The study was approved by the Institutional Ethical Committee Review Board of Fudan University Eye & ENT Hospital (2019013) and registered with the Chinese Clinical Trial Registry, registered February 13, 2019 (
Interventions
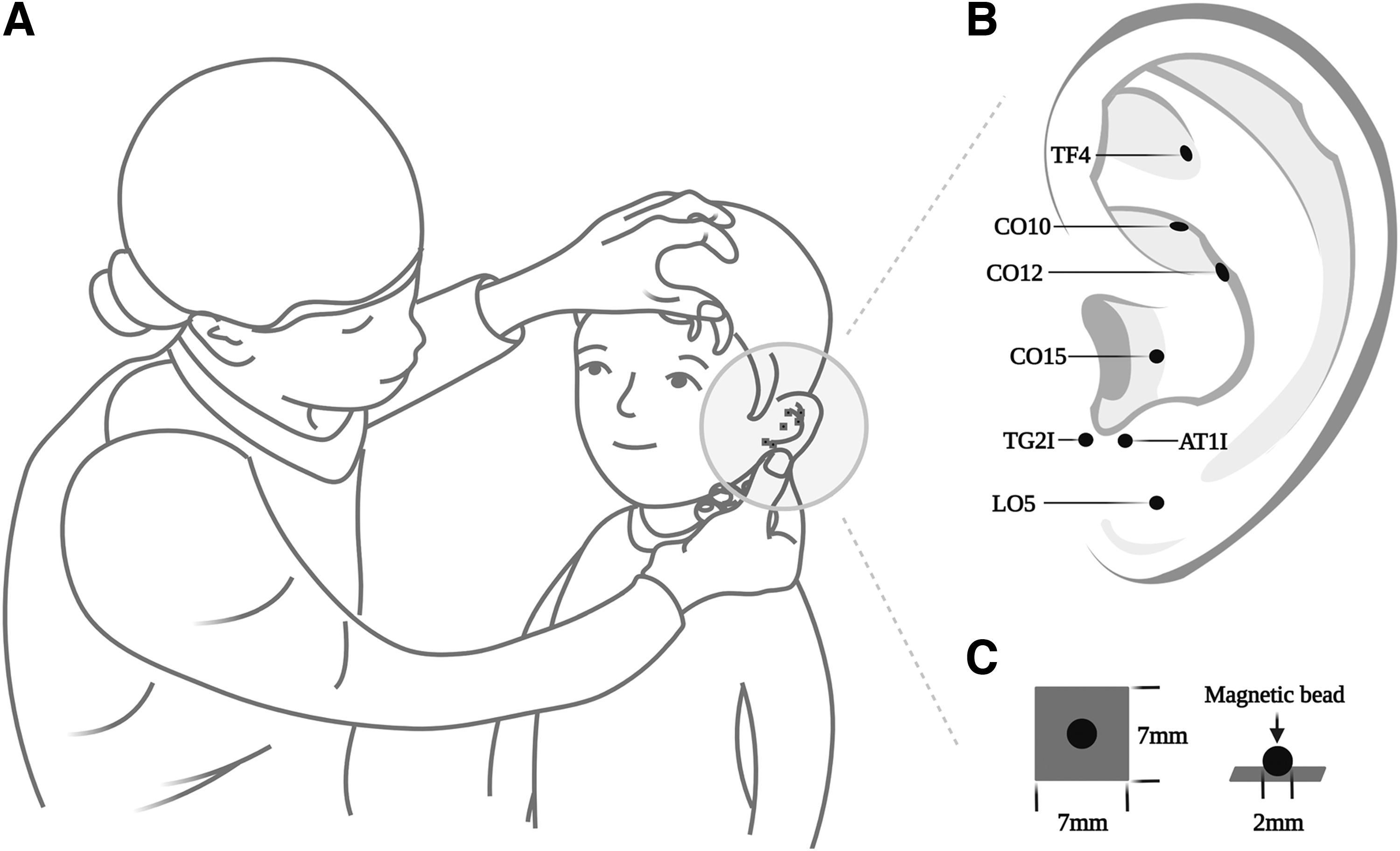
The 0.01% A were administered once every night for 12 months. They were prepackaged as eye drops in monodose preparations with atropine sulfate concentrations at 0.01% (0.4 mL:0.04 mg, preservative free; Xingqi Pharmaceutical Co., Ltd., Shenyang, China). Add-on AAS therapy in the 0.01% A + AAS group was administered with magnetic beads (Hwato, Suzhou Medical Appliance Factory Co., Ltd., Suzhou, China) at seven selected acupoints (LO5, TG2l, AT1l, CO15, CO12, CO10, TF4) and fixed with opaque adhesive patches (Fig. 1). Two ears received the treatment alternately from licensed acupuncturists weekly. A teaching video for locating the acupoints was distributed to the guardians, so they could reapply the magnetic beads to the acupoints when any of them fell off by chance. Quality control was performed through the instant photographs sent by the guardians. Any other concomitant therapies for myopia control were considered to violate the study protocol, for which participants would be withdrawn.
Stimulation to auricular acupoints
Outcome measures
The primary outcome was the difference in the mean cycloplegic spherical equivalent refraction (SER) between the baseline and the 12-month visit. The secondary outcome variables included the change of axial length (AL) and accommodative lag. Keratometry, anterior chamber depth (ACD), lens thickness (LT), intraocular pressure (IOP), and pupil size were also assessed as additional outcomes.
Cycloplegic SER was measured by WAM-5500 autorefractor (Grand Seiko Ltd., Japan) 14 30 min after the instillation of one drop of 0.5% alcaine and two drops of 1% cyclopentolate HCL. Measurements were taken while participants viewed a Maltese cross at 5 m to minimize any residual accommodation after cycloplegia. SER was measured five times and averaged. The AL, keratometry, ACD, and LT were then measured with IOL-Master 700 (Carl Zeiss Meditec, Inc., Germany). 15 Three measurements were made and averaged.
Before cycloplegia, IOP was measured by a noncontact tonometer (NT-510; NIDEK, CO., LTD, Japan); pupil size (560 lux) and noncycloplegic autorefraction were carried out also using WAM-5500; subjective refraction was performed to determine the distant prescriptions of the participants' spectacles. Accommodative response (lag of accommodation) was measured monocularly (the right eye) using the Hi-Speed (5 Hz continuous recording) mode of WAM-5500 for 30 sec at each of the four accommodative distances: 50 cm (2 D demand), 33 cm (3 D demand), 25 cm (4 D demand), and 20 cm (5 D demand). During the measurements, the participant with best spectacle correction fixated high-contrast Maltese cross targets through the beam splitter, while the left eye was occluded with an infrared filter. A 3-min break was taken between two consecutive recordings. The targets were displayed on an iPhone (1920 × 1080 pixels; Apple, Inc., Cupertino, CA, USA) and scaled for each viewing distance, such that they subtended the same visual angle at 98.1% Michelson contrast. The room was kept dark, except for the light from the targets and the computer screen.
Data analysis
The 30-sec photorefraction data were filtered offline to eliminate outlying data points unlikely to be physiologic. Readings were removed if the change in focus between two data points was >10 D/sec.
16
The remaining readings were averaged and used to calculate the accommodative lag as the difference between the measured accommodative response and accommodative stimulus by the following formulas
17
:
L = 1/(l* + d), l* and d (12 mm) are the distances from the eye to the target and lens, respectively; SR is the spectacle refraction; R is the average autorefractor reading referenced to the spectacle plane.
Statistical analysis
As described previously, 9 52 participants per arm would be needed to detect a 0.17 D treatment difference for the SER comparison.
Analyses were conducted based on a modified intention-to-treat principle (mITT), and only involved participants with outcome measurements at and after baseline. The missing data were imputed using the last observation carried forward method. Only data from the right eyes were used for analyses. Changes in parameters between the two groups were compared using the unpaired t-test or the Mann–Whitney U test. Within-group differences between different timepoints were assessed using paired t-tests or the Wilcoxon signed ranks test. Bonferroni's method was used to adjust the threshold for statistical significance. The model-adjusted changes from baseline in SER and AL were analyzed using a linear mixed model, with the change from baseline at each scheduled visit as the dependent variable. The model for the fixed effects includes gender, number of myopic parents, treatment, visit, and treatment-by-visit interaction, with age, baseline SER, and outdoor time as continuous covariates. Subgroup analyses were conducted by adding the main effect for the prespecified subgroup (age, gender, and baseline SER) in the model, and an interaction term between the subgroup and the treatment group. All effects tests were conducted at a two-sided alpha level of 0.05 using SPSS version 24.0.
Results
The trial started on April 13, 2019, and finished on July 4, 2021, of whom 104 were included and randomly assigned to treatment, and a final 100 were included in the mITT (Fig. 2). Commencing other antimyopic treatments was the most common reason for trial discontinuation in both groups. Baseline demographics and clinical characteristics were similar between the two groups (Table 1). Further, the demographics of the 90 participants who completed the 12-month observation were similar to those of the 14 participants who did not.
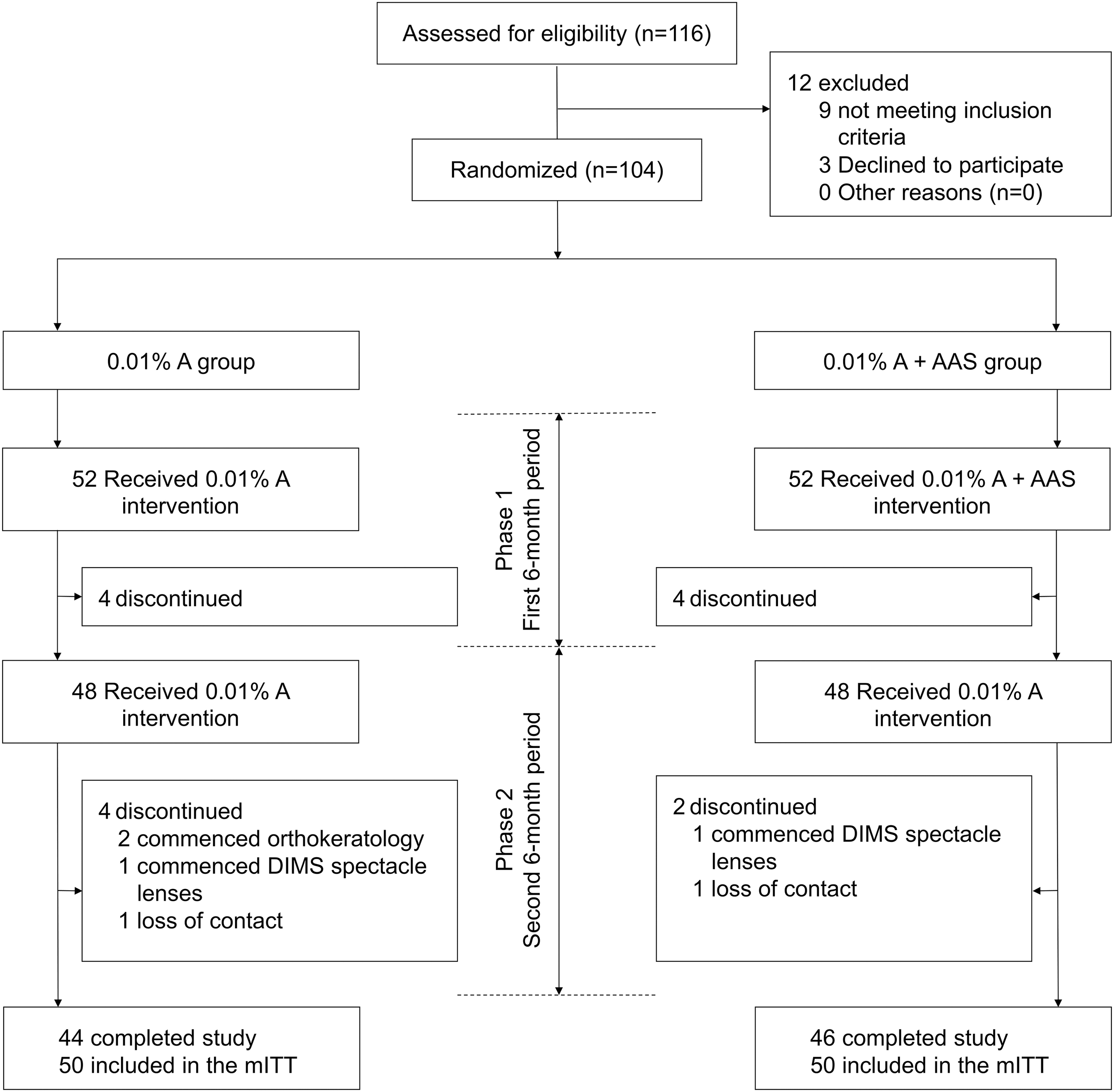
Trial profile. mITT, modified intention to treat.
Baseline Demographics and Clinical Characteristics of All Participants
Values are means (SD) or n (%).
Cumulative time outdoors from 7:00 to 17:00.
AAS, auricular acupoint stimulation; ACD, anterior chamber depth; AL, axial length; IOP, intraocular pressure; LT, lens thickness; SD, standard deviation; SER, spherical equivalent refraction.
Changes in SER over 12 months
At the end of 12 months, the unadjusted mean change in SER was −0.66 D in the 0.01% A group and −0.50 D in the 0.01% A + AAS group, for a between-group difference of 0.15 D (95% confidence interval [CI] 0.01–0.30 D; p = 0.03; Table 2). In a model adjusted by age, gender, baseline SER, number of myopic parents, and outdoor time, the 12-month difference in progression between 0.01% A and 0.01% A + AAS participants was 0.16 D (95% CI 0.04–0.29 D; p = 0.01), favoring the 0.01% A + AAS group (Fig. 3A). There was no evidence that the 6-month AAS add-on effect of 0.13 D was lost 6 months after discontinuing AAS treatment.
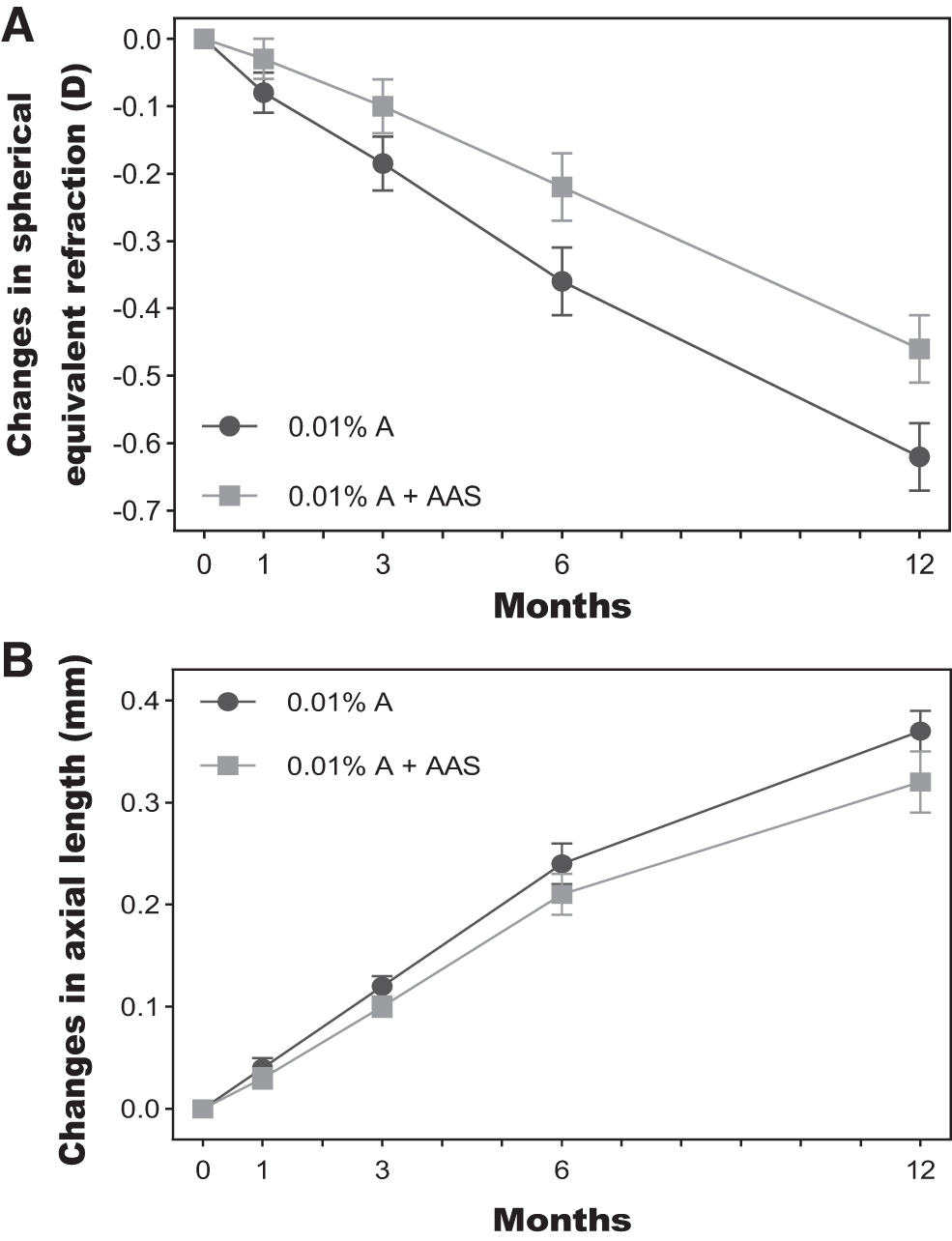
Model-adjusted mean change in SER
Primary and Secondary Outcomes
Values are means (SE). Each outcome was analyzed with unpaired t-test when normally distributed.
Analyzed using the Mann–Whitney U test.
CI, confidence interval; SE, standard error.
The difference in SER between 0.01% A and 0.01% A + AAS was 0.27 D among participants aged 7–9 years and 0.02 D in participants aged 10–12 years, with a borderline interaction between treatment and age (p = 0.06; Table 3). Scatter plots of age and 12-month SER change are shown in Figure 4. SER progression in the 0.01% A group was inversely correlated with age (R 2 = 0.19, p = 0.001). In contrast, no such correlation was found in the 0.01% A + AAS group (R 2 < 0.01, p = 0.52).
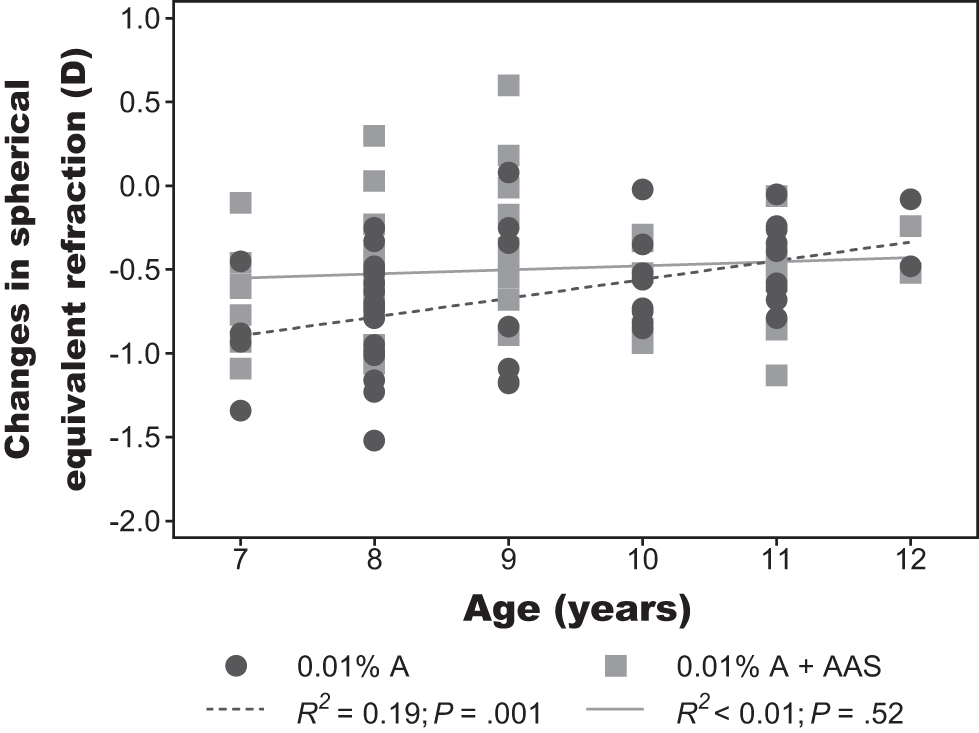
Correlation between the progression in SER and age of the participants.
Adjusted 12-Month Myopia Progression Between Study Groups by Baseline Characteristics
Values are means (SE).
p Value tests for the interaction between treatment and baseline characteristics.
Adjusted for age, gender, baseline spherical equivalent refraction, number of myopic parents, and outdoor time unless stratified by that factor.
Changes in AL over 12 months
The unadjusted 12-month change in AL was 0.37 mm in the 0.01% A group and 0.32 mm in the 0.01% A + AAS group, with a between-group difference of −0.04 mm (95% CI −0.11 to 0.02 mm; p = 0.13; Table 2). After adjusting for age, gender, baseline SER, number of myopic parents, and outdoor time, the difference between 0.01% A and 0.01% A + AAS participants was −0.05 mm (Fig. 3B) of marginal statistical significance (95% CI −0.10 to 0.00 mm; p = 0.05). A high significant correlation was found between the SER and AL progression in both groups (0.01% A: r = −0.76, p < 0.001; 0.01% A + AAS: r = −0.83, p < 0.001).
Changes in accommodative lag
The amount of lag for each near target in the 0.01% A and 0.01% A + AAS groups as a function of follow-up time is shown in Figure 5. Participants in the 0.01% A group generally had a consistent amount of lag throughout the observation period for either the 2D, 3D, or 4D near target. The accommodative lag for the 5D near target was elevated initially at month 1, but then returned to its baseline level. The lag in the 0.01% A + AAS participants showed a volatile downward trend during phase 1, followed by a rising trend during phase 2 in each of the four stimulus conditions. Significant between-group difference in the change of accommodative lag from baseline was only observed in 5D stimulus condition at 1 month (p = 0.002) and 6 months (p = 0.002), suggesting a downregulatory effect of add-on AAS on the accommodative lag in response to high accommodative stimuli. For participants in the 0.01% A + AAS group, the mean change from baseline to 6 months in the lag for the 5D target was not associated with either the 6-month (p = 0.19) or 12-month (p = 0.36) change in SER.

Accommodative lag as a function of follow-up time in the study groups.
Additional outcomes
Supplementary Figure S1 displays the average ACD, LT, pupil size, and IOP in the 0.01% A and 0.01% A + AAS groups as a function of each follow-up visit. There was no significant between-group difference in the change in these outcomes from baseline. The ACD showed an upward trend, whereas the LT showed a downward trend in both groups throughout the observation period. In both groups, the pupil size increased markedly at 1 month, and remained prominent at 3, 6, and 12 months. The IOP of both groups was statistically unchanged during the trial.
Discussion
In this report, adding 6-month AAS treatment to 0.01% A resulted in an adjusted reduction in SE progression of 0.16 D over the 12-month observation period in Chinese children, accompanied by a marginal decrease in axial elongation (−0.05 mm). Chinese clinicians have long used AAS as an alternative therapy for myopia control. However, the existing trials provide insufficient evidence to determine its effectiveness because of several methodological flaws, particularly short follow-up periods. 11,18 To our knowledge, only two studies conducted explored the antimyopic efficacy of AAS for ∼6 months. 7,8 In these two studies, adding AAS treatment to 0.25% and 0.125% atropine eye drops slowed myopia progression by 0.17 D7 and 0.25 D8 over 1 year, respectively. The present results have strengthened the evidence that adjunctive AAS can also improve the antimyopic effect of low-concentration atropine to a similar extent. Furthermore, the 0.13-D treatment effect of AAS in phase 1 did not wear off 6 months after discontinuing AAS therapy, implying that this therapy may target the underlying pathophysiologic mechanisms of myopia and, indeed, slow down the myopia progression. 10 Although a significant effect associated with add-on AAS on SER was detected, only a marginal effect on AL was detected. Since the sample size was calculated based on the primary outcome of SER, it may not be necessarily sufficient to detect statistical differences in AL between groups. However, the correlation coefficients for SER and AL progression were similar and high in both groups (0.01% A: r = −0.76; 0.01% A + AAS: r = −0.83).
Phase 1 report showed that children with higher myopia or lower age had greater 6-month add-on AAS treatment effects. 9 A similar trend was also observed at the 12-month follow-up, with the treatment effect of AAS particularly apparent in the younger subgroup. A post hoc analysis of the LAMP study suggested that younger age was the only risk factor for poor response to low-concentration atropine; higher concentration was required for younger children to achieve equivalent efficacy. 19 However, the 3-year results from the LAMP study reported a greater rebound effect of atropine associated with higher concentration and younger age at treatment cessation. 20 Taken together, it was considered that the combination of AAS and 0.01% A should be effective for younger children, which can both enhance the reduction in myopic progression and minimize the rebound effect of abrupt atropine withdrawal.
Hyperopic defocus with image plane formed posterior to the retina is considered a stimulant to eye growth. 21 –23 A prominent hypothesis for myopia development is that high levels of accommodative lag during near-work activities produces hyperopic retinal defocus that leads to accelerated axial elongation. 24 –26 Although longitudinal studies exploring the link between accommodative lag and subsequent myopia progression have come to conflicting conclusions, 27,28 a number of optical interventions that act to slow the progression of myopia at least partially work through reducing accommodation errors. 29 Li et al. reported that massage on myopia-related periocular acupoints compared with massage on sham acupoints reduced accommodative lag by 0.07 D in response to the 3D stimulus in the short term. 30 Zou found that AAS by thumbtack needles relative to nonintervention alleviated accommodative lag by 0.19 D in a 4-week observation. 31 The results of the present study showed that children treated with add-on AAS exhibited lower accommodative lag, and such response was lost after discontinuing AAS treatment, which further supports the downregulatory effect of acupoint stimulation on accommodative lag. Of note is that the significant effect only occurred in the 5D stimulus condition (20 cm). According to the data collected by an objective wearable device (Clouclip), 32 the average daily time spent within a working distance of <20 cm (equivalent to >5D accommodative stimulus) in Chinese children was ∼1.5–1.9 h, which was considered as a risk factor for myopia. Therefore, it was speculated that AAS has a potential in slowing myopia progression through reducing the level of accommodative lag, despite the negative findings of correlation between the change in accommodative lag and SER in this study. Future studies with longer observational period and larger sample size are needed to further explore this correlation.
Atropine, a nonspecific muscarinic receptor antagonist, can paralyze ciliary muscle contraction. Most of the available studies reported that 0.01% A had a subtle effect on accommodation amplitude, 33 –35 but very few studies focused on its influence on accommodative response/lag. It was found that participants experienced a slight increase of accommodative lag for 5D near target after 1-month 0.01% A treatment, although the lag returned to baseline at 3 months and remained stable thereafter. In a study by Mitsukawa et al., 36 with the 5D accommodative stimulus condition, the ACD and posterior curvature of the lens 1 h after instillation of 0.01% A were significantly larger compared with those at baseline. This study did not directly measure the accommodative response. Still, the changes in these ocular biometric components supported a decrease in the accommodative response to 5D stimulus, in line with the findings presented in the present study. Despite that, a relatively transient and slight lag-raising effect of 0.01% A was unlikely to promote myopia progression.
In addition to several limitations mentioned in the phase 1 report, future investigation may need to address the following puzzles: (1) whether continuing AAS treatment as opposed to discontinuation after 6 months would further reduce myopia progression; (2) whether AAS acted independently or in synergy with atropine to slow myopia progression.
Conclusions
In summary, in this 12-month study of AAS added to 0.01% A for myopia control, supplemental AAS therapy resulted in a significant reduction in myopia progression, where the treatment effect was sustained after discontinuing AAS. Add-on AAS reduced accommodative lag in response to high accommodative stimulus (5D), yet its role in mediating the therapeutic response should be interpreted with caution.
Footnotes
Authors' Contributions
X.K., G.Y., Z.C., R.H., and Y.Z.: contributed equally to this study. X.K. assisted with writing—original draft, funding acquisition, methodology. G.Y. designed conceptualization, writing—review and editing. Z.C. contributed to writing—review and editing, resources and methodology. R.H. performed investigation, resources, validation. Y.Z. contributed to writing—original draft, funding acquisition, methodology. L.Z. and X.G. conducted investigation. Z.S. assisted with supervision and resources. D.Z. provided visualization and data curation. Y.Y. performed formal analysis and data curation. J.L. provided software. XZ contributed to writing—review and editing, project administration, and supervision. X.M. designed conceptualization, project administration, supervision, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The work was supported by Shanghai Municipal Health Commission (20194Y0210, ZY(2021-2023)-0105-17) and Shanghai Sailing Program (22YF1444400). The funding sources had no role in the design of the study and collection, analysis, interpretation of data or in writing the article.
Supplementary Material
Supplementary Figure S1
Supplementary File S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.