
Abstract
Purpose:
To investigate the effect of walking meditation on vascular function, aerobic fitness, and quality of life in breast cancer patients receiving anthracycline chemotherapy and compare with the nonexercising control group.
Methods:
Patients aged 40–60 years with newly diagnosed, histologically confirmed resected stage I–II breast cancer were studied in a parallel randomized controlled trial. The participants were randomly assigned to either the nonexercising control group (n = 15) or the Buddhist walking meditation group (n = 15). All participants received four cycles of anthracycline chemotherapy every 3 weeks starting at 2 weeks before the start of the exercise intervention. The walking meditation group performed home-based mindfulness walking exercises at a moderate exercise intensity for 30 min/session, 3 times/week for 12 weeks. The primary outcome measures were vascular reactivity (flow-mediated dilation [FMD]) and arterial stiffness (brachial–ankle pulse wave velocity [baPWV]).
Results:
Eleven participants from each group completed the entire study. Analysis of variance with repeated measures indicated that FMD and peak oxygen consumption (VO2peak) decreased in both groups after the initiation of anthracycline chemotherapy (all p < 0.05). After the exercise intervention, FMD, VO2peak, peak stroke volume, and peak cardiac output remained lower in the controls, but improved in the walking meditation group (all p < 0.05). baPWV increased in the control group, while no such change was observed in the walking meditation group. There were no significant changes in blood cortisol, malondialdehyde, and interleukin-6 concentrations in both groups. Overall quality of life decreased after 2 weeks of anthracycline chemotherapy in both groups (all p < 0.05). However, the walking meditation group improved many of these symptoms significantly (all p < 0.05), while no such changes were observed in the control group.
Conclusions:
Buddhist walking meditation exercise was effective in mitigating cardiotoxicity of anthracycline chemotherapy on vascular function, aerobic fitness, and quality of life in breast cancer patients.
Clinical trial registration number:
NCT02676531
Introduction
Breast cancer is the most common malignancy among women worldwide. 1 Advancements in the cancer therapies have contributed to dramatic improvements in survival, but many of these therapies, particularly anthracycline chemotherapy, are associated with cardiovascular toxicities 2 creating the new discipline of cardio-oncology. 3 Indeed, patients receiving anthracycline chemotherapy demonstrate vascular disorders including vascular stiffening and endothelial dysfunction. 4
Current strategies to mitigate cardiotoxicity associated with anthracycline treatment include dose reductions, modified administrations, liposomal formulations, and coadministrations of cardioprotective medications. 5 However, these procedures may result in compromised oncologic treatment and management. 6 In addition, patients with breast cancer commonly have undesirable physical symptoms such as pain, sleep disturbances, fatigue, psychological symptoms, 7 and reduced quality of life. 8 Therefore, more effective preventive modalities that simultaneously act on “mind and body” are urgently needed to reduce risks of cardiovascular and other complications in patients receiving anthracycline chemotherapy.
Exercise interventions are generally safe in patients with breast cancer and can be used to reduce fatigue, chemotherapy-induced peripheral neuropathy, cancer-related cognitive impairment, and mortality rate. 9 However, the influence of exercise intervention on cardiovascular disease and its risk is not well documented during breast cancer treatment. Walking meditation is a widely performed form of Buddhist practices that focuses on mind–body interactions. It incorporates the basic principles of traditional Buddhist meditation performed in the sitting position, including breathing, awareness, concentration, and relaxation, with rhythmic walking. 10,11
The authors have previously demonstrated that walking meditation, a spirituality-based physical and mental exercise program, was effective not only in improving cardiometabolic health and but also in reducing stress levels in patients with type 2 diabetes. 11 In addition, Buddhist walking meditation that incorporated arm-swing exercises was also effective in improving the physical and psychological function in elderly women with mild and moderate depression symptoms. 10 Given the fact that breast cancer patients undergoing anthracycline chemotherapy suffer from multiple comorbidities, walking meditations that could act on multitudes of physical and psychological health might be particularly beneficial. However, this possibility has not been tested.
Accordingly, the primary aim of the present study was to determine the effect of Buddhist walking meditation on vascular function, aerobic fitness, and quality of life in breast cancer patients receiving anthracycline chemotherapy and compare with the nonexercising control group that received anthracycline chemotherapy only. The authors hypothesized that 12 weeks of Buddhist walking meditation would demonstrate improvements in vascular endothelial function, arterial stiffness, cardiorespiratory fitness, and quality of life in patients with breast cancer receiving anthracycline chemotherapy, while the nonexercising control group would exhibit worsening of these factors.
Methods
Participants
Middle-aged women aged 40–60 years with newly diagnosed histologically confirmed resected stage I–II breast cancer scheduled for the first-line adjuvant anthracycline chemotherapy were recruited for study participation at the King Chulalongkorn Memorial Hospital. The exclusion criteria included history of malignancy, chronic diseases such as acute/chronic renal failure, ischemic heart disease, chronic obstructive pulmonary disease, myasthenia gravis, current pregnancy, chronic smoking, and chronic alcohol drinking. The candidates were excluded if they had contraindications to chemotherapy, absolute contraindications to exercise training (e.g., recent myocardial infarction), unwillingness to participate in exercise training sessions, a lack of approval of their primary attending oncologists, and previous performance of walking meditation. Elimination of patients with comorbidies was necessary to minimize significant risks associated with exercise training because all the exercise training was conducted at home without direct clinical supervision. Before participation, all of the participants provided written informed consent.
The study was approved by the Institutional Review Board at Chulalongkorn University. The trial was registered with
Participants receiving adjuvant anthracycline chemotherapy were randomly assigned to the control group (n = 15) or the walking meditation exercise group (n = 15). Randomization was performed immediately after the inclusion of an eligible patient. Randomization sequence was created using Excel 2013 (Microsoft, Redmond, WA) with a 1:1 allocation using random block sizes of 6 (Supplementary File S1, CONSORT 2010 Checklist). Randomization sequence was organized and conducted by a clinical staff who was not involved in day-to-day operation of the testing and procedures. The control group was a nonexercising control group that underwent routine clinical therapy. They were contacted by investigators every 3–4 weeks. No exercise was prescribed to the control group. The walking meditation group performed home-based mindfulness walking exercises at a moderate exercise intensity for 30 min/session, 3 times/week for 12 weeks.
Adjuvant anthracycline chemotherapy was started 2 weeks before the beginning of the exercise intervention and consisted of four cycles of doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2) every 3 weeks, for a total of 12 weeks. Before the initiation of therapy, patients underwent clinical cardiac assessments using the echocardiogram to minimize the potential risks of physical exercise. Adverse events were recorded in both groups regardless of their severity and/or perceived causal relation to the intervention.
Walking meditation exercise intervention
The walking meditation exercise program was composed of home-based (i.e., unsupervised) mindfulness walking exercises. Before the initiation of the exercise program, detailed face-to-face instructions involved in the walking meditation exercise were given to each participant. During walking, the participants listened to a sound audio rhythm (MP3 recorder) at 25 beats/min, voiced “Budd” and “Dha,” and concentrated on squeezing rubber balls in both hands rhythmically and simultaneously. The walking meditation exercise program was divided into two phases. In phase 1 (weeks 1–6), the walking exercise was performed at an intensity of 41%–50% of individual heart rate reserve (HRR) for 30 min (separated in 3 intervals, 10 min/interval with 3-min rest between the intervals), 3 times per week.
In phase 2 (weeks 7–12), the walking meditation exercise was performed at an intensity of 51%–60% of HRR for 45 min (separated in 3 intervals, 15 min/interval with 3-min rest between the intervals), 3 times per week. Exercise intensity was determined with the Karvonen formula: % of target exercise intensity (e.g., 50%) × (maximal heart rate – resting heart rate) + resting heart rate. Adherence to the prescribed exercise intensity was confirmed using heart rate monitors (Polar® FT7, Kempele, Finland) that the participants were required to wear during each exercise session. The heart rate data were downloaded by the investigators for further analyses, and the subsequent feedback was delivered to the participants in terms of staying in the target heart rate zone during exercise. In addition, exercise logs were filled out by the participants, and random calls were made to the participants every week to confirm adherence to the exercise program.
Measurements
The primary outcome measures were vascular reactivity (flow-mediated dilation [FMD]) and arterial stiffness (brachial–ankle pulse wave velocity [baPWV]). The authors also collected aerobic fitness (peak oxygen consumption [VO2peak]) and quality of life as the secondary outcome measures. As illustrated in Figure 1, measurements were performed 3 times; before anthracycline chemotherapy (Baseline), before the exercise intervention (Pre-intervention

The schematic diagram showing the study design.
General physiological characteristics
Body composition was determined by bioelectrical impedance using a standardized body composition analyzer (Whole Body Bioelectrical Impedance Analysis, ioi 353; Jawan Medical). Dietary intake and fluid intake before the body composition measurement were standardized before and after the intervention period. Heart rate and blood pressure were recorded after >5 min of resting in the seated position using a semiautomated blood pressure device (CARESCAPE V100 monitor; GE Healthcare, Milwaukee, WI). Physical activity level was assessed using the Global Physical Activity Questionnaire (GPAQ) developed by the World Health Organization (WHO). 12
The GPAQ consisted of 16 items that measured physical activity for work, travel to and from places, recreational activities, and time spent in inactivity, and quantified the physical activity levels of a normal active week for the participants. Activities were classified into three intensity levels: inactivity (1 metabolic equivalent [MET]), moderate (4 METs), and vigorous (8 METs). The duration and frequency of physical activity over a typical week were recorded and calculated to total physical activity per week (MET-min/week).
Heart rate variability
Heart rate variability (HRV) was recorded using the Polar chest strap ECG measuring device (RS800CX; Polar Electro Oy, Kempele, Finland). The RR intervals were recorded and transferred to the Polar Precision Performance software (v. 3.0; Polar Electro). Cardiac interval variability was evaluated into the frequency domain by means of spectral analysis. Total power and low-frequency and high-frequency power were appointed in absolute values of power. 13
Vascular function
FMD was measured as an index of endothelium-dependent vasodilation using the blood flow occlusion technique on the forearm as previously described. 10,11 All the vascular measurements were performed around the same time of the day throughout the study after controlling for the influence of prior exercise and diet. The brachial artery was imaged above the antecubital fossa in the longitudinal plane with the ultrasound machine (Philips CX50, Andover, MA). Arterial diameter was measured using a computer software program (Brachial Analyzer; Medical Imaging Applications, Coralville, IA). Brachial artery mean blood flow velocity was measured with duplex ultrasound and analyzed using software integral to the ultrasound machine. FMD was calculated using the formula (D2–D1) × 100/D1, when D1 is the brachial artery diameter at baseline, and D2 is the maximal postocclusion brachial artery diameter. 14
Shear rate was calculated using the following equation: 4 × time average mean blood velocity (cm/sec)/baseline brachial artery diameter (mm). 15 baPWV, a measure of arterial stiffness, was measured using a noninvasive vascular testing device (Omron Healthcare VP-1000plus, Kyoto, Japan). Waveforms were obtained from plethysmographic sensors in blood pressure cuffs placed on both arms and ankles as previously described. 16
Blood biochemistry analyses
A venous blood sample was collected from the antecubital vein after an 8-h fasting period. Complete blood count, cortisol, high-sensitivity C-reactive protein (hs-CRP), malondialdehyde (MDA), interleukin-6 (IL-6), and total nitric oxide (NO) concentrations were measured according to the standard procedure at a certified clinical chemistry laboratory (National Healthcare Systems Co.). Total NO was a measure of nitrite and nitrate in the blood sample.
Cardiorespiratory fitness
Cardiopulmonary exercise tests were performed with the Bruce protocol on the treadmill to determine VO2peak. Pulmonary ventilation and gas exchange were measured using breath-by-breath cardiopulmonary gas exchange system (Stationary Gas Analyzer; Vmax Encore 29 System, Yorba Linda, CA). Oxygen consumption was considered “peak” if two of the following three criteria were met: (1) age-predicted maximal heart rate within 10 bpm; (2) respiratory exchange ratio of >1.10; and/or (3) volitional exhaustion. 17 VO2peak was a 30-sec average of the highest VO2. Stroke volume and cardiac output were determined at rest and during peak exercise for each subject by a transthoracic electrical bioimpedance meter (PhysioFlow® PF07 Enduro™, Poissy, France) as previously described. 18
Quality of life
Quality of life was assessed using a questionnaire of the European Organization for Research and Treatment of Cancer (EORTC)—quality of life of patients with cancer QLQ-C30 (version 3.0) with 30 questions. 19 The questionnaires consisted of global health status, physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning, as well as scales of symptoms such as fatigue, nausea and vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties.
Statistical analyses
The sample size calculation was conducted using the G*power software version 3.1.9.2 (Heinrich-Heine-Universitat, Dusseldorf, Germany) on previously reported data on VO2peak in breast cancer patients receiving neoadjuvant chemotherapy following supervised moderate intensity aerobic exercise. 20 A 4.1 mL/kg/min difference in mean VO2peak between the aerobic exercise trainings in combination with neoadjuvant doxorubicin–cyclophosphamide and drug alone from pre- and postintervention. With a two-sided, 0.05 significance level and VO2peak as the primary variable using a two-group F-test, total sample size = 12 subjects (6 subjects in each group) would allow us to detect a significant difference between the groups at 80% statistical power.
Statistical analyses were performed using the SPSS software package (SPSS, Chicago, IL). Before the statistical analyses, tests for normality were conducted using the Shapiro–Wilk test. For each variable, the authors have constructed box plot analyses to visualize the data. Outliers defined as data points that are 3 standard deviation (SD) away from the mean were eliminated from the data analyses. They had only few data points that were removed for being outliers and a few missing data points.
These few data were dealt with the imputation methods after the authors determined that these data were found to be missing completely at random and that inclusion or elimination of these data points did not impact the primary findings and data interpretation. The 2 × 3 (group × time) analysis of variance with repeated measures followed by Bonferroni multiple comparisons was used to determine significant differences among all variables. Associations between variables were determined using Pearson correlation analyses. Significance was set a priori at p < 0.05. All data are expressed as mean ± SD.
Results
As shown in Figure 2, the eligible participants were randomly allocated into two groups: the nonexercising control group (n = 15) or the walking meditation exercise group (n = 15). A total of eight participants dropped out of the study. Therefore, each group comprised 11 participants for the final analyses. Following the anthracycline chemotherapy treatment, 10 patients (6 in the control group and 4 in the walking meditation) received tamoxifen, 9 patients (4 in the control group and 5 in the walking meditation) received other chemotherapy, and 3 patients (1 in the control group and 2 in the walking meditation) received tamoxifen combining with radiation.
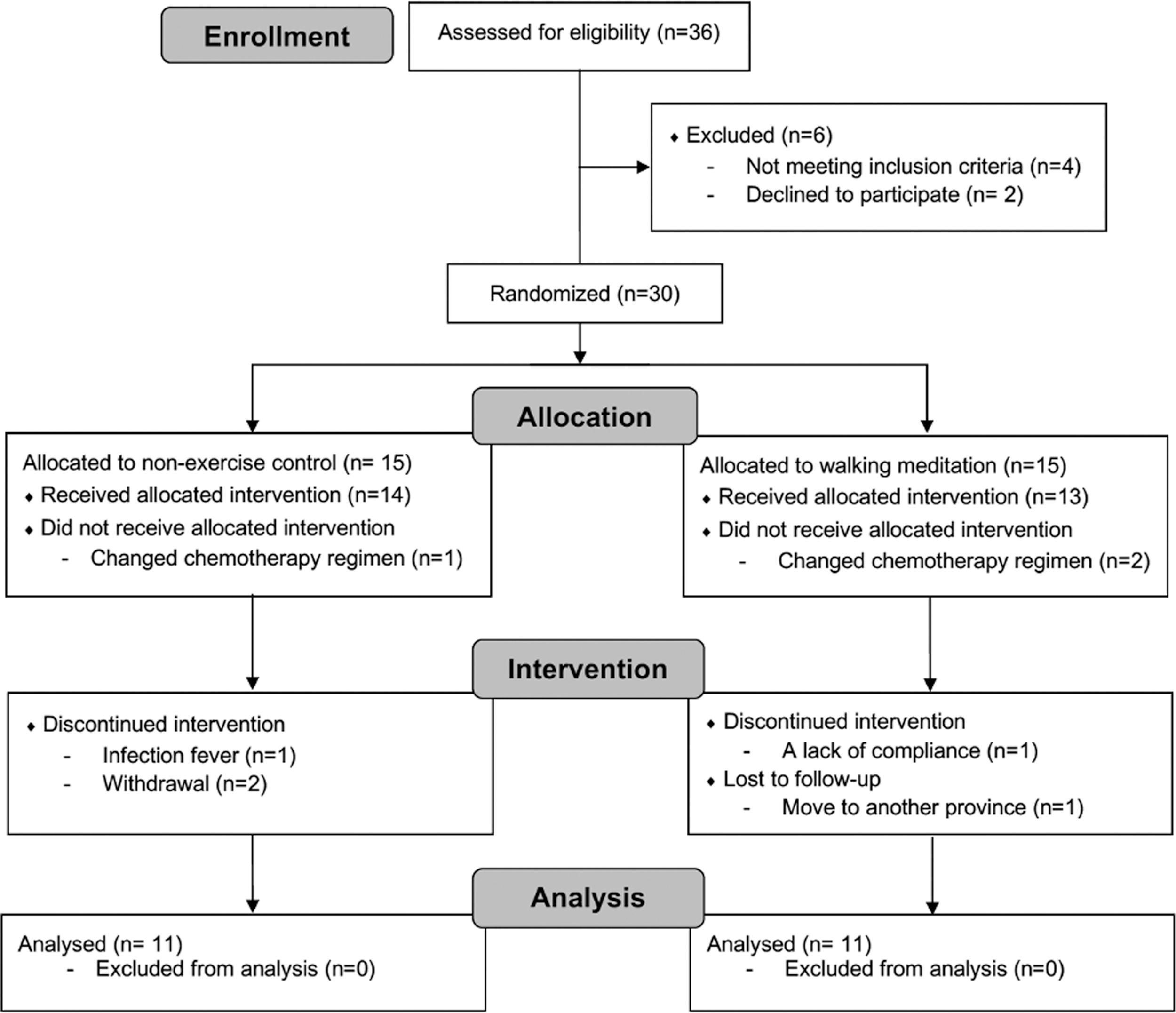
Flow of trials through the participant selection process.
The general characteristics of the subjects are shown in Table 1. All the partipants were Thai. There were no significant baseline group differences in the participant characteristics, including body mass, body mass index (BMI), and body fat percentage. None of the body composition variables showed significant changes throughout the study. Physical activity levels, as measured in work, recreation, and total, decreased significantly after the initiation of anthracycline chemotherapy in both groups (all p < 0.05). However, the walking meditation group had greater work, recreation, and total physical activity following the exercise intervention (all p < 0.05).
Selected Characteristics of the Participants in the Nonexercising Control and Walking Meditation Groups
Data are mean ± SD (95% CI).
p < 0.05 vs. baseline in the same group.
p < 0.05 vs. preintervention (2nd week AC) in the same group.
p < 0.05 vs. postintervention (14th week AC) in the controls.
AC, anthracycline chemotherapy; ANOVA, analysis of variance; BMI, body mass index; CI, confidence interval; HF, high frequency; LF, low frequency; MET, metabolic equivalent; SD, standard deviation.
No serious adverse events, accidents, or other adverse events that exceed the indicated frequency threshold were reported in either group even though one participant from the control group had an infection fever and discontinued from the study participation. Adherence and compliance of 92% to the walking meditation were found as evidenced by the exercise log and heart rate monitors returned to the investigators. Both control and walking meditation groups did not show significant changes in HRV.
As shown in Table 2, heart rate at rest increased in both groups after the initiation of anthracycline chemotherapy (all p < 0.05). The corresponding increases in peak stroke volume and peak cardiac output were observed in the walking meditation group (all p < 0.05) and these changes were greater than the control group (all p < 0.05).
Changes in Cardiovascular and Hemodynamic Measures in the Nonexercising Control and Walking Meditation Groups
Data are mean ± SD (95% CI).
p < 0.05 vs. baseline in the same group.
p < 0.05 vs. preintervention (2nd week AC) in the same group.
p < 0.05 vs. postintervention (14th week AC) in the nonexercising controls.
AC, anthracycline chemotherapy; ANOVA, analysis of variance; BP, blood pressure; CI, confidence interval; SD, standard deviation.
The main cardiovascular indicators are shown in Figure 3. FMD decreased in both groups after receiving anthracycline chemotherapy (all p < 0.05). However, after the intervention, FMD increased in the walking meditation group (p < 0.05), whereas FMD stayed depressed in the nonexercising control group. The walking meditation group had greater increases in FMD than the nonexercising control group (p < 0.05). Arterial stiffness as measured by baPWV increased after the intervention in the control group, while no significant change was seen in the walking meditation group, with no differences between the groups. VO2peak decreased in both groups after the initiation of anthracycline chemotherapy (all p < 0.05). After the exercise intervention, VO2peak remained depressed in the control group but increased in the walking meditation group (p < 0.05).

Changes in the main cardiovascular indicators in the nonexercising control and walking meditation groups. Data are mean ± SD (95% CI). *p < 0.05 versus baseline in the same group, † p < 0.05 versus pretraining (2nd week AC) in the same group, ‡ p < 0.05 versus postintervention (14th week AC) in the nonexercise controls. AC, anthracycline chemotherapy; baPWV, brachial–ankle pulse wave velocity; CI, confidence interval; FMD, flow-mediated dilation; hs-CRP, high-sensitivity C-reactive protein; SD, standard deviation; VO2peak, peak oxygen consumption.
This group difference was significant (p < 0.05). hs-CRP increased in both groups after anthracycline chemotherapy (all p < 0.05). The level of hs-CRP remained elevated in the control group, but decreased in the walking meditation group (all p < 0.05). The walking meditation group had a lower level of hs-CRP than the control group (p < 0.05). Changes in VO2peak were not associated with the corresponding changes in vascular function including FMD and baPWV.
As shown in Table 3, hemoglobin, hematocrit, absolute neutrophil count, and white blood cell count decreased in both groups after anthracycline chemotherapy (p < 0.05). There were no significant changes in blood cortisol, MDA, IL-6, and total NO concentrations in both groups, with no significant differences between the groups.
Changes in Blood Chemistry Variables in the Nonexercising Control and Walking Meditation Groups
Data are mean ± SD (95% CI).
p < 0.05 vs. baseline in the same group.
p < 0.05 vs. preintervention (2nd week AC) in the same group.
p < 0.05 vs. postintervention (14th week AC) in the nonexercising controls.
AC, anthracycline chemotherapy; ANC, absolute neutrophil count; ANOVA, analysis of variance; CI, confidence interval; MDA, malondialdehyde; NOx, nitrogen oxide; SD, standard deviation; WBC, white blood cell.
The data on quality of life are shown in Table 4. Overall quality of life as assessed by global health decreased after 2 weeks of anthracycline chemotherapy in both groups (p < 0.05). Fatigue, nausea and vomiting, dyspnea, insomnia, and appetite loss symptoms increased in both groups (all p < 0.05). Global health status, emotional functioning, and social functioning decreased after 2 weeks of anthracycline chemotherapy in both groups (all p < 0.05). However, the walking meditation group improved these symptoms significantly (all p < 0.05), while no significant changes were observed in the control group. Global health status was found to be higher in the walking meditation group than in the control group (p < 0.05).
Changes in Quality of Life as Assessed by the European Organization for Research and Treatment of Cancer QLQ-C30 in the Nonexercising Control and Walking Meditation Groups
Data are mean ± SD (95% CI).
p < 0.05 vs. baseline in the same group.
p < 0.05 vs. preintervention (2nd week AC) in the same group.
p < 0.05 vs. postintervention (14th week AC) in the nonexercising controls.
AC, anthracycline chemotherapy; ANOVA, analysis of variance; CI, confidence interval; QoL, quality of life; SD, standard deviation.
Discussion
This is the first study to report the beneficial effects of Buddhist walking meditation on cardiotoxicity indices that are relevant to cancer populations. Anthracycline chemotherapy rapidly and persistently reduced endothelium-dependent vasodilation. The present results are consistent with previous studies that reported decreased endothelial function in breast cancer patients undergoing chemotherapy. 21 –23 These effects have been attributed to anthracycline causing apoptosis of vascular endothelial cells 24 resulting in a reduced bioavailability of NO. 25 Walking meditation exercise performed during chemotherapy improved FMD significantly to the level that was not different from the baseline and normalized the endothelial dysfunction.
Interestingly, significant changes in FMD (functional indicator of endothelium-dependent vasodilation) were not associated with the corresponding changes in shear rate (stimuli for FMD) or total NO (biochemical indicator of endothelial function) as the authors did not observe significant changes in these variables. 26,27 Moreover, arterial stiffening that was observed in the control group was absent in the walking meditation group. Collectively, these results indicate that walking meditation exercise could enhance key vascular function even during chemotherapy in patients with breast cancer.
Regular aerobic exercise is associated with significant improvements in cardiorespiratory fitness and related outcomes across a broad range of oncology settings. 28 The results of meta-analysis indicated that cardiorespiratory fitness remained low or became even further impaired in patients during adjuvant therapy, but exercise training was associated with a significant increase in cardiorespiratory fitness. 29 In the present study, walking meditation exercises performed at a moderate intensity for 30–45 min, 3 times per week, produced significant improvements in VO2peak. Consistent with the Fick equation, the increase in VO2peak was associated with the corresponding increases in peak cardiac output and peak stroke volume. Moreover, walking meditation was accompanied by greater total physical activity as well as work and recreation activities after 12 weeks of walking meditation. Collectively, these results indicate that the Buddhist walking meditation was highly effective in enhancing aerobic fitness in breast cancer patients receiving anthracycline chemotherapy.
In the present study, it is not possible to attribute the effects of walking meditations separately to the physical components (aerobic walking) and mental components (Buddhist meditation). The overall benefits of regular aerobic exercise have been well established, but the additive effects of meditations or mindful exercises are not known. However, at least two previous studies compared the effects of Buddhist walking meditation and the traditional aerobic walking programs. 10,11 In depressed elderly women, depression symptom was reduced, and low density lipoprotein-cholesterol, cortisol, and IL-6 concentrations were decreased only in the walking meditation group as no such changes were observed in the aerobic exercise-only group. 11 Similarly, in a study involving patients with type 2 diabetes, significant decreases in hemoglobin A1c, systolic blood pressure, and arterial stiffness were only observed in the walking meditation group, and no such changes were seen in the traditional walking group. 10
Taken together, these results suggest that a combination of physical exercise with mental exercise as seen in the walking meditation may elicit greater benefits on a variety of systems and cardiovascular risk factors.
The decrease in aerobic capacity was significantly associated with the decrease in the overall quality of life during breast cancer treatment. 30 Anthracycline chemotherapy decreased quality of life quickly within 2 weeks in most patients with breast cancer. The most affected changes at the 2nd week after receiving anthracycline chemotherapy were global health status, fatigue, nausea, vomiting, and dyspnea. Regular exercise has been shown to play an important role in determining quality of life among women with breast cancer. 31 A recent study reported that 10-week moderate-intensity aerobic exercise improved the global quality of life and physical functioning component in survivors of breast cancer. 31 Mindfulness-based exercise may be superior to gentle exercise alone for improving self-report of cognitive function and distress after treatment for breast cancer. 32
In the present study, walking meditation was effective in attenuating these changes in many aspects of quality of life including global health status and physical and emotional functioning, but did not affect fatigue, nausea and vomiting, and dyspnea.
Study limitations
There are a number of limitations in the present study that should be emphasized. First and most importantly, the number of subjects studied is relatively small. As such, the results should be interpreted with caution. Second, the walking meditation used in the present study was based on the Buddhist practices and was prescribed to Buddhist believers as the majority of Thai practice Buddhism. It is not known if this would be effective when applied to non-Buddhist practitioners. However, this novel form of walking meditation can be modified for believers of different religions. For instance, instead of “Budd” “Dha” used in the present study, Christians could chant “Je” “Sus” and Muslims “All” “Lah.”
Third, the walking meditation group seems to have lower body mass, BMI, and body fat percentage, and higher peak O2 uptake at baseline compared with the nonexercising control group. However, group differences were not statistically significant and are fairly small within the ranges that are considered to be normal. More importantly, because of the “law of initial baseline,” it will be harder to induce improvements in those who have better baseline fitness scores. So, if there is any influence of the baseline group differences, the impact of walking meditation may have been underestimated.
Conclusion
In conclusion, fairly rapid deteriorations of cardiovascular fitness, vascular function, and quality of life were visible within a few weeks of initial anthracycline exposure. Those cardiotoxicities got worse during the subsequent anthracycline chemotherapy as seen in the nonexercise control group. In contrast, walking meditation exercise produced increases in cardiovascular fitness and hemodynamics at peak exercise and improvements in endothelium-dependent vasodilation. In addition, the overall quality of life was significantly elevated by walking meditation exercise to the level that is equivalent to the prechemotherapy levels. Collectively, these results indicate that walking meditation that incorporates physical exercise of walking and mental meditations mitigated cardiotoxicities associated with anthracycline chemotherapy in breast cancer patients. More importantly, these effects were achieved in the home-based exercise settings.
Footnotes
Authors' Contributions
S.S. was involved in conceptualization, methodology, data curation, project administration, and writing—original draft. N.P. was involved in conceptualization, methodology, supervision, and project administration. H.T. was involved in conceptualization, supervision, and writing—review and editing. D.S. was involved in conceptualization, methodology, funding acquisition, data curation, supervision, project administration, and writing—review and editing.
Author Disclosure Statement
All the authors declare that there are no conflicts of interest.
Funding Information
This study was supported by the 100th Anniversary of Chulalongkorn University Fund for doctoral scholarship.
Supplementary Material
Supplementary File S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.