
Abstract
Background:
As a mind–body therapy, music may have a positive effect on patients with postoperative pain and anxiety.
Objective:
The aim of this systematic review and meta-analysis was to explore the effects of perioperative music therapy on postoperative pain and anxiety based on existing clinical trials.
Methods:
The Cochrane Library, PubMed, and Embase were searched from their inception to August 2022, selected the literature according to the inclusion and exclusion criteria, and completed the meta-analysis using RevMan 5.3.
Results:
A total of 19 eligible randomized controlled trials were enrolled, including 1803 patients. The results of the meta-analysis showed that the scores of pain (standardized mean difference [SMD], −0.90; 95% confidence interval [CI], −1.26 to −0.53; p < 0.00001) and anxiety (SMD, −0.75; 95% CI, −1.19 to −0.31; p = 0.0008) decreased in the music group on postoperative day 1. The blood pressure (mean difference [MD], −5.29; 95% CI, −9.53 to −1.06; p = 0.01) and heart rate (MD, −6.13; 95% CI, −11.69 to −0.58; p = 0.03) also decreased on the same day. Further, the score of change in pain (SMD, 0.35; 95% CI, 0.01 to 0.68; p = 0.04) and anxiety (SMD, 1.35; 95% CI, 0.01 to 2.69; p = 0.05) increased between preoperative and postoperative days in the music group. However, the scores of hospital satisfaction (MD, −0.07; 95% CI, −1.40 to 1.27; p = 0.92) and incidences of postoperative nausea and vomiting (risk ratio, 0.41; 95% CI, 0.13 to 1.34; p = 0.14) did not decrease in the music group.
Conclusion:
Perioperative music therapy can significantly reduce postoperative pain and anxiety and avoid fluctuations in blood pressure and heart rate but does not improve patient hospital satisfaction or incidences of postoperative nausea and vomiting.
Introduction
In recent years, with increasing incidence of various diseases and progress in technology for early diagnosis, related surgical treatments have increased significantly. In a closed operating room environment without the support of family members, patients worry about the success of surgery and surgical incision pain, which makes them feel anxious. 1 –3 To date, many studies have shown that postoperative pain and anxiety can increase the incidence of postoperative complications, such as prolonged mechanical ventilation, hemodynamic disorders, increased dosage of analgesics, delayed recovery of behavioral motor function, and reduced patient satisfaction in hospitals.
In recent years, with the continuous development of enhanced recovery after surgery, surgery, anesthesia, nursing, and other disciplines have attached great importance to reducing the perioperative stress response and postoperative complications, shortening the length of hospital stay, and promoting patient recovery. Therefore, the optimization of perioperative pain and anxiety treatment is particularly important.
The advantages of music therapy in improving perioperative pain and anxiety have been demonstrated in various surgical procedures and patients undergoing them. Many studies have shown that perioperative music therapy can significantly reduce postoperative pain, anxiety, postoperative analgesic drug use, shorten the length of hospital stay, and improve hospital satisfaction. 4 –6
In recent years, many clinical studies have evaluated the effects of perioperative music therapy on postoperative pain and anxiety. However, due to the differences and limitations of the study endpoints, observation indices, and sample sizes, the results were also different. In this study, a meta-analysis was conducted to evaluate whether perioperative music therapy affected postoperative pain and anxiety among patients to provide a reference for the popularization of perioperative music therapy.
Methods
Search strategy
The Cochrane Library, PubMed, and Embase were searched from their inception to August 2022 and investigated the accessibility of online citations of the literature. The keywords used in the search were: perioperative, music, therapy, treatment, postoperative pain, and postoperative anxiety.
Inclusion criteria
Participants
Patients undergoing elective surgery who received perioperative music therapy, had no limitations on age and sex, and had no previous reports of depression, brain, organic, and physical diseases associated with mental disorders, or serious damage to the heart, liver, and kidney were selected for the meta-analysis.
Intervention and controls
The interventions included were music therapy alone or music therapy combined with other therapies. The control group did not receive any music therapy or drug treatment.
Outcomes
The primary outcomes were pain and anxiety scores on postoperative day 1, and the secondary outcomes were blood pressure and heart rate on postoperative day 1, change in pain and anxiety, hospital satisfaction, and incidence of postoperative nausea and vomiting.
Types of studies
Only randomized controlled trials of perioperative music therapy for the improvement of postoperative pain and anxiety were considered eligible.
Exclusion criteria
The exclusion criteria were as follows: (1) non-randomized trials, (2) studies that did not use music as the major treatment, (3) reviews and case reports, and (4) animal experiments.
Data extraction
Three evaluators independently read the literature, selected it according to the inclusion and exclusion criteria, and re-read the full text of the articles that met the criteria for re-selection. If there was any disagreement between the three parties in the discussion, it was further referred to a fourth party 7 for their opinion. Basic data that were extracted included the following: first author of the literature, age and number of participants, year of publication, intervention and control measures, pain and anxiety scores, blood pressure and heart rate, changes in pain and anxiety scores, hospital satisfaction scores, and incidence of postoperative nausea and vomiting (PONV).
Risk of bias assessment of included studies
The quality of the included studies was independently evaluated by the two reviewers according to the risk of bias assessment recommended by the Cochrane Evaluation Manual. 7 The assessment comprised the following seven domains: adequate sequence generation, blinding of outcome assessment, allocation concealment, blinding of participants and personnel, selective reporting, incomplete outcome data, and other biases. Each question was rated as yes (+), low risk of bias, or unclear (?) risk of bias; no (−), high risk of bias.
Statistical analysis
The analysis was conducted using RevMan 5.3. Risk ratio (RR) or odds ratio was used for dichotomous data. Mean difference (MD) or standardized mean difference (SMD) was used for continuous data. We measured heterogeneity using Q statistics and the I 2 index according to the suggestions of the Cochrane Collaboration. I 2 <50% was considered no (I 2 = 0) or low heterogeneity, and the outcome was pooled with a fixed-effect model, otherwise a random-effect model was used.
A meta-analysis was performed to calculate RRs, MDs, SMDs, and 95% confidence intervals (CIs) using the Mantel–Haenszel statistical method. If zero events were reported for one group in comparison, a value of 0.5 was added to both groups for each study. In addition, a subgroup analysis based on different music therapy periods was performed. Sensitivity analyses were performed, as required. The reporting and publication biases of the included studies were assessed by visually inspecting funnel plot asymmetry (Supplementary Table S1).
Results
Study selection
In total, 108 articles were selected, including 81 from PubMed, 12 from the Cochrane Library, and 15 from Embase. After reading the title, abstract, and full text, 19 randomized controlled trials were included, all of which were published in English. The 19 articles included 1803 patients, including 865 in the music therapy group and 938 in the control group. A flowchart of the included and excluded studies is shown in Figure 1.
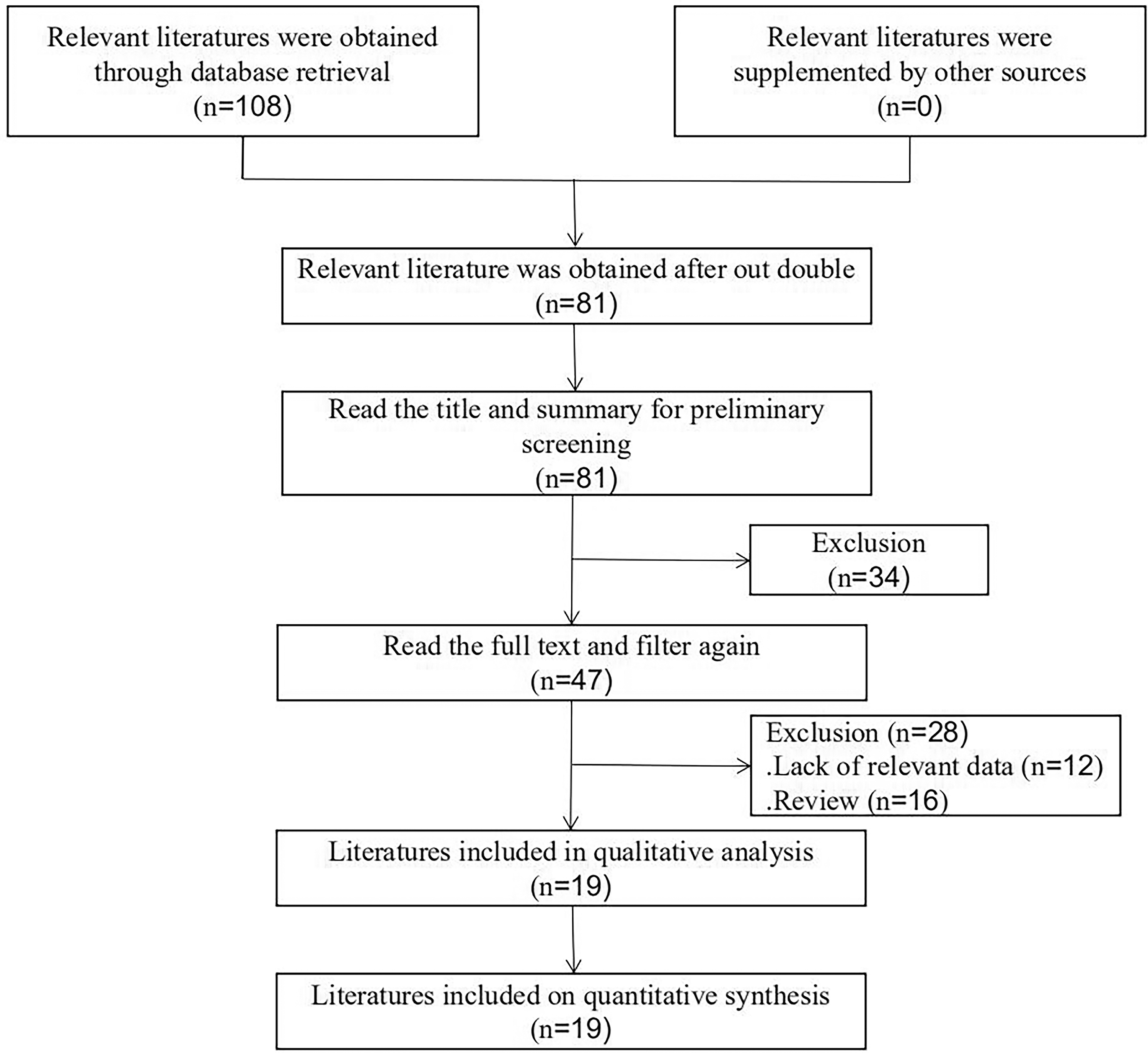
Flow chart of included and excluded studies.
Characteristics and risk of bias assessment of included studies
General information, sample sizes, interventions, and outcome indicators of the included studies are shown in Table 1. The risk of bias assessment of the included studies is shown in Figure 2. The publication bias of the included studies is shown in Supplementary Figure S3.
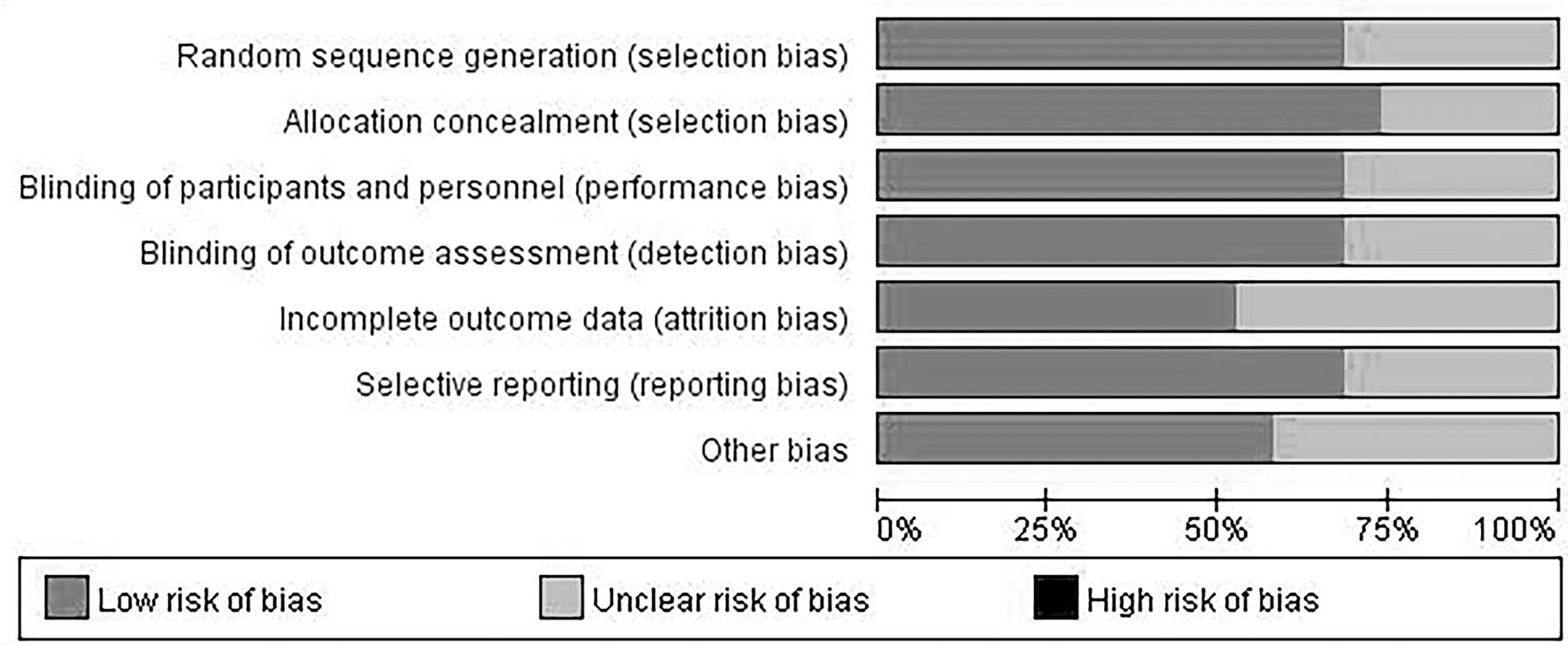
Risk of bias assessment of included studies.
Characteristics of Included Studies
GAD-7, generalized anxiexy disorder-7; HADS, hospital anxiety and depression scale; HAMD, hamilton's depression scale; LLETZ, large loop excision of transformation zone; MVR, mitral valve replacement; NRS, numerical rating scale; OR, operating room; STAI, state-trait anxiety inventory; TLH, total laparoscopic hysterectomy; TOP, termination of pregnancy; VAS, visual analogue scales.
Results of meta-analysis
Pain and anxiety score at postoperative day 1
The pain score on postoperative day 1, based on 15 studies 8,10 –14,17 –21,23 –26 showed that the pain score in the music therapy group was lower than that in the control group (Fig. 3), with a statistically significant difference (SMD, −0.90; 95% CI, −1.26 to −0.53; p < 0.00001).

Meta-analysis of pain score on postoperative day 1-revision. CI, confidence interval; IV, inverse variance; SD, standard deviation.
The subgroup analysis showed that the pain score of the music therapy group was lower, with a statistically significant difference (intraoperative: SMD, −0.80; 95% CI, −1.31 to −0.29; p = 0.002; postoperative: SMD, −1.26; 95% CI, −2.23 to −0.30; p = 0.01; preoperative and postoperative: SMD, −0.86; 95% CI, −1.19 to −0.53; p < 0.00001). But there was no statistically significant difference in postoperative pain score between the two groups receiving preoperative music therapy based on the subgroup analysis (SMD, −0.71; 95% CI, −1.47 to 0.05; p = 0.07).
The results of the anxiety score on postoperative day 1, based on six studies 8,9,13,21,23,24 showed that the music therapy group had lower scores than the control group (Fig. 4), with a statistically significant difference (SMD, −0.75; 95% CI, −1.19 to −0.31; p = 0.0008). The subgroup analysis results showed that anxiety scores in the music therapy group were lower, with a statistically significant difference (preoperative: SMD, −0.91; 95% CI, −1.74 to −0.08; p = 0.03; intraoperative: SMD, −0.75; 95% CI, −1.38 to −0.11; p = 0.02).

Meta-analysis of anxiety score on postoperative day 1.
However, there was no statistically significant difference in postoperative anxiety score between the two groups receiving postoperative music therapy based on the subgroup analysis (SMD, −0.63; 95% CI, −1.53 to 0.26; p = 0.16).
These results indicated that perioperative music therapy can significantly reduce postoperative pain and anxiety.
Blood pressure and heart rate on postoperative day 1
The results of blood pressure on postoperative day 1, based on five studies, 8,9,20,22,24 showed that the music therapy group had lower blood pressure (Fig. 5), with a statistically significant difference (MD, −5.29; 95% CI, −9.53 to −1.06; p = 0.01). The results of heart rate on postoperative day 1, based on six studies, 8,9,18,20,22,24 showed that the music therapy group had lower values than that in the control group (Fig. 6, with a statistically significant difference (MD, −6.13; 95% CI, −11.69 to −0.58; p = 0.03).

Meta-analysis of blood pressure on postoperative day 1.
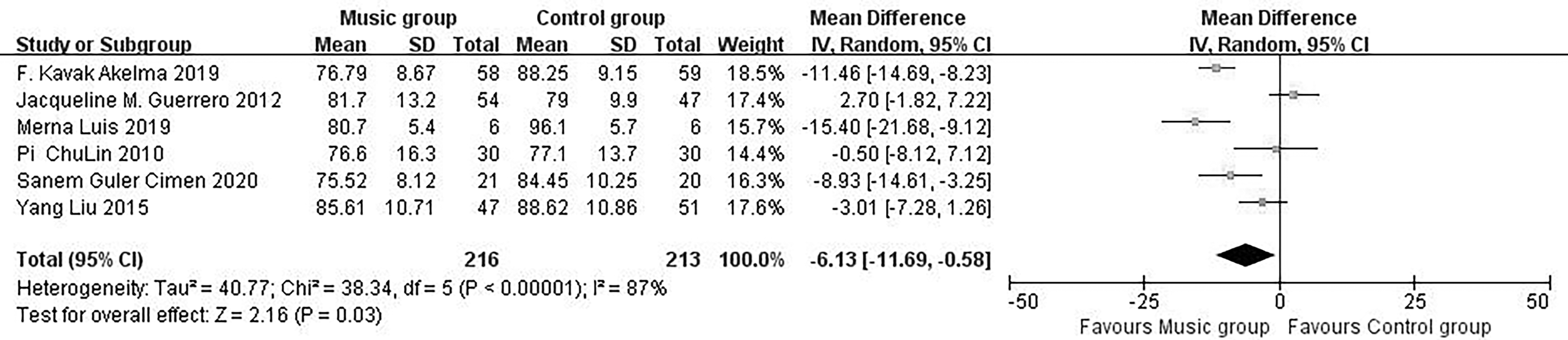
Meta-analysis of heart rate on postoperative day 1.
Therefore, perioperative music therapy can significantly avoid fluctuations in blood pressure and heart rate.
Change in score of pain and anxiety
The change in pain and anxiety scores in the music therapy group was higher than that in the control group, based on two studies 11,22 on pain and five studies 8,11,13,15,22 on anxiety. The difference of change in pain score was statistically significant (SMD, 0.35; 95% CI, 0.01 to 0.68; p = 0.04), as shown in Figure 7. In addition, the difference of change in anxiety score was also statistically significant (SMD, 1.35; 95% CI, 0.01 to 2.69; p = 0.05) in Figure 8.

Meta-analysis of change in score of pain.
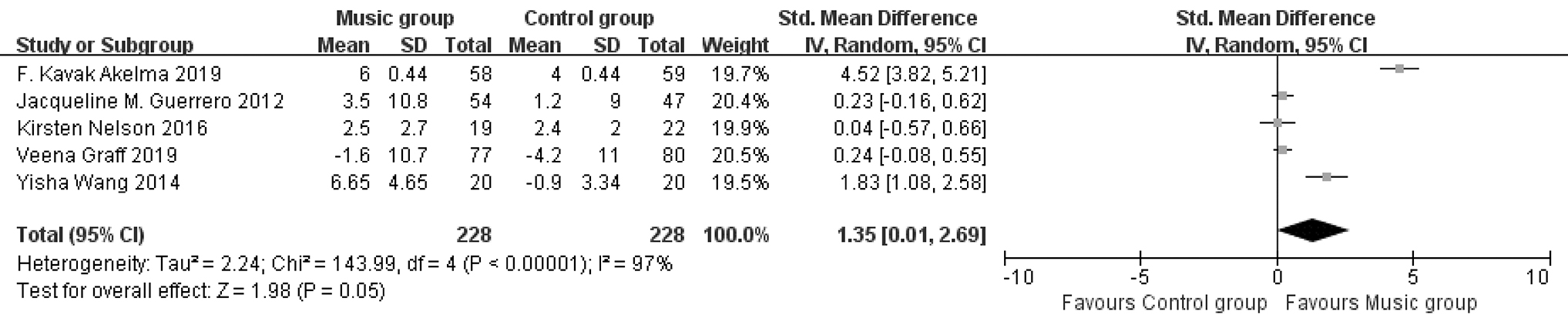
Meta-analysis of change in score of anxiety.
Hospital satisfaction score and incidence of postoperative nausea and vomiting
A total of three studies, 8,15,19 included the hospital satisfaction scores. However, the difference of the change in hospital satisfaction score was not statistically significant (MD, −0.07; 95% CI, −1.40 to 1.27; p = 0.92), as shown in Supplementary Figure S1. Incidence of PONV was reported by two studies. 16,25 Moreover, the difference was not statistically significant (RR, 0.41; 95% CI, 0.13 to 1.34; p = 0.14) in Supplementary Figure S2.
Publication bias analysis
The funnel plot of the pain scores on postoperative day 1 in the included studies was symmetrical, resulting in a small publication bias (Supplementary Fig. S3).
Incidence of adverse events
A study observed four cases of intraoperative awareness in the music therapy group and nine cases in the control group. 12 Another study found two cases of pruritus in the control group and none in the music therapy group. 16 No serious adverse events were observed in any of the studies. Therefore, music therapy is safe and effective.
Discussion
Treatment of postoperative pain and anxiety is an important aspect of perioperative management. Studies have shown that postoperative anxiety increases the occurrence of postoperative pain and vice versa, both of which affect the postoperative recovery of patients, increase the amount of postoperative analgesic use, prolong the length of hospital stay, and reduce patient satisfaction. 8,11,14
Perioperative pain and anxiety management is mainly achieved by drug therapy, but this has certain side effects, such as gastrointestinal side effects and a gradual increase in the dose of treatment and increasing the burden of patients' medical expenses. Therefore, an increasing number of non-drug treatment methods are being adopted gradually. 10,15
Recently, the clinical application of perioperative music therapy has gradually increased. Music therapy can improve postoperative anxiety, relieve postoperative incision pain, maintain postoperative hemodynamic stability, reduce postoperative complications, and shorten hospital stays. Therefore, various forms of perioperative music therapy are administered, 27 –31 such as listening to their favorite music using headphones or receiving soft and relieving music.
Pain is an unpleasant feeling and emotional experience belonging to a type of stressor that can affect the recovery of local or systemic functions in patients and even endanger their lives. 16,17 It is more common in patients undergoing surgery. Pain stimulates the sympathetic-adrenal medullary system, leading to increased secretion of catecholamines in the body, resulting in increased blood pressure, heart rate, and affect mood and appetite. 18,20
Therefore, it prolongs the postoperative recovery time of patients, increases postoperative hemodynamic fluctuations and the incidence of postoperative complications, and affects postoperative recovery and overall prognosis. 19,21 Continuous pain makes patients susceptible to anxiety, tension, and other negative emotions. Pain-related receptors, such as endogenous opioids, γ-aminobutyric acid, and dopamine, are distributed in the ventral striatum, dorsal medial midbrain, amygdala, and hippocampus.
These neuronal mediators play important roles in the occurrence and development of pain. 32 Music therapy modulates the neurotransmitter activity in these areas, thereby affecting pain occurrence. Many studies have shown that music therapy can improve postoperative acute and chronic pain and reduce opioid use in patients undergoing colon, burn, and cardiac surgery.
The results of this study showed that the pain score of the music treatment group was lower than that of the control group on the first postoperative day, and the pain score of the music treatment group changed significantly, which was consistent with other studies. 8,12,26
These results suggest that perioperative music therapy can regulate the release of neurotransmitters in the cerebral cortex, thereby improving the release of catecholamines by the sympathetic adrenergic medullary system stimulated by these stressors, reducing postoperative pain and the use of postoperative opioids.
Anxiety is a pathological state of continuous tension and fear accompanied by vegetative neural activity dysfunction. It is a type of stressor that can continue to affect patients' emotions and behaviors and increase patients' abnormal sensitivity to pain. 16,17 Anxiety can excite the sympathetic nervous system and stimulate the body to secrete catecholamines, resulting in adverse complications.
Music therapy stimulates the cerebral cortex, reduces the secretion of hormones related to stress and anxiety, and improves negative emotions in patients through the neuroendocrine pathways. 21 At the same time, it can directly stimulate the brain stem reticular nervous system structure, increase parasympathetic nervous activity, and reduce the body's physiological response to tension, fear, and other negative emotions. 22
Studies have shown that perioperative music therapy can relax patients, reduce, or divert attention to negative stimuli, such as surgery and pain, and make patients feel happy. The results of this study showed that the postoperative anxiety score of the music treatment group was significantly improved and was lower than that of the control group, consistent with previous studies. 9,13,24
These results suggest that perioperative music therapy may inhibit the excitation of the sympathetic nervous system and relieve postoperative anxiety from the neuroendocrine and brainstem reticular systems, thus reducing sensitivity to pain and the incidence of postoperative acute pain.
Continuous pain and anxiety stimulate the sympathetic nervous system of the body to produce adrenaline, norepinephrine, dopamine, and other substances, causing increased blood pressure, accelerated heart rate, and increased incidence of postoperative incision bleeding. Postoperative hemodynamic fluctuations, 20,22,24 surgical incision bleeding, and other related complications delay the recovery of postoperative functional behavior, prolong the length of hospital stay, and increase medical costs.
The results of this meta-analysis showed that the blood pressure and heart rate of the music therapy group did not significantly increase on the first postoperative day compared with those of the control group, and the hemodynamics were relatively stable, which was consistent with other studies. 8,18,24
However, this study found that perioperative music therapy did not improve patient satisfaction in hospitals or reduce the incidence of postoperative nausea and vomiting. Considering that satisfaction with the hospital and postoperative nausea and vomiting complications of patients were affected by multiple factors, a few studies were included in the two study indexes, which lacked a sufficient sample size for evaluation.
This study had some limitations. The heterogeneity of the included literature was large, and gray literature was not searched or screened. Therefore, a large number of multicenter randomized controlled trials with large sample sizes and rigorous designs are needed to provide a stronger scientific basis for clinical practice.
Conclusion
Perioperative music therapy can significantly improve patients' postoperative pain and anxiety, avoid complications, such as postoperative hemodynamic fluctuations, shorten the length of hospital stay, and reduce medical costs; however, it does not improve patients' satisfaction in the hospital and the incidence of postoperative nausea and vomiting.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank all the participants involved in this study.
Authors' Contributions
G.L. planned and designed the study. L.Y., Y.Y., and J.D. screened the potential studies and extracted data from the included studies. G.L., L.Y., and L.S. assessed the manuscript. C.Z. provided guidance on the overview methodology, and G.L. drafted the manuscript. All authors read, critically reviewed, and approved the final manuscript.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This study did not receive any specific grants from funding agencies in the public, commercial, or non-profit sectors.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.