
Abstract
Objectives:
The aim of this study was to investigate whether a combination of nutrients designed to promote gut and brain health also lowers psychological distress. The hypothesis is that a probiotic with fish oil, and glutamine supplement will reduce psychological distress.
Design:
A multiple baseline design was used to collect data from seven naturopathic patients in private naturopathic clinics in Australia. Patients were between 18 and 65 years of age, and had a Kessler-10 (K10) score between 16 and 30 and symptoms associated with mild gastrointestinal discomfort experienced several times most weeks for 3 months. They were randomized into one of three pathways to stagger the introduction of the intervention.
Interventions:
Participants received either a supplement incorporating a probiotic formulation (including Lactobacillus rhamnosus), a glutamine powder formulation, and fish oil, or matched placebos. The primary outcome measure was psychological distress as measured by the K10 scale of psychological distress.
Results:
The data showed a general trend toward lower K10 scores during the active phase compared with the baseline phase, with a marked reduction in the variances between phases. After controlling for time and baseline values, no significant difference between the phases for the K10 and the Perceived Stress Scale was found, but there was still a significant reduction in symptoms on the Gastrointestinal Symptom Rating Scale.
Conclusions:
A combination of a probiotic formulation, a glutamine powder formulation, and fish oil did not affect psychological distress and perceived stress, but had a significant beneficial effect on gastrointestinal symptoms in patients with high distress and concurrent gut symptomology.
Clinical trial registration number:
ACTRN12620000928910.
Introduction
About one in five Australians experience a mental disorder each year. 1 Mental health disorders can substantially impact individual well-being and operational capability. For example, psychological distress can have a significant impact on the capacity of those affected to perform adequately at work and contributes to absenteeism. 2 Recent discoveries that bacteria in the human intestinal tract can influence stress pathways opens new frontiers for interventions in mental health. 3 –5 An expanding branch of this research is providing evidence that supports the link between the microbial state of our gut and our emotional functioning, particularly in relation to stress, anxiety, and depression. 6
It is now widely accepted that psychosocial stress induces an inflammatory physiological state. 7 Signaling molecules in the immune system called cytokines provide a bidirectional link between body and brain. Cytokines are secreted from cells during stress and link both cognitive stress (emotional or physical) and noncognitive stress (infection or inflammation) with the same neuroendocrine response—activation of the hypothalamic-pituitary-adrenal (HPA) axis. 8 HPA axis homeostasis is an important mechanism for psychological resilience and healthy responses to stress, 9 while dysregulation increases susceptibility to chronic inflammatory diseases and mental health disorders such as depression. 10
HPA axis overactivation may be caused by prolonged, repetitive or traumatic exposure to stress 11 and this response may be mediated and moderated, to some degree, by cytokines signaling the HPA axis. 12 Proinflammatory cytokines exaggerate the stress response, while anti-inflammatory cytokines help to regulate it and promote psychological and physical resilience. 13 Therefore, interventions that target proinflammatory cytokines have the potential to support stress feedback mechanisms.
The recent discovery of the gut microbiome opens up new avenues of inquiry for stress-related disorders. 14 –16 New studies have found that an imbalance of gut microorganisms is associated with a range of modern lifestyle diseases, such as allergies, obesity, and mental health disorders. 17,18 Common digestive symptoms associated with altered balance in the microbiota include changes in gas production, characteristically experienced in irritable bowel syndrome (IBS). 19 The microbiota can also be influenced by diet, particularly probiotics (foods that contain living microorganisms). 20 A number of animal studies suggest that these microbes act as signaling components of the gut-brain axis. 21 One study investigating the effect of a 4-week probiotic food supplement on 20 healthy adults concluded that the intake of probiotics may help reduce negative thoughts associated with sad mood. 22 Further investigation of probiotic treatment, particularly treatment with the probiotic species Lactobacillus rhamnosus, for clinically relevant anxiety, is warranted. 23
Whole systems research was proposed almost 20 years ago as an alternative clinical research design to the gold standard randomized controlled trials used in biomedical research. 24 While randomized controlled trials look for a single treatment that can be applied to all patients, whole systems research accommodates complex and multitiered approaches that are individualized for each patient in healthcare, and typically used in complementary medicine. 25 The shift from single-intervention clinical trials to more wholistic multiple intervention trials, such as N-of-1, provides a realistic platform for complementary medicine research. 26 N-of-1 trials have been recognized by the Oxford Centre for Evidence-Based Practice as the highest level of evidence (level 1) for the efficacy of an intervention in an individual, along with systematic reviews of randomized controlled trials. 27
This study employed an N-of-1 trial design to determine whether a combination of a probiotic formulation, fish oil, and glutamine powder formulation can reduce symptoms of psychological distress in individuals with symptoms consistent with a compromised microbiome. There is evidence that fish oil targets complex mechanisms, including gut dysbiosis and inflammation in the brain in stressed rats. 28 Probiotics are effective at reducing gut symptoms such as abdominal pain and diarrhea, potentially by reducing gut permeability, 29 and have been implicated as novel treatments in brain diseases such as Parkinson's disease. 30 Glutamine is an amino acid that has been shown to reduce gut permeability, 31 helping to restore the integrity of the gut in people with leaky gut. It is hypothesized that the combination of these interventions may have an effect on the gut environment and microbiome, which may in turn have an effect on distress in individuals with gut symptoms and distress.
Materials and Methods
Design
A multiple baseline design (MBD), a variant of an N-of-1 series, was used to collect data from patients of naturopaths in their private practices in Australia. The CONSORT extension for reporting N-of-1 trials (CENT) 2015 Statement was used to assure the quality of the study (Supplementary Table S1). MBDs are suitable when the interventions cannot not be rapidly cleared from the body, as is the case in nutritional interventions such as probiotics and fish oil. 32 For instance, when taken in sufficient doses for a sufficient period of time, the essential fatty acids+docosahexaenoic acid (DHA) from fish oil are incorporated into cell membranes, 33 while probiotics are incorporated into the microbiome. 34 Cao et al. 33 demonstrated that at 8 weeks of fish oil supplementation, erythrocyte eicosapentaenoic acid (EPA)+DHA had increased by 300% EPA +42% DHA; therefore, the minimum time period for a phase in this study was set at 8 weeks.
Several dependent variables were measured repeatedly throughout the study, although commencement of the active intervention was staggered across a priori allocated experimental conditions (pathways). Baseline (i.e., placebo control condition) was the first measurement point for all pathways. The time to treatment was randomly allocated for individual patients, as shown in Figure 1.
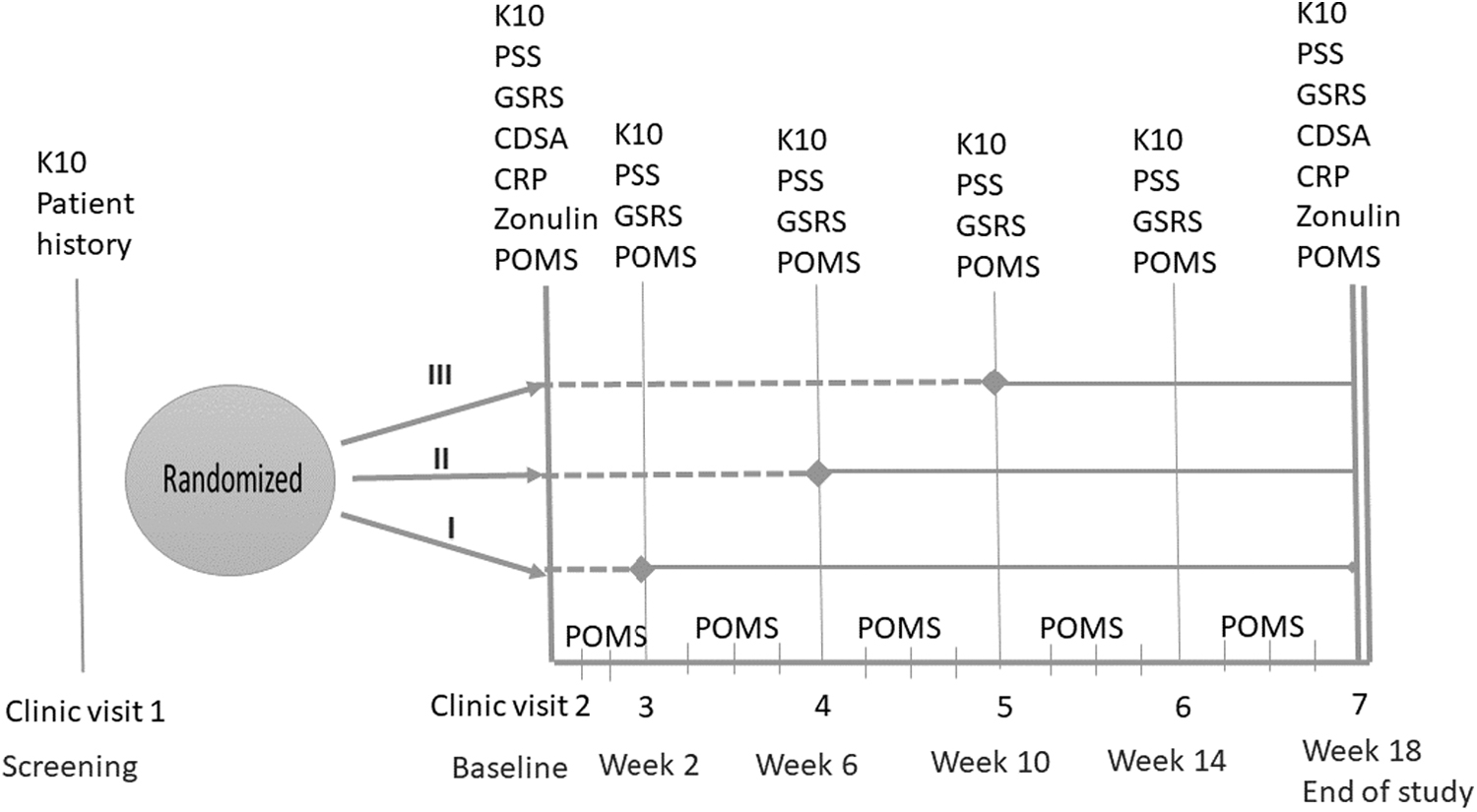
Design of multiple baselines (i.e., three pathways) for individual participants across multiple measurement points (broken line denotes baseline phase; unbroken line denotes active phase).
Trial protocol
Participation in this trial involved two phases where the control phase (A) preceded active phase (B). Participants were randomly allocated to one of three control phase durations of 1, 2, or 3 months. Total trial duration was 18 weeks. Commencement of the control phase (A) occurred from baseline, but commencement of the active phase (B) was sequentially staggered across the different tiers (Fig. 1). As all participants were administered placebo interventions in the control period, no washout was required.
Hypothesis
The primary hypothesis was that psychological distress will be reduced during the active phase compared with the baseline phase.
Participants
This study was conducted with approval of Southern Cross University Human Research Ethics Committee (ECN-18-192). We aimed to recruit up to nine practitioners and nine patients. This was based on the rationale that three participants per pathway would be sufficient to enable data trends (Fig. 1).
Clinical and research data were collected from July 2019 to December 2020 by the naturopathic practitioners who had completed two training sessions. The target patient population were patients 18 to 65 years of age with a psychological distress score between 16 and 30 on the Kessler-10 (K10) scale, with concomitant symptoms associated with mild gastrointestinal discomfort (e.g., excessive wind or abdominal bloating) experienced several times most weeks for 3 months. Exclusion criteria included immunosuppressive medication, Warfarin or other anticoagulant medication, major surgery within the previous 6 months, diagnosed with serious psychiatric conditions, diabetes, poor venous access, body mass index ≥35, unexplained recent weight loss, and pregnancy.
Randomization and blinding
The treatment and placebo interventions were prepared by the sponsoring industry partner (Metagenics [Aust] Pty Ltd.), who conducted the computer-generated randomization, labeled the bottles of supplements using a code and no identifying information, supplied bottles directly to practitioners, and assigned participants to interventions. The random schedule was sent to an academic staff member who was independent of the study and kept it securely until the completion of the study. After enrolment by the trial coordinator, participants were randomly allocated to a 1-, 2-, or 3-month time to treatment (active phase), with a total trial duration of 5 months. The university researchers, practitioners, and patients were blinded to the randomization schedule. Practitioners and patients were additionally blinded to the study design.
Outcome measurements
The primary outcome was psychological distress as measured by the K10 scale of psychological distress. 35
Secondary outcomes included the following: Gastrointestinal Symptom Rating Scale (GSRS), a valid and reliable evaluation of common symptoms of gastrointestinal disorders.
36
It contains 15 items, each rated on a 7-point Likert scale from no discomfort to very severe discomfort.
37
Participants completed the GSRS on six occasions. Perceived Stress Scale-10 (PSS-10),
38
a valid and reliable 10-item self-reported measure of perceived stress.
39,40
Participants completed the PSS-10 on six occasions. The abbreviated Profile of Mood States short form scale
41
used to assess transient distinct mood states over a period of time.
42
In this study, the subscales relating to depression, fatigue, and vitality were used. A total mood disturbance (TMD) score was calculated by summing the total scores from the depression and fatigue subscales and subtracting the total score for vigor. This was administered weekly (24 occasions). Complete digestive stool analysis (CDSA). Participants collected stool samples using NutriPATH CDSA Stool Kit before and after the study. The CDSA tests included four strains of bacterial flora: Lactobacillus species (range: 8.6–6200.0 × 105 colony-forming unit [CFU]/g); Bifidobacterium species (range: >6.7 × 107 CFU/g); Escherichia species (range: 3.7–38,000 × 106 CFU/g); and Enterococcus species (range: 1.9–2000.0 × 105 CFU/g). Also included were the following GIT functional markers: calprotectin (range: 0.0–173 μg/g) as a marker of bowel inflammation, pancreatic elastase (range: >200.0 μg/g), and short chain fatty acids (i.e., buterate) μmol/g. Zonulin is a protein biomarker of impaired gut barrier activity of the tight junctions in the bowel
43
and is used as a biomarker for “leaky gut” syndrome. Fecal zonulin levels were included in the CDSA tests (range: 0.0–107.0 μ/g). C-reactive protein (CRP), a serum inflammatory marker, was collected on two occasions. Pathology tests were conducted at pathology service providers local to the participants. Concomitant and rescue medication usage during the trial was collected at each clinic visit.
Study treatment
Participants consumed the following active supplements or the corresponding placebo (all matched for size, color, weight, and smell) twice daily:
L. rhamnosus (LGG®) (10 × 109 CFU), Saccharomyces cerevisiae (boulardii) (7.5 × 109 CFU), and Bifidobacterium animalis spp. lactis (BB-12®) (5 × 109 CFU) (Metagenics Ultra Flora Intensive Care ARTG ID 286746).
Aloe vera 3.25 mg/g (equiv. fresh herb 649.35 mg/g); Boswellia serrata 19.48 mg/g (equiv. fresh herb 194.8 mg/g); cholecalciferol 1.6233 mcg/g; glutamine 285.71 mg/g; Larix arabinogalactan 259.74 mg/g; Rretinol palmitate 178.57 mcg/g; and zinc amino acid chelate 9.74 mg/g (Metagenics Glutagenics ARTG ID 349170).
Concentrated fish omega-3 triglycerides 952.38 mg/mL (Metagenics Metapure EPA/DHA Liquid ARTG ID 227557).
Statistical analysis
Individual level data were explored by visual graphs of the outcome measures by phase, as recommended by the CONSORT collaboration extension for N-of-1 studies. 44 This was augmented by an exploratory modeling approach, combining data across all participants. A linear mixed random effects modeling approach was used to take account of the longitudinal nature of the data. Parameters were estimated using a simple random intercepts model with a restricted maximum likelihood estimator assuming an exchangeable marginal error covariance structure. Individual participants were the clustering variabe (random effects). In the adjusted model, the estimates are adjusted for the effects of time and for the baseline values for the outcome. Inclusion of time controls for the effects of regression to the mean, and baseline value controls for the individual variation due to small sample size. Data analysis was conducted using Stata 16. 45
Safety monitoring
Before the trial commenced, a Safety Monitoring Group, comprising a registered medical practitioner and a registered psychiatric nurse, was established and each participant had a full clinical assessment provided by the practitioner, who discussed any abnormal result in general physical health with the patients and referred them to their medical practitioner if required. The practitioner also notified the Chief Investigator who discussed the concern with the Safety Monitoring Group and acted on their advice. Continued good health was monitored at each clinic visit. Each participant was supplied with a wallet card that detailed their participation in a clinical trial.
At follow-up visits, patients were carefully assessed for adverse events (i.e., any new complaint or symptom, or any pre-existing symptom that increased in frequency and/or intensity during the trial). Fortnightly contact with the trial coordinator provided another opportunity for participants to volunteer adverse events and report any issue associated with the trial.
Trial registration
The trial was registered with the Australian Clinical Trials Register (ACTRN12620000928910).
Results
Seven naturopathic practitioners were recruited into the study. Two withdrew as they were unable to recruit patients who met the study criteria. Eight patients, recruited May to June 2019, were randomized into the trial. One patient withdrew during the trial due to increased abdominal symptoms during the first week of the study (Fig. 2). No other adverse event was reported. Five naturopathic practitioners and seven patients completed the trial.
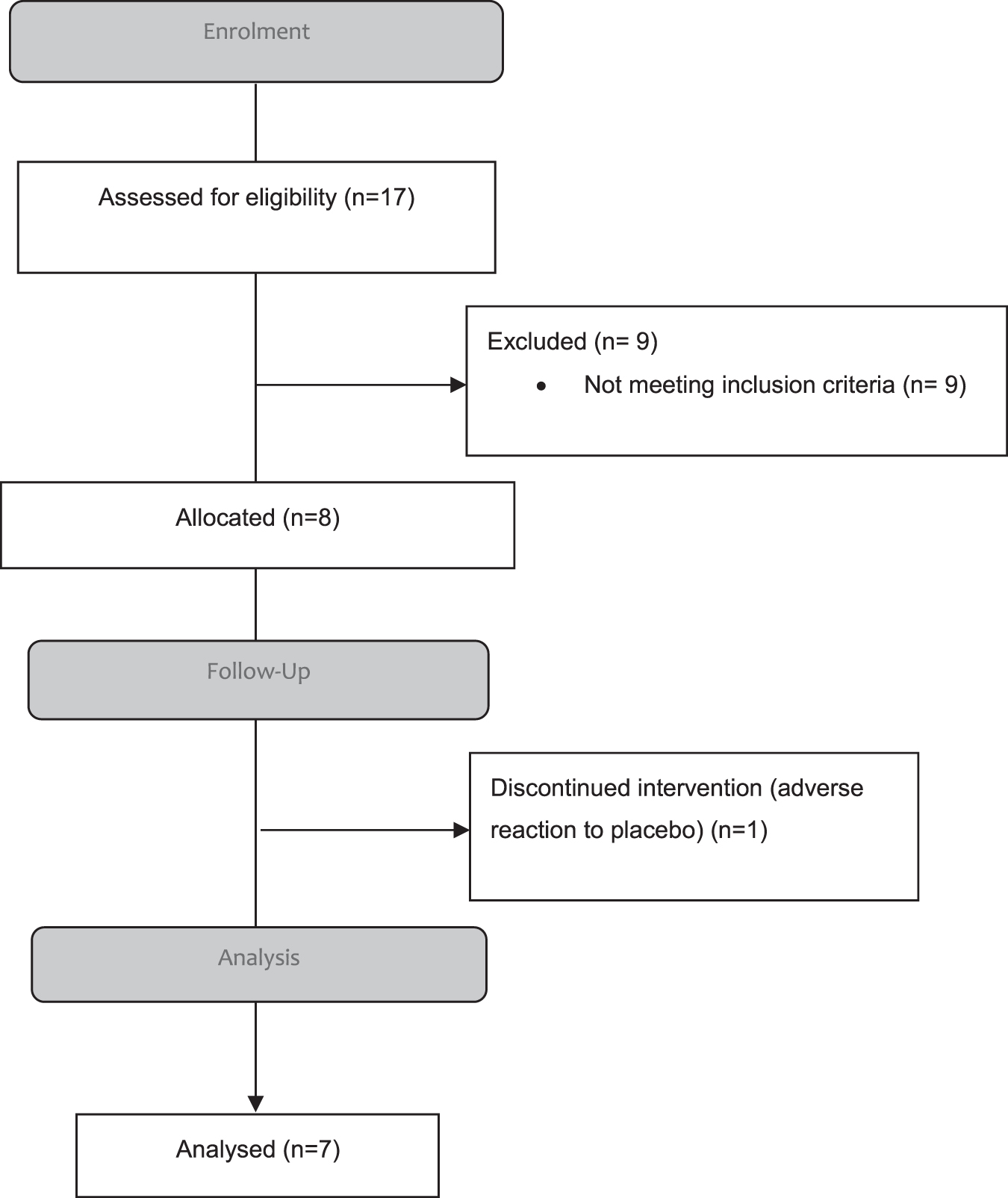
Participant flow.
Sample characteristics
The ages of participants ranged from 32 to 61 years, with a mean of 45.5 years. Six participants were female and one was male. Other participant characteristics are provided in Table 1. Figure 2 shows the flow of participants through the study.
Participant Characteristics at Baseline
BMI, body mass index; SD, standard deviation.
The individual plots show the patterns of change over time in the raw data for the psychological distress (K10) scores through the multiple baseline study (Fig. 3).

Individual plots of K10 scores over time through three concurrent baselines/pathways. Pathways I and III each had n = 21 observation points; pathway II had n = 7 observation points. K10, Kessler-10.
There was a general trend toward lower mean K10 scores during the active phase compared with the baseline phase, with a marked reduction in the variances between phases (Table 2). In the unadjusted analysis, there were reductions in scores on the K10, PSS, GSRS, and TMD from baseline to the active phase (Table 2).
Unadjusted Treatment Effects
Using a random effects model to take account of clustered data (i.e., multiple observations from participants).
CI, confidence interval; GSRS, Gastrointestinal Symptom Rating Scale; K10, Kessler-10; PSS-10, Perceived Stress Scale-10; SD, standard deviation; TMD, total mood disturbance.
After adjusting for time and baseline values, the estimate remained significant in the GSRS and there were trends toward significance in stress and distress (Table 3).
Treatment Effects After Adjustment for Time and Baseline Values
Significant at the p = 0.01 level.
Using a random effects model to account for clustered data.
CI, confidence interval; GSRS, Gastrointestinal Symptom Rating Scale; K10, Kessler-10; PSS-10, Perceived Stress Scale-10; TMD, total mood disturbance.
The mean trajectories for each phase are plotted in Figure 4. For the K10, there was a steep reduction through baseline that tended to plateau during the active phase. The PSS shows similar reductions through both phases. The GSRS shows lower level of symptoms during the active treatment phase compared with baseline.

Predicted changes over time for K10 (top left), PSS (top right), GSRS (bottom left), and TMD (bottom right). Grid lines at the means: dashed for baseline; solid for active intervention phase. GSRS, Gastrointestinal Symptom Rating Scale; K10, Kessler-10; PSS-10, Perceived Stress Scale-10; TMD, total mood disturbance.
Biomarkers
The four strains of bacterial flora (Table 4) demonstrated extreme variability. There was a significant increase in Lactobacillus spp. at the completion of the study compared with baseline. Bifidobacterium spp. was reduced. The descriptive statistics for the CDSA tests and serum CRP at both time points (before and after the trial) is provided in Table 4.
Descriptive Statistics for Complete Digestive Stool Analysis Tests
Lactobacillus species (range: 8.6–6200.0 × 105 CFU/g); Bifidobacterium species (range: >6.7 × 107 CFU/g); Escherichia species (range: 3.7–38,000 × 106 CFU/g); Enterococcus species (range: 1.9–2000.0 × 105 CFU/g); Bacteroides fragilis (range: 1.6–250 × 109 CFU); calprotectin (range: 0.0–173 μg/g); pancreatic elastase (range: >200.0 μg/g); SCFAs (i.e., butyrate) μmol/g; fecal zonulin (range: 0.0–107.0 μg/g); fecal secretory IgA (range: 510.00–2010.0 μg/g); serum CRP (range: 0.3–10 mg/L); Bacteroidetes (range: 8.61–33.10 × 1011 org/g); Firmicutes (range: 5.70–30.40 × 1010 org/g). SCFAs were not available at baseline due to a problem at the outsourced laboratory and are denoted as missing (—).
CFU, colony-forming unit; CRP, C-reactive protein; SCFA, short chain fatty acid; SD, standard deviation.
Discussion
Significance for treatment of patients with gut and stress-related disorders
This study set out to investigate whether a combination of nutrients designed to promote a healthy gut and brain could lower psychological distress and improve gut outcomes. There were significant reductions from baseline in all four outcome measures (K10 scale of psychological distress, perceived stress [PSS], gastrointestinal symptoms [GSRS], and TMD) in the unadjusted analysis. However, when modeling adjusted for the effects of time and baseline values of the outcome, there were no longer significant reductions in psychological distress or perceived stress, but there were for gastrointestinal symptoms. It is likely that the inclusion of L. rhamnosus in the intervention contributed to this outcome. An extensive systematic review of probiotics in IBS found that the efficacy of different probiotics has been investigated for the most common IBS outcome (change in abdominal pain scores). L. rhamnosus GG was one of only four strains found to significantly reduce these scores. 46
The adjusted scores account for the well-known regression to the mean phenomenon. This describes the natural tendency of follow-up scores to fall closer to the mean than the initial or baseline scores. 47 This can be largely controlled for statistically by including a variable that represents time as a covariate and also by including the baseline values of the outcome as another covariate in the model, as was the case in this study. 48,49
After controlling for potential regression to the mean, the mean scores in the active phase remained significantly lower on the GSRS compared to baseline for gastrointestinal symptoms. This treatment effect for gastrointestinal symptoms for the intervention supports the hypothesis that the intervention helps to improve the gut. However, the hypotheses that the intervention would also reduce psychological distress and perceived stress were not supported in this study.
Biomarkers: exploring mechanisms
To understand the effect of a nutrient intervention on the intestinal microbiome, the whole microbiota homeostasis needs to be taken into account. CDSA stool testing provides a snapshot of the whole microbiome ecosystem and is useful in understanding the effects of probiotics and other targeted treatment(s). Microbiome testing generally assesses for beneficial bacteria, opportunistic bacteria, pathogenic bacteria, parasites, and gastrointestinal epithelial markers. If a parasitic invasion is present in the microbiome, it is likely that the Bifidobacterium and Bacteroides species will be low or reduced, as reflected in our trial (participants 7 and 12). These beneficial bacteria are responsible for inhibition of mucosal adhesion and invasion of pathogens. 50
The proportion of participants with a beneficial Fimicutes/Bacteroidetes ratio was increased through the trial, indicating a reduction in intestinal dysbiosis. 49 Fecal samples of healthy adults taking an almost comparable daily dose of L. rhamnosus (10 billion CFU/day) and a second Bifidobacterium species (Bifidobacterium longum) for 30 days revealed a significantly reduced population of Firmicutes and the ratio of Firmicutes/Bacteroidetes indicated a more benign microbiome. These changes were even more significant in a follow-up assessment a month later. 51 Omega-3 fatty acids have also been associated with beneficial changes to the intestinal health, including increasing the population of Bacteroidetes. 52
Implications for whole-systems research
The study demonstrates the usefulness of multiple baseline trials for the kind of complex treatment approaches that are commonly used in complementary medicine. 25,26 MBD trials are particularly useful for determining functional relations when an independent variable is unable to be removed between phases 53 —in this case, the effect of the probiotics, glutamine powder formulation, and fish oil supplement. The study generated high-level evidence for the effectiveness of a supplement of probiotic formulation, glutamine powder formulation, and fish oil for individual participants who were patients of naturopaths in clinical practice. This evidence was subsequently used to inform ongoing treatment protocols for individual participants.
Limitations
In MBD studies, all participants begin with the placebo and commencement of the intervention is randomized. Future studies should collect data weekly to increase the number of measurement observations. It may also be that the stress and distress measures required longer exposure to the active intervention than were offered in this trial.
This MBD was not powered to demonstrate statistical significance using linear mixed modeling. Larger numbers of participants or observations are required to demonstrate conclusivity. A major issue is the hypothesis testing was underpowered. However, there were sufficient data to allow exploratory modeling for data trends. Collectively, the graphs and modeling propose that there were consistent trends over multiple outcomes, suggesting that the active phases may be associated with lower mental health scores. Further studies with larger samples are warranted.
Conclusions
This novel intervention of a probiotic formulation, a glutamine powder formulation, and fish oil demonstrated data trends toward reduction of psychological distress and perceived stress. There was a significant beneficial effect on gastrointestinal symptoms in patients with high distress and concurrent gut symptomology. Further research with more observations and longer active phases are required to conclusively determine whether there could also be a significant treatment effect for this nutritional intervention in mental health.
Footnotes
Acknowledgments
We would like to thank Dr. Richard Lakeman for his online education session on mental health for our practitioners. We also thank Drs. Richard Lakeman and Rosemary Craig who were available to monitor data collection, and Dr. Jacinta Arellano who maintained the blinding code until all analysis was completed.
Authors' Contributions
S.G.—conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, and writing—original draft and review and editing.
J.B.—conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, and writing—original draft and review and editing.
C.A.—conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, and writing—original draft and review and editing.
L.T.—formal analysis, investigation, and writing—original draft.
S.M.-B.—–investigation and writing—review and editing.
Author Disclosure Statement
The first author is a member of the Board of the Australian Traditional Medicine Society. The Society had no involvement in the conceptualization, conduct, or reporting of the study. All other authors have no conflicts of interest to report.
Funding Information
This work was supported by the Australian-Traditional Medicine Society [Project No. 51704] and the supplements were provided by Metagenics Australia. The supporters had no role in the study design, data collection, and analysis and interpretation of data, in the writing of the article, or in decision to submit the article for publication.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.