
Abstract
Introduction:
The first signs of deteriorated balance impairment begin during middle age. Early intervention could delay the fall risk in older populations; hence, addressing balance deficits during this age is crucial. The authors aimed to determine the effects of transcranial direct current stimulation (tDCS) combined with balance training (BT) on the improvement of static and dynamic balance in a middle-aged population, along with the participants' safety and satisfaction.
Methods:
Participants (n = 28) were randomized into two groups: active tDCS (active tDCS + BT) and sham tDCS (sham tDCS + BT). Both groups received the intervention thrice a week for 6 weeks. Dynamic and static balance were assessed by sway rate changes with eyes open and closed, and the functional reach test and a postintervention survey were conducted to assess participants' safety and satisfaction.
Results:
The active tDCS group showed significantly greater static and dynamic balance improvements in sway scores. The surveys demonstrated the safety of the program and satisfaction of 80% of the participants with the combined intervention.
Conclusion:
tDCS could be used in a middle-aged population as part of regular BT to improve balance and minimize the risk of balance deficits in older populations while ensuring patient safety and satisfaction. This study is a subanalysis of a larger clinical trial that included young adults as well (Clinical trial number: KCT0007414).
Introduction
Balance is defined as the ability to maintain the body's center of gravity within the base of support with minimal postural sway. 1 Co-activation of multiple regions of the central nervous system, such as the cerebellum, primary motor cortex (M1), dorsolateral prefrontal cortex, and supplementary motor area, results in proper postural balance. 2
All of these brain areas work together to produce a correlated pattern of muscle activation during motion and response to sensory feedback from external perturbations. In particular, M1 is crucial in anticipatory adjustments in task-related postural regulation and the initiation of voluntary movement to maintain stability during movement. 2,3
An indication of a deteriorated balance is an increase in the displacement in the velocity of the center of pressure (COP) while standing in a static position. 4 A study revealed that there is a constant increase in COP over the human life span, which begins in middle age. Furthermore, the same study revealed that deficits in lower extremity reach appeared in the same age group and deteriorated over time. 5
A deteriorated balance increases the risk of falling and affects an individual's capacity to participate in daily life activities; however, the first signs of balance impairment begin during middle age. 2 Addressing balance deficits is crucial in clinical practice, since its early intervention could delay fall risk in older populations.
To address the balance deficits, balance exercises are frequently used in sports and neuromuscular training programs to improve performance, reduce injury, and provide rehabilitation. Exercise therapy has been used traditionally in the treatment and prevention of balance disorders in the form of balance training (BT). 2,6
Although there is evidence to support the use of BT for the treatment or prevention of balance disorders, its use is challenging because it involves numerous weeks of training (8–24 weeks) to yield positive effects, which is both time and money intensive. 6,7 Furthermore, some studies on BT support only minor to moderate effects, particularly in older adults. 2,8,9 As a result, developing a method for improving balance and reducing imbalance disorders is an important step forward that could lead to better management of balance deficits and a reduction in the future burden of diseases associated with poor balance.
In recent years, noninvasive brain stimulation techniques have gained interest as tools for modulating cortical excitability in a range of clinical settings and experimental conditions to improve behavioral outcomes such as balance. 10,11 Transcranial direct current stimulation (tDCS) is a noninvasive stimulation technique that emits continuous low-intensity electric current to specific areas of the scalp over different regions of the cerebral cortex using two or more electrodes. 12 Its effects depend on the combined influence of the polarity of the current, intensity, and time of application. 13,14 For example, an anodal current applied at 1 mA intensity for 15 min increases cortical excitability, whereas a cathodal current with the same parameters decreases cortical excitability. 15
tDCS has been promoted as a useful technique for improving physical exercise and balance. 16,17 A study that applied tDCS over the M1 combined with postural training in an older adult population for 2 weeks found improvements in static and dynamic balance. 18 Another study determined the short effect of tDCS over M1 on static and dynamic postural stability in young healthy adults, obtaining improvement effects in both. 19
Based on the evidence regarding the efficacy of tDCS in improving balance in young and older populations, it can be expected that when combined with BT, tDCS may have positive effects on early intervention and delay of balance deficits in middle-aged adults. In addition, to the best of the authors' knowledge, the combined effects of BT and tDCS in this population have yet to be investigated.
Following past studies on tDCS application, the authors hypothesized that tDCS combined with BT would improve static and dynamic balance in middle-aged adults. In addition, it is a safe intervention for use in future regular physical training.
Materials and Methods
Participants
The sample size, determined using G*Power 3.1.9.7 (Franz Faul, University Kiel, Kiel, Germany), was calculated with an F test, statistical test: repeated measures analysis of variance (ANOVA), within-between interaction, type 1 error rate set at 5%, a desired power of 80%, and an effect size of f 0.25 for two groups. 20 Consequently, a total sample size of 28 participants was estimated to determine the differences in outcome measurement scores.
Twenty-eight participants (14 men and 14 women) aging 36–62 years met the inclusion criteria. The selected participants were randomly distributed into two groups: active (active tDCS + BT) and sham (sham tDCS + BT).
The inclusion criteria were as follows: (1) men and women, (2) aging between 36 and 64 years, and (3) no acute or chronic muscular pain. The exclusion criteria were as follows: (1) presence of neoplasm; (2) orthopedic deformities; (3) pregnancy; (4) evidence of skin disease or abnormalities near the tDCS application area; (5) history of epileptic seizures; (6) metal implants in the skull; (7) use of hearing aids and anticonvulsants or muscle relaxant drugs; (8) neurologic disorders, such as epilepsy, Alzheimer disease and other dementias, stroke, multiple sclerosis, Parkinson's disease, neuroinfections, brain tumors, or traumatic disorders of the nervous system; (9) medical conditions, such as rheumatologic diseases (osteoarthritis, rheumatoid arthritis, lupus, Sjogren's syndrome, gout, scleroderma, and infectious arthritis; and (10) drug or alcohol dependence or abuse.
The study was approved by the Institutional Review Board of Korea University (KUIRB-2021-0372-01) and registered under the number: KCT0007414 (https://cris.nih.go.kr/). It was carried out in accordance with the 1964 Declaration of Helsinki. Additionally, the Consolidated Standards of Reporting Trials (CONSORT) checklist is included as Supplementary Material.
The participants were recruited through advertisements, and after a month of receiving a full general description of the study, they signed an informed consent form. They were free to leave the study at any time, without any consequences.
Experimental design
This study was a randomized double-blind sham-controlled trial designed to evaluate the effectiveness, safety, and satisfaction of a middle-aged population on the combined application of tDCS and BT on balance over 6 weeks (thrice per week). The participants were distributed into two groups (active and sham) in a 1:1 ratio by using simple randomization through a computer-generated list (https://www.randomlists.com/team-generator) (Fig. 1).

Flowchart of the study based on Consolidated Standards of Reporting Trials. tDCS, transcranial direct current stimulation.
It was performed by the researcher in charge of applying the tDCS intervention to the participants, who was not present during the outcome measurement periods or the BT training. The participants were unaware of the group to which they belonged until the completion of the study, and the data were analyzed.
The intervention and measurements were performed in a training center called Startrain Fitness Center (Seoul, South Korea). tDCS was applied in a meeting room within the center, whereas BT was executed in a regular training area.
During the intervention period, participants were instructed not to drink coffee or alcoholic beverages and to abstain from participating in any other external physical activity.
Intervention
Transcranial direct current stimulation
Participants underwent 18 sessions of active tDCS or sham tDCS (thrice per week for 6 weeks) for 20 min, and the stimulation intensity was set to 2 mA. Wireless rechargeable tDCS (Y-brain Inc., Seoul, Korea) with anodal and cathode electrodes, 6 cm in diameter and covered with 0.9% NaCl sponges, was used. In the active group, the anodal electrode was placed over M1 on the nondominant side (over the C3 or C4 zone of the 10/20 electroencephalogram coordinates) and the cathode electrode was placed over the supraorbital zone on the opposite side (Fig. 2). Rubber bandages were used to secure both electrodes. The sham group had the same electrode montage as that of the active group.
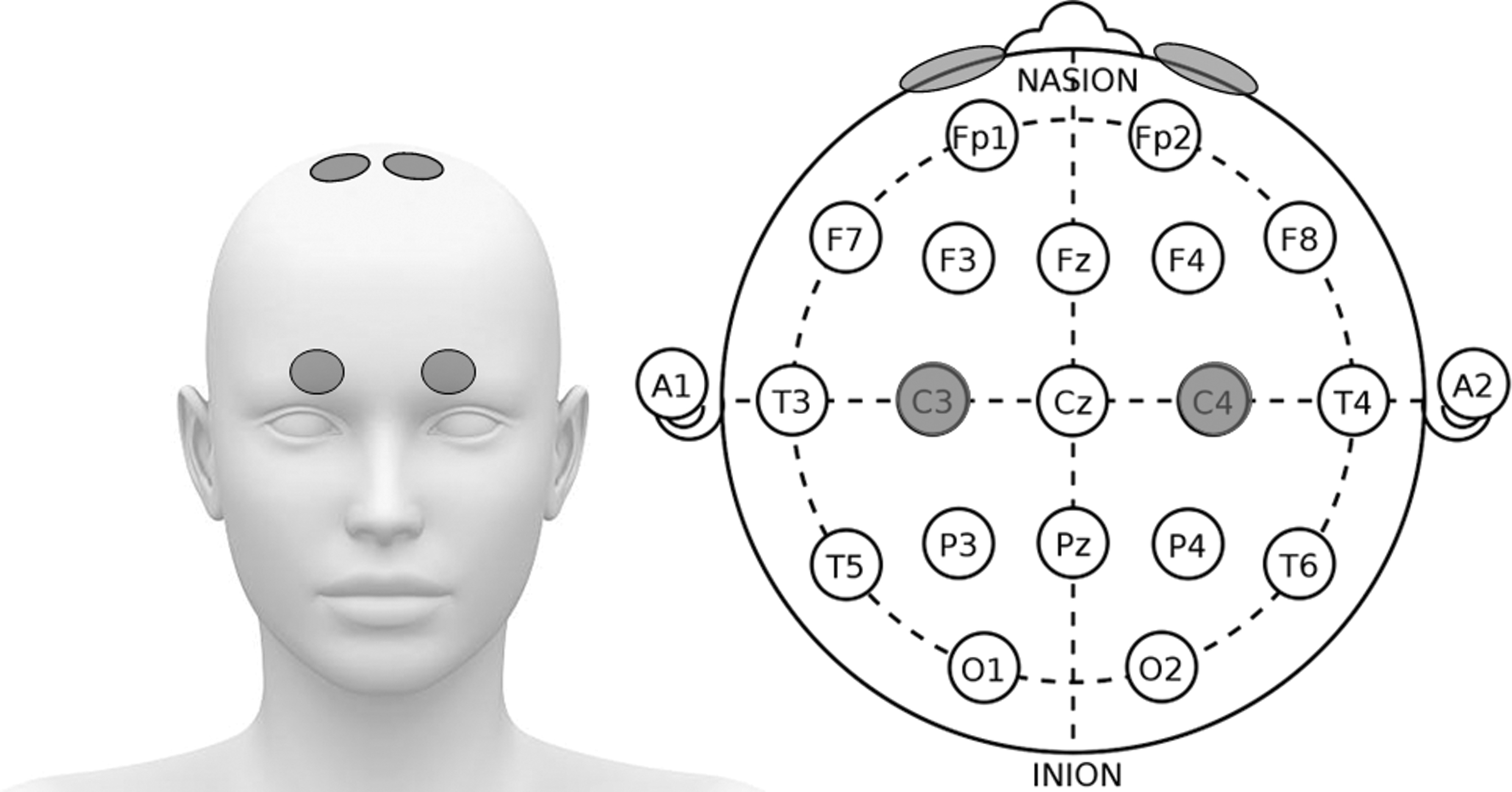
Transcranial direct current stimulation electrode positions based on the nondominant side. Anode located on the nondominant side (C3 or C4) and Cathode over the supraorbital zone on the opposite side.
The intensity and duration were selected based on a systematic review that reported the effectiveness of tDCS protocol for balance improvement. 2 In addition, the nondominant side was targeted to prevent any potential ceiling impact, because there is greater potential for further improvement owing to optimal cortical excitability, inhibition, and descending drive.
tDCS was administered using a ramp protocol. The device was set to ramp-up the current in 30 sec to minimize the discomfort sensation for the participant. The sham tDCS was programmed to ramp-up for 30 sec and then ramp-down for another 30 sec. This is a reliable method for generating the initial sensation associated with tDCS, and the sensations generated are easily perceivable by individuals.
Participants were informed that they could stop participating in the study at any moment if they experienced any discomfort (headache, itching, tingling, or burning sensations).
Balance training
After tDCS application, all participants underwent a supervised identical 40-min BT program thrice per week for 6 weeks. The BT program was based on a systematic review stating that BT programs with various exercises and a small number of sets showed better balance improvements. In addition, the same study suggested that BT should include exercises that promote static/dynamic steady state, proactive, and reactive balance. 7 The BT program was performed in small groups of seven people composed of participants from both sham and active groups.
Therefore, the program consisted of two sets of exercises, each lasting ∼16 min, with a 30 sec rest between sets. Each set included two series of individual exercises, with a 10 sec rest between switching exercise series.
The first group of exercises consisted of jump rope, sidestep jumps, in–out jumps, and box steps. These exercises were performed as many times as possible for 1 min. The second group included bipedal standing on a wobble board (front–back with switch to side–side movements), one-leg standing on a wobble cushion, one-leg standing with clapping under the leg, and the Superman plank. Each exercise was executed for 30 sec before switching. During the first set, the exercises were performed with eyes open, whereas during the second set, the same exercises were executed with eyes closed.
Outcome measurement tools
Demographic and outcome data were collected from all participants at baseline. Postintervention data were assessed immediately after the last intervention. The measurements were performed by two physical therapists with >4 years of experience and expertise in the tests. The physical therapists were unaware of the group affiliation of the participants.
Static balance
The ability to maintain an upright posture and retain the line of gravity within the limits of the base of support is known as static balance. 21 Static balance parameters were obtained using Zebris FDM-T Treadmill data (Zebris Medical GmbH, Germany). The treadmill was fitted with an electronic mat embedded underneath the belt consisting of 10,240 sensors, each ∼0.85 × 0.85 cm. The force exerted by the feet was recorded as the participants stood on the treadmill.
The dedicated software was integrated into the force signals and provided a two-dimensional or three-dimensional graphic representation of the COP trajectories during the static stance. The participants stood under two different conditions (eyes open and closed) to measure the sway rate. Each session was repeated thrice for 30 sec. While standing, the participants maintained a posture while visually focusing on a dot marked 1 m in front of them. The mean sway rate was assessed under the same conditions.
Dynamic balance
The ability to maintain balance while moving by maintaining the body's center of gravity over the base of support is known as dynamic balance. 22 The parameters were measured using the functional reach test (FRT). The FRT is a clinical outcome measure and assessment tool for ascertaining dynamic balance in simple tasks. The FRT assesses the forward stability of a participant while standing and extending one arm as forward as possible in the horizontal plane while keeping both heels in contact with the ground. The score was calculated by measuring the distance between the start and end positions of the fingertips. 23
Adequacy of blinding, safety, and participants' satisfaction assessment
At the end of the study, the participants were asked to complete an anonymous survey about their experiences during the intervention. To probe the correct blinding of the participants during the study, the participants were asked to answer whether they felt they belonged to the sham or active group as well as the sensations they perceived during tDCS application. The survey questioned the presence of any side effects during and after tDCS application as well as the overall satisfaction with the combined tDCS and BT program.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to examine data normality. There was no evidence of non-normality for the three variables examined: FRT [W(28) = 0.95, p = 0.30], sway with eyes open [W(28) = 0.93, p = 0.10], or sway with eyes closed [W(28) = 0.93, p = 0.18]. After verifying normality, a 2 × 2 (group × time) two-way repeated-measures ANOVA was used to assess differences in dependent variables (FRT, sway with eyes open and closed), with the significance level set at p < 0.05. In addition, one-way analysis of covariance (ANCOVA) was conducted to determine the differences in the dependent variables between the two groups at the post-test time point after adjusting for baseline values.
A chi-square test was performed to determine the association between the results of the adequacy of blinding survey and the actual intervention allocation.
Results
The trial was concluded by all 28 participants after the last postevaluation was performed and the data analysis was completed. Without any inconvenience to report, all the participants successfully attended all the scheduled sessions.
The active group mean age was 50 (standard deviation [SD] = 6.69) years with a median of 51 (interquartile range [IQR] = 44.7, 54.25), whereas the sham group mean age was 49.28 (SD = 9.74) years with a median of 50 (IQR = 41, 57.5). Detailed demographic data are described in Table 1.
Demographic Characteristics of the Participants
Mean (SD) (n = 28). Active group: active transcranial direct current stimulation + balance training; sham group: sham transcranial direct current stimulation + balance training.
BMI, body mass index; SD, standard deviation.
The outcome measurement characteristics are detailed in Tables 2 –4.
Mean ± Standard Deviation of Functional Reach Test, Sway Rate (Opened Eyes) and Sway Rate (Closed Eyes) for the Active and Sham Groups
There was no significant difference at baseline between the groups. Active group: active transcranial direct current stimulation + balance training; sham group: sham transcranial direct current stimulation + balance training.
FRT, functional reach test; SD, standard deviation.
Adequacy of Blinding
Active group: active tDCS + balance training; sham group: sham tDCS + balance training.
N, number of participants; tDCS, transcranial direct current stimulation.
Transcranial Direct Current Stimulation Safety Assessment
Active group: active tDCS + balance training; sham group: sham tDCS + balance training.
N, number of participants; N/A, no answer; tDCS, transcranial direct current stimulation.
Static and dynamic balance
Two-way repeated-measures ANOVA scores for static balance showed a significant effect over time and between time and group. In the case of sway rate with eyes open, the effect over time was F(1, 26) = 20.84, p < 0.001, whereas that between time and group was F(1, 26) = 4.95, p = 0.04. For sway rate with eyes closed, the effect over time was F(1, 26) = 23.02, p < 0.001, and the effect between time and group was F(1, 26) = 6.07, p = 0.02.
The one-way ANCOVA results revealed significant differences in the post-test sway rate with eyes opened scores between groups, adjusted for baseline (F = 4.889, p = 0.036), as well as in the sway rate with eyes closed scores (F = 10.980, p = 0.003).
For the dynamic balance (FRT scores), the two-way repeated-measures ANOVA scores also showed a significant effect at all times with F(1, 26) = 66.13, p < 0.001, whereas the effect over time and group was F(1, 26) = 5.38, p = 0.03.
The one-way ANCOVA results revealed significant differences in the post-test FRT values between groups, adjusted for baseline (F = 6.053, p = 0.021).
Adequacy of blinding, safety, and participants' satisfaction assessment
Overall, according to the chi-square (1) = 0.243; p = 0.62, the blinding was successful, as only 3 out of 14 participants correctly guessed the sham, whereas the active group had 2 participants guessing that they were part of the sham group.
Furthermore, there were no serious side effects, such as dizziness, headache, swelling, redness, or temperature increase in the area of tDCS application during and after tDCS application. Only one participant in the sham group admitted to experiencing a headache while using tDCS; however, it disappeared quickly thereafter. As well, only three participants reported an itching sensation that disappeared during or after tDCS use without any lasting additional sensations.
The survey revealed that >80% of participants were satisfied with the combined program. Although the intensity of the exercises was mainly described as hard or moderate, the recovery time after completion of the program was short. Furthermore, the participants expressed their willingness to recommend the program to others. Although seven participants agreed that they wanted to quit the program at some point, the given reasons were lack of time, the program was difficult to follow, and the training center was far from their residence (Table 5).
Participant Satisfaction Assessment
Active group: active tDCS + balance training; sham group: sham tDCS + balance training.
N, number of participants; N/A, no answer; tDCS, transcranial direct current stimulation.
Discussion
This study aimed to assess the effectiveness of tDCS combined with BT in static and dynamic balance and determine the safety and satisfaction of middle-aged men with the combined intervention for future implementation in regular physical training. The results showed that tDCS combined with BT for 6 weeks, thrice per week, was effective in improving static and dynamic balance compared to BT alone. In addition, the participants showed great satisfaction with the program and a willingness to continue and recommend it to others.
Previous studies have shown that tDCS over the M1 area of the bilateral limbs improves balance in healthy individuals (younger and older adults). A systematic review that studied the effects of a single session of tDCS on postural balance found that tDCS over the M1 seemed to be the most effective in improving balance, specifically under a protocol of 1–2 mA and an application time of 15–20 min 2 , which correlates with this study. Different studies have shown that central stimulation of the M1 (10–20% before CZ) increases cortical excitability and reinforces neuroplasticity over the bilateral lower limb zone, proving to be effective in improving balance in healthy individuals as well as in people with leukoaraiosis, stroke, and cerebral palsy. 3,24 –28 In addition, tDCS over the M1 appears to improve kinematic variable velocity during a dynamic balance task in healthy adults. 29
In addition, the results showed that the combined application of anodal tDCS and BT was more effective than BT alone. Previous studies have shown that anodal tDCS, together with other tasks, is more effective at enhancing motor function and balance. A study that combined tDCS with constraint-induced movement therapy for the recovery of motor function in patients with stroke reported that the combined intervention was more effective than constraint-induced movement therapy alone. 30 Another study combined gait training and anodal tDCS to improve balance in children with cerebral palsy and found positive effects, with a reduction in COP sway with eyes closed and open in the experimental group. 31
BT typically requires several weeks of training to demonstrate effects. Studies have shown that an effective BT protocol should last between 11 and 12 weeks, with a frequency of 3–6 training sessions per week and a duration of 11–15 min for each session. 6,7 However, a study showed that static postural sway on stable platforms improved after 6 weeks of BT. 6 This study considered the aforementioned information and performed an intervention protocol that combined the minimum BT required to improve balance with an anodal tDCS set within the parameters proven to be effective in previous studies.
In addition, the survey demonstrated that tDCS is safe for use in this population, with minimal health risks. Furthermore, the participants' satisfaction assessments generally revealed positive responses from the active and sham groups. This includes opening the possibility of integrating tDCS with BT in normal program settings in physical training centers.
The authors' findings corroborate that tDCS with BT is an effective and safe practice to improve balance in a middle-aged healthy population and could be used in the near future as a regular training technique for healthy people.
This study is a subanalysis of a study involving a sample of 55 participants, which includes participants aging between 19 and 35 years (young adults). After conducting initial data analysis and in-depth research, it was planned to publish one article with the complete data set and another focusing solely on the middle-aged participants. This decision was motivated by extensive research, which revealed that, to the best of the authors' knowledge, even though there is evidence showing that the increase in the displacement in the velocity of the COP while standing in a static position starts from this age group, there are no studies focused on the improvement of balance in this population through tDCS intervention.
The authors believe that this article could promote preventive therapy in middle-aged adults, as enhancing balance from this age could greatly benefit the older adult population by reducing accidents caused by balance deficits.
This study's limitation is the absence of a follow-up assessment to evaluate the extended effects of the intervention in this population. Future research should include follow-up testing to better understand the long-term effects of tDCS and BT on the delay of balance deficit.
Conclusion
According to the findings of this study, anodal tDCS combined with BT was more successful than BT alone in enhancing static balance with closed and open eyes in a healthy population and increased dynamic balance compared with sham tDCS. Furthermore, the use of tDCS was considered safe, with minimal to no side effects, and participants reported satisfaction with the new intervention. Therefore, this study can be considered as a step forward in the use of anodal tDCS as part of regular BT to avoid injuries and minimize the risk of balance impairment.
Footnotes
Acknowledgments
The authors are grateful to the Startrain Fitness Center (Seoul, South Korea) for their assistance in recruiting participants and facilitating their installation to complete this study successfully. The authors also thank Y-Brain for supplying the tDCS device used in this study.
Authors' Contributions
Conceptualization, methodology, and writing—original draft by J.J. Data curation, formal analysis, writing—review and editing, and visualization by J.C.S.F. Investigation by S.K. and B.K. Project administration by S.O. Conceptualization and supervision by B.C.Y.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This research was supported by Korea University (Grant No. K2220181), and the R&D Program for Forest Science Technology (Project No. 2021407A00-2225-0101) provided by Korea Forest Service (Korea Forestry Promotion Institute).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.