
Abstract
Introduction:
Severe pain, anxiety, and high opioid use are common following lumbar spine surgery (LSS). Yoga helps to reduce pain and anxiety, but it has not been considered for postsurgical care. The authors developed and tested the feasibility of a tailored yoga program designed for individuals undergoing LSS and explored clinical feasibility of yoga intervention on measures of pain, function, psychological status, and opioid use.
Methods:
Individuals scheduled for LSS were randomized into yoga versus control groups presurgery. Participants in the yoga group received tailored yoga sessions plus usual care, whereas participants in the control group received usual care only during the hospital stay post-LSS. In-person daily yoga sessions were individually presented and performed in the participant's hospital room. Feasibility was assessed by recruitment and retention rates, rate of yoga session completion, tolerance to yoga intervention, and ability to carry out planned assessment. Exploratory clinical outcomes included pain, psychological measures, Timed-Up-and-Go test, gait distance, and opioid use, during the hospital stay post-LSS.
Results:
Forty-one participants were enrolled, of which 30 completed. There were no dropouts. Planned assessments were completed within 45 min, suggesting no excessive burden on participants. Baseline variables were similar across both groups. The majority of participants participated in yoga intervention on the day of surgery or one day after surgery with acceptance rate of 100%. Participants showed good tolerance to yoga intervention on 0–4 tolerance scale and by their reports of exploratory clinical outcomes.
Conclusion:
This study indicates feasibility for a modified yoga program for postoperative care following LSS due to participant tolerance and retention. The results provide preliminary framework for future confirmatory studies that can assess the potential benefits of yoga in reducing pain, catastrophizing behavior, and opioid use and improving function. A modified yoga program focusing on diaphragmatic breathing, relaxation, and core isometric contraction exercises can be an important adjunct intervention for patients undergoing LSS.
CTR Number: This trial was registered in UMIN CTR (https://rctportal.niph.go.jp/en/) with registration number: UMIN000032595.
Introduction
The prevalence of lumbar spine surgery (LSS) is rising internationally, 1 with the highest increase in the United States. 1,2 Laminectomy/discectomy with or without fusion are common treatment options for disc or degenerative lumbar conditions. 3 Due to the complex nature of LSS, severe postoperative pain is common, with ∼80% of patients experiencing moderate-to-severe pain at discharge. 4,5 Severity of postoperative pain adversely affects outcomes, including associated anxiety, 6 less participation in rehabilitation, decreased function, and delayed mobility. 7 Severe acute pain, anxiety, depression, pain catastrophizing behavior, and high consumption of opioids are also risk factors for the development of chronic postoperative pain and opioid reliance. 8,9
Acute postoperative pain management is challenging and current practice is primarily limited to medication utilizing opioids alone or a combined multimodal pharmacological approach. 10,11 However, high opioid consumption during hospital stay does not translate into better outcomes of pain or function. 12 Patient walking distance is a strong predictor of hospital length of stay and discharge planning. 13 The ability to function depends on effective pain management strategies. Furthermore, psychological symptoms, such as anxiety and pain catastrophizing have been associated with poor functional recovery, increased opioid use, and persistent pain following LSS. 10 However, current practices do not routinely address psychological issues. Thus, there is a need for additional interventions to manage acute postoperative pain and optimize physical and psychological wellbeing during perioperative period post-LSS.
Yoga as an integrative medicine has shown to be effective for managing chronic pain, disability, and psychological stress, 14 –17 but its feasibility for postoperative care has not been tested. Scientific evidence is sparse in examining the benefits of yoga for postoperative care. Yoga that focuses on mind–body components are a potentially safe avenue to mitigate acute pain and anxiety, reduce opioid intake, and engage core muscle activation; all factors are important for acute and long-term recovery post-LSS. Mindfulness meditation and diaphragmatic breathing of yoga induces relaxation and reduces anxiety, 14,18 through the central 19,20 and the parasympathetic nervous system, 19,21 leading to reduced pain 22 –24 and potentially less use of opioids that impede patient recovery. 25
A few previous studies have demonstrated the feasibility and therapeutic benefits of yoga with acute conditions. 26 –29 Yoga/mindfulness meditation lessened experimental pain in healthy individuals, acute pain in women undergoing gynecologic surgery, 29 and in hospitalized children with sickle cell disease. 30 Relaxation breathing was linked to improvements in pain, anxiety, and trunk control. Yogic relaxation and diaphragmatic breathing lessened anxiety in hospitalized patients with traumatic brain injury, 31 spinal cord injury, COVID-19, 32 hematological cancer, 33 and children with cancer. 28 Diaphragmatic breathing equalizes abdominal and thoracic cavity pressure and is a possible mechanism for improving trunk control. 23,34 Isometric contraction during yoga practice (volitional preemptive abdominal contraction series) engages key core muscles 34,35 (transverse abdominis, pelvic floor musculature, and multifidi) that are important for trunk stability following LSS.
Thus, a tailored yoga program seems to be an ideal supplement to post-LSS recovery while considering surgical precautions. No prior study has tested the feasibility of yoga intervention and explored its potential effects on pain and anxiety in patients undergoing LSS. The primary objective of this pilot randomized trial was to determine feasibility of the tailored yoga intervention implemented during the hospital stay post-LSS. We also explored how yoga intervention may influence measures of postoperative care, for example, acute pain, psychological stress, function, opioid use, and length of hospital stay. We hypothesized it is feasible for patients to practice modified yoga intervention while considering the participant's pain, anxiety, medication use, and function during hospitalization.
Methods
Study design
Study methodology has been previously published 36 outlining development of a tailored yoga program for post-LSS and randomized controlled design yoga versus usual care during hospital stay. This article focuses on the feasibility and exploratory clinical measures during hospitalization post-LSS. The study was conducted at the University of Kansas Medical Center. The study was approved by the Institutional Review Board (IRB No. 4283). Targeted sample estimation was 20 participants per group, based on recommended sample size for feasibility trials 37,38 and estimated 80% retention rate. The Consolidated Standards of Reporting Trials (CONSORT) flow diagram (Fig. 1) describes the study methodology and sample size.
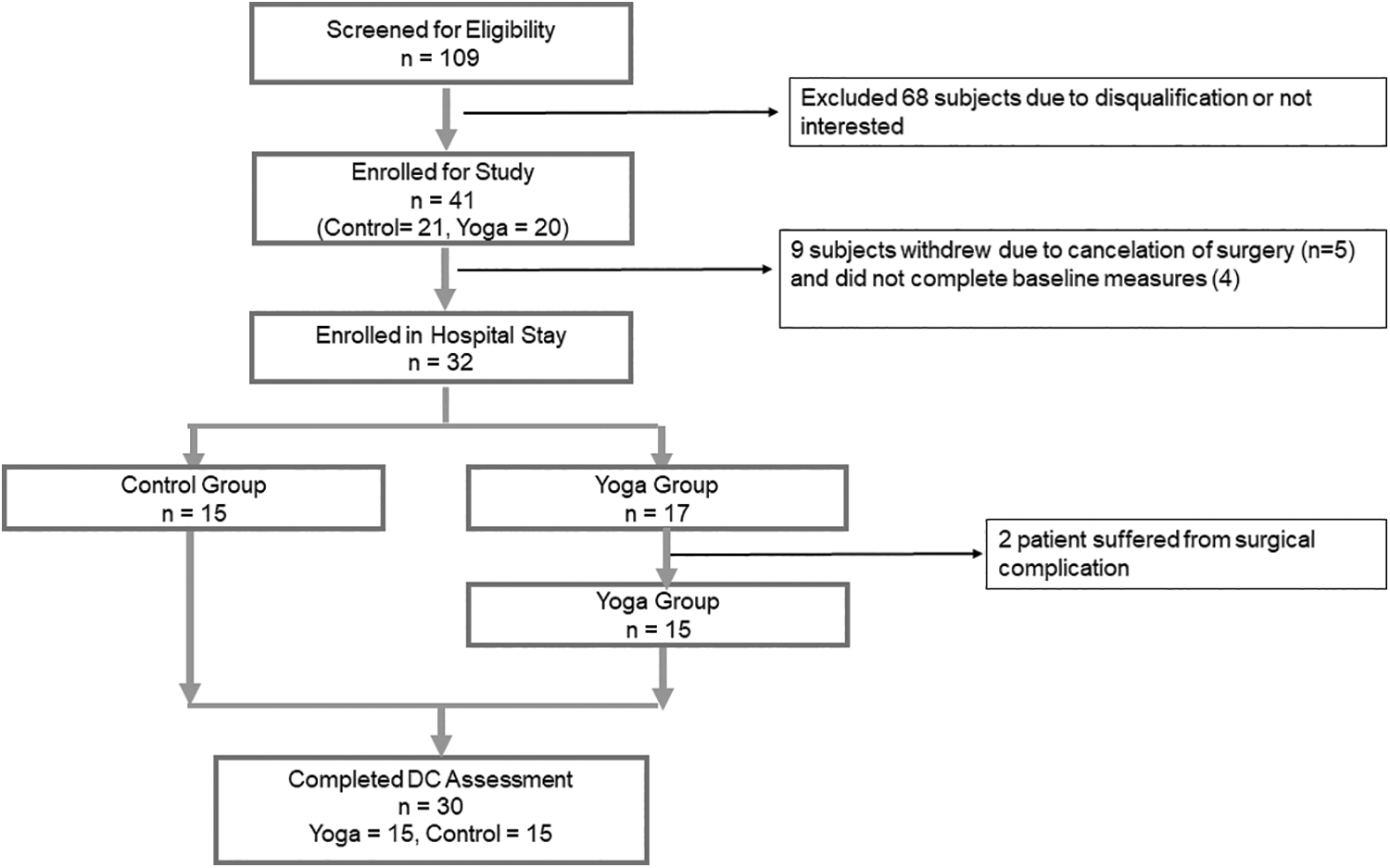
Consolidated Standards of Reporting Trials diagram.
Study population
All English-comprehending patients scheduled for LSS of laminectomy with or without fusion were eligible and recruited at the preoperative visit from participating surgeons' clinics. We included individuals between the ages of 40 and 80 years who had not practiced regular yoga within the past 6 months. Exclusion criteria included cancer-related spine pain, cauda equina syndrome, psychiatric illness, dementia, or spinal tumor and more than two previous lumbar surgeries (laminectomy or fusion). Predetermined withdrawal criteria included postoperative complications such as admission to intensive care, blood clots, surgical-site dehiscence, infection, and requirement of restricted mobility during the hospitalization.
Eligible participants were consented at the presurgery visit and were randomized to either the intervention group who received standard care plus tailored yoga or to the control group who received standard hospital care. Computer-generated block randomization was used to ensure equal sample/group allocation. Assessors collecting outcomes were blinded to group allocation.
Outcomes
The primary outcome of feasibility was defined as 80% success rate in the following measures: recruitment and retention rates, rate of compliance (refusal/lack of participation in yoga sessions), and ability to complete planned assessment (proportion and duration) and tolerance to yoga practice (change in pain rating pre/post each session; duration of yoga participation/session and yoga teacher-assigned tolerance level). Tolerance to planned assessment was assessed by the number of participants willing to complete the assessment and duration of assessment. Tolerance to yoga was assessed with 0–4 Likert scale (0 = no tolerance and 4 = excellent tolerance).
To strengthen the feasibility of the trial, the following exploratory clinical outcomes were included: pain, psychological stress, function, and opioid use. These outcomes are relevant to postoperative care, discharge planning, and patient health needs. The outcomes were assessed with standard and validated questionnaires at baseline (presurgery visit) and hospital discharge. Pain intensity was assessed with the Numeric Rating Pain Scale (NRS; 0–10 scale). 39 The Beck Anxiety Index measured anxiety on a scale of 0–63 categorized from low to high anxiety. 40
The Perceived Stress Scale used a scale of 0–40 for no to high perceived psychological stress levels. 41 The Pain Catastrophizing Scale quantified catastrophic thinking related to pain having three subscales of rumination, magnification, and helplessness, where a total score above 30 indicates clinically relevant level of catastrophizing thoughts and behavior. 42 Finally, the Timed-Up-and-Go test measured physical functional mobility. 43,44 In addition, daily pain (NRS), function (walking/gait distance in feet), and opioid consumption (Oral Morphine Equivalent) for the duration of the hospitalization length of hospital stay 13 data were collected from the Electronic medical records (EMR).
Yoga interventions
A tailored yoga intervention specifically designed to improve pain, anxiety, and trunk stability for the individuals undergoing LSS was created in collaboration with the participating surgeons. 36 The yoga intervention considered stringent surgery precautions of no twisting, stooping, squatting, pushing/pulling, crawling, reaching overhead, or no prolonged sitting or standing for 8–12 weeks. The yoga program focused on diaphragmatic breathing, relaxation, and core isometric contraction that was tailored for postsurgical recovery.
Two certified yoga teachers implemented the yoga intervention of each individual patient in a one-on-one session. The intervention was delivered in-person, each day during hospital stay starting as early as the day of the surgery. Participants performed the intervention in the position of comfort (supine or reclined) maintaining neutral trunk posture in their hospital room. Each yoga component was progressed based on the participant tolerance, ability to maintain neutral posture and activation of core/pelvic muscles while monitoring pain and discomfort level. Before and after completion of each yoga session, participants were asked to rate their back pain.
Control intervention
Participants in the control group received usual standard care of pain medications, rehabilitation services, and nursing care without yoga intervention.
Statistical analysis
Feasibility of the yoga intervention was analyzed with descriptive statistics using Sigma Plot 14.0 software. After meeting normality assumption with Shapiro–Wilk test, outcomes were reported as means and standard deviations for continuous variables and frequencies or percentages for categorical variables. Variables were inspected for any differences at baseline between the groups. Changes in exploratory variables from baseline to hospital discharge (pre/post) and pre/post yoga sessions were averaged and reported as descriptive statistics. Hospital stay variables, for example, hospital length of stay and EMR outcomes (pain, gait distance, opioid use) were described with mean changes from day one to hospital discharge without conducting any statistical analyses between the groups due to small sample size, using SPSS software (version 26).
Results
Participant characteristics
Participant baseline characteristics are shown in Table 1. Participants in both groups were similar with regard to demographics, low back pain (LBP) history, and medication status. The majority of participants across both groups were mid-60's white and non-Hispanic with a BMI in the obesity range. Participants experienced moderate-intensity chronic LBP defined as 4–6 on NRS. 42 This was the first LSS for majority of participants. A similar number of participants in both groups used opioids and other pain medications before the surgery.
Participant Demographics and Baseline Characteristics
F, Friday; M, Monday; NSAIDS, non-steroidal anti-inflammatory drugs; SD, standard deviation.
Feasibility
The study met 100% of the feasibility goals regarding recruitment/retention, compliance (acceptance and participation), and tolerance to yoga intervention. The CONSORT diagram (Fig. 1) outlines the recruitment and retention process. One hundred and nine participants scheduled for LSS were screened. Forty-one qualified and consented to participate, indicating 100% target sample size achievement. Nine patients did not participate in the study; four participants did not complete baseline data/withdrew from the study, suggesting 90% success rate (4/41) and five participants' surgery was canceled. Thus, an overall presurgical attrition rate was 22%, leaving 32 enrolled in the study at the time of surgery. All enrolled participants agreed to be randomized and none refused to participate due to randomization. Planned assessment was entirely completed without any deviation. The estimated duration for assessment completion was 45 min. No participants dropped out following completion of baseline due to assessment's burden. Of 32 participants, 30 completed the study, indicating 97% postsurgical retention rate.
Two participants in the yoga group were excluded during the study due to meeting the withdrawal criteria of postsurgical complication (dural leak, infection) leaving 15 participants in each group. There was zero dropout rate across both groups.
Compliance rate of yoga intervention for all 15 participants was 100%. No patient refused the yoga intervention. Four participants began yoga on the day of surgery, 9 began yoga the next day, and 2 started yoga 2 days after surgery with an average of 2.07 days that intervention was offered. Of 31 sessions completed, 18 were performed in supine/reclined, 4 in side lying, and 9 in the sitting position.
The average duration/visit was 37.5 min with average time/component: meditation = 5.10 min, breathing = 4.93 min, and physical movement = 4.71 min (Table 2). Overall tolerance was good. The intervention was delivered entirely as initially planned and described in the previously published methodology article. 36 On average, participants reported presession pain (5.03 ± 2.9) and postsession pain (4.46 ± 2.9). One participant did not provide pain rating postsession. No participants reported increased pain from yoga sessions. Pain rating remained the same for 50% of the sessions and decreased during 50% of sessions.
Feasibility of Yoga Intervention
Tolerance was rated on 0–4 Likert scale: 0 = no tolerance, 1 = poor, 2 = fair, 3 = good, 4 = excellent.
Table 3 shows the descriptive results of exploratory clinical outcomes with change in score from baseline to discharge/group. Figure 2 displays baseline and discharge scores of perceived stress for both groups. Baseline measures were similar but change in score from baseline to discharge in the yoga group was 22 points, suggesting clinically meaningful improvement. Figure 3 displays catastrophizing behavior of total scores/group (baseline and discharge), change in scores and three subsections: rumination, magnification, and helplessness from baseline to hospital discharge.
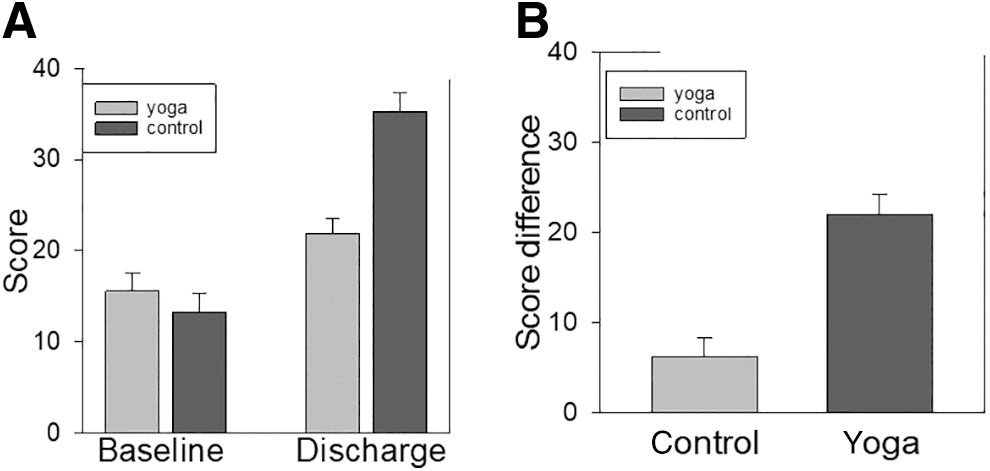
Perceived Stress Scale: Baseline and Discharge
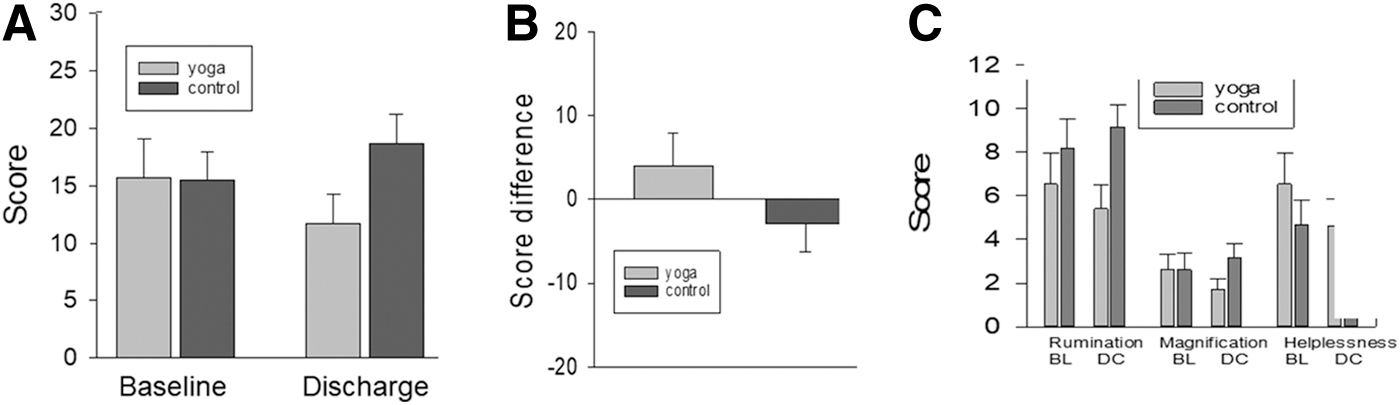
Pain Catastrophizing Scores: Baseline and Discharge
Clinical Outcomes: Change in Scores from Baseline to Hospital Discharge
NRS, Numeric Rating Pain Scale.
Figures 4–6 show averages for pain, gait distance, and opioid consumption for each day/hospitalization across both groups (Figs. 4A, 5A, and 6A) and change in scores from day 1 to discharge (Figs. 4B, 5B, and 6B), respectively. This information can be used to gain an understanding of pattern of each variable/group/day across these clinical measures. Average length of stay for yoga group was 3.93 ± 0.27 and for control group was 4.40 ± 0.36 days. The results demonstrate that none of the clinical measures was negatively impacted by the yoga intervention and a potential positive impact on participants' perceived stress.

Numeric Rating Pain Scores
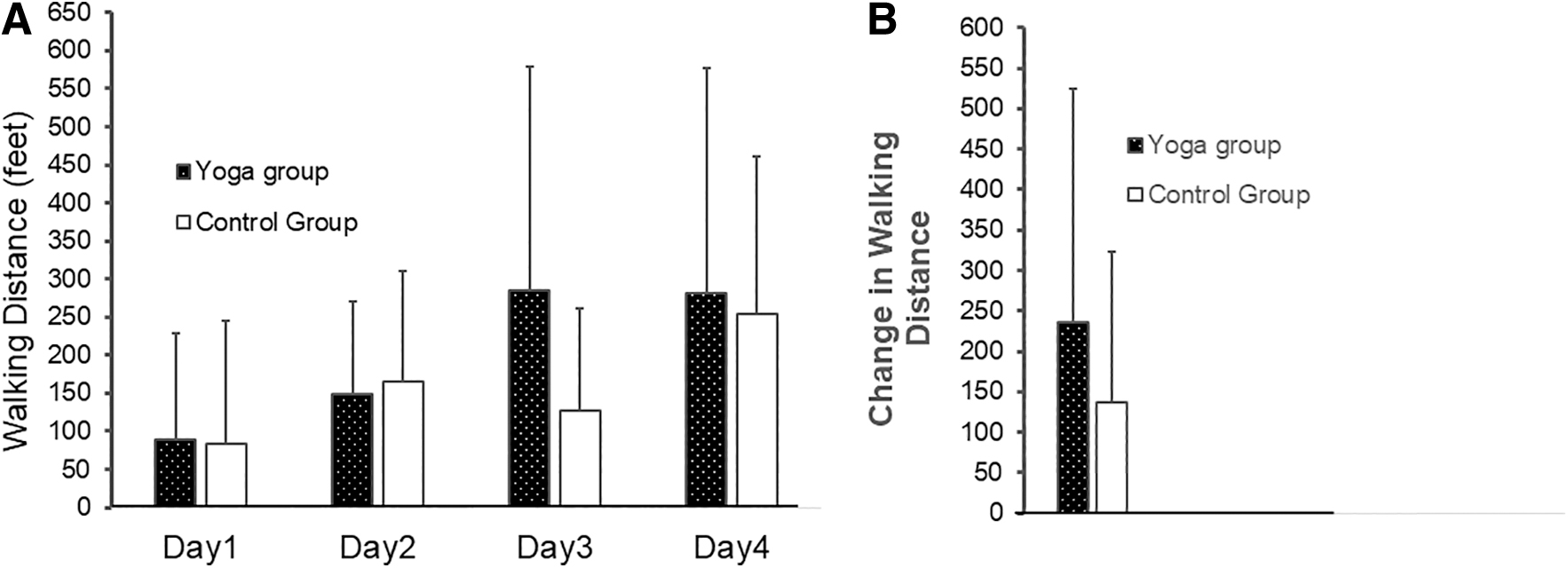
Gait Distance
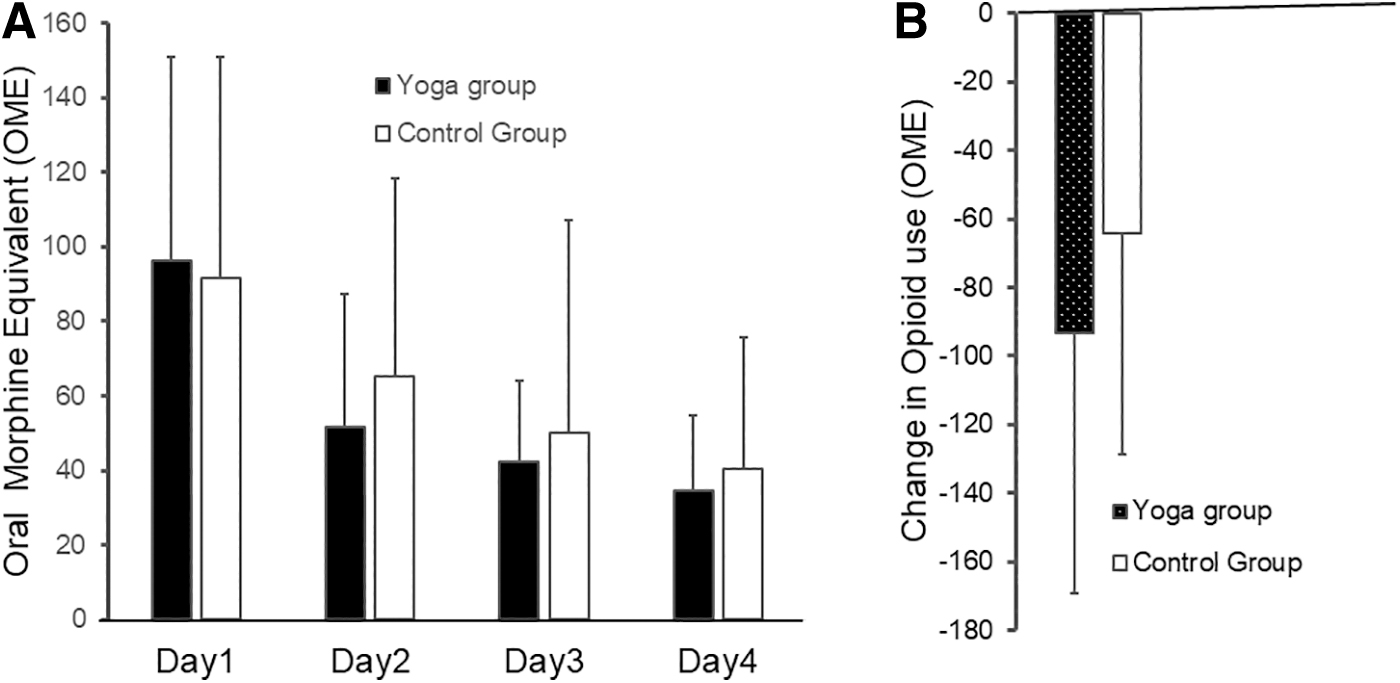
Opioid Consumption
Discussion
This is the first randomized yoga pilot trial designed to investigate the feasibility of incorporating a tailored yoga program in the inpatient hospital environment for individuals with acute post-LSS pain. The high rates of retention and compliance with good tolerance to yoga intervention (3.02 ± 0.407) and planned assessment provide evidence that tailored yoga intervention is feasible for acute postoperative care. Yoga may be beneficial in reducing perceived stress, but such efficacy needs to be determined in a future larger pragmatic trial. The findings suggest that a tailored yoga program is feasible and can be delivered per protocol for acute LSS postoperative symptoms. The exploratory clinical outcomes are relevant to postoperative care and can serve main outcomes in subsequent trials. Future confirmatory studies may use these findings to investigate the efficacy of the tailored yoga intervention on common postsurgical symptoms of acute pain, perceived stress, catastrophizing thoughts, opioid consumption, and function/walking distance during the hospital stay.
Our findings are consistent with previous data supporting the feasibility of yoga intervention for hospitalized patients. In this study, patients tolerated about 15 min of yoga without any adverse events. No participants experienced an increase in pain or psychosocial stress or refused to participate. In fact, there was minimum relief in pain from the beginning to the end of the yoga session, indicating an immediate tolerance to yoga intervention. The complexity of the surgical procedure causes severe postoperative pain, and strict postoperative precautions limit the patient's ability to engage in standard rehabilitation. Thus, a modified yoga intervention, that is constructed within the boundaries of surgical precautions and well tolerated by the patients can be a safe adjunct treatment during acute hospital stay. Participant ability to engage deep trunk and pelvic floor muscles with physical movement is important for LSS recovery. Participants tolerated muscle awareness with breathing the best, followed by pelvic floor engagement. Overall, the current results indicate that adaptive yoga practices coordinated with breath could be safely practiced in a bed or chair.
Additionally, the achievement of retention and recruitment rates, participant compliance and adherence (no dropouts due to assessment or yoga intervention burden), participant willingness to be randomized, and participant ability to complete planned assessments within 45 min confirm the operational feasibility and acceptability of the trial. Four participants' unwillingness to complete the baseline assessment may suggest potential minimum burden on participants but other reasons for not completing the baseline assessment cannot be ruled out, as the participants did not provide any reasons.
The exploratory clinical measures further add to the feasibility of the trial and clinical relevance, as none of the measures was negatively impacted by the yoga intervention. Based on published reports, the mind–body components of yoga may be a beneficial approach in reducing acute pain, overall opioid consumption, and emotional and physical symptoms. That the yoga group showed less-perceived stress over the hospitalization possibly is related to the immediate pain reduction postyoga session. The improvement in perceived stress shows minimal clinically important change, 45 however, this finding should be confirmed with a larger pragmatic trial. In a previous study, subjects who underwent yoga relaxation training were less distressed during hospitalization for breast cancer surgery than those who did not. 46 Temporary pain relief and less stress may potentially be related to less opioid use and decreasing the pain catastrophizing thoughts observed. Yoga may help reduce negative thoughts and helplessness associated with coping and managing pain and decrease symptom magnification during acute postsurgical pain management.
The observed changes noted in the yoga group for hospitalization measures (daily pain, opioid use, and gait distance) contribute broadly toward the feasibility of the study and perhaps validate participant-reported and trainer-observed tolerance to yoga intervention. Participants in the yoga group used less opioid (∼30 mg overall) than the participants in the control group (Fig. 6B) from day one to discharge. It is difficult to determine a clinical significance of 30 units of less opioid, but more opioid use is associated with side effects like nausea and vomiting, 47 can impede postoperative recovery, and can have potential long-term consequences. One prior study of hospitalized children with sickle cell vaso-occlusive crisis reported no opioid use difference between yoga versus control groups. 30 Further studies are needed to examine whether yoga's immediate positive impact on acute pain results in less opioid use.
Participants in the yoga group showed greater walking distance (∼100 feet) over the course of their hospital stay than participants in the control group. Increased gait distance is an important measure for safe and timely hospital discharge following LSS 48 and total hip replacement. 7,49 Gait distance reflects improved recovery and quicker return to baseline function. 49 Although walking ability depends on many factors, it is linked to pain intensity and adequate pain management strategies. Relying only on pharmacological interventions/opioids alone is not beneficial in improving patient's function. The study identifies potential clinical measures relevant to post-LSS recovery that can be considered for a future confirmatory trial.
Yoga is a multimodal intervention that includes relaxation, mindfulness, breathing exercises, and muscle activation with physical postures. The combination of these elements may account for less pain, stress, negative thoughts, and opioid use, and improved function, and others. Catastrophizing behavior, high use of opioids, and severe pain are predictors of poor long-term outcomes, and are associated with development of chronic postoperative pain, high reliance on opioids, and poor function/quality of life. 8,9,50 Intervention strategies should be implemented to minimize these effects for both short and long-term outcomes.
Due to the pilot nature of the study, the small sample size is a limitation and as such no inferential tests were used to discern any therapeutic benefits. A larger sample size would have allowed power calculation, which can be addressed in a future confirmatory study. Second, due to the small sample size, safety and tolerability of yoga intervention should be validated in future studies. This feasibility study has provided the tailored yoga intervention and preliminary framework for the incorporation of tailored yoga into the inpatient care for individuals undergoing LSS to allow future studies to investigate its potential health benefits.
Conclusion
A tailored yoga program constructed within postsurgical restrictions is feasible and can be implemented as outlined in future confirmatory studies to explore its impact on surgery-related acute pain, perceived stress, negative thoughts, and opioid use. Our results expand the available evidence supporting the use of yoga for surgical care post-LSS. Yoga is relatively inexpensive, culturally acceptable, require minimum infrastructure, and can potentially improve the physical and psychological wellbeing of individuals with various medical conditions. Surgery and hospitalization can be stressful and painful experiences for patients. Our results support integration of complementary medicine techniques in an inpatient environment where this type of therapy is typically not considered.
Footnotes
Acknowledgments
The authors would like to thank Alyssa Parrish, Katie Mena, Garrett Holle, Chaz Johnson, Anita Jeyakumar, Ashton Lee, Samantha Keeling, Missy Hipp, and Anna Hegarty for data collection and contribution to analysis; Mary Crouch Young and Kelly Colln for their contribution toward yoga intervention (design and delivery); Mary Crouch Young for editing the article; Vann Bradham (5T32HD57850-8) for EMR data extraction; and Lachlan Moore for editing and updating citations.
Authors' Contributions
Dr. N.K.S. acquired funding, conceptualized the study, supervised the study, and wrote and finalized the article; Dr. H.L. assisted with electronic data extraction and performed data analysis; Dr. K.A. assisted with data collection and reviewed and edited article draft; S.R. and E.M. assisted with data collection, contributed to writing the article, and outlined the article; Drs. D.C.B. and P.M.A. assisted with study design, yoga intervention design, data interpretation, and reviewed and edited article draft; Dr. Y.C. co-wrote the grant, conceptualized the study, developed yoga protocol, assisted with supervision and training of research personnel, collected outcomes assessments, assisted with data analysis, and article preparation and revision. All authors read and approved the final article.
Author Disclosure Statement
The authors have no conflicts of interest and nothing to disclose.
Funding Information
This work was funded by Frontiers: Heartland Institute for Clinical & Translational Research (UL1TR002366).