
Abstract
Objectives:
Preventing postpartum depression (PPD) is a public health goal. The scientific literature has demonstrated the short-term efficacy of Mindfulness-Based Interventions (MBIs) delivered during pregnancy on PPD. Nevertheless, the long-term outcomes of MBIs are still unclear.
Design:
Systematic review and meta-analysis of randomized controlled trials (RCTs). Four databases were searched to identify RCTs focused on describing the efficacy of MBIs on PPD and published in English up to February 2022.
Settings/Location:
The study was conducted globally.
Subjects:
Pregnant women who received MBIs.
Interventions:
MBIs were delivered during pregnancy in the included RCTs.
Outcome Measures:
Data collection and analysis effect size were combined using a random-effects model. The reporting in this study was consistent with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
Results:
Six studies were included. The overall effect size significantly reduced PPD symptoms severity in the MBI group versus the control group in the first 3 months after childbirth (standardized mean difference = −0.26; 95% confidence interval = −0.51 to −0.01; I 2 = 30.65%). The effects of MBIs were significant in women who started MBIs with a low risk of developing PPD.
Conclusions:
MBIs delivered during pregnancy have long-term benefits for PPD.
Implications for Practice:
Further studies focused on testing MBIs starting during pregnancy and lasting over the postpartum and modulating the intensity of delivering MBIs based on the risk for developing PPD are needed to inform the practice with solid evidence.
Introduction
Pregnancy and motherhood are periods of profound transformation, involving long-term processes that qualitatively reorganize both internal thoughts and external behaviors. 1 This transition may be fraught with difficulties and stresses, making mothers more vulnerable to mental health problems during the perinatal and postpartum period, defined as the time from the onset of pregnancy up to the end of an infant's first year. 1 –3
The most common mental disease is depression. Approximately 10%–15% of women experience the onset of a major or minor depressive episode during the perinatal period, and nearly a fifth of women experience depression in the first 3 months after giving birth. 1,3 –5 The prevalence of postpartum depression (PPD) is reported to be high, and it varies by country, cultural background, and economic conditions. For instance, the prevalence of PPD in China is the highest (21.4%); this is significantly higher than the prevalence in the United States (8.6%) and Japan (14.0%). 6 The risk factors for PPD mainly involve physical, psychological, and social aspects. 6 More precisely, gestational diabetes mellitus, depression during pregnancy, pregnant women giving birth to boys, epidural anesthesia during delivery, depression during pregnancy, and history of depression were identified as risk factors for PPD. 6
PPD is associated with serious adverse consequences for parents and infants. One significant consequence of undertreated maternal depression is a disrupted relationship with the newborn, which can result in fewer positive feelings toward the infant, less emotional availability, insecure bonding, and adverse neurodevelopmental outcomes in the short and long-term periods. 3,7 Moreover, the babies of depressed mothers exhibit lower social engagement, fewer mature regulatory behaviors and more negative emotionality, and higher cortisol reactivity. 6 In addition to PPD, other postnatal psychological difficulties, called Maternal Mental Health Diseases (MMHD), can occur in mothers, such as stress or anxiety (e.g., about 10% of women experience the acute debilitating condition of Generalized Anxiety Disorder [GAD]). 6 Severe postpartum psychiatric disorders are also associated with high rates of maternal suicide, showing a 70-fold increase in suicide risk in the first postnatal year compared with age-specific rates for the general female population. 3,7
Due to the negative consequences of PPD and MMHD, reducing perinatal psychological distress (e.g., stress, depression, and anxiety) during pregnancy and the first-year postpartum should be a crucial public health goal. 1,6 To prevent depression recurrence/relapse in pregnant women and mothers, a widely used method is pharmacotherapy: current estimates suggest that over 7% of pregnant women overall use antidepressant medication, and at least 75% of women identified as depressed are referred for pharmacotherapy. 4 Nevertheless, in the United Kingdom, the NICE guidelines point out that “there are risks associated with taking psychotropic medication in pregnancy and during breastfeeding” and recommend psychological interventions. 8 In addition, literature shows that many women prefer psychological interventions during the perinatal period, expressing fears about medication harming their developing baby, guilt about taking medication, and concerns about becoming dependent. 3
In this regard, Mindfulness-Based Interventions (MBIs) are a relatively novel psychological method employed to promote emotional positivity and stability in women. 9 Mindfulness has been defined as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment.” 3,9 The process of accepting things as they are and approaching situations with an open mind reduces tension and fear and increases trust. MBIs are verbally guided and invite participants to focus attention with an attitude of curiosity and acceptance on present-moment experiences, such as the breath, body sensations, sounds, and thoughts. 3,9
Short-term effects of MBIs in the perinatal and postpartum period
MBIs are actively studied in clinical trials to assess their efficacy in improving health outcomes during pregnancy, acknowledging their growing popularity in clinical practice. 4,10,11 Some literature reviews and meta-analyses were conducted to assess all trial findings about mindfulness brief-term effects in the perinatal period 3,9 : results suggest that MBIs can be beneficial for outcomes, such as depression, anxiety, perceived stress, and levels of dispositional mindfulness (i.e., individual's trait to be mindful in their everyday life), during the perinatal period.
In addition, short-term results regarding the utilization of mindfulness were observed implementing an intervention in the postpartum period. In Spain, the implementation of an 8-week mindfulness meditation intervention to assess maternal self-efficacy, depression, anxiety, stress, and mindfulness in breastfeeding mothers obtained positive results compared with the control group in samples that were, on average, 10 months postpartum. 2 Another example is offered by a small, nonequivalent control group quasi-experimental study involving postpartum women with a formal diagnosis of depression or GAD: it demonstrated that, in the MBI group, depression and anxiety levels decreased while mindfulness levels increased. 7
Long-term effects of MBIs in pregnancy during the postpartum period and rationale for the current meta-analysis
There is preliminary evidence that implementing mindfulness programs during pregnancy could have lasting effects on PPD. 12 In this regard, Dimidjian et al. demonstrated significantly lower postpartum relapse rates in the MBI group by 6 months postpartum. 4 Pan et al. demonstrated that depression scores (and stress scores) were significantly better in the intervention group than in the comparison group at 3 months postpartum. 1 Nevertheless, Dhillon et al. suggest that further research would be useful to explore if MBI benefits are sustained during the postnatal period. 9
So far, the literature concerning long-term outcomes—defined in this study as periods ranging from 3 to 6 months postpartum, a definition that may encompass what could be considered “medium-term” in other contexts—of implementing MBIs during pregnancy in the postpartum period has not been synthesized quantitatively by pooling the effects from primary studies. The employed definition of long-term effects is empirical and based on the follow-up periods commonly used in primary studies. 12 The absence of quantitative synthesis in this regard hinders the prompt definition of the state of the art concerning the efficacy of MBIs in optimizing outcomes related to mental health over long-term follow-ups. For all these reasons, analyzing the existing literature using quantitative pooling techniques to estimate the overall effect size of MBIs in long-term outcomes with a specific focus on PPD offers an evidence-based foundation for clinical decision making.
Objective
This systematic review and meta-analysis aimed to pool the effects from the available primary studies on the efficacy of MBIs on PPD in long-term periods defined as 3 and 6 months of follow-up in the postpartum period.
Materials and Methods
Study design
This is not a registered systematic review and meta-analysis of randomized controlled trials (RCTs). The review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) recommendations. 13 Guidance set out by the Cochrane Collaboration informed methods for data extraction and synthesis. 14 The review protocol and further data can be accessed by contacting the authors. This study was granted an Institutional Review Board waiver as per local regulations, which do not require approval for systematic reviews.
Review question
This systematic review will address the following research question: “What are the pooled estimates from existing literature examining the association between MBIs during pregnancy and postnatal maternal mental health, particularly postpartum depression?”
Population, intervention, comparison, outcome(s), study design
The defined framework to guide the review and develop the queries for answering the research question was based on the “Patient, Intervention, Comparison, Outcome(s), Study design” (PICOS) framework. The population included pregnant women and mothers; the intervention was based on MBIs; the control was given by any active or nonactive (standard of care) practice; the primary outcome was the PPD, and the secondary outcomes were perceived stress, dispositional mindfulness, positive state of mind (i.e., positive thoughts, emotions, and attitudes toward oneself), and anxiety. As the aim of this systematic review is related to the efficacy of MBIs, the study design for answering the research question was given by RCTs.
Eligibility criteria
The inclusion criteria for eligible studies were as follows: (1) RCTs in which MBIs were proposed during pregnancy, while PPD and postnatal MMHD were the outcomes of interest; (2) peer-reviewed literature published in electronic databases up to February 2022.
The exclusion criteria for eligible studies were as follows: (1) studies not written in English; (2) studies where participants were not human or were not pregnant women; (3) quasi-experimental studies, cohort, case–control, or cross-sectional studies, case reports, case series, letters, commentaries, notes, editorials, and conference abstracts.
In case of missing data, the lead reviewer made every attempt to contact the authors of the studies to account for the missing information. 14 If no response was received from the authors, RCTs for which no quantitative analysis could be conducted due to missing data were excluded from the meta-analysis, but still considered for the qualitative synthesis. 5,15,16
Search strategy and data extraction
A systematic search of the literature was conducted at the end of February 2022 in the following electronic databases: PubMed, CINAHL, Web of Science, and PsycInfo. A detailed search strategy was compiled using keywords and Medical Subject Headings. Booleans and truncation symbols were used to combine the key concepts and index terms, and filters were employed to refine the search results. Supplementary File S1 shows this in more detail. In addition, bibliographies of relevant reviews and included studies were hand-searched for potential articles by two independent reviewers. When any discrepancy arose, a third content expert was consulted, and the issue was discussed until a consensus was reached. 17
According to PRISMA guidelines, two reviewers independently screened each record and extracted data from the eligible studies, including the author and year of publication, study design, sample size, intervention, and findings. 13 A third reviewer solved discrepancies if necessary. Supplementary File S2 presents the PRISMA checklist, outlining the comprehensive reporting standards followed for this article.
Quality appraisal
Two reviewers independently conducted the quality assessment of the included studies using a Cochrane quality assessment tool, that is, the risk of bias 2 (RoB 2) tool, which assessed common features of the six types of bias most often associated with RCTs (randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result, overall bias). 18 Randomization process examines the method used to generate the random allocation sequence, including details about sequence generation and allocation concealment (selection bias). Deviations from intended interventions assess whether there were any significant deviations from the intended intervention protocol and whether there were differences in the care provided between intervention and control groups (performance bias). Missing outcome data evaluate the extent and reasons for missing outcome data, including whether there were dropouts or exclusions and how they were handled in the analysis (attrition bias).
Measurement of the outcome examines the measurement of the outcome of interest, including whether the outcome was measured in a valid and reliable manner and whether the methods of measurement were consistent between groups (detection bias). Selection of the reported result evaluates whether the reported results were selected based on the statistical significance or direction of the findings, rather than being based on a prespecified protocol (reporting bias).
The bias was then classified as low, high, or not reported for each of the six types of bias, and an overall likelihood of bias was measured and reported.
Study selection
Figure 1 illustrates the PRISMA Flow Diagram in the process of identification, screening, eligibility, and inclusion of studies in this research. Sixteen articles were eliminated because the study method did not follow the criteria set for the inclusion (e.g., they were RCT protocols), while 8 studies were not focused on describing the efficacy of MBIs in mitigating or preventing PPD or the secondary outcomes. Another seven articles were excluded in the eligibility phase after reading the full texts, as they did not respond to the research question, and specifically, the outcomes were investigated during pregnancy and not after childbirth. A total of nine RCTs were included in the qualitative summary, six of which contributed to the quantitative analyses of the primary outcome (PPD) and/or secondary outcomes (stress, dispositional mindfulness, positive state of mind, and anxiety). 1,4,5,10,15,16,19 –21
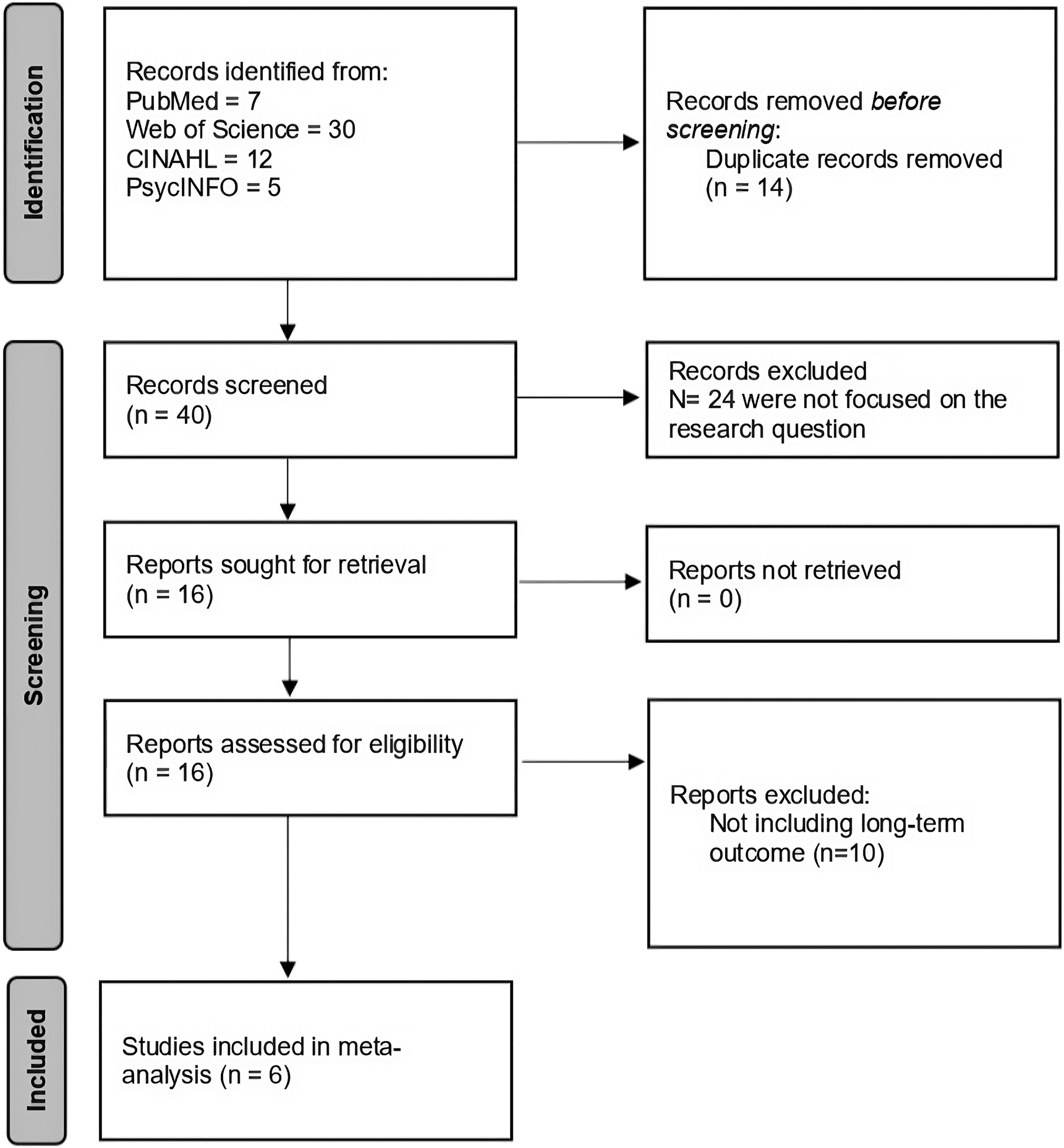
Flow diagram.
Data synthesis
Meta-analyses were performed to calculate overall pooled estimates of the relationship between MBIs in pregnancy with PPD and MMHD (when secondary outcomes were assessed in the primary studies). Every included RCT defined the severity of the considered outcome through a validated self-report scale (e.g., the Edinburgh Postpartum Depression Scale [EPDS] or the Center for Epidemiologic Studies Depression [CES-D] Scale for PPD), and these data were employed for the quantitative analyses. The standardized mean difference (SMD) was chosen as the measure of synthesis to calculate the effect size in two different groups (MBI group and control group) because the scales assessing the outcomes were not the same measures. In this regard, the SMD directly accounts for the measure's variance in the effect size rather than the analytical weights, managing the underlying different assessing tools for the outcome. Stata 17 (StataCorp, 2021) was used to perform analytics.
The framework of random-effects modeling 17 was used to perform the quantitative pooling because it was plausible to account for true differences in the effects between MBIs and outcomes in the primary studies. Therefore, random-effects models allow authors to manage the heterogeneity from one study to another in terms of the type of employed MBIs and population.
The Forest Plots were used to depict the meta-analytical models. Each effect size was reported with its confidence interval (95%CI) and its statistical significance (p-values). The I-squared statistics described statistical heterogeneity (I 2 ), 14 representing the percentage of the study's total variation due to heterogeneity rather than chance. An I 2 value of <35% indicates a low degree of heterogeneity, 36%–75% indicates moderate heterogeneity and greater than 75% means high heterogeneity. 14 To examine the robustness of our findings and assess the influence of individual studies on the overall effect size, we conducted a sensitivity analysis. This was achieved by performing a leave-one-out analysis, in which the meta-analysis was rerun multiple times, each time excluding one study. This iterative process allowed us to identify any particular study that could potentially have a disproportionate impact on the pooled effect size. The process facilitated the evaluation of the stability of our results and confirmed the reliability of our meta-analysis findings.
Subgroup analyses were employed to explain heterogeneity accounting for categorical variables in relation to the population (i.e., high-risk of PPD vs. low-risk of PPD). Considering the potential variability in the characteristics of the MBIs, such as their duration, we sought to control for this variability by incorporating the duration in weeks of the MBIs as a moderator in a meta-regression model. This approach allowed us to investigate whether the duration of MBIs has an influence on the severity of PPD symptoms, thereby providing insights into the potential role of intervention length in determining outcomes.
Results
Characteristics of the included studies and nonstatistical heterogeneity
The characteristics of each included study in this systematic review were reported in a Synoptic Table (Table 1). The assessed items for summarizing the included articles included aim, methodology (number of included mothers, kinds of proposed intervention and comparison, outcome measures, and postassessment time), and results.
Characteristics and Results of the Included Studies
CBSEI, Childbirth Self-Efficacy Inventory; CES-D, Center for Epidemiological Studies-Depression; EPDS, Edinburgh Postpartum Depression Scale; FFMQ, Five Facets Mindfulness Questionnaire for mindfulness; GAD-7, General Anxiety Disorder-7; LIFE, Longitudinal Interval Follow-up Evaluation; MAAS, Mindful Attention Awareness Scale; MAIA, Multidimensional Assessment of Interoceptive Awareness; MBCP, Mindfulness-Based Childbirth and Parenting; MBCT, Mindfulness Behavioral Cognitive Therapy; MBCT-PD, mindfulness behavioural cognitive therapy for perinatal depression; MBSP, Mindful-based Self-Compassion Program; MIL, Mind in Labor; NA, negative affectivity; PA, positive affectivity; PCS, Pain Catastrophizing Scale; PM, prospective memory; PRA, pregnancy-related anxiety; PSI, Parenting Stress Index; PSOM, positive states of mind; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; RCTs, randomized controlled trials; RM, retrospective memory; SCS, self-compassion scale; STAIT, State-Trait Anxiety Inventory-Trait; TAU, treatment as usual; VAS, Visual Analog Scale; W-DEQ, Wijma Delivery Expectancy/Experience Questionnaire; WHO-5, Five Well-Being Index.
The included studies varied in their aims, methodologies, and results. The studies primarily focused on evaluating the efficacy of MBIs during pregnancy and postpartum on various psychological outcomes, such as stress, depression, anxiety, and mindfulness. The studied populations were primarily pregnant women at different stages of pregnancy. The included studies focused on women with a history of depression, 1 first-time expectant mothers, 4 women experiencing high levels of psychological distress, 5 women in the second or third trimester with antenatal psychiatric disorders or depressive/anxiety symptoms, 19,20 and women who self-identified as experiencing high levels of psychological distress. 21 The control groups in these studies typically received treatment as usual (TAU) or standard childbirth education without mindfulness. 1,4,5,19 –21 The outcome measures used in these studies included various scales to assess stress, depression, anxiety, mindfulness, self-compassion, and other psychological and behavioral outcomes. 1,4,5,15,16,19 –21
The interventions included mindfulness behavioural cognitive therapy (MBCT) for perinatal depression, 4,15,20,21 mindfulness-based childbirth and parenting (MBCP) program, 1,16,21 mind in labor program, 16,19 and other mindfulness training programs delivered through different formats such as group sessions, 5,10 weekend workshops, 5,10 and online courses. 19 Concerning the intervention, the studies varied in terms of the types and duration of MBIs provided, ranging from an 8-week MBCT for perinatal depression, 4,15 a short, time-intensive 2.5-day mindfulness-based childbirth preparation course, 19 a 10-h training Mindful-based Self-Compassion Program (MBSP) program, an 8-week online mindfulness course, 20 an 8-week group-based MBCP, 1,21 and a modified 8-week MBCT. 15 The control groups in these studies typically received TAU 4,15,19,20 or standard childbirth education without mindfulness. 19 The outcome measures used in these studies included various scales to assess stress, 1,4,10,15,16,19 –22 depression, 1,4,10,15,16,19 –22 anxiety, 4,10,15,16,19,20 self-compassion, 10,20 and other psychological and behavioral outcomes. 1,4,5,10,15,16,19 –22 The postassessment times ranged from 3 months postpartum 4,5,10,19 –22 to up to 1-year postpartum. 15,16,21
Several studies reported improvements in stress, depression, and mindfulness scores in the intervention groups compared with the control groups. 1,4,10,15,16,19 –22 However, the extent of these improvements and the duration of their effects varied across studies. 4,5,10,15,16,19 –22 Three studies reported sustained improvements in psychological outcomes over time, 15,16,21 while one found that the initial effects of the interventions were not maintained during the follow-up period. 21 High dropout rates were also observed in two studies, 4,5 indicating potential issues with the acceptability or feasibility of the interventions.
Risk of bias between the studies
A Risk of Bias assessment was performed for each study included in the qualitative summary (Fig. 2). A Risk of Bias Graph 13,17 was developed to summarize the assessment. The biases most frequently encountered were the “Blinding of participants and personnel” and the “Incomplete outcome data”. These biases were found in >50% of the included articles, likely due to the need to organize different activities for the intervention and control groups, and the high number of mothers lost to follow-up as the surveys were conducted in the long-term period. Three of the RCTs included in our meta-analysis had participant samples that were predominantly Caucasian, well educated, and employed. 4,16,21 While these studies provided valuable insights, their findings may not be fully generalizable to broader populations. This is because the characteristics of the study participants may not accurately reflect the diversity of the general population in terms of race, education level, and employment status. Therefore, while interpreting the results of our meta-analysis, it is important to consider these potential limitations in the applicability of the findings to other demographic groups.
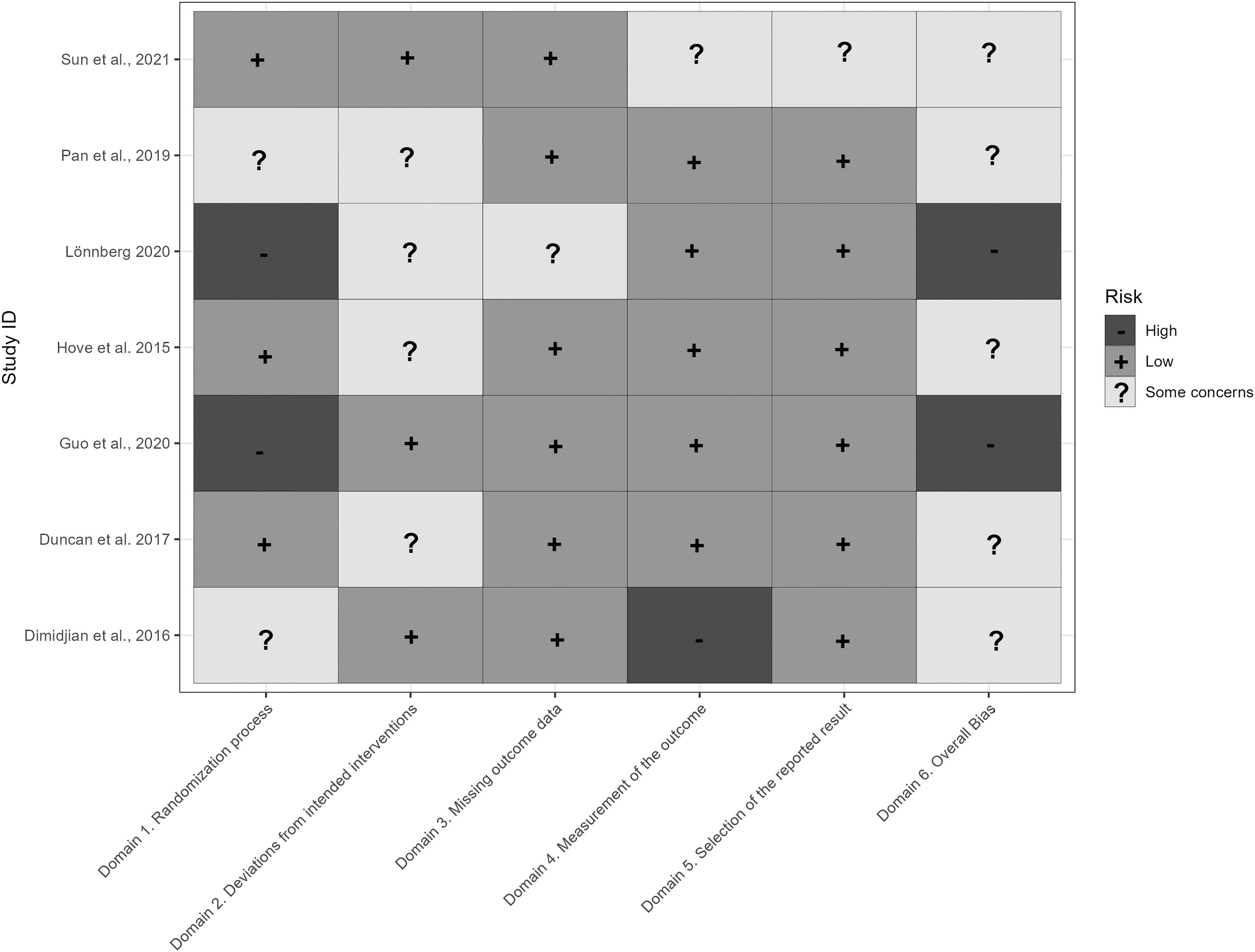
Risk of Bias (Rob 2) Summary.
Quantitative synthesis of the results
The Forest Plot in Figure 3 demonstrates the effects of MBIs on PPD within 3 months postpartum (SMD = −0.26; 95% CI = −0.51 to −0.01; I 2 = 30.65%). Specifically, Dimidjian studied this outcome 1 month after delivery (through EPDS), 4 whereas Duncan at 6 weeks (with CES-D). 19 Lönnberg (at 3 months postpartum), 21 Pan (at 3 months postpartum), 1 and Sun (at 6 weeks postpartum) 10 used EPDS.
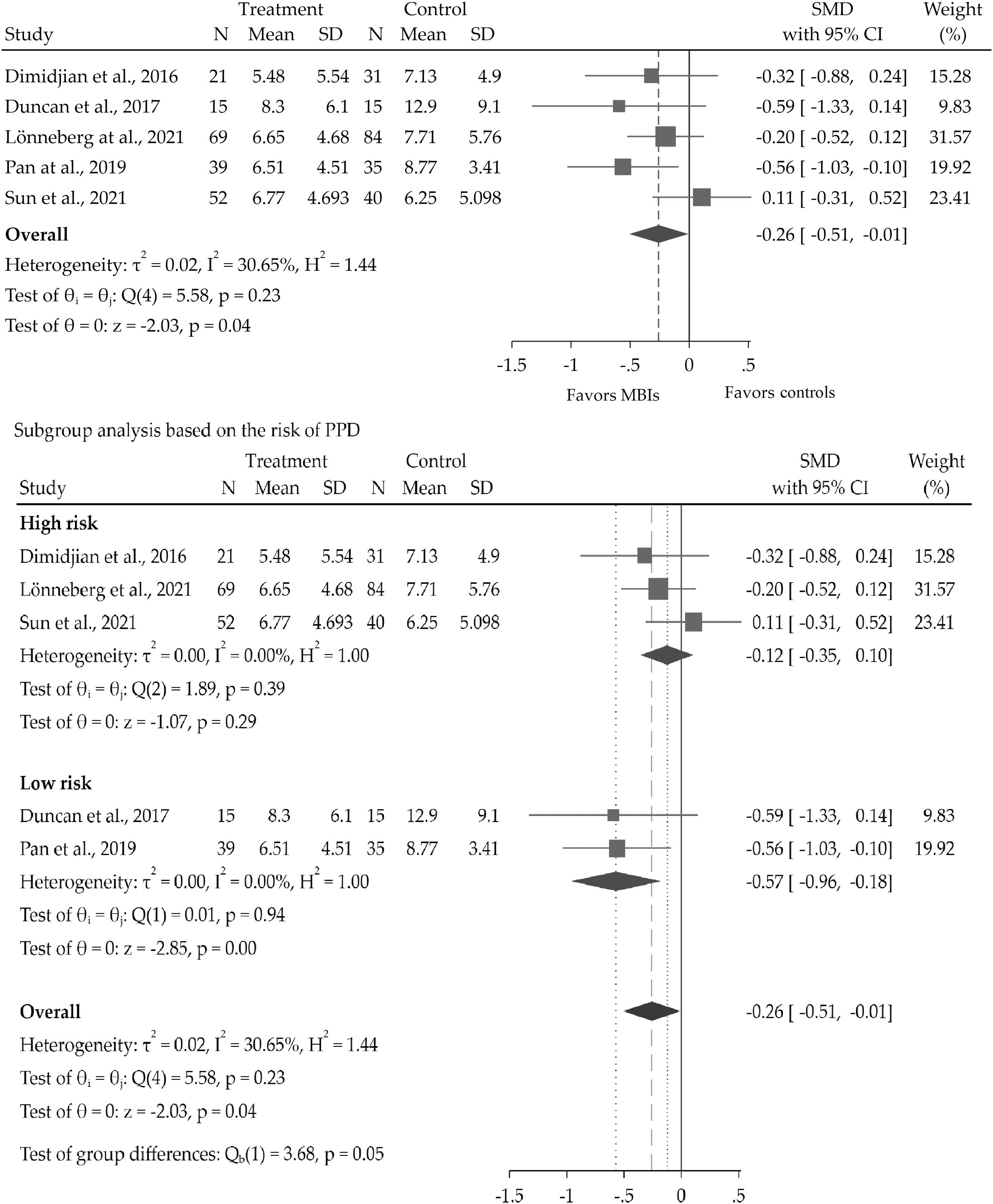
PPD severity after 3 months postpartum. CI, confidence interval; PPD, postpartum depression; SD, standard deviation; SMD, standardized mean difference.
An included study, the sixth included RCT, 20 was not added to the meta-analysis because the presence of missing data referred to the outcome did not make it possible to extract data for the overall model. Considering the individual study level, it is possible to summarize the contribution of each RCT on PPD. Dimidjian et al., 4 Duncan et al., 19 and Lönnberg et al. 21 reported a statistically not significant trend in favor of the intervention group (postpartum depressive symptoms were more severe in the control group even if it did not show significant associations with the experimental arm); Pan et al. indicated a significant effect in favor of the intervention group (postpartum depressive symptoms were worse in the control group and the CI did not intersect the nonsignificance line) 1 ; Sun et al. found a not significant effect in favor of the control group (postpartum depressive symptoms were worse in the intervention group, but the CI intersected the nonsignificance line). 10
Overall, effect size (SMD = −0.26, 95% CI = −0.51 to −0.01; I 2 = 25%) showed a significant reduction of PPD symptom severity in the MBI group versus the control group in the first 3 months after childbirth. The analysis revealed a nonsignificant trend toward reduced severity of depressive symptoms between 6 and 12 months postpartum in the MBI group. The findings of the sensitivity analysis confirmed the robustness of these primary results, demonstrating that no single study disproportionately influenced the pooled effect size.
The subgroup analysis with respect to the type of population (high risk of PPD vs. low risk of PPD) showed that: (1) in the case of low risk of PPD, depressive symptoms severity was significantly worse in the control group (SMD = −0.57, 95% CI = −0.96 to −0.18; I 2 = 0%); (2) in case of high risk of PPD, depressive symptom severity did not differ in the two groups (SMD = −0.12, 95% CI = −0.35 to 0.10; I 2 = 0%) (Fig. 3). A random-effects meta-regression analysis was performed to assess the impact of the duration of MBIs on PPD severity. However, the duration of MBIs did not significantly influence the severity of PPD symptoms (coefficient = 0.0237, p = 0.525). This suggests that the length of the intervention did not have a statistically significant effect on the outcome. In terms of residual heterogeneity, the I 2 statistic was 42.37%, suggesting moderate heterogeneity. The test for residual homogeneity (Q_res = χ 2 (3) = 5.08) yielded a p-value of 0.1663, indicating that the observed variation in effect sizes is not significantly greater than what would be expected by chance alone.
The secondary outcomes (i.e., stress, dispositional mindfulness, anxiety, and positive state of mind, which were the MMHD reported in the included studies) were analyzed at 3 months postpartum (Fig. 4). MBIs were found to significantly reduce perceived stress (SMD = −0.23, 95% CI = −0.41 to −0.05; I 2 = 17.33%). Results showed that MBIs were not significantly associated with dispositional mindfulness, anxiety, and a positive state of mind.
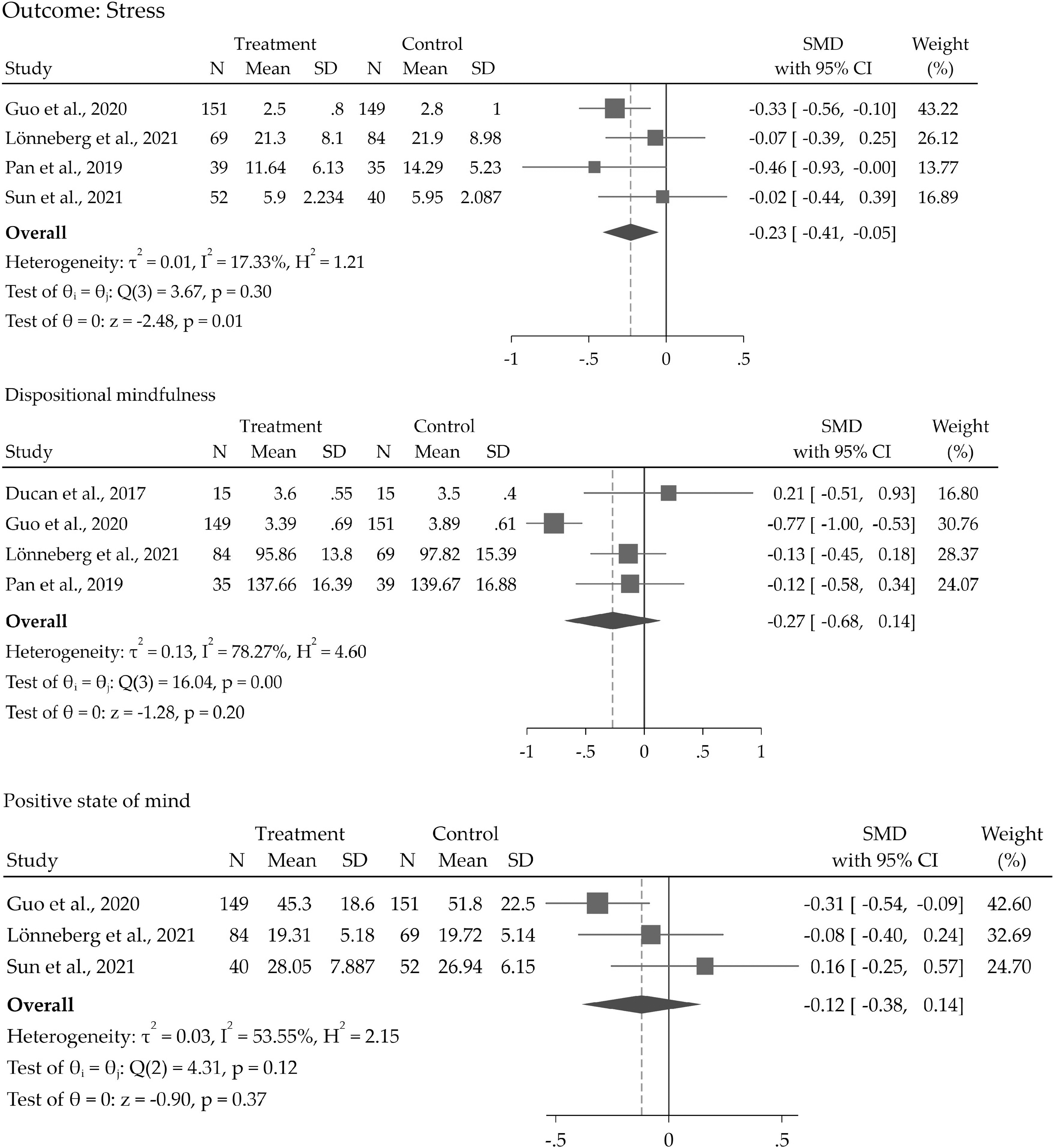
Forest plots of stress, dispositional mindfulness, and positive state of mind. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
Discussion
The increasing recognition of PPD and MMHD as significant clinical issues underscores the urgency of identifying effective interventions. 8 The high prevalence of PPD and MMHD has critical implications not only for the mother's health but also for mother–infant bonding and long-term child development. This systematic review and meta-analysis aimed to determine the long-term (postpartum) effects of MBIs administered during pregnancy on PPD and MMHD. In this regard, the purpose of this study was relevant for framing up-to-date knowledge in relation to the efficacy of MBIs on PPD and MMHD, closing a current gap in knowledge. 3,20 The clinical and epidemiological significance of PPD and MMHD is relevant, given the high number of women who experience difficulty coping with this major life transition. 3,20
In the context of PPD, our study reveals that MBIs introduced during pregnancy significantly mitigate the severity of depressive symptoms within 3 months after childbirth. However, the effectiveness of such interventions initiated during pregnancy tends to diminish by 6 months postpartum considering the current available literature. This finding highlights a crucial clinical consideration: the timing and continuity of MBIs. Given this diminishing efficacy, there is a pressing need for RCTs that not only incorporate MBIs during pregnancy but also continue these interventions in the early postpartum period, perhaps even extending into the second month of motherhood. Such an approach could help sustain the therapeutic effects of MBIs and mitigate or prevent PPD over the longer term. These results underscore the importance of strategic planning in clinical practice to maximize the longevity of MBIs' benefits. Future RCTs can help inform clinicians on how to best design and implement MBIs, ensuring a long-lasting impact on maternal mental health.
A previous meta-analysis conducted by Dhillon et al. investigated the effects of MBIs on perinatal depression, demonstrating the concrete short-term benefits of mindfulness training. 9 Compared with this evidence, the current systematic review demonstrated that MBIs performed during pregnancy have positive effects on PPD even after childbirth (3 months later), which was the main time point used in the previous meta-analysis. 9 However, the effects of MBIs delivered during pregnancy are not significant over 6 months of follow-up in the postpartum. This result is consistent with a previous study 10 where data collection and outcomes assessment took place over four time points in the follow-up period.
Beyond PPD, this meta-analysis demonstrated that MBIs show long-term effects on perceived stress. This result is in line with some evidence showing that MBIs can improve physiological stress reactivity (including blood pressure and heart rate variability, as well as reduce cortisol levels and adrenocorticotropic hormone reactivity), 15 with the novelty that these conditions could be maintained over 3 months in the postpartum. However, the currently available primary studies did not support the significant effects of MBIs on other MMHD (secondary outcomes), even if two previous meta-analyses had demonstrated that MBIs might have a positive short-term effect on these outcomes. 3,9
The present systematic review paves the way for deepening the research in the postpartum period in terms of highlighting the need for further empirical studies focused on the postpartum period and new schemes for implementing MBIs with the purpose of having long-term effects. For example, it would be worth exploring if a precise scheme for delivering MBIs, including pregnancy and the early postpartum period, might have long-term efficacy in relation to PPD and MMHD. 22 In fact, one possible explanation for the nonsignificance of the MBI's positive effects on postnatal outcomes could be that participants did not engage in sufficient skills for self-performing mindfulness practice over time. 3,22
Finally, only one of the studies included in the meta-analysis 10 focused on anxiety within 6 weeks after childbirth. The reported result in the primary study did not show a favorable effect of MBIs on PPD. This outcome confirms the result obtained in the postnatal period by an uncontrolled, nonrandomized pilot study. 22 Nevertheless, future well-conducted research with larger samples is needed to better investigate anxiety symptoms during the puerperium, and multicenter RCTs could be useful to obtain generalizable findings.
Our subgroup analysis elucidates the differential effectiveness of MBIs based on the risk level for PPD. Interestingly, MBIs seem to confer more pronounced benefits at the 3-month postpartum follow-up for mothers with a low risk of PPD. Contrastingly, mothers with a higher risk of PPD might necessitate additional mindfulness booster sessions, suggesting the need for a more tailored, intensity-based approach in delivering MBIs based on the individual risk profiles for PPD. 15 In light of these findings, it becomes imperative to adopt screening strategies during pregnancy to identify mothers with a higher predisposition toward PPD, as advocated by Liu et al. 6 This strategic identification would allow for the personalized implementation of MBIs, not only during pregnancy but also extending into the postpartum period. Moreover, for those identified as high risk, opting for specialized interventions such as Mindfulness Behavioural Cognitive Therapy for Perinatal Depression (MBCT-PD) or MBSP could potentially offer more targeted therapeutic benefits. 15,20
The decision to persist with MBIs even after childbirth is based on the aspiration that these mothers could continue reaping the short-term benefits of these interventions, well established in existing literature, into the long term during their motherhood journey. However, this assertion warrants further empirical validation. Therefore, our study emphasizes the value of personalized, risk-based, and longitudinally extended MBIs in enhancing their therapeutic potential, which could guide future clinical strategies in managing PPD. 2,3,7
In assessing the influence of the duration of MBIs on their impact on PPD, the performed meta-regression analysis provides a valuable contribution to our understanding of how MBIs could be optimized in a clinical setting. The results, however, reveal a nonsignificant relationship between the duration of MBIs, as measured in weeks, and their effect sizes. This suggests that extending the duration of the MBIs may not necessarily result in a proportional increase in their effectiveness, contrary to what one might expect intuitively. The implication of this finding is twofold. On one hand, it reassures clinicians that short-term MBIs can still deliver significant benefits, which could have considerable utility in settings where long-term interventions are impractical due to factors such as resource constraints or patient availability. On the other hand, it emphasizes the need to explore other dimensions of MBIs that could be modified to enhance their efficacy, such as the intensity or the specific content of the intervention. The heterogeneity across studies was moderate (I 2 = 42.37%), suggesting a reasonable level of consistency in the results of the different studies included in this analysis.
This increases our confidence in the reliability of the nonsignificant relationship identified in this meta-regression. However, the need for further research to confirm these findings and to identify other possible factors influencing the effectiveness of MBIs remains. The lack of a significant R 2 value, indicating that the duration of interventions does not explain the variability in effect sizes, underscores the potential complexity of the factors influencing the outcomes of MBIs. Future research should delve deeper into understanding the role of various characteristics of the MBIs, such as their specific components, the way they are delivered, and the individual characteristics of the patients, in determining their effectiveness. Lastly, the practical application of these findings suggests the need for flexibility in designing and implementing MBIs in clinical settings. Given that the duration does not appear to have a significant impact, the focus might better be placed on tailoring the intervention to the individual needs and circumstances of the patient. This might include considerations of the risk profile for PPD, the patient's preferences, and the availability of resources for implementation.
Moreover, these results also underscore the importance of maintaining a commitment to evidence-based practice, as the quest for optimizing the use of MBIs in the management of PPD and MMHD continues.
Limitations
The main strength of this study is that it is the first meta-analysis to investigate the long-term effects (3 and 6 months in the postpartum) of MBIs delivered during pregnancy. However, there are several limitations to be acknowledged and discussed.
One notable limitation is the heterogeneity among the included studies in terms of the specific MBIs used and the exact composition of the study cohorts in terms of populations. However, all included studies did employ interventions that were based on the principles of mindfulness, which provides some level of commonality. Furthermore, although there was variation in how outcomes were measured across the studies, all focused on the common outcome of PPD and employed the standardized mean effect helped to manage these aspects. Some weaknesses resulting from bias attributable to the individual studies in the systematic review might be reflected in the effect size of the meta-analysis. These limitations are compounded by potential biases attributable to the individual studies included in the systematic review, which might be reflected in the effect size of the meta-analysis. Furthermore, the included RCTs differed in terms of the type of the delivered mindfulness intervention, activities planned for the control group, and the tool for detecting the results, suggesting caution in interpreting the overall estimate of the effect size. 23
The narrow selection of the primary studies (only RCTs) is another limitation, as information derived from quasi-experimental and cohort studies was not synthesized in this systematic review. An additional limitation is that the protocol for this meta-analysis was not registered in a database such as PROSPERO. Initially, this work began as an educational project and exploratory research, and the decision to conduct a formal meta-analysis evolved later in the process. Finally, as few primary studies were included, the publication bias was not assessed by using the Funnel plot investigation or Egger's regression test because the paucity of few studies may reflect per se a publication bias, and performing statistical tests may be misleading for the limited available power. 24
Conclusions
This systematic review and meta-analysis of RCTs demonstrate the efficacy of MBIs administered during pregnancy for achieving long-term outcomes, which were defined in this study as periods ranging from 3 to 6 months postpartum. The benefits were observed up to 3 months postpartum for both PPD and perceived stress, predominantly among mothers identified as low-risk for developing PPD. We encourage continued research into the long-term effects of MBIs during the postpartum period, to inform the most effective protocols for clinical practice. Critical to this future research is the consideration of the timing and intensity of MBIs, which should take into account the screening for risk factors of PPD. Such adaptive approaches may provide better outcomes, tailoring treatment to the individual needs and risk profiles of the patients. Moreover, further investigation is necessary to examine the potential impact of MBIs on other MMHD.
The current literature in this area remains limited, with a small number of studies not specifically designed to discern the effects of MBIs on aspects of MMHD, such as anxiety, dispositional mindfulness, and positive maternal mental states. Through such investigations, we can refine our understanding of the breadth of influence of MBIs on maternal mental health and optimize their implementation for more comprehensive care.
Footnotes
Authors' Contributions
Each author has made substantial contributions to the work (in the conception and design of the study, in the acquisition, analysis and interpretation of data, or in writing the article). All the reviewers substantively revised the work and approved the final article. We further confirm that the order of authors listed in the article has been approved by all of us.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary File S1
Supplementary File S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.