
Abstract
This study reports on 54 homeless and 53 stably housed veterans who received battlefield acupuncture (BFA) between September 2018 and October 2022. Linear mixed-effects regressions were used to examine change in overall pain score and how pain impacted four areas: (1) activity, (2) sleep, (3) mood, and (4) stress over the course of 8 weeks from the baseline visit at one BFA clinic. Results indicated significant reductions in the impact of pain on activity, sleep, and stress among both homeless and housed veterans. Although overall pain levels were not significantly impacted, further research on the impact of BFA on homeless populations is warranted.
Introduction
Chronic pain is common among U.S. military veterans, where up to 65% of veterans reported pain in the previous 3 months. 1 Pain symptoms among veterans are associated with increased psychiatric diagnoses, including depression and post-traumatic stress disorder, and poor psychosocial outcomes, including worse sleep and lower resilience. 2 Chronic pain is particularly prevalent in homeless populations, 3 and use of both prescribed and nonprescribed pain medications is common among homeless veterans. 4,5 These factors are all associated with an increased risk of opioid misuse, 6 which is, in turn, associated with poor quality of life and higher health care utilization. 7
Use of complementary and integrative health (CIH) therapies is increasing for the treatment of chronic pain. The U.S. Department of Veterans Affairs (VA) now includes the incorporation of nonpharmacologic therapies into pain management plans. 8 One CIH modality that has gained traction within the VA is battlefield acupuncture (BFA). 9 BFA is considered a safe treatment and studies have shown improvement in pain scores in a large national sample of veterans. 9,10
However, to date, studies that examine the impact of BFA on veterans experiencing housing instability have not been located. The aim of this project was to better understand the changes in pain outcomes reported by homeless and housed veterans during their participation in a BFA clinic. The main outcome was change in overall pain scores and secondary outcomes were changes in how pain specifically impacted activity, sleep, mood, and stress.
Methods
BFA protocol
BFA was developed by Dr. Richard Niemtzow. 11 The protocol used in this project was a modified BFA protocol utilized by VA practitioners, 9 which consisted of inserting up to five Sedatalec ASP Gold needles into each ear. First, three needles were inserted into points (1) Cingulate Gyrus, (2) Thalamus, and (3) Omega 2 (see Supplementary Fig. S1 BFA points). The veterans were instructed to walk for 5 min, and pain was reassessed. If pain decreased by <3 points, an additional two needles would be placed (4. Point Zero, 5. Shen Mein). 9,12
The needles remained in the ear until they fell out on their own. BFA was performed by a family nurse practitioner who was trained and credentialed by the VA in BFA. BFA clinic participants were 107 veterans with a history of chronic pain from one VA medical center who attended a weekly BFA pain clinic between September 2018 and November 2022. This was a quality improvement project deemed exempt by the institutional review board.
Measures
Housing status was dichotomized as stably housed (i.e., had a stable, full-time residence) or unstably housed (i.e., using any VA homeless services). Participants self-completed a questionnaire at the beginning of the visit before the BFA procedure started, which included rating their pain on a scale of 0–10 where 0 is “no pain” and 10 is “pain as bad as you can imagine.” In addition, participants were asked to rate their pain's impact over the past 24 h on four parameters: sleep, mood, stress level, and activity.
They rated each of these items in the same way utilizing the scale from 0 to 10. In addition, participants were asked to rate their pain again after five BFA needles were inserted (see Supplementary Data BFA questionnaire). Demographic information and medical history were not collected during the visit and, therefore, were unavailable for analysis.
Analysis
Visit characteristics and the outcomes at baseline were analyzed using descriptive statistics. t-Tests were used to compare baseline characteristics between stably housed and unstably housed participants. Five outcomes were examined using linear mixed effects regression: overall pain level at beginning of each visit, effect of pain on sleep, effect of pain on activity, effect of pain on mood, and effect of pain on stress. The change in outcomes over 8 weeks from the baseline visit was examined. A timeline of 8 weeks was selected because 92% (47/51) of follow up visits (i.e., visits after baseline) occurred within an 8 week time frame of the baseline visit.
Therefore, 8 weeks provided a reasonable timeframe to examine change in outcomes. Housing status and weeks from baseline were included as fixed effects and participants were included as random effects in the model. A post hoc interaction model for the overall pain score was examined to detect whether pain varied by housing status and the likelihood ratio test was used to determine whether the interaction model was a better fit.
Results
Sample description
Between September 2018 and October 2022, 107 veterans (54 homeless and 53 stably housed veterans) attended the clinic. The participants averaged 2.1 (±2.5, range 1–9) visits within 8 weeks of their baseline visit, and the average number of days between visits was 11 (±8 days). There was no significant difference between the homeless and housed participants in the number of visits (p = 0.65). In addition, participants averaged a 2.2 (±1.9) point decrease in their reported pain during their visit between the pre- and post-BFA pain assessments, and the decrease in reported pain did not differ between stably housed and homeless veterans (p = 0.3). Figure 1 depicts the means of the reported outcomes of overall pain and the effect of pain on activity, sleep, mood, and stress over the 8-week timeframe examined.
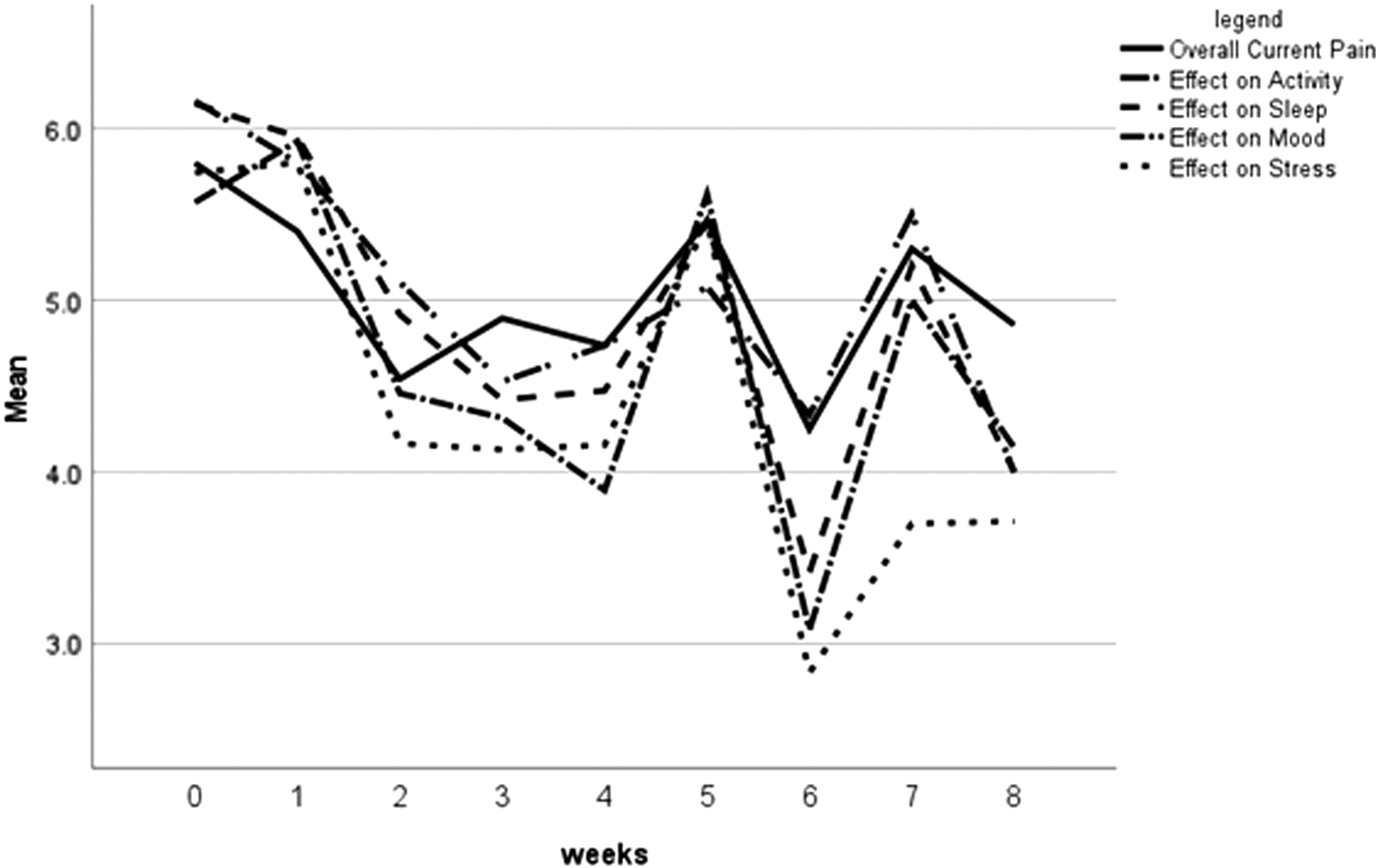
The means of reported outcomes for overall pain, effect of pain on activity, effect of pain on sleep, effect of pain on mood, and effect of pain on stress over 8-week timeframe.
Baseline visit
Table 1 describes the five outcomes as reported at the baseline visit. Overall, participants reported a mean pain score of 5.68 (±2.11). Overall pain was the only outcome assessed that had a significant difference between stably housed and homeless veterans at baseline (5.23 vs. 6.10, p = 0.03). The reported effect of pain on activity, sleep, mood, and stress was not different between the stably housed and homeless veterans.
Description of the Five Outcomes at Baseline Visit with Comparison Between Stably Housed and Homeless Veterans
Bold values indicate a p value < .05.
M, mean; SD, standard deviation.
Linear mixed effects regressions
The linear mixed effects regressions (Table 2), which examined the change in pain outcomes over time, found that the outcomes of overall pain score and the effect of pain on their mood did not change in the 8-week time period. However, a significant decrease in three outcomes over the 8-week timeframe was detected: (1) the impact of pain on activity (β = −0.14, p = 0.01), (2) the impact of pain on sleep (β = −0.15, p = 0.003), and (3) the impact of pain on stress (β = −0.25, p < 0.001). Housing status was not a significant factor in any of the five models.
Linear Mixed Regression Results Over 8-Week Time Period from Baseline Visit
Bold values indicate a p value < .05.
p < 0.05, ** p < 0.01, *** p < 0.001.
A post hoc interaction model was explored to examine overall pain scores over time between homeless and housed participants, which did not yield a significant interaction (likelihood ratio of p = 0.9), therefore, the interaction term to present the most parsimonious model was not included.
Discussion
Although change in overall pain levels was not significantly different between stably and unstably housed veterans after BFA over 8 weeks, both groups reported significant reductions in impacts of pain on activity, sleep, and stress. These findings extend those of a previous study that reported a decrease in pain immediately post-treatment with BFA, 10 but did not have longitudinal follow-up data and did not examine the impact of pain on other outcomes. This project adds to the body of research by demonstrating an association between BFA and a decrease in the reported impact of pain on activity, sleep, and stress over time.
There was no difference in the number of visits or in pain outcomes between the homeless and stably housed participants, suggesting that BFA is an acceptable CIH modality to offer veterans experiencing homelessness or housing instability. Participants of BFA have also shown increased likelihood of later participating in traditional acupuncture. 13 Future research could examine whether this holds true for veterans experiencing homelessness and housing instability and look at the likelihood of using other CIH modalities offered through the VA, such as yoga or chiropractic care.
This project does have some limitations. First, demographic information such as age, gender, race, and military service, and medical history such as type of chronic pain or complicating factors such as substance use were not available; therefore, these variables in the multivariate analyses were not able to be controlled. Second, because this is a quality improvement project, the authors did not have a control or placebo group, so they were not able to determine the effectiveness of BFA on the pain outcomes that were examined.
Third, participants were only from one BFA clinic, which limits generalizability. Finally, the number of visits and amount of time between visits were not consistent between participants. It is possible that participants who went longer between BFA treatments may have had less of a positive impact on their pain than participants who attended the BFA clinic regularly. Future research should explore the effects of BFA on participants with a more consistent visit schedule.
Previous research has shown BFA to be a safe and promising CIH modality to improve pain. 9 The analysis demonstrated this holds true for veterans experiencing homelessness, where the utilization and impact on pain outcomes did not differ for homeless and unstably housed participants when compared with participants with stable housing. In addition, the results revealed a decrease over time in the impact of pain on three quality-of-life indicators of activity, sleep, and stress. Additional research examining longer time periods and more consistent BFA treatments among homeless and unstably housed veterans is warranted.
Footnotes
Acknowledgments
This project was supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Health Services Research, the Center for Healthcare Organization and Implementation Research (CHOIR), Bedford VA Healthcare System, and the National Center on Homelessness Among Veterans.
Authors' Contributions
K.F. contributed to writing—original draft, methodology, and formal analysis. C.S.P. was involved in conceptualization, investigation, and writing—review and editing. A.H. carried out data curation, project administration, and writing—review and editing. J.T. was in charge of conceptualization, methodology, supervision, funding acquisition, writing—original draft and review and editing.
Author Disclosure Statement
The authors report that there are no competing interests to declare.
Funding Information
This project was funded with internal funds by the VA National Center on Homelessness Among Veterans.
Supplementary Material
Supplementary Data
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.