
Abstract
Background:
Qigong exercise training has been suggested to elicit beneficial effects on physical functioning, reduction of oxidative stress, and improved antioxidant capacity in women. However, regular exercise training may support the development of antioxidant defense mechanisms and beneficially modulate oxidant/antioxidant responses.
Objective:
To evaluate the effects of an 8-week qigong exercise training on exercise performance and oxidative stress responses in sedentary middle-aged and elderly women suffering from type 2 diabetic mellitus (T2DM).
Method/design:
Quasi-experimental design, placebo-controlled study.
Setting:
The Department of Physical Therapy, Faculty of Allied Health Science, Burapha University, Thailand.
Participants:
Thirty-six sedentary middle-aged and elderly women with T2DM.
Intervention:
Participants were allocated to qigong exercise (n = 20) or to the control group (CG, n = 20).
Primary outcome measures:
Muscle strengths, flexibility, VO2 max predicted, and walking intensity derived from the 6-minute walk test.
Secondary outcome measures:
Fasting plasma glucose, antioxidant/oxidant stress parameters, and body composition.
Results:
Leg strength and trunk flexibility were improved after qigong training and changes were significantly different compared with the CG (all p < 0.05). VO2 max predicted, 6-min walking distance, and walking intensity were all increased (p < 0.05), and oxidative stress markers were diminished after qigong training (p < 0.05). The antioxidant/oxidant balance was improved after qigong training (p < 0.05).
Conclusion:
The presented findings indicate that 8 weeks of qigong training significantly improved leg strength and trunk flexibility in middle-aged and elderly women with T2DM, partly associated with a more favorable antioxidant/oxidant balance. These effects may beneficially impact on health in this specific population.
Clinical Trial Number: TCTR20221003001.
Introduction
Type 2
Underlying mechanisms relate to oxidative stress in diabetic people accompanied with glycoxidation, formation of advanced glycation products, activation of polyol pathway, etc. 6 –8 Moreover, highly oxidized low-density lipoproteins and sensitivity to oxidation are additional contributors. 9 Previous findings suggested interventions, including healthy diet and physical exercise, that would significantly and more successfully have an impact on T2DM than metformin. 10,11 For example, flexibility training is important to maintain a full range of motion in T2DM individuals with joint limitations, which result from glycation of joint structures. 12 Major goals of T2DM therapy are to maintain blood glucose and blood pressure levels. 13 Those people can control blood glucose through nutritional plans, exercise programs, and self-care behaviors. 14 As mentioned above, oxidative stress is closely linked to T2DM, but regular exercise training may counteract oxidative stress by increasing antioxidant defense and decreasing lipid peroxidation. 15
Qigong exercise represents a combination of aerobics, isometric, and isotonic contractions, meditation, and relaxation with slow and simple movements. It is well suited for a beginner, elderly sedentary people, and those suffering from chronic diseases. 16,17 Previous findings suggest that qigong exercise training promotes beneficial effect on physical functions 16,18 as well as reduction of oxidative stress and improved antioxidant capacity in women. 18 Moreover, studies showed increased exercise performance and improved somatosensation 17 in T2DM patients following qigong training. In addition, Tai Chi or qigong was reported to provide more advantages on cardiovascular performance in elderly than younger adults. 19
The combined effects of regular qigong training on exercise performance, oxidative stress, and antioxidant responses have been rarely investigated, and reported results were equivocal, particularly in sedentary middle-aged and elderly women suffering from T2DM. Accordingly, this study set out to establish effects of an 8-week lasting qigong training on these parameters in this specific risk group. The authors hypothesized that qigong training would improve components of physical fitness accompanied with beneficial effects on the oxidant/antioxidant balance.
Materials and Methods
Design
Initially, this study has been designed as a randomized control trial, however, with the COVID-19 pandemic, the authors were forced to employ a Quasi-experimental design, placebo-controlled study, with a blinded outcome assessor. The planned sample size was 50 sedentary middle-aged and elderly women with noncommunicable diseases, and due to the pandemic, the authors had to reduce this number to 40. The participants were enrolled from Bangsean district communities, Chonburi Province, Thailand. The following inclusion criteria have been applied: age between 45 and 70 years, willingly participated in the study, not being physically active more than once per month, being a nonsmoker, not consuming alcohol, and not using antioxidant supplements. The sedentary lifestyle was assessed by using physical activity records. 20 Diseases representing a potential health risk for executing the qigong training were considered exclusion criteria.
The Physical Activity Readiness Questionnaire was used for the assessment of a possible health risk related to qigong training. 21 Ethical approval was obtained from the Burapha University-Institutional Review Board for Protection of Human Subject in Research (041/2563) and the Thai Clinical Trials Registry (TCTR20221003001). The study was carried out in accordance with the institutional committee on human research and the ethical standards laid down in the Helsinki Declaration as revised in 2013.
Intervention
Participants were assigned to qigong exercise (QG, n = 20) or to the control group (CG, n = 20). Qigong exercise comprised gentle practice, paying attention to movements, as well as breathing, relaxation, and mindfulness, by 18 basic movements modified in line with Taiji qigong by Robinson 22 and Ladawan et al. 23 Qigong exercise training was led by an experienced instructor. Training sessions consisted of warm-up with stretching for 2 min, followed by 60 min of performing the 18 movements and ended by stretching for 2 min as cool down. The training sessions took place once a day, 3 days per week over 8 weeks. Members of the CG have been advised to carry on their routine behavior and dietary habits over the entire study period.
Blood samples were taken from antecubital veins two times at the same time and days for both QG and CG. Subjects fasted overnight before the blood collections were taken at around 7

Schedule for qigong exercise training intervention. CG, control group; QG, qigong exercise group.
Primary outcome measurements
Determination of muscle strengths
The strength of back and leg muscles was determined by the use of a digital dynamometer (T.K.K. 5102 Back-D; Takei Scientific Instruments Co., Tokyo, Japan). Subjects were asked to stand on the dynamometer board with 20–30 cm feet apart. The back-muscle strength was determined by holding the grips with both hands at 30° of hip flexion without bending the knees, customized the chain length, and smoothly loaded the back muscles. 24 The leg muscle strength was assessed with subjects grasping the grips in stretch position with knee bending around 130°–140°. The chain length was maintained at a suitable knee angle. The leg strength was assessed when subjects strongly extended their legs but did not use back muscles. 25 Two trials were done for each test with a 1-min rest between trials. The measurements were obtained as means with units in kilogram and divided by the individual body mass (kilogram).
Determination of trunk flexibility
The trunk flexibility was assessed by the sit and reach box. Subjects were sitting on the floor with feet against the box (Baseline 12-1085 Sit n’ Reach Trunk Flexibility Box-Standard; Fabrication Enterprises, Inc., White Plains, NY). Legs had to be stretched with both knees locked and placed on the floor. One hand was placed on top of the other. Subjects reached forth along the measuring line as far as possible. Posterior of the knees had to hold even on the floor without any lunging, bobbing, or forced compensation. The reach forward had to remain for 1–2 sec while the distance was read. 26 Two attempts were carried out and values were noted as means (unit in centimeters).
Determination of VO2 max predicted and walking intensity derived from the 6-minute walk test
The 6-minute walk test (6MWT) was performed according to the guidelines of the American Thoracic Society.
27
The participants were informed to walk for 6 min along a 30-m line at an interval of 1.5 m on an outdoor corridor, and the distance walked was recorded in meters. Subjects were encouraged to walk continuously as fast as possible. Individual VO2 max was predicted as follows:
Walking intensity was estimated as metabolic equivalents of task (METs) using metabolic prediction equation for the 6MWT: METs = [3.5 + (0.1 × 6MWTspeed)] ÷3.5. 29
Secondary outcome measurements
Assessment of body composition and basal metabolic rate
Body composition and basal metabolic rate (BMR) were measured, including body mass, body mass index, height, waist-to-hip ratio (WHR), fat mass, and lean body mass, by using bioelectrical impedance analysis (In Body 270; Body Composition Analyzer, Korea).
Determination of FPG
Plasma was transferred on ice and directly analyzed by NHealth (Samitivej Chonburi Hospital). FPG was determined by the hexokinase method (ARCHITECT ci4100, integrated system; Abbott Diagnostics, Abbott Park, IL).
Evaluation of oxidative stress measurement
The oxidative stress was measured as malondialdehyde (MDA) level, assessed by thiobarbituric reactive substance (TBARS). The TBARS assay was modified from Nielsen et al. and Tsai et al. 30,31 The reaction mixture consisted of 1 mL of 1:2 diluted plasma, 50 μL of 0.1 mmol/L butylated hydroxyl toluene, 500 μL of 5 mmol/L EDTA, 1 mL of 8.1% (w/v) sodium dodecyl sulfate (SDS), 1 mL of 10% (w/v) trichloroacetic acid, and 1.5 mL of 0.67% (w/v) thiobarbituric acid. The mixture was kept at 95°C for 30 min, and the reaction was stopped by immersing in water for 5 min. Then, it was centrifuged at 3000 rpm for 15 min. The supernatant was delivered for identification of optical density at 532 nm. The tetraethoxypropane concentration was set as the standard curve at a range between 0.25 and 2 μmol/L.
Evaluation of total antioxidant capacity as ferric reducing antioxidant power assay
Total antioxidant capacity (TAC) was determined by ferric reducing antioxidant power (FRAP) assay, modified from Benzie and Strain. 32 The freshly prepared working FRAP reagent consisted of 300 mmol/L of acetate buffer, pH 3.6, 10 mmol/L of 2,4,6-tri [2pyridyl]-s-triazine (TPTZ), and 20 mmol/L of ferric chloride hexahydrate (FeCl3·6H2O) at a ratio of 10:1:1. The 900 μL of FRAP reagent was warmed at 37°C and 90 μL of deionized water was added. Then, 30 μL of plasma sample was added to the reaction mixture. The ferric tripyridyltriazine (Fe3+-TPTZ) complex was reduced to ferrous tripyridyltriazine (Fe2+-TPTZ), which had a blue color at low pH. The reaction was completely incubated for 4 min. The absorbance was immediately detected at 593 nm. Ferrous sulfate heptahydrate (FeSO4·7H2O) was used as standard.
Evaluation of catalase enzyme activity
The catalase enzyme activity (CAT) assay was analyzed by combining the optimum state of enzyme activity and spectrophotometric measurement of hydrogen peroxide (H2O2) that make the stable compound with ammonium molybdate at absorbance 405 nm. 33 In brief, 1 mL of substrate (H2O2 in phosphate buffer, pH 7.4) was kept with 50 μL of plasma at 37°C for 1 min. The reaction was halted with 1.0 mL of 32.4 mmol/L ammonium molybdate. The yellow compound was determined at 405 nm against reagent blank. The plasma CAT was linear up to 100 kU/L. One unit of CAT will decompose 1 μmol of H2O2 per minute to oxygen and water on the analysis conditions. The CAT was indicated as kilo unit per liter.
Statistical analysis
Data analyses were analyzed by using SPSS version 17.0 (SPSS, Inc., Chicago, IL). Normality was tested by the Kolmogorov–Smirnov test. Data with normal distribution were showed as mean ± standard deviation. The primary outcomes (back and leg strength, trunk flexibility, 6MWT, VO2 max predicted, walking intensity—METs), body composition, BMR, and oxidative stress and antioxidant for changes from PRE to POST within each group were calculated using paired t-test or Wilcoxon signed-rank test as appropriated. Student's t-test or Mann–Whitney U-test was executed to compare mean differences of POST minus PRE between QG and CG. Statistical significance was indicated by a p-value <0.05.
Power and sample size estimations were based on expected leg strength changes with respect to Song et al. This study compared leg strength pre- to postexercise with Tai Chi training over 4 months in elderly women. 34 By using paired t-test with α = 0.05 and power = 0.80, the calculated sample size was 17 participants per group (G*power 3.1 software).
Results
PRE- and POST-assessments were achieved by 19 participants of the QG and 17 participants of the CG. One participant of the QG had stopped because she did not carry on the training as indicated in the study progress (Fig. 2). Three participants of CG dropped out because they were concerned about the COVID-19 situation. Basic characteristics indicate no significant differences between QG and CG, as given in Table 1.
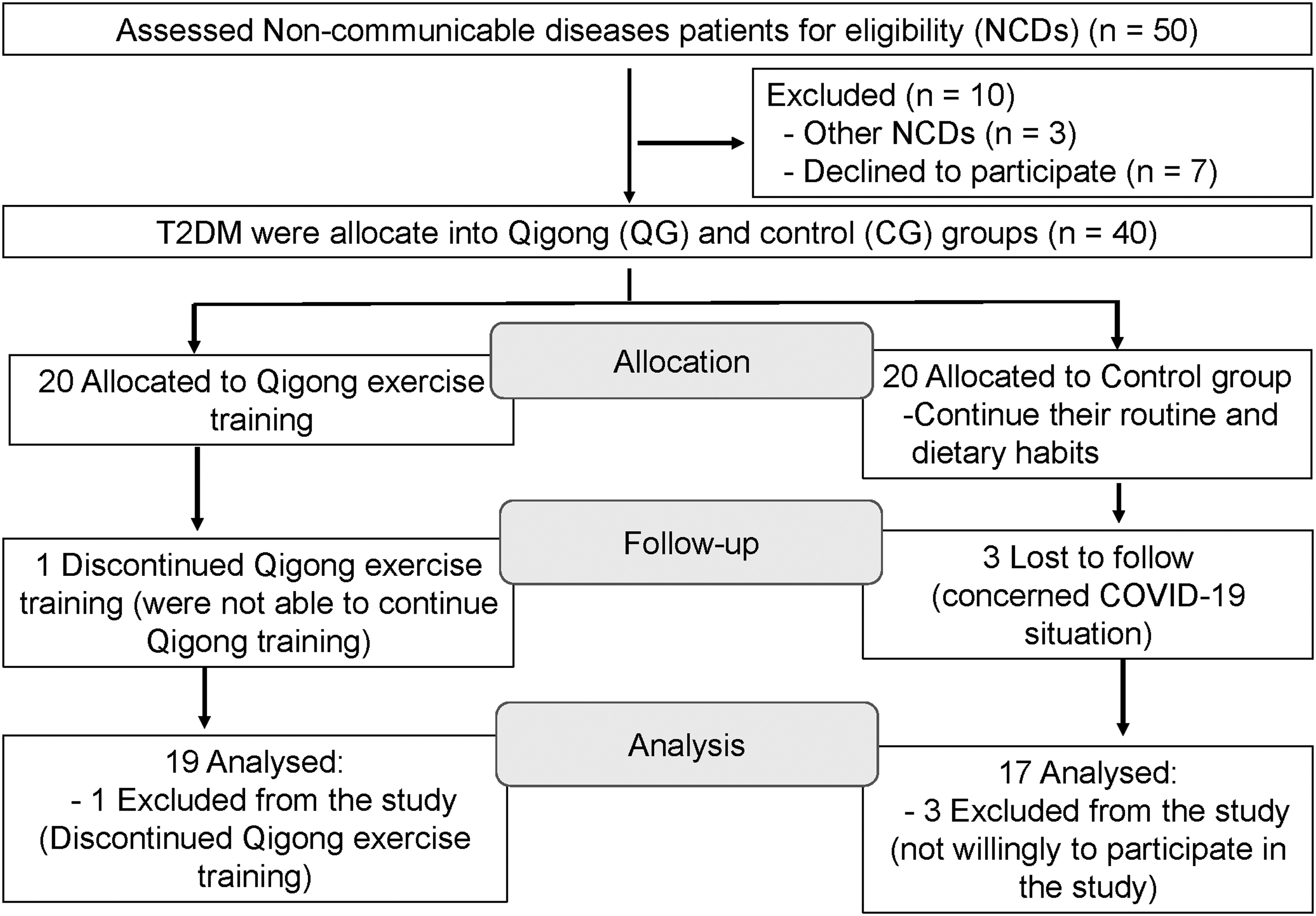
Flow diagram of study progress.
Baseline Characteristics of the Qigong and the Control Group
Values are presented as mean ± standard deviation.
BMI, body mass index; CG, control group; FPG, fasting plasma glucose; QG, qigong group.
Primary outcomes
Physical performance
Both leg strength and trunk flexibility were significantly enhanced after qigong training compared with control conditions (+25% vs. −2.9% for leg strength and +11.2% vs. −7.2% for trunk flexibility, p < 0.05) (Table 2). VO2 max predicted, 6-min walking distance, and related walking intensity were significantly increased after qigong training (+5.5% for VO2 max predicted, +7.3% for 6-min walking distance, and +5.2% for walking intensity, p < 0.05), but did not differ between groups (p > 0.05).
Physical Performances at Baseline (PRE) and After the Intervention (POST) in the Qigong and the Control Group
Values are presented as mean ± standard deviation.
Significant difference at p < 0.05.
6MWT, 6-minute walk test; CG, control group; MET, metabolic equivalent of task; QG, qigong group.
Secondary outcomes were FPG, body composition, antioxidant/oxidant parameters
There were no significant differences in FPG levels at PRE and POST within both the QG (p = 0.111) and the CG (p = 0.297), and no different changes between groups (p = 0.824). However, WHR tended to decrease within the QG compared with the CG (p = 0.093), Table 3. MDA was significantly decreased only after qigong training (−23.7%, p < 0.05) but did not differ between groups (Table 4). The antioxidant/oxidant balance improved after qigong training (+32.8%, p < 0.05), but changes between groups were not different.
Fasting Plasma Glucose, Body Composition, and Basal Metabolic Rate at Baseline (PRE) and After the Intervention (POST) in the Qigong and the Control Group
Values are presented as mean ± standard deviation.
BMI, body mass index; BMR, basal metabolic rate; CG, control group; FPG, fasting plasma glucose; QG, qigong group; WHR, waist-to-hip ratio.
Oxidative Stress, Nonenzymatic and Enzymatic Antioxidants at Baseline (PRE) and After the 8-Week Intervention Period (POST) in the Qigong and the Control Group
Values are presented as mean ± standard deviation.
Significant difference at p < 0.05.
CAT, catalase enzyme activity; CG, control group; MDA, malondialdehyde; QG, qigong group; TAC, total antioxidant capacity.
Discussion
The main findings of the present study indicate enhanced leg strength and trunk flexibility in the QG compared with the CG (p = 0.001 and p = 0.012). Distance in 6MWT, VO2 max predicted, and METs (walking intensity) were improved only after qigong training. In addition, qigong exercise resulted in improved antioxidant/oxidant balance (TAC/MDA).
FBG levels remained unchanged by qigong training, likely associated with complex regulatory mechanisms. 35 Various exercise studies reported conflicting results, for example, decreased FBG, 36 no change, 37 and increased FBG. 38
The association between muscle force and reactive oxygen species (ROS) has been described by Reid et al., who suggested that increasing force production by skeletal muscles corresponds with the alteration of ROS. 39 On the one hand, regular exercise is associated with increased levels of oxygen consumption, thus generating more ROS 40 ; however, exercise training also upregulates antioxidants, typically resulting in improved oxidant-antioxidant balance. 41,42 In agreement, the presented finding of improved oxidant-antioxidant balance after qigong training may suggest reduced oxidative stress. In T2DM, there are increasing indices of lipid peroxidation and protein oxidation, even in patients without complications. 43,44 ROS development along with a decreasing endogenous antioxidant performance causes a redox imbalance, promoting generation of T2DM and its complications. 45
Current literature findings demonstrate that moderate-to-high intensity exercise can activate adaptive responses and enhance endogenous antioxidant protection systems for encountering ROS with sustaining muscle redox equity. 46,47 These results support those findings and are also in accordance with Pittaluga et al., who observed that oxidative stress markers after moderate training exercise in T2DM were decreased due to improved redox homeostasis by increasing endogenous antioxidant defenses. 48
The benefits of qigong training on muscle strength are compatible with current studies presenting the development of knee strength in elderly people after Tai Chi training. 34,49,50 Qigong training postures are comparable with Tai Chi training, which accomplish in semisquat with gentle motions and load movement of the body. The flow movement sequence of concentric and eccentric contractions is basically related to lower extremities in close kinetic chain posture. 49,50 The improved trunk flexibility in the present trial is in accordance with previous studies. 51,52 T2DM patients are susceptible to contracture, resulting in joint limitation. 53 Notably, Herriott et al. reported that after flexibility training for 8 weeks, flexibility was improved only in the older diabetes group but not in the older healthy group. 54 Practicing qigong postures is related to considerable stretches of the spine and limbs, likely alleviating stiffness in the spine and maintaining muscle relaxation. 55
Qigong exercise training was repeatedly shown to enhance aerobic exercise capacity in patients suffering from chronic diseases, for example, Parkinson's 56 or chronic obstructive pulmonary disease. 57 These findings are also in accordance with Molina-Sotomayor et al., who demonstrated that older women with T2DM improved cardiorespiratory fitness (determined by the 6MWT) after aerobic exercise training. 58 Moreover, aerobic physical exercise training is of importance for older adults, indicating improved aerobic power 59 and physical state through walking-based training. 60 Zhao et al. found enhanced aerobic capacity, general physical fitness, and bone mineral density in stable coronary artery disease patients after cardiac rehabilitation by the use of qigong exercise. 61
Underlying mechanisms may include improvement of respiratory function through the constant alteration of thoracoabdominal pressure following the movement of expiration and inspiration with qigong training. The increase in circulating blood volume extends blood volumetric loading as well as muscle contraction stimulating backflow of blood together with reducing the resistance of peripheral arteries. As a consequence, long-term adaptation to training improves cardiac output, myocardial oxygen consumption, and effective cardiac contraction. 61 –63
The following limitations have to be considered: first, participants were not randomly allocated to the QG or CG due to the COVID-19 pandemic, the long period of training, and time constraints. Depending on their baseline characteristics, there were no differences between QG and CG. Second, despite a priori power calculations, the study may be underpowered with regard to certain outcomes, but changes observed within the QG may be meaningful and will stimulate future studies with larger sample sizes. Strengths of the present study include the homogenous sedentary group of middle-aged and elderly women with T2DM and the proper monitoring of exercise training.
Conclusion
The present findings show significantly improved leg strength and trunk flexibility in sedentary middle-aged and elderly women with T2DM after 8 weeks of qigong training, accompanied by slight improvements in the antioxidant/oxidant balance. These effects may beneficially impact on health in women suffering from T2DM. Nevertheless, future more large-scaled studies are necessary to confirm these findings and to demonstrate their clinical relevance.
Footnotes
Acknowledgments
The authors express their thanks to the Faculty of Allied Health Science, Burapha University.
Authors' Contributions
K.K. contributed to the design of the study, data collection, data analysis, and first draft of this article; S.S. contributed to data collection and laboratory analysis; N.L. and S.K. contributed to the design of the study and data collection; P.B. contributed to the supervision of the article; M.B. contributed to data analysis and supervised the article. All authors contributed to the article writing. All the authors have read and approved the final version of the article, and agree to the order of presentation of the authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Faculty of Allied Health Science, Burapha University, Chonburi, Thailand. Grant Number is AHS6/2563.