
Abstract
Introduction:
Endothelial dysfunction is the initial step in the pathogenesis of atherosclerosis; and it plays a central role in the development of cardiovascular diseases and many types of human diseases (diabetes, kidney failure, cancer, and viral infections). Strategies that are effective in protecting vascular endothelial function and retard or reversing endothelial dysfunction in the early stage appear to be potential in the prevention of vascular, cardiac, and many human diseases. Several studies have been carried out on the effects of yoga on endothelial function, but the results of these studies have not been synthesized. This study aimed at conducting a systematic review and meta-analysis to determine the effectiveness of yoga on endothelial function.
Methods:
A systematic review and meta-analysis of studies that assessed the effect of yoga practice on vascular endothelial function was done as per the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The PubMed, Scopus, Google Scholar, and Cochrane controlled register of trials (CENTRAL) were searched from inception to August 2022. The search strategy was constructed around yoga-based techniques and endothelial function. All the yoga-based interventional studies on endothelial function or dysfunction were included in this review. A narrative synthesis and descriptive analysis were done due to the diverse methodology of selected studies. We carried out a formal meta-analysis of controlled trials that assessed the effect of yoga on flow-mediated dilatation (FMD), a measure of endothelial function.
Results:
A total of 18 studies were included for review involving 1043 participants. Yoga training showed improved endothelial function in 12 studies, whereas 6 studies did not find any statistically robust effect. Meta-analysis (n = 395 participants, 6-studies, 7 comparisons) showed an increase in brachial FMD by yoga practice (mean difference = −1.23%; 95% confidence interval −2.23 to −0.23; p = 0.02). The heterogeneity between the studies was 43% (Tau2 = 0.70, χ2 = 10.49). The risk of bias was low to moderate in these studies. No adverse effects were reported.
Conclusions:
Yoga practice improved endothelial function. Yoga could be a safe and potential integrative medicine to improve endothelial function. However, as the statistical heterogeneity, that is, variation in the FMD among the studies was moderate, large clinical trials are necessary for its clinical recommendations.
Introduction
Endothelial dysfunction is a well-documented predictor of atherosclerosis and plays a central role in the development of cardiovascular (CV) diseases and many types of human diseases (diabetes, kidney failure, cancer, and viral infections). 1,2 It is mainly characterized by a disturbance in the balance between vasodilators and vasoconstrictors; impairment in endothelial-dependent relaxation, and the induction of a proinflammatory and prothrombic state. 3
The endothelium is involved in a multitude of physiological functions and plays a critical role in controlling vascular tone, blood pressure, vascular permeability, blood fluidity, fibrinolysis, and angiogenesis; inhibiting platelets aggregation, leukocyte adhesion, and migration; preventing inflammatory response and thrombogenesis; suppressing vascular smooth muscle cell proliferation; and maintaining CV integrity and homeostasis of different organs and systems. 4 The endothelium regulates these functions by synthesizing and releasing several factors such as vasodilators, vasoconstrictors, antithrombotic factors, growth factors, and inflammatory mediators. 5,6
Nitric oxide is recognized as the most essential endothelial-derived relaxation factor (EDRF) and a key molecule in the maintenance of vascular tone, integrity, and homeostasis. Reduction in the bioavailability of nitric oxide results in endothelial dysfunction. 7 Impaired endothelial-dependent vasodilation, which is mediated by nitric oxide, is a hallmark of endothelial dysfunction. 8
The endothelium is the primary site of dysfunction in CV and metabolic diseases. Factors that impair endothelial function and subsequently damage vasculature are common CV risk factors such as hypertension, diabetes, insulin resistance, dyslipidemia, homocysteine, hypercholesterolemia, oxidative stress, inflammatory factors, aging, obesity, smoking, estrogen deficiency, menopause, chronic inflammatory diseases, environmental stressors (noise and air pollution), and mental stress. 1,4,7
Currently, there are several methods to measure endothelial function. Ultrasound assessment of endothelial-dependent flow-mediated vasodilation (flow-mediated dilatation [FMD]) of the brachial artery is the gold-standard clinical measure of endothelial function. 9 Other measures are cardiac catheterization, venous occlusion plethysmography pulse wave analysis (PWA), flow-mediated magnetic resonance imaging (MRI), laser Doppler skin-flowmetry, and digital pulse amplitude tonometry (PAT). 10
Biomarkers of endothelial function include endothelial progenitor cells, endothelial microparticles, asymmetric dimethyl arginine (ADMA), adhesion molecules, selectins, nitric oxide concentration (NOx), and endothelins. 11
There is convincing evidence that endothelial dysfunction predicts future CV events. Strategies that are effective in improving or reversing endothelial dysfunction in the early stage appear to be potential in the prevention and control of vascular, cardiac, and many human diseases. 2 Several interventions (lifestyle and pharmacological treatment) have been shown to improve endothelial function and reduce CV risk. 12 Statins, 13,14 angiotensin-converting enzyme inhibitors, 15 and aspirin 16 improve endothelial function and reduce CV morbidity and mortality. Favorable responses of the endothelium to lifestyle changes have also been reported. 12
Yoga is a mind–body exercise rooted in Vedas and ancient Indian literature is beneficial for physical, mental, and spiritual well-being. Yoga is associated with a significant reduction in CV risk and diseases. 17 Several studies have been carried out on the effects of yoga on endothelial function, where a few studies reported an improvement in endothelial function 18 –29 whereas a few showed no effects; 30 –35 but the results of these studies have not been synthesized. Therefore, this study aimed at conducting a systematic review and meta-analysis to determine the effectiveness of yoga practice on endothelial function.
Methods
This systematic review has been registered prospectively in the PROSPERO (CRD42020195995). The guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) were followed for reporting this systematic review and meta-analysis.
Data sources and search strategy
Four electronic databases: PubMed, SCOPUS, Cochrane Controlled Register of trials (CENTRAL), and Google Scholar were searched for eligible studies that are published in English language through August 2022. 36 Google Scholar was used to search academic and gray literature. 37 The keywords used for the searches are: “Yoga,” “Meditation,” “Pranayama,” “yogic breathing exercise,” “Yogasanas,” “asanas,” “endothelial,” “endothelium,” “flow-mediated vasodilation,” “endothelial-dependent vasodilation,” “vascular reactivity,” “nitric oxide,” and “endothelial markers.”
The Boolean operators “AND,” and “OR” were used to capture relevant and related articles (four reviewers). The references were also searched manually to find articles for review (two reviewers). Independently, two reviewers (V.K., R.C.) screened the titles and abstracts in the databases as per the eligibility criteria, whereas a third reviewer (S.G.P.) was consulted whether any disagreement existed between them.
Study selection
Types of participants: Studies including human participants of any age or gender.
Types of interventions: Yoga-based interventions: asanas (stretching and maintaining postures), pranayama (breathing exercises), meditation, relaxation techniques, yoga diet, yoga lifestyle; either of these used as a single technique or combined/integrated were included.
Type of Comparator: Active control, passive control, and single group studies without comparator were included.
Main outcome and measures of effect: Changes in the endothelial function assessed by FMD was the primary outcome. However, other measures and biomarkers of endothelial function were also considered for review.
Types of studies: All the interventional studies (i.e., controlled, uncontrolled, randomized, non-randomized, and cross-over) that assessed the effect of yoga on endothelial function were included in this review. There were no restrictions on language while searching or filtering the studies. Those studies whose full text was not available were excluded from the review.
Data extraction
The data were extracted and analyzed by two independent reviewers (E.C., V.K.). The third reviewer (R.M.D.) was consulted whether there was any discrepancy or no consensus between the two authors. A narrative synthesis was done due to the diverse methodology (study design, study quality, and measures of outcomes) of all selected studies.
Data extraction proforma of the current review included the following items: details of eligibility criteria, number of participants, participant characteristics (age, sex, diagnosis, duration of illness and eligibility criteria), type of yoga intervention and comparator, details of yoga-based intervention (duration of each session, frequency, type of yoga techniques, total duration of intervention), adherence to the intervention, outcome measures and method of measurement, results and conclusions, and adverse events. Details of the control group intervention were also recorded.
Mean change in FMD and standard deviation (SD) were recorded from only those studies that have FMD as an outcome. Missing SDs were imputed from the provided data as either 95% confidence interval (CI) or standard error or p-value according to the Cochrane statistical methods. 38 Authors were contacted for missing data and any additional information if required.
Quality assessment
The quality of the method of individual studies was assessed independently by two reviewers (H.S.V., A.M.C.) using the Cochrane risk of bias (RoB) tool. The third reviewer (R.R.) was consulted for any discrepancy between the two authors or whether there is no consensus between the two authors. The RoB tool includes the following items: Randomization sequence generation, allocation concealment, blinding of participants and investigators, the blindness of outcome assessments, incomplete outcome data, selective outcome reporting, and other biases. The quality of the studies was divided into three categories: low risk, high risk, and unclear bias according to the guidelines of Cochrane systematic review. 39
Data analysis
Meta-analysis of the results (FMD %) of the eligible studies was done using Review Manager (RevMan 5.4) software produced by Cochrane Collaboration. Mean change and SD values were added into RevMan 5.4. Statistical heterogeneity between the studies was assessed using the χ 2 test and I 2 value. Based on the I 2 value, heterogeneity between studies was categorized as low risk of heterogeneity (<25% of I 2 value), moderate risk of heterogeneity (25%–75% I 2 value), and high risk of heterogeneity (>75% I 2 value).
We have selected mean difference and 95% CIs for estimating the effect size of individual studies (as the measure of the primary outcome was the same in all studies). A fixed-effects model was used if there was homogeneity between studies or a random-effects model for heterogeneity. 40 A p-value <0.05 was considered as statistically significant. A result of the meta-analysis was shown in the form of a forest plot. A sensitivity analysis was performed to identify any undue influence of an individual study with a bias on the overall meta-analysis.
Results
Study selection process and search results
The study selection process and results are depicted in detail in Figure 1. The database search resulted in 399 titles and abstracts, out of that 21 studies were reviewed for eligibility. Of these, five studies were excluded: two had no yoga-based intervention, 41,42 one was an observational study, 43 and the measures of two were imprecise. 44,45 The full details and data of two conference abstracts were obtained by contacting the authors. Finally, 18 articles were included in the qualitative synthesis. Of these, six studies that assessed FMD were included for quantitative synthesis, that is, meta-analysis. 21,23,27,28,33,35
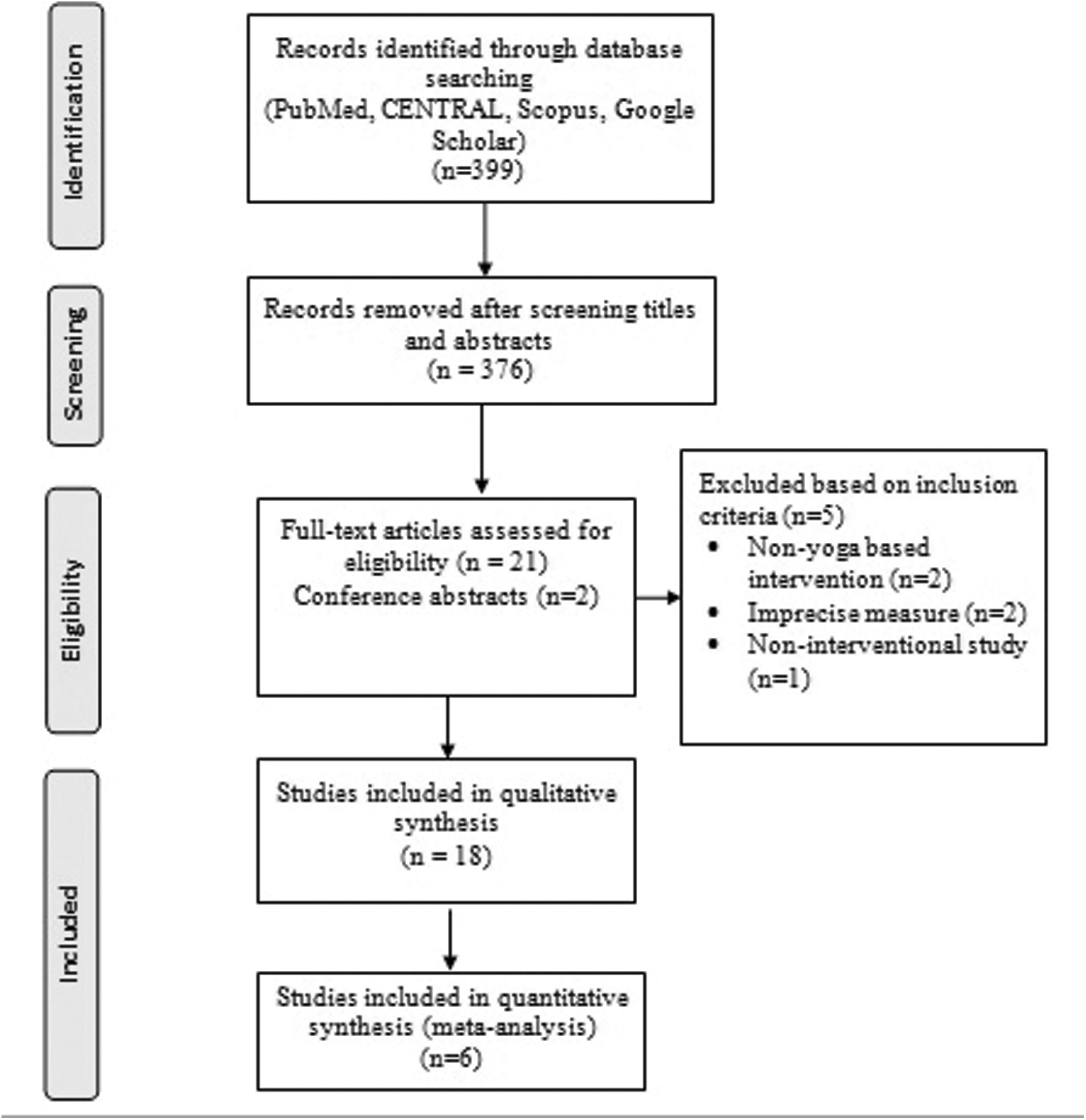
Flow diagram showing the results of database search.
Study characteristics and participants
A descriptive summary and study characteristics including study outcomes and results were provided in Table 1. There were 10 randomized controlled trials, 19,21,23 –26,28,30,32,33 1 randomized cross-over design, 35 4 non-randomized studies, 18,20,22,27 and 3 single group (without control group/comparator) studies with pre-post design. 29,31,34
General Characteristics of Included Studies
Age is given as mean ± SD; M/F indicates number of males/females.
ADMA, asymmetric dimethyl arginine; CAD, coronary artery disease; CHD, coronary heart disease; CRM, consciously resting meditation; DBP, diastolic blood pressure; ELISA, enzyme-linked immunosorbent assay; eNOS, endothelial nitric oxide synthase; ET-1, endothelin-1; FMD, flow-mediated dilatation; HE, health education; ICAM, intercellular cell-adhesion molecule; NOx, nitric oxide concentration; PP, pulse pressure; RCT, randomized controlled trial; SBP, systolic blood pressure; SD, standard deviation; VCAM, vascular cell-adhesion molecule.
Most of the studies originated in USA (n = 8). 18,22,23,27,28,31,33,35 Five studies were from India, 21,25,26,29,34 one each from Iran (two papers from the same project), 24,30 Taiwan, 20 Korea, 32 and China. 19 Type of participants were healthy, 19,22,23,29,31,32,35 overweight, and obese; 34 patients with coronary artery disease, 18,27,33 myocardial infarction, 21,26 metabolic syndrome, 28 dysmenorrhea, 30 migraine, 23,29 and elderly hypertension. 25
The total number of participants was 1043 (ranging from 13 to 200 subjects in each study) in the 18 included studies. Most of the studies included both genders, 18,21 –23,26–29,32,33,35 whereas a few had only females 19,20,24,30 or males, 25,34 and one study did not provide any information on gender. 31 Age of the participants was ranging from 17 to 70 years.
Details of interventions
The yoga programs used in the included studies are given in detail in Table 2. The total duration of yoga intervention was ranging from 10 days to 52 weeks. One study assessed the immediate effects of several yoga postures. 35 The minimum duration of each session was 40 min and the maximum was 120 min; and the frequency of sessions was 2–7 times/week. Dod et al. evaluated the Ornish program, which is a multicomponent intervention including yoga, increasing physical activity, dietary approaches, and tobacco cessation. 18
Details of Intervention: Yoga Programs
Method of assessment of endothelial function
The method used for the assessment of endothelial function in the included studies is given in Table 1. The measure used in most studies was brachial FMD (which is a gold-standard measure of endothelial function). 18,22,23,27,28,31,33,35 However, others evaluated the biomarkers of endothelial function such as ADMA, 25 NOx, 20,25,26,29,30,32 endothelin-1 (ET-1), 26,34 endothelial nitric oxide synthase (eNOS), 26 cell-adhesion molecules, 24,26 and endothelial microparticles. 19
Effect of yoga practice
Meta-analysis of effect of yoga on FMD
The results of the meta-analysis were presented in a forest plot (Fig. 2). Among the 15 controlled trials, 7 assessed FMD whereas the other studies evaluated different biomarkers of endothelial function such as circulating endothelial microparticles, ADMA, nitric oxide, or ET-1. One of the studies (Dod et al.) included aerobic exercise (3 h/week) along with yoga and meditation (1 h daily) in its intervention program, so it was excluded from the meta-analysis. 18

Forest plot.
Hence, the results of six controlled trials assessing FMD were included in the meta-analysis, which showed a significant increase in brachial FMD with yoga practice (Mean difference −1.23%, 95% CI −2.23 to −0.23, p = 0.02). Hunter et al.'s study included two yoga groups where participants practiced yoga at two temperatures: yoga at 23°C and 40.5°C, respectively; and one control group. Hence, the data of this study in the forest plot are shown as Hunter 2018a (Yoga at 23°C) and Hunter 2018b (Yoga at 23°C). 24 These 6 studies included 7 comparisons and a total of 395 participants (188 in the yoga group and 207 in the control group). The heterogeneity between the studies was 43% (Tau 2 = 0.70, χ 2 = 10.49). The RoB was low to moderate in these studies.
Narrative review
The results of the effect of yoga on endothelial function have been summarized in Table 1. Out of 18 studies, 12 had reported a significant favorable change in the measures of endothelial function with yoga intervention, 18 –29 whereas 6 studies did not find any significant effect. 30 –35 Yoga intervention has improved endothelial function in healthy subjects 19,22,23,29 and in patients with coronary heart disease, 18,27 myocardial infarction, 21,26 metabolic syndrome, 28 hypertension, 25 migraine, 24 and dysmenorrhea. 20 Among the three studies on patients with coronary heart disease, two studies showed an improvement in endothelial function with yoga 18,27 whereas one study did not find any significant effect. 33
Among healthy subjects, four studies showed an improvement in endothelial function 19,22,23,29 whereas three studies observed no significant change. 31,34,35 Chen et al. showed an improvement in female healthy participants. 19 One study reported a favorable change in endothelial function by yoga in middle-aged and older subjects but not in young healthy. 22 The comparator and the type of data analysis (i.e., between-groups or within-group) have been given in detail in Table 1. Most of the studies did both between-groups and within-group data analysis, 18 –20,24–26,28,30,32,33 whereas a few used only within-group data analysis. 23,27,29,31,34,35
Studies have reported significant favorable changes in circulating endothelial microparticles, 19 ADMA, 26 and homocysteine. 20 Among the six studies that evaluated NOx, there were increased NO levels in two studies, 25,29 decreased levels in one study, 32 and no significant difference in the other three studies. 20,26,29 One study showed a significant decrease in ET-1 levels in patients with acute myocardial infarction 26 whereas the other study found no change in healthy obese individuals. 34
There was no significant effect of yoga on intercellular cell-adhesion molecule (ICAM), 18,24,26 vascular cell-adhesion molecule (VCAM), 18,24,26 E-selectin, 18,26 eNOS, 26 and P-selectin. 26 Naji-Esfahani et al. found a favorable change in VCAM in patients with migraine. 24
Quality assessment and potential bias
The summary and graphical representation of the assessment of RoB of the included studies is shown in Figures 3 and 4. Out of 18 studies, 10 studies reported appropriate generation of random allocation of sequence. Five studies presented the concealment of the allocation sequence. 19,21,26,28,33 Two studies masked the participants about interventions either by presenting it as health-promoting to minimize expectation bias/performance bias 28 or till baseline data collection. 23
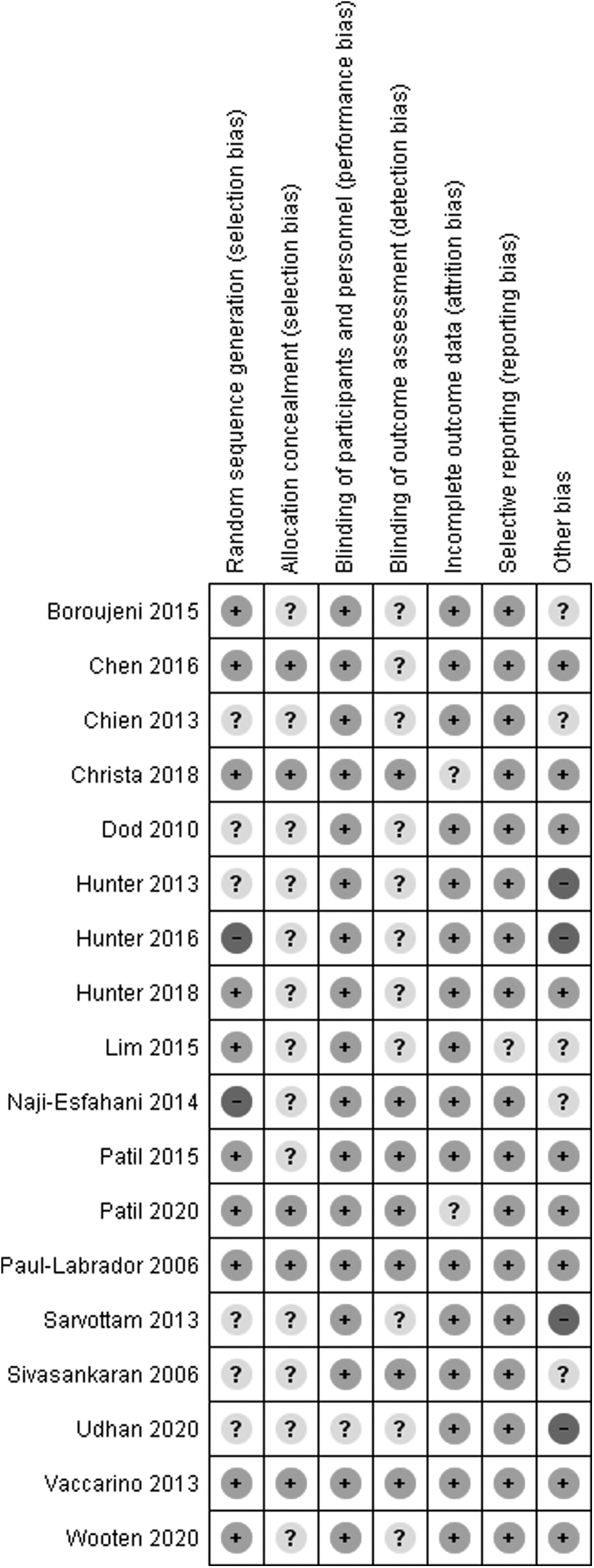
Risk-of-bias summary.
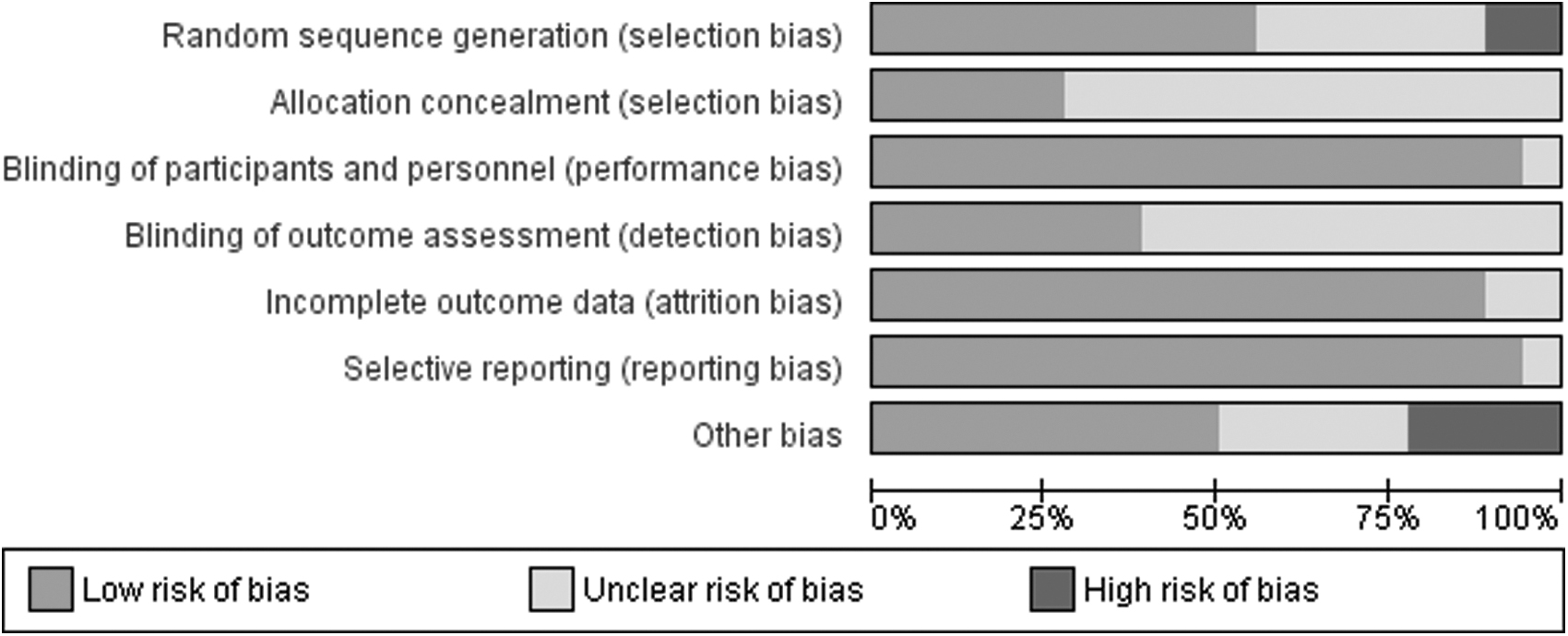
Risk-of-bias graph.
However, we believe that the outcomes of lifestyle modification studies are not likely to be influenced by lack of blinding. Blinding of assessment outcomes was done by seven studies. All the studies presented complete outcome data except two where the information was unclear, 24,30 There was no reporting bias in 17 studies, of which 1 study split the outcomes of a single study into 2 publications. 24,30
However, it is to be noted that very few studies have either registered in clinical trial registries or published the protocol. We found a high RoB in the design of a few studies; either the participant's condition of the comparator group was not similar to the study group 20,27 or no comparator 22,27 or single-group studies. 29,31,34
Sensitivity analysis
A sensitivity analysis of the studies included in the meta-analysis did not show any significant influence of an individual study on the overall meta-analysis.
Adverse events
Among the included studies, only two studies had reported adverse events. 23,33 Of these, one had reported a pulling hamstring during the practice of asana (Half-moon pose/Ardha-chandrasana) 23 whereas other studies had no adverse events. 33
Discussion
We believe that this is the first systematic review and meta-analysis of the effect of yoga on endothelial function. We have included 18 studies involving 1043 participants for review and narrative synthesis; and 6 studies (that assessed FMD) involving 395 participants for meta-analysis.
Yoga training showed an improvement in endothelial function in 12 studies whereas 6 studies did not find any statistically robust difference. The meta-analysis of six studies showed a significant increase in brachial FMD in the yoga group, indicating an improvement in endothelial function with yoga practice. A moderate (43%) heterogeneity was found between the studies.
The variability in the duration, frequency, and type of yoga techniques among the intervention programs of the reviewed studies may be attributed to the differences in the results (effect size) of the studies. The duration of yoga intervention ranged from 6 weeks to 12 months, except in one study that evaluated the immediate effect of 20 selective yoga postures practiced for 30 sec each. 35
Studies with yoga intervention for ≥12 weeks have shown better beneficial changes in endothelial function (77%; 10 out of 13 studies) than those with ≤12 weeks of yoga intervention (40%; 2 out of 5 studies). Duration of each session did not affect much but studies that delivered the intervention for ≥5 times a week (frequency; 87.5%; 7 out of 8 studies) showed greater response than those using intervention ≤5 times a week (62.5%; 5 out of 8 studies).
In one study by Sarvottam et al., the frequency of intervention was 7 times/week but the total duration of yoga training was only 1.5 weeks 34 whereas in another study immediate effects were observed. 35 These findings suggest that higher frequency and duration of yoga intervention is associated with greater endothelial response. However, the adequate dosage (duration and frequency) of yoga intervention for endothelial protection or improvement remains unclear and needs to be determined.
The RoB was low in 50% of the studies, moderate in 30%, and high in 20% of the studies included in the narrative syntheses (n = 18). However, the quality of the methodology of the six studies included in the meta-analysis was good with low to moderate RoB.
The intervention program of most of the studies of this review included only yoga-based techniques except one study by Dod et al., where apart from yoga and meditation (1 h daily), aerobic exercise (3 h/week) was also part of their Multisite Cardiac Lifestyle Intervention Program. 18 Hunter et al. compared the effect of yoga training at two temperatures on FMD, in which they reported a significantly better improvement in FMD with yoga, practiced in a thermoneutral condition (23°C) than heated condition (40.5°C). 23
Limitations
There are several limitations to this review. The search strategy was focused only on studies published in the English language, so we may have missed studies published in other languages. Instead of focusing on one clinical condition, all studies that assessed the effects of yoga on endothelium were included. There was both clinical and methodological diversity that may affect and vary the intervention effects. Hence, statistical heterogeneity among the included studies was significant.
Due to fewer numbers of controlled studies that assessed the biomarkers of endothelium, it was not possible to conduct a meta-analysis of yoga effects on endothelial biomarkers. Since unpublished and non-English language studies were not searched, and the study protocols of most of the studies included for review were not published or registered prospectively, so potential for publication bias cannot be ruled out.
Implications for research and clinical practice
Despite the successful control of CV risk factors with several strategies including drugs, the reduction of CV morbidity and mortality is limited to about 20%–45%. 12 The tool that helps in monitoring the response to treatment and can predict future events will be useful in identifying the patients at risk (despite optimal treatment). A growing number of interventions that are known to reduce CV risk are found to be associated with improved endothelial function. 46
Because endothelial dysfunction predicts future events, major research efforts have been focused on the early detection of endothelial dysfunction and the identification of new treatment approaches in humans. Available evidence supports that change in endothelial function can be used in the care of patients and as a surrogate measure for assessing the effectiveness of interventions that prevent CV events. 46,47
The findings of this review are intriguing, as they showed a favorable endothelial response to yoga in people with varying health issues and during cardiac rehabilitation. The methodological quality of the controlled trials included in the meta-analysis was good and demonstrated significant improvement in endothelial function with yoga practice. This implies that yoga could be a potential clinical tool to improve endothelial function.
However, most of the studies did not assess the association between improvement in endothelial function and clinical outcomes with yoga; and were limited by small sample size. Therefore, still there is a need for clinical trials with large sample sizes; and those that can focus and provide evidence on the association of change in the endothelial function with clinical outcomes following yoga practice. Further, future studies should also focus on the underlying mechanisms through which yoga influences endothelial function.
Mechanism of yoga on endothelial function
The precise mechanism underlying the benefit of yoga on the endothelial system remains to be elucidated. Oxidative stress and vascular inflammation play a major role in the development of endothelial dysfunction. Vascular oxidative stress reduces the bioavailability of nitric oxide either by scavenging nitric oxide by superoxide or by altering the function of eNOS, where it produces superoxide instead of nitric oxide (eNOS uncoupling).
Oxidative stress also induces ET-1 synthesis in endothelial cells and human macrophages. 48 Either reduction in bioavailability of nitric oxide or increased production of ET-1 results in endothelial dysfunction and shifts the physiological endothelial balance toward vasoconstrictor dominance. 49 A few studies endeavored to explore the mechanism underlying the yoga-induced changes in the endothelial system. We have recently investigated the effect of 3 months of a yoga-based cardiac rehabilitation program on several biomarkers related to the endothelial system and oxidative stress in patients after acute myocardial infarction.
Our study found a significant reduction in ADMA, ET-1, ICAM-1, VCAM, E-selectin, and total antioxidant capacity (TAOC) with yoga CaRe program. In this study, yoga did not induce any change in eNOS, P-selectin and total NOx, oxidized low density lipoproteins (LDL) (Oxd-LDL), superoxide dismutase (SOD), and inflammatory markers: tumor necrosis factor-alpha (TNFα), C-reactive protein (CRP). 26 However, in the study of Dod et al., there was no significant change in cell-adhesion molecules after 3 months of lifestyle intervention program (yoga and meditation, nutrition, aerobic exercise, smoking cessation, and psychological support) in patients with coronary artery disease. 18
Yoga also induced significant enhancement in NOx in healthy 29 and elderly patients with hypertension, 25 but not in women suffering from migraine 30 and dysmenorrhea. 20 A few studies have demonstrated the beneficial effects of yoga on oxidative stress, inflammation, and its related genes expression. 50 –56 In the studies of Bhasin et al., and Dusek et al., they reported a reduced expression of gene linked to oxidative response, inflammatory response, and stress-related pathways in healthy individuals. 55,56
Thus, the probable mechanism by which yoga improved the endothelial function is by restoring the vasoconstrictor and vasodilator balance (either decreasing ET-1 or increasing bioavailability of NO) by reducing the vascular oxidative stress and inflammation. However, further studies focusing on molecular mechanisms (particularly, expression of genes related to endothelium) are required to understand the precise mechanism of yoga on endothelial function.
Conclusions
Yoga practice improves endothelial function and can restore the endothelial balance toward physiological vasodilator dominance. Yoga could be a safe and potential integrative medicine to improve endothelial function. However, as the statistical heterogeneity, that is, variation in the FMD among the studies was moderate, large clinical trials are necessary for its clinical recommendations.
Footnotes
Acknowledgment
The authors are thankful to Shri Dharmasthala Manjunatheshwara University for the partial support to this project.
Authors' Contributions
S.G.P. and P.D. contributed to the conception or design of the work. V.K., E.C., R.C., A.M.C., H.S.V., R.R., K.A., and S.G.P. contributed to the acquisition, analysis, or interpretation of the work. S.G.P. and R.M.D. drafted the manuscript. K.K.D., A.R., S.K., and P.D. critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring the integrity and accuracy.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.
Supplementary Material
PRISMA Checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.