
Abstract
Background:
Sleep disturbances, which are common problems in older adults, often lead to cognitive decline and depression and may even increase mortality risk. Foot thermal therapy is a simple and safe approach for improving sleep and is associated with relatively few side effects. However, the effect of different operations of foot thermal therapy on sleep quality in older adults is inconclusive. This study aimed to access the effects of temperature, duration, and heating height of foot thermal therapy (administered through a footbath) on the subjective and objective sleep quality of older adults.
Methods:
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline, eight databases were searched for all relevant articles published up to July 2023, and a rigorous systematic review and meta-analysis was conducted. This study was registered in the PROSPERO database (CRD42022383460). Inclusion criteria were: (1) participants with a mean age ≥60 years; (2) interventions that included foot thermal therapy; (3) a control group that received routine care but no thermal therapy; (4) outcome measurements that assessed sleep quality; and (5) the studies that utilized randomized controlled trials or quasi-experimental studies. Methodological quality was assessed using the Joanna Briggs Institute critical appraisal tools. The meta-analysis was performed using RevMan version 5.4.
Results:
A total of 11 studies were included. Foot thermal therapy before bedtime improved subjective sleep quality in older adults, with optimal parameters of 40°C temperature (standardized mean difference [SMD] = 0.66, 95% confidence interval [CI]: 0.33 to 0.99), ≤20-min duration (SMD = 0.66, 95% CI: 0.39 to 0.93), and 10 cm heating height (SMD = 0.78, 95% CI: 0.45 to 1.11). Subgroup analyses revealed that a temperature of 41°C–42°C can improve objective sleep latency (SMD = 0.54, 95% CI: 0.09 to 0.99).
Conclusions:
It is recommended to administer foot thermal therapy (40°C; ≤20 min; 10 cm above the ankle) to older adults 1 h before their bedtime. If they have trouble falling asleep, the temperature can be increased to 41°C–42°C.
Introduction
Sleep disturbances are a common problem in older adults, with an overall prevalence of ∼41%–58%. 1 –3 After the age of 60, there are significant differences in sleep structure compared to younger adults. 4 –6 These include prolonged sleep latency, increased wakefulness time and waking frequency after falling asleep, and decreased total sleep time and sleep efficiency. 6,7 Approximately 50% of older adults have difficulty in initiating and maintaining sleep, which results in early awakening and daytime sleepiness. 8,9 The effect of aging on sleep becomes noteworthy when considering the rapid increase in the population of older adults. One-sixth of the global population is expected to be aged ≥60 years by 2030; this proportion is projected to double by 2050. 10 Consequently, the number of older adults with sleep disturbances will increase. Therefore, understanding sleep disturbances in older adults and addressing these problems are imperative. Effective interventions to improve the sleep quality of older adults would significantly enhance their health.
Multiple methods can be applied to evaluate sleep disturbances in older adults. Examples of frequently used scales to measure subjective sleep quality are the Pittsburgh Sleep Quality Index (PSQI) and the Verran and Snyder-Halpern Sleep Scale (VSH). Objective sleep quality can be evaluated by estimating parameters such as total sleep time, sleep efficiency, sleep latency, and the duration of each sleep stage through polysomnography (PSG) and actigraphy (ATG). These measures collectively offer insights into sleep patterns, with total sleep time, sleep efficiency, and sleep latency indicating the sleep duration, sleep proportion, and sleep onset time, respectively. These data can be collected using PSG and ATG, thus providing a better understanding of sleep in older adults. 11,12 Health care providers should prioritize addressing sleep problems in this population.
Sleep disturbances are associated with many adverse events in older adults, including increased fall risk, cognitive decline, depression, and poor health. These adverse events may also reduce the quality of life of older adults and increase their risk of mortality. 13 –15 Most people resort to medications to rapidly alleviate sleep disturbances; however, some medications have adverse effects such as drug tolerance and dependence, which may lead to sleep apnea. Furthermore, because of the aging-related decline in the metabolic capacity of older adults, drug residual effects are prevalent, which lead to accidents. 16 These events increase the associated medical cost and mortality rate. 17
Nonpharmacologic approaches may have efficacy similar to that of sleeping pills but with fewer adverse effects, 16,18 –20 such as foot thermal therapy. 21 The diurnal regulation of skin and core body temperature are associated with the sleep cycle. During the daytime, when the core body temperature increases, people awake. During habitual sleep, the core body temperature decreases considerably, causing sleepiness. The decrease in core body temperature is associated with distal vasodilatation. When the blood vessels in the distal skin of the extremities dilate, heat from the core body is transferred to the distal skin, thus increasing the distal skin temperature and dissipating heat. 22,23 Therefore, a decrease in core body temperature accompanied by an increase in distal skin temperature is closely associated with sleep onset. 24 The difference between core body and peripheral temperatures, known as the distal-proximal skin temperature gradient, is the best physiological predictor of rapid sleep onset. 25 Before bedtime, a footbath or other passive heating methods for the foot can increase the distal extremity temperature without affecting the core body temperature, resulting in reduced sleep latency, prolonged sleep time, and reduced wakefulness during sleep. 26
Some studies have confirmed that the passive heating of the lower extremities improves sleep quality in older adults; 27 –34 however, other studies have reported opposite results. 35 –37 In these studies, the temperature, duration, and heating height of foot thermal therapy were not assessed using any standardized methods. Because of aging and body degradation, the heat perception and conduction velocity differ between older and younger individuals. 38,39 Different temperatures, durations, and heating heights may affect sleep quality in older adults. Hence, this systematic review and meta-analysis was aimed to access the effects of temperature, duration, and heating height of foot thermal therapy on the subjective and objective sleep quality of older adults.
Materials and Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and registered with the PROSPERO database. The PRISMA checklist is contained in Supplementary Data.
Search strategy and selection criteria
The following eight databases were searched without any restriction for the date or language to identify all relevant articles published till July 2023: PubMed, Embase, CINAHL, Airiti, Web of Science, MEDLINE, EBSCO, and Cochrane. The keywords and MeSH terms used were: thermal therapy (or footbath, footbath*, foot bath, bath, bath*, feet warming, topical warming, local hyperthermia, thermotherapy, or lower extremity warming) and sleep quality (or insomnia, sleep initiation, or maintenance disorders).
The inclusion criteria were as follows: (1) participants with a mean age ≥60 years; (2) interventions that included foot thermal therapy; (3) a control group that received routine care but no thermal therapy; (4) outcome measurements that assessed sleep quality; and (5) the studies utilized randomized controlled trials (RCTs) or quasi-experimental studies. Exclusion criteria included: (1) case reports, conference abstracts, review studies, systematic reviews, and meta-analysis studies; and (2) studies in which interventions were combined with other modalities or administered for other body parts.
Study selection and quality appraisal
All search results were recorded in the EndNote 20 citation manager and independently reviewed by two reviewers. Decisions were based on the predefined inclusion and exclusion criteria, with recorded reasons for exclusions. The Joanna Briggs Institute (JBI) critical appraisal tools were used to evaluate the identified studies. The 13-item checklist for RCTs and the 9-item checklist for quasi-experimental studies were applied according to the study design. Each item on the checklists is scored as 1 (yes) or 0 (no, unclear, or not applicable), 40 and the following criteria were set in this study: if >70% of items have a “yes” score, the risk of bias of the study will be low; if 50%–69%, moderate; and if <49%, high. 40,41 Hence, the RCTs with a score of ≥6 and quasi-experimental studies with a score of ≥4 were included in their analysis. All included studies were determined by agreement between the two reviewers. Any disagreement was resolved through discussion; if needed, a third reviewer was included to achieve consensus. 40
Data synthesis and statistical analysis
Data were extracted and synthesized on the following categories: author name, publication year, study design, participant characteristics, interventions, assessment tools, and outcomes. 42 The meta-analysis was conducted using RevMan version 5.4. To ensure that the subjective sleep quality scores were consistent across all included studies, the scores were reversed in eight of the included studies 27,28,30,32 –36 and then combined; thus, higher scores indicated better sleep quality in all studies. Because different assessment tools and scoring methods were used in the studies, the sleep quality data were presented in terms of standardized mean difference (SMD) and 95% confidence interval (CI). The effect sizes were estimated using SMD values. Effect sizes of 0.2, 0.5, and 0.8 were considered to represent small, medium, and large effects, respectively. The statistical significance was determined by a p-value of <0.05. 43,44
Heterogeneity was evaluated using Cochrane's Q test and I 2 test. If heterogeneity was found (p-value of Q test <0.05 and I 2 > 50%), a random-effect model was used for statistical analysis; otherwise, a fixed-effect model was used. 42 If a high degree of heterogeneity was found, a sensitivity analysis was performed to eliminate unsuitable articles. 45 If more than 10 studies had heterogeneity, funnel plots were used to assess the publication bias, and the symmetry of the funnel plots was examined using Egger's regression test, which was conducted using JASP version 0.16.4. A p < 0.05 indicated statistical significance, which implied publication bias. 46 In addition, subgroup analyses were conducted to access the effects of different temperatures, durations, and heating heights of foot thermal therapies on the sleep quality of older adults.
Results
Design and participants of the included studies
Figure 1 presents the flowchart for study selection. A total of 5399 published articles were identified. After 612 duplicates were excluded, 4787 articles were reviewed. Irrelevant articles were removed after their titles and abstracts were examined. In total, 149 potential studies were retrieved for full-text analysis. Based on the inclusion and exclusion criteria, 15 studies were selected for quality evaluation based on the JBI critical appraisal tools (Table 1). Of the 15 studies, four were at a high risk of bias and were eliminated. Finally, 11 studies were included in this systematic review and meta-analysis.

Study selection flow chart. EBSCO, Academic Search Complete; WOS, Web of Science.
Methodological Quality of the Included Studies
Questions in the JBI Scale:
1. Checklist for RCTs: (1) Was true randomization used for assignment of participants to treatment groups? (2) Was allocation to treatment groups concealed? (3) Were treatment groups similar at the baseline? (4) Were participants blind to treatment assignment? (5) Were those delivering treatment blind to treatment assignment? (6) Were outcomes assessors blind to treatment assignment? (7) Were treatment groups treated identically other than the intervention of interest? (8) Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analyzed? (9) Were participants analyzed in the groups to which they were randomized? (10) Were outcomes measured in the same way for treatment groups? (11) Were outcomes measured in a reliable way? (12) Was appropriate statistical analysis used? (13) Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial?
2. Checklist for quasi-experimental studies: (1) Is it clear in the study what is the “cause” and what is the “effect” (i.e., there is no confusion about which variable comes first)? (2) Were the participants included in any comparisons similar? (3) Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? (4) Was there a control group? (5) Were there multiple measurements of the outcome both pre and post the intervention/exposure? (6) Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analyzed? (7) Were the outcomes of participants included in any comparisons measured in the same way? (8) Were outcomes measured in a reliable way? (9) Was appropriate statistical analysis used?
JBI, Joanna Briggs Institute; NA, not applicable; RCT, randomized controlled trial.
Of the 11 studies, 6 were RCTs, 27,28,32,35 –37 and 5 were quasi-experimental studies. 29 –31,33,34 The included studies were conducted in China (n = 3), Iran (n = 3), Korea (n = 2), Japan (n = 1), and Taiwan (n = 2), respectively. The years of publication ranged from 2012 to 2021. The minimum sample size was 6, 37 and the maximum sample size was 140. 30 The average age range of the participants was 60–82 years. Of the studies, two included only men 30,32 and three had a higher proportion of women; 29,31,34 in the remaining studies, the sex ratio (men/women) was ∼1:1 (Appendix A1).
Nature of interventions
Foot thermal therapy was administered through a footbath in all of the 11 included studies. The temperature of heating ranged from 37°C to 42°C. In only one study, 34 the minimum temperature during the procedure was 36°C. The minimum duration of passive heating was 10 min, whereas the maximum duration was 40 min. The heating height was at the ankle, 10 cm above it, or 20 cm above it. Foot thermal therapy was administered 1–2 h before bedtime (n = 11). The shortest intervention duration was 1 day, whereas the longest intervention duration was 3 months (Appendix A1).
Tools used to assess sleep quality
Sleep quality was assessed using subjective self-report questionnaires or objective physiological measures. Subjective self-report tools were used in nine studies, including the PSQI (n = 5), Morning Questionnaire (n = 2), VSH (n = 1), and 10-cm visual analog scale (n = 1). Objective physiological evaluation tools included PSG (n = 3) and ATG (n = 2). In most studies, a single method was used to assess sleep quality; by contrast, in three studies, a combination of subjective and objective methods was applied to assess sleep quality.
Effects of foot thermal therapy on subjective sleep quality
Of the 11 studies, 9 reported the effects of foot thermal therapy on subjective sleep quality: positive effects (n = 7) and no effects (n = 2). A meta-analysis of these nine studies revealed a high degree of heterogeneity (Q = 39.17, p < 0.001; I 2 = 74); sensitivity analyses were performed using the heterogeneity test. Substantial heterogeneity was noted in the study by Xiong; 33 thus, this study was deemed unsuitable and excluded from the meta-analysis. Consequently, heterogeneity decreased significantly (Q = 10.22, p = 0.333; I 2 = 12); moreover, the Egger's regression test (p = 0.440) revealed no publication bias.
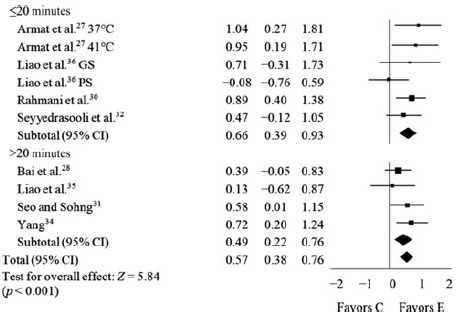
Using a fixed-effect model, data from the remaining eight studies were analyzed; the results revealed an effect size of 0.57 (95% CI: 0.38 to 0.76; p < 0.001), indicating that foot thermal therapy is moderately effective for enhancing the subjective sleep quality of older adults. Hence, subgroup analyses were further performed to determine the optimal values of the therapeutic parameters for older adults as shown below.
Effects of temperature
Of the eight studies, one study 28 did not indicate the temperature of heat therapy and one study 34 included a temperature range larger than that could be categorized. After excluding these two studies, the subgroup analysis was conducted among the remaining six studies, which were grouped as 40°C (n = 3; 123 subjects) and 41°C–42°C (n = 3; 125 subjects); the effect sizes for these two groups were 0.66 (95% CI: 0.33 to 0.99; p < 0.001) and 0.43 (95% CI: 0.08 to 0.79; p = 0.017), respectively. Regardless of the heating temperature, the therapy markedly improved subjective sleep quality in older adults. The temperature of 40°C had moderate efficacy and was more effective than 41°C–42°C in improving subjective sleep quality (Table 2).
Foot Thermal Therapy Effects on Subjective Sleep Quality

C, control group; CI, confidence interval; E, experimental group; F, fixed-effect model; GS, good sleep; PS, poor sleep; SMD, standardized mean difference.
Effects of duration
All eight studies were included in the subgroup analysis of heating duration and were grouped as ≤20 min (n = 4; 184 subjects) and >20 min (n = 4; 189 subjects); the effect sizes were 0.66 (95% CI: 0.39 to 0.93; p < 0.001) and 0.49 (95% CI: 0.22 to 0.76; p < 0.001), respectively. Regardless of the heating duration, foot thermal therapy effectively improved subjective sleep quality in older adults. The duration of ≤20 min exhibited moderate efficacy and was more effective than the duration of >20 min in improving subjective sleep quality (Table 2).
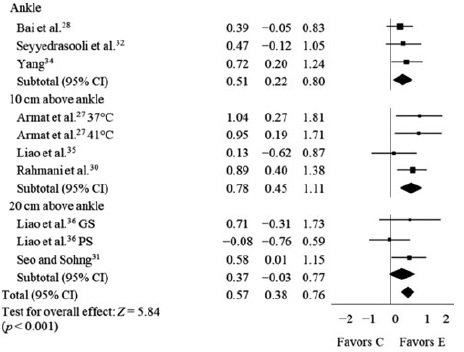
Effects of heating height
All eight studies were included in the subgroup analysis of heating height and were grouped as: at ankle (n = 3; 156 subjects), 10 cm above the ankle (n = 3; 130 subjects), and 20 cm above the ankle (n = 2; 87 subjects); the effect sizes were 0.51 (95% CI: 0.22 to 0.80; p < 0.001), 0.78 (95% CI: 0.45 to 1.11; p < 0.001), and 0.37 (95% CI: −0.33 to 0.77; p = 0.072), respectively. Foot thermal therapy administered at ankle and 10 cm above it effectively improved subjective sleep quality in older adults and had moderate efficacy. However, the efficacy of therapy administered 10 cm above the ankle was slightly higher compared with therapy administered at ankle (Table 2).
Effects of foot thermal therapy on objective sleep quality
Of the 11 included studies, objective methods were used to assess sleep quality in 5 studies (PSG, n = 3; ATG, n = 2). The sleep parameters assessed in this meta-analysis were sleep latency, sleep efficiency, and total sleep time. Among the five studies, total sleep time (n = 2), sleep latency (n = 1), and sleep efficiency (n = 1) were reported as effective. Because foot thermal therapy was administered 10 cm above the ankle in only one study, 35 subgroup analysis could not be performed for heating height. The subgroup analyses were performed only for heating temperature and duration.
Effects on sleep latency
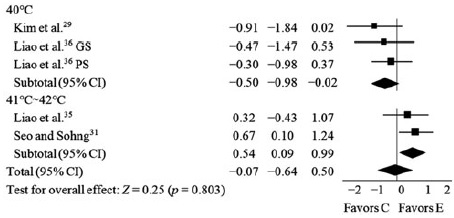
Four out of the five studies measured sleep latency and a heterogeneity among studies was found (Q = 11.22, p = 0.024; I 2 = 64); however, since less than 10 studies were included, funnel plot and Egger's regression test could not be used to examine publication bias. A random-effect model showed an effect size of −0.07 (95% CI: −0.64 to 0.50; p = 0.803). In the subgroup analysis of heating temperature, the four studies were grouped as 40°C (n = 2; 43 subjects) and 41°C–42°C (n = 2; 79 subjects); the effect sizes were −0.55 (95% CI: −0.98 to −0.02; p = 0.039) and 0.54 (95% CI: 0.09 to 0.99; p = 0.020), respectively (Table 3). The subgroup analysis on duration did not show any significant differences. Foot thermal therapy before bedtime did not lead to a significant improvement in the sleep latency of older adults. Nonetheless, subgroup analyses indicated a considerable improvement in sleep latency, specifically when the intervention was conducted at a temperature of 41°C– 42°C; this effect was of moderate efficacy. Conversely, a temperature of 40°C exerted a moderate adverse effect on sleep latency.
Temperature of Foot Thermal Therapy Effects on Sleep Latency
C, control group; CI, confidence interval; E, experimental group; GS, good sleep; PS, poor sleep; R, random-effect model; SMD, standardized mean difference.
Effects on sleep efficiency
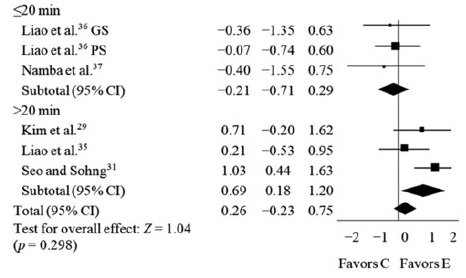
All five studies measured sleep efficiency, and a heterogeneity among studies was found (Q = 10.92, p = 0.053; I 2 = 54); however, since less than 10 studies were included, funnel plot and Egger's regression test could not be used to examine publication bias. A random-effect model was used, and the effect size was 0.26 (95% CI: −0.23 to 0.75; p = 0.298). The subgroup analysis on temperature did not show any significant differences. In the subgroup analysis of heating duration, five studies were grouped as ≤20 min (n = 2; 29 subjects) and >20 min (n = 3; 85 subjects); the effect sizes were −0.21 (95% CI: −0.71 to 0.29; p = 0.418) and 0.69 (95% CI: 0.18 to 1.20; p = 0.008), respectively (Table 4). Foot thermal therapy before bedtime did not result in a significant improvement in the sleep efficiency of older adults. Nonetheless, subgroup analyses revealed a considerable improvement in sleep efficiency, specifically when the intervention was conducted for >20 min; this effect was of moderate efficacy.
Duration of Foot Thermal Therapy Effects on Sleep Efficiency
C, control group; CI, confidence interval; E, experimental group; F, fixed-effect model; GS, good sleep; PS, poor sleep; SMD, standardized mean difference.
Effects on total sleep time
All five studies measured total sleep time, and a heterogeneity among studies was found (Q = 11.39, p = 0.044; I 2 = 56); however, since less than 10 studies were included, funnel plot and Egger's regression test could not be used to examine publication bias. A random-effect model was used, and the effect size was 0.29 (95% CI: −0.20 to 0.79; p = 0.027) (Table 5). The subgroup analysis results for neither temperature nor duration reached statistical significance. Foot thermal therapy before bedtime did not improve total sleep time in older adults.
Foot Thermal Therapy Effects on Total Sleep Time
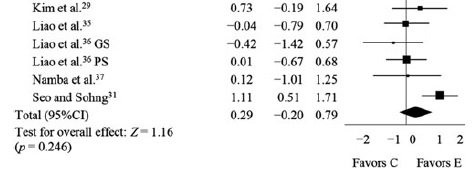
C, control group; CI, confidence interval; E, experimental group; F, fixed-effect model; GS, good sleep; PS, poor sleep; SMD, standardized mean difference.
Discussion
Passive heating or a foot bath before bedtime is often used to improve sleep quality in patients with insomnia. 47,48 Insomnia in older adults is a complex problem. Because of the natural aging of the body, the outcomes of the same intervention measures may differ between older and younger individuals. The administration of foot thermal therapy 1–2 h before bedtime significantly improved subjective sleep quality in older adults; however, no significant effects were noted on objective sleep quality. Such inconsistency between subjective and objective outcomes is common in both patients with insomnia and healthy individuals. 49,50 The differences may be associated with physiological functioning and psychosocial factors. 51 –53 In the absence of other disorders, insomnia does not necessitate admission to a sleep center or the use of objective physiological instruments for diagnosis. 49 Therefore, sleep quality, whether subjective or objective, is equally important in clinical settings and can serve as a reference for clinical professionals.
Yamamoto et al. 54 reported that the passive heating of lower extremities decreases sympathetic nerve activity but increases parasympathetic nerve activity, which in turn relaxes the body and mind, alleviates fatigue, and increases the pain threshold. 55 Aging may be accompanied by feelings of chronic discomfort that affect sleep quality. 9 Increasing parasympathetic activity and the pain threshold through foot thermal therapy can improve sleep quality in these individuals. This study noted that a heating temperature of 40°C–42°C and a duration of 10–40 min can improve subjective sleep quality in older adults. When people are about to sleep, warm-sensitive neurons (WSNs) in the hypothalamic preoptic area are automatically discharged; passive heating of the lower extremities stimulates these WSNs, thereby promoting sleep. 56 The passive heating of lower extremities can also dilate distal blood vessels, which decreases core body temperature, thus shortening sleep latency. 39,48 The most common sleep problems in older adults are difficulties in falling asleep and maintaining sleep; 8,9 the passive heating of lower extremities can reduce these problems.
This meta-analysis revealed that foot thermal therapy exerted no significant effect on objective sleep quality of older adults; this may be attributed to the physical decline due to aging. Raymann et al. 39 confirmed that the passive heating of lower extremities before bedtime shortens sleep latency in older adults without sleep disturbances, but not in those with sleep disturbances. This might be because older adults with sleep disturbances have poorer peripheral circulation and temperature perception than older adults without sleep disturbances and younger individuals. The older adults with sleep disturbances showed an attenuated increase in foot temperature after the passive heating of the lower extremities, thus failing to promote sleep. 23,39 Among the studies included in our meta-analysis, two did not indicate the sleep status of participants before the intervention. In two other studies, at least 50% of the participants had sleep disturbances; in one study, all participants had sleep disturbances. Therefore, the passive heating of the lower extremities might not have improved objective sleep quality of participants in this meta-analysis.
The results of subgroup analysis indicated that a temperature of 41°C–42°C effectively shortened sleep latency; this might have been due to the maximum vasodilatation of the skin, which reached a plateau after 25–30 min of heating, resulting in the maximum blood flow. However, if the heating duration is extended to 50 min, blood flow will decrease in some individuals, leading to the occurrence of the rebound phenomenon. 57 Because of aging, vasodilation is poorer in older individuals than in younger individuals. 58 Aging reduces sensitivity to nitric oxide, a key vasodilator, or causes a decrease. A rapid increase in skin temperature or slight pain sensation due to heating may increase the activity of nitric oxide synthase, which increases the level of nitric oxide, thus enhancing vasodilation. 59,60 As mentioned earlier, heat perception and conduction velocity may differ between older and younger individuals.
In this meta-analysis, the effectiveness of foot thermal therapy at 40°C in promoting objective sleep onset latency appears to be suboptimal and may even worsen, possibly due to the duration of footbath exposure. In the study of Zhao et al., 61 model data suggested that it took ∼24 min of soaking at 42°C to induce sweating, whereas at 40°C, it might take around 50 min. The study suggested that the optimal footbath duration should be determined by the time required for sweating to occur. 61 An insufficient soaking time at 40°C may not achieve the appropriate temperature difference, potentially hindering the initiation of sleep onset. In other words, the footbath duration and temperature at 40°C may not reach the optimal conditions for promoting sleep onset latency. It might require a longer duration or higher temperature to induce the desired physiological responses and facilitate the initiation of sleep. Therefore, further research is needed to explore the optimal footbath conditions and their impact on sleep onset latency to gain a better understanding of how to effectively utilize foot thermal therapy to improve sleep quality.
In most of the included studies, a constant temperature was maintained for foot thermotherapy throughout the study. Four studies 27,28,30,37 did not mention whether the temperature was constant; in these studies, the soaking time was relatively short. Further experiments should be conducted to investigate whether this factor influences sleep.
Finally, it was further noted that heating up to the ankle or 10 cm above the ankle, but not 20 cm above the ankle, significantly improved sleep quality. Although the heating of the extremities accelerates sleep, heating which part of the skin exerts the strongest positive effects remains unknown. 39 The optimal temperature, duration, and heating height of foot thermal therapy must be applied.
Limitations
This study has some limitations. First, some of the studies analyzed in this systematic review and meta-analysis included participants of a single sex; sex imbalance may introduce bias. Second, all included studies were conducted in Asia; therefore, the findings may not be generalized to populations other than the Asian population. Finally, the use of foot thermal therapy for sleep improvement differs between older adults with sleep disturbances and those without sleep disturbances; moreover, various temperatures and heating heights differentially affect therapeutic outcomes. Further experimental studies are needed for an in-depth analysis.
Conclusion
The administration of foot thermal therapy at a temperature of 40°C–42°C for 10–40 min at the ankle or 10 cm above the ankle 1–2 h before bedtime may substantially improve subjective sleep quality in older adults. Specifically, the optimal therapeutic parameters were a temperature of 40°C, a duration of ≤20 min, and a heating height of 10 cm above the ankle. A temperature of 41°C–42°C appeared to be the most effective for improving sleep latency; however, data on the optimal heating height were limited. Therefore, further studies are necessary. Based on the study findings, the authors recommend that clinical health care providers offer or instruct older adults to use foot thermal therapy 1 h before bedtime to promote sleep quality. During the therapy, a temperature of 40°C should be used, and the soaking time should not exceed 20 min, with the feet immersed up to approximately 10 cm above the ankles. If they have trouble falling asleep, the temperature can be increased to 41°C–42°C.
Footnotes
Authors' Contributions
All authors meet the criteria for authorship, have approved the final article, and all those entitled to authorship are listed as authors. C.-S.J.: Conceptualization, data curation, formal analysis, and article preparation. K.-M.C.: Conceptualization, data curation, formal analysis, methodology, and article preparation. F.B.: Data validation and article reviewing and editing.
Systematic Review Registration
This study was registered in the PROSPERO database (CRD42022383460).
Author Disclosure Statement
The authors declare no conflict of interests.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Appendix
Appendix A1. Summary of the Studies
| Author (year) Country | Study design; population; use of psychotropic agents | Participants number (age range or mean); female % | Intervention a | Assessment tools | Outcome |
|---|---|---|---|---|---|
| Armat et al. 27 (2021) Iran | RCT; Older adults; Excluded |
Exp1: 15 (≥60); F = 67; Exp2: 15 (≥60); F = 80; Con: 15 (≥60); F = 40 |
Temperature: 37°C and 40°C Duration: 10 min for 2 weeks. Heating height: 10 cm above ankle |
PSQI | Improvement in the PSQI score |
| Bai et al. 28 (2017) China | RCT; Older adults with CHF; Excluded |
Exp: 40 (67); F = 63 Con: 40 (64); F = 55 |
Temperature: NR Duration: 20–30 min Heating height: ankle |
PSQI | Improvement in the PSQI score |
| Kim et al. 29 (2016) Korea | QE; Older adults; Not excluded |
Exp: 10 (82); F = 90 Con: 10 (77); F = 70 |
Temperature: 40°C Duration: 30 min for 4 weeks. Heating height: 20 cm above ankle |
ATG | Improvement in TST and SE (highly effective in older adults with poor sleep quality) |
| Liao et al. 35 (2008) Taiwan | RCT (crossover); Older adults; Excluded |
Exp: 15 (67); F = 60 | Temperature: 41°C Duration: 40 min for 1 day Heating height: 10 cm above ankle |
PSG MQ 10 cm VAS |
No significant improvement in PSG or QNR (MQ and 10 cm VAS) |
| Liao et al. 36 (2013) Taiwan | RCT; Older adults; Excluded |
Exp1: 8 (57); F = 63 Exp2: 17 (61); F = 47 |
Temperature: 40°C ± 0.5°C Duration: 20 min for 1 day Heating Height: 20 cm above ankle |
PSG MQ 10 cm VAS |
No significant improvement in PSG or QNR (MQ and 10 cm VAS) |
| Namba et al. 37 (2012) Japan | RCT (crossover); Older adults; Not excluded |
Exp: 6 (65); F = 50 | Temperature: 40°C Duration: 10 min for 1 day Heating height: ankle |
PSG Subjective self-report |
No significant improvement in PSG |
| Rahmani et al. 30 (2016) Iran | QE; Older adults with ACS; Excluded |
Exp: 35 (61); F = 0 Con: 35 (61); F = 0 |
Temperature: 40°C Duration: 10 min for 3 days Heating height: 10 cm above ankle |
VSH | Improvement in the VSH score |
| Seo and Sohng 31 (2011) Korea | QE; Older adults; Excluded |
Exp: 27 (80); F = 96 Con: 23 (77); F = 83 |
Temperature: 42°C Duration: 30 min for 3 days Heating height: 20 cm above ankle |
ATG 10 cm VAS |
Improvement in the10 cm VAS score and ATG (TST, SL) |
| Seyyedrasooli et al. 32 (2013) Iran | RCT; Older adults; Not excluded |
Exp: 23 (68); F = 0 Con: 23 (67); F = 0 |
Temperature: 41°C–42°C Duration: 20 min for 6 weeks. Heating height: ankle |
PSQI | Improvement in the PSQI score |
| Xiong 33 (2018) China | QE; Older adults with COPD; Not excluded |
Exp: 77 (68); F = 47 | Temperature: 40°C Duration: 30 min for 4 weeks. Heating height: NR |
PSQI | Improvement in the PSQI score |
| Yang 34 (2012) China | QE; Older adults; Not excluded |
Exp: 30 (70); F = 77 | Temperature: 36°C–42°C Duration: 15–30 min for 3 months Heating height: ankle |
PSQI | Improvement in the PSQI score |
With the exception of Liao's study, 36 all other original studies in this research presented temperature measurements as whole numbers without decimal places.
ACS, acute coronary syndrome; ATG, actigraphy; CHF, congestive heart failure; Con, control group; COPD, chronic obstructive pulmonary disease; Exp, experimental group; MQ, morning questionnaire; NR, not reported; PSG, polysomnography; PSQI, Pittsburgh Sleep Quality Index; QE, quasi-experimental study; QNR, questionnaire; RCT, randomized controlled trial; SE, sleep efficiency; SL, sleep latency; TST, total sleep time; VAS, visual analog scale; VSH, Verran and Snyder-Halpern Sleep Scale.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.