
Abstract
Introduction:
The concept of acupoints is a key defining feature of acupuncture, yet the scientific basis of acupoints remains unclear. In recent years, there has been an emerging body of animal studies demonstrating an association between cutaneous sensitivity and visceral pathophysiology, through which acupoints over the skin are sensitized in pathologic conditions. Several studies with humans have also been conducted to assess whether the sensitivity of acupoints is distinct in healthy versus clinical populations. However, no systematic review has been conducted to collate and synthesize the status and quality of human studies on this topic.
Methods:
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA). Literature search was performed by combining variations of search terms related to acupoints and pain sensitivity in PubMed, EMBASE, and Alt HealthWatch (EBSCOHost). Screening of titles and abstracts and review of full-text articles for eligibility were performed by two independent investigators. Using a predefined template, information on subject characteristics, pathologic conditions, names of assessed acupoints, and relevant main findings were extracted from the included studies. The methodological quality of included studies was assessed using a modified Newcastle–Ottawa Scale (NOS) for case–control studies. A quality assessment checklist was also developed by the present authors to examine the quality of reporting of experimental variables that were considered important for evaluating acupoint sensitivity.
Results:
A total of 3453 studies were identified from the database search, of which 11 met the eligibility criteria to be included in this review. Six studies examined the mechanical sensitivity of body acupoints, and the remaining five studies examined the mechanical sensitivity of auricular points. Overall, findings suggest that the sensitivity of acupoints may be distinct in healthy versus clinical populations. However, there were various potential sources of bias and substantial heterogeneity across included studies in clinical conditions and acupoints.
Conclusion:
There is at present insufficient evidence to support or refute that acupoints in humans are sensitized in pathologic conditions. There were various methodological issues, including small sample size and poor reporting of experimental design and variables, which limit the ability to draw a definitive conclusion on this topic. It is also largely unclear whether it is the general body regions rather than specific acupoints that may be sensitized, as most studies did not include nonacupoint location(s) for comparison. Thus, further rigorous research is warranted.
Introduction
Acupuncture is defined by the National Center for Complementary and Integrative Health as “a technique in which practitioners stimulate specific points on the body—most often by inserting thin needles through the skin.” 1 Accordingly, acupuncture is theorized to “work” or provide therapeutic benefits through stimulation of specific body locations, collectively referred to as acupuncture points or acupoints. 2,3 The concept of acupoints is thus fundamental to the theory and practice of acupuncture. However, to date, the scientific basis of acupoints remains largely unclear and controversial. 4 –6 Despite previous research efforts to identify anatomical correlates of acupoints, there is a lack of scientific clarity and conclusive evidence supporting systematic differences between acupoint and nonacupoint locations. 7 There is also conflicting clinical evidence as to whether the therapeutic outcomes of acupuncture depend on the specific points (e.g., verum vs sham points) that are stimulated. 7 Given that the concept of acupoints is central to the very definition of acupuncture, this knowledge gap impacts the understanding of acupuncture as an evidence-based therapy.
In recent years, there has been an emerging body of preclinical animal studies suggesting that acupoints may be viewed as dynamic, functional entities whose physiological characteristics (e.g., pain sensitivity) are associated with corresponding internal or visceral pathophysiology. 8 Findings from these studies demonstrate that under experimental conditions of visceral diseases (e.g., colitis, gastritis, cystitis), the skin overlying certain acupoints is sensitized. 9 –14 The sensitized points in these studies have been shown to exhibit various signs of cutaneous neurogenic inflammation, including increased pain sensitivity (e.g., mechanical hyperalgesia). 9 –14 These recent research efforts underscore the potential importance of understanding the dynamic physiological states of acupoints in the context of the subject’s health-disease status.
The concept of the inter-relationship between the external (i.e., acupoints on the body surface) and internal aspects (i.e., visceral organs) of the body is important for the practice and theory of acupuncture. 9 In clinical practice, manual palpation is frequently performed by acupuncturists to identify locations of tender points for both diagnostic and therapeutic purposes. 5 Based on traditional theories of acupuncture, there are approximately 361 acupoints on the body surface (“body acupoints”), which are connected to the Zang-Fu organs (i.e., internal organ systems in Traditional Chinese Medicine, TCM). 3 Through such “viscero-somatic” connections, specific acupoints over the skin are posited to be sensitized in pathologic conditions, in a phenomenon referred to as acupoint sensitization. 8 These connections are thought to be bidirectional, such that stimulation of sensitized acupoints is, in turn, more effective in treating the corresponding conditions. 15,16 Thus, the identification of tender or sensitized points is important in clinical practice. In addition to body acupoints, acupoints on the external ear (“auricular acupoints”) are theorized to reflect the health-disease status of corresponding parts of the whole body, and sensitized auricular acupoints are often selected for stimulation in auricular acupuncture (AA) treatment. 17,18
Acupoint sensitization may represent one traditional explanation of acupuncture that is congruent with the findings of prior preclinical studies and may provide a possible explanatory model for understanding the scientific basis of acupoints. To investigate the validity of acupoint sensitization in humans, several studies have been conducted to assess and compare acupoint sensitivity in healthy and clinical populations. Some of these studies have been described in a recent narrative review on the topic of acupoint sensitization and have suggested that sensitivity (e.g., pressure pain threshold, PPT) of specific acupoints is distinct in healthy versus clinical populations. 8 However, to date, the scope and quality of existing literature on this topic have not been systematically reviewed. Therefore, we conducted this systematic review to collate, synthesize, and critically evaluate existing literature addressing the question of whether pain sensitivity of specific acupoints is altered in pathologic visceral conditions. We also assessed the quality of included studies to identify any gaps and deficiencies in the existing literature and provide recommendations for future clinical studies in this area.
Methods
Search strategy
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA). 19 The PRISMA checklist for this review can be found in Supplementary Table S1. The following databases were searched from database inception to September 2021: PubMed, EMBASE, and Alt HealthWatch (EBSCOHost). The search was performed by combining variations of search terms and subject headings related to the concept of acupoint and pain sensitivity. The detailed search strategy with search terms and subject headings used across the three databases can be found in Supplementary Table S2.
Study selection process
All resulting titles and abstracts from the search were independently screened by two authors (EY and DMV), and any disagreement was resolved through discussion. Studies were eligible for inclusion if they met the predefined inclusion and exclusion criteria, structured according to the PICOS framework, which stands for Population, Intervention, Comparison, Outcomes, and Study design, respectively.
Population
The population of interest in this review included human adults with pathologic visceral conditions. No restriction was placed on the different types of visceral conditions. Nonhuman research or studies involving preclinical animal models were excluded from the review.
Intervention
Intervention was considered not applicable in the context of this review. Studies were neither included nor excluded on the basis of the intervention.
Comparison
Comparison or control groups included healthy adults without pathologic conditions. Studies without a healthy control group for comparison were excluded.
Outcomes
Studies involving pain sensitivity assessment of acupoints in healthy versus clinical populations were included. Studies were excluded if they had an irrelevant outcome (e.g., pain assessment sites did not include acupoint locations).
Study design
The eligible study design was case–control. Studies were excluded if they did not provide a comparison between healthy and clinical populations.
In addition, studies were excluded if they were non-English and/or had insufficient original data (e.g., protocol, case reports, conference abstracts).
Data extraction
Two authors (E.Y. and E.G.) independently extracted data from included studies using a predefined template. Any discrepancies were resolved through discussion. The data extraction template included the following: (1) first author name, publication year, and the country in which the study was conducted, (2) description of the study sample (i.e., case and control) and sample size, (3) name(s) of assessed acupoint(s) and any other assessed locations on the body, (4) relevant outcome measures, (5) data collection procedures, including the method or device used for pain assessment of acupoints, (6) statistical analysis, and (7) relevant main findings.
Quality assessment
The methodological quality of included studies was assessed independently by two authors (E.Y. and D.M.V.) using two types of instruments, and any discrepancies were resolved through discussion. First, a modified Newcastle–Ottawa Scale (NOS) was used to assess the quality of the case–control study design. The NOS is a commonly used risk-of-bias assessment tool for evaluating the quality of observational studies, including case–control studies. 20 It consists of the following categories of items: selection of cases and controls, comparability of cases and controls, and ascertainment of exposure. Items related to ascertainment of exposure were excluded as they were considered nonrelevant for the studies included in this review. The criteria used for judgment as “yes (+)” or “no or unclear (−)” for items pertaining to the other two categories are outlined in Supplementary Table S3.
Second, a quality assessment checklist was developed by the present authors to examine the quality of reporting of experimental variables that were considered important for evaluating acupoint sensitivity. The checklist consisted of 13 such items, including environmental factors (e.g., “ambient temperature”), experimental design (e.g., “blinding of the assessor to participant status”), data collection procedures (e.g., “number of assessment[s] per point” and “time interval between assessments”), and pressure algometer specifications (e.g., “algometer tip size”). Pressure algometer is a commonly used tool to assess the PPT or the pressure at which it elicits pain in the subject. There were three possible responses for the checklist: “yes” for items described, “no” for items not described, and “NA” for items not applicable. The complete list of 13 items and criteria used to rate the quality of reporting for each item can be found in Supplementary Table S4. Information provided by the studies relevant to each item can also be found in Supplementary Table S5.
Results
Study selection
Figure 1 shows the PRISMA flow diagram for studies included in this systematic review. This search strategy identified a total of 3453 studies, of which 499 were removed as duplicate citations. During screening of titles and abstracts, 2845 records were excluded as irrelevant studies based on predefined inclusion and exclusion criteria. After assessing the remaining 109 full-text articles for eligibility, 98 were excluded for reasons outlined in Figure 1, and 11 studies met the eligibility criteria to be included in the present review.
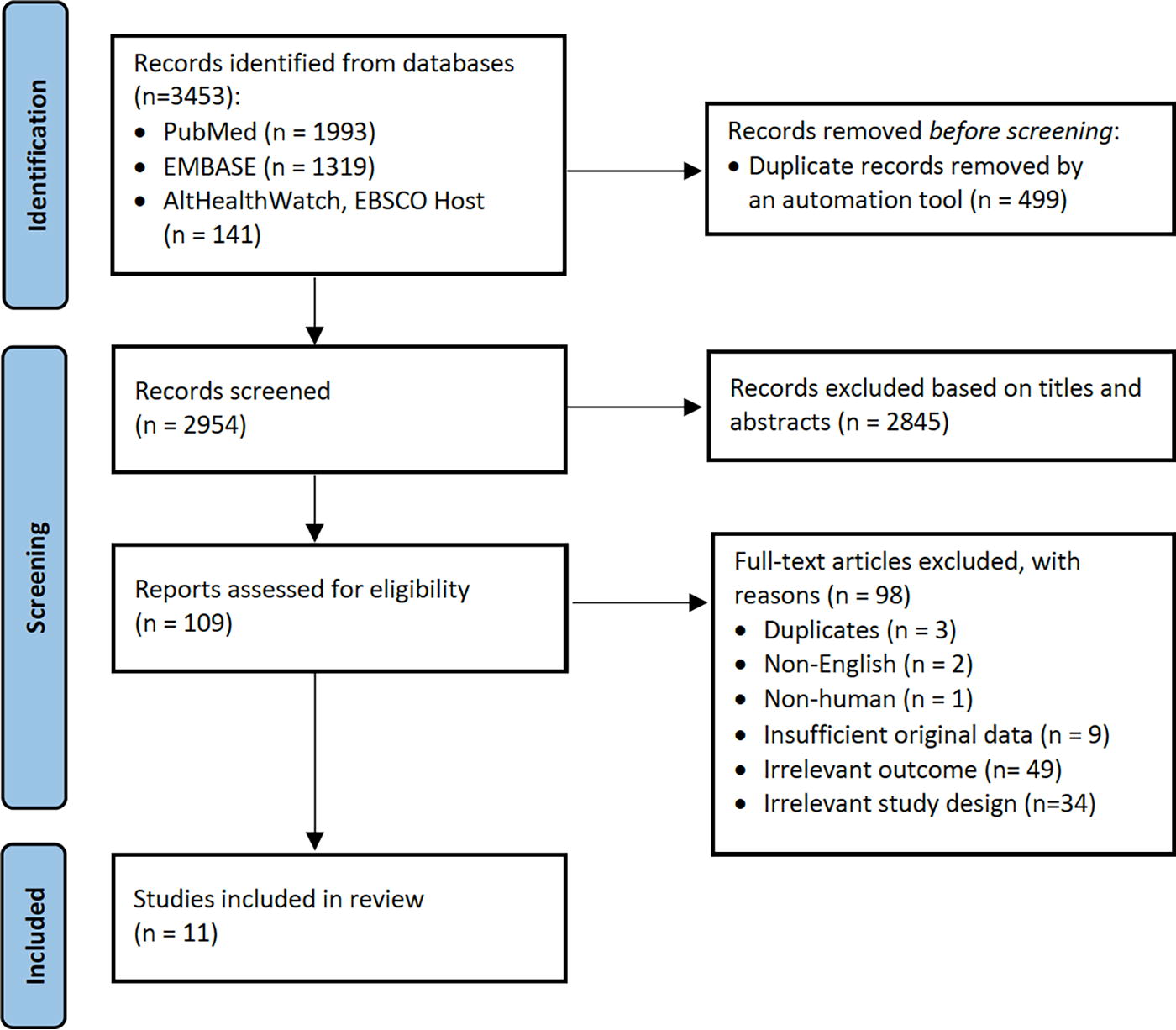
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Study characteristics
All 11 studies assessed the participants’ pain sensitivity in response to mechanical stimuli or pressure (e.g., algometer) applied onto the body surface at the acupoint location(s). However, there was substantial heterogeneity in terms of assessed acupoint locations and clinical conditions. Of these studies, six examined body acupoints 21 –26 and five examined auricular acupoints. 27 –31 In reporting the results, we have categorized the tables and summary of main findings according to acupoint “type” (i.e., body or auricular).
Body acupoints
The characteristics of studies pertaining to body acupoints are presented in Table 1. Among these studies, five clinical conditions were examined as follows: (1) functional dyspepsia 21,23 ; (2) pelvic inflammatory disease 22 ; (3) dysmenorrhea 24 ; (4) gastric ulcer 25 ; and (5) premenstrual syndrome. 26 The number of subjects ranged from 12 to 44 for both groups (i.e., cases and controls).
Characteristics of Included Studies Evaluating Body Acupoints
For acupoint SP8, PPT was assessed on the most tender point in the vicinity around standard position of SP8.
HS, healthy subjects; n/a, not available; No., number; PPT, pressure pain threshold; SH, Simhabi; SHK, Simhabikyung; SD, standard deviation; TKM, traditional Korean medicine; VAS, visual analog scale.
Across these studies, a total of 26 acupoints were assessed. Figure 2 shows the approximate locations of these acupoints. With the exception of the CV and GV acupoints, which are located along the anterior and posterior midlines of the body, respectively, all other acupoints were assessed on both the left and right sides of the body in five of the six studies. For one study, while it is likely that the acupoints were assessed bilaterally, this information was not explicitly provided. 25 Only two studies included nonacupoint locations as control points for comparisons. 25,26 A complete list of acupoints in alphanumerical order along with their corresponding study references can be found in the Supplementary Table S6.

Approximate locations of body acupoints assessed in the included studies.
Three types of outcomes were collected for pain sensitivity assessment of acupoints as follows: (1) occurrence rate of tenderness (e.g., the proportion of subjects with tenderness at the assessed point); (2) visual analog scale (VAS) pain intensity score (i.e., the intensity of subject-reported pain in response to the applied pressure at the assessed point); and (3) PPT (i.e., the amount of pressure at which the applied pressure becomes painful for the subject). One study reported the occurrence rate of tenderness 21 and three studies reported measures of PPT, 23,25,26 while the remaining two studies collected all three outcomes. 22,24 Two methods were used to apply pressure and evoke pain for assessment of acupoint sensitivity as follows: (1) manual palpation (i.e., investigator’s fingertip[s] pressure) and (2) pressure algometer. In two studies, data were collected at multiple time points: (1) in Wu et al.’s 22 study, data were collected at three time points (days 0, 7, and 14 after enrollment), and (2) in Chen et al.’s 24 study, data were collected at two time points (menstrual and nonmenstrual periods). In the other four studies, data were collected at one time point.
Auricular acupoints
The characteristics of five studies pertaining to auricular acupoints are presented in Table 2. Among these studies, the following five clinical conditions are examined: (1) metabolic syndrome, 27 (2) type 2 diabetes mellitus, 28 (3) lower urinary tract symptoms, 29 (4) coronary heart disease, 30 and (5) hepatic disorders. 31 Four studies were conducted by the same research team, Suen et al., in Hong Kong, China. 27 –30 The sample size ranged from 20 to 141 for cases and 25 to 141 for controls.
Characteristics of Included Studies Evaluating Auricular Acupoints
HS, healthy subjects; PPT, pressure pain threshold; VAS, visual analog scale; No., number; AA, auricular acupuncture; SD, standard deviation.
There were a total of 12 auricular acupoints assessed across these studies. These acupoints are also commonly referred to the AA zones. Figure 3 shows the approximate locations of these auricular acupoints or AA zones on the ear. In all five studies, auricular acupoints were assessed bilaterally on both ears. For outcome, all five studies used a pressure algometer to assess and compare PPTs of auricular acupoints to that of a reference point on ear. The reference point for these studies was generally defined as another auricular acupoint that was not directly associated with the clinical condition but would account for the individual variability in pain sensitivity across subjects. The data were collected at one time point across all studies.
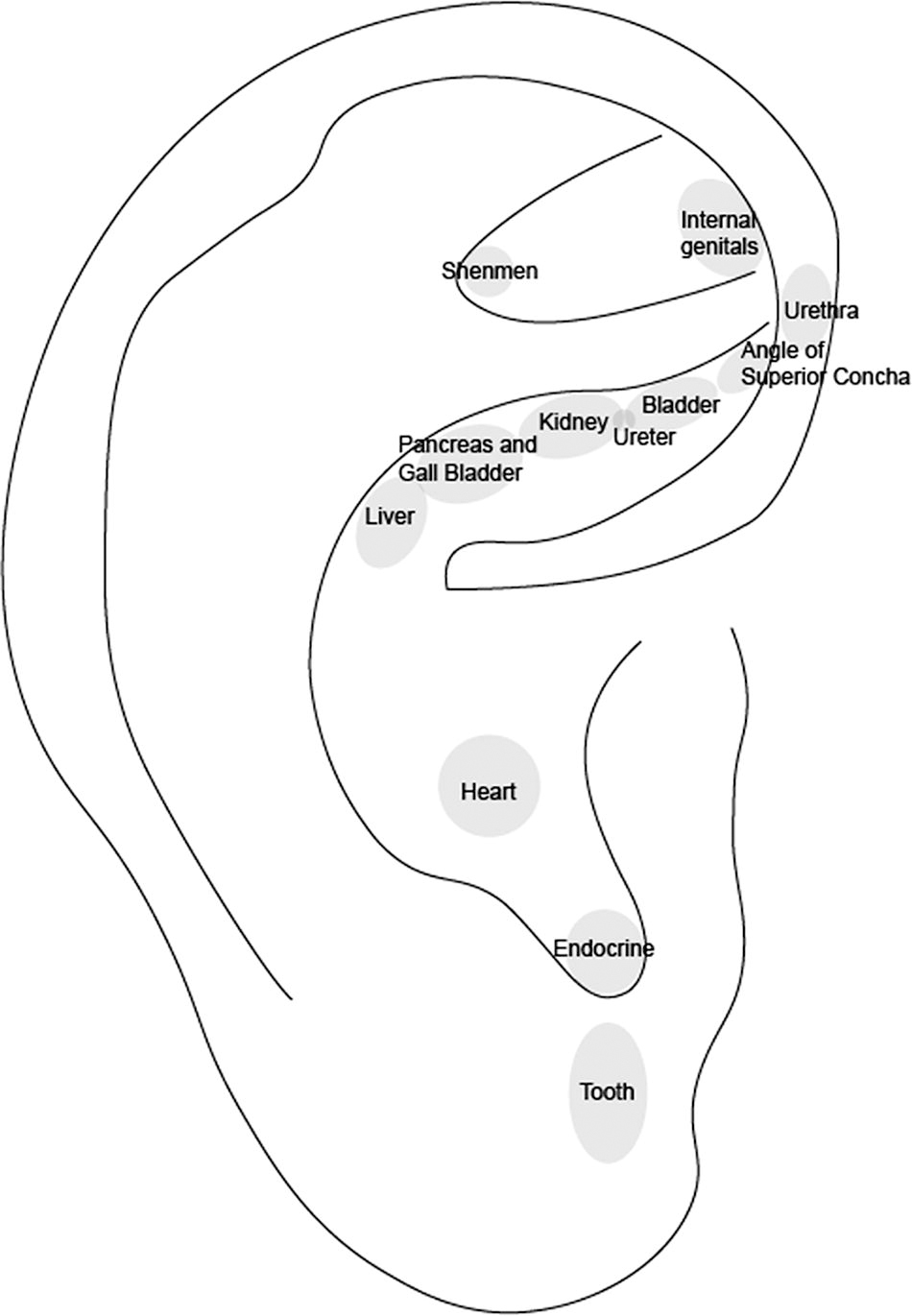
Approximate locations of auricular acupoints assessed in the included studies.
Quality assessment of case–control design
Methodological quality rating of included studies based on a modified NOS is shown in Table 3 and categorized into two sections by acupoint type (i.e., body and auricular acupoints).
Methodological Quality of Included Studies Based on a Modified Newcastle–Ottawa Scale a
Adapted from the Newcastle–Ottawa Scale (NOS) (See Supplementary Material Table S3 for details on criteria used for judgment).
Items: 1. adequate validation of cases; 2. representativeness of the cases; 3. selection of controls; 4. definition of controls; 5. comparability of cases and controls on age; 6. comparability of cases and control on sex; “+” indicates that the study provided relevant and sufficient information, which meets the criteria defined for this item. “−” indicates that the study provided insufficient or unclear information and does not meet the criteria defined for this item.
Body acupoints
Of the six studies pertaining to body acupoints, one study did not provide sufficient information for representativeness of the cases 25 ; two studies did not provide sufficient information regarding validation of cases, 22,25 selection of controls, 22,25 definition of controls, 22,25 and comparability of cases and controls on age 21,25 ; and three studies did not provide sufficient information regarding comparability of cases and controls on sex. 21 –23
Auricular acupoints
As for the five studies pertaining to auricular acupoints, one study did not provide sufficient information regarding comparability of cases and controls on sex. 31 For the remaining studies, sufficient information was provided for all items of the modified NOS quality assessment used in this review.
Quality of reporting of experimental conditions and data collection procedures
Table 4 shows the quality of reporting of experimental variables that were considered important for evaluating acupoint sensitivity. Of the 13 items in this quality assessment checklist, five items involved pressure algometry specifications (i.e., items 9–13) and were considered not applicable (“NA”) if the study did not use a pressure algometer. Item 6 (“sequence of assessments for multiple points”) was considered “NA” if only one acupoint was assessed in the study. Items 7 (“laterality of assessed points”) and 8 (“order of assessment for bilateral points”) were considered “NA” if the assessed point(s) were located along the midline of the body (i.e., on GV or CV meridians). Table 4 is subdivided into two sections, by acupoint type (i.e., body and auricular acupoints).
Quality of Reporting of Experimental Conditions and Data Collection Procedures for Included Studies
Items: 1. information on ambient temperature; 2. participant testing position; 3. blinding of assessor to participant status (case vs. control); 4. number of assessment(s) per point; 5. time interval between assessments; 6. sequence of assessments for multiple points; 7. laterality of assessed points (i.e., left, right, or bilateral points); and 8. sequence of assessments for bilateral points (e.g., left or right first); 9. manufacturer of the pressure algometer used in the study; 10. algometer tip size; 11. algometer tip material; 12. angle of algometer application; 13. rate of algometer application; See Supplementary Material Table S4 for criteria used to judge rating and Supplementary Material Table S5 for information provided in included studies for each item and used for judgment.
N, no (item not described); NA, not applicable (item not applicable); Y, yes (item described).
Body acupoints
The quality of reporting was generally poor across the studies pertaining to body acupoints. There was only one study each providing sufficient information for “ambient temperature” 23 and “blinding of the assessor to participant status (case vs. control).” 26 Information on “participant testing position” was provided by four studies. 21,23,24,26 Items 9–13 were applicable for all studies except for Ko et al.’s 21 study. Information pertaining to item 9 (“algometer manufacturer”) and item 12 (“angle of algometer application”) was provided by all five studies. However, item 10 (“algometer tip size”) was described by three studies, 23,24,26 and items 11 and 13 (“algometer tip material” and “rate of algometer application,” respectively) were described by two studies. 23,26 Four studies described “number of assessment(s) per point” and “time interval between assessments.” 22,23,25,26 As for the “sequence of assessments for multiple points,” none of the studies described the sequence in which the acupoints were assessed, and it is unclear whether there was a method in place to determine the sequence (e.g., same across all subjects or randomized for each subject).
Auricular acupoints
The quality of reporting was very poor for most items across the five studies pertaining to auricular acupoints. None of the studies provided sufficient information regarding “ambient temperature,” “participant testing position,” “algometer manufacturer,” “algometer tip material,” “rate of algometer application,” “number of assessment(s) per point,” “time interval between assessments,” “sequence of assessments for multiple points,” and “sequence of assessments for bilateral points.” Information on “algometer tip size” was provided in only one study. 31 Two studies described “angle of algometer application” 27,28 and four studies described “blinding of assessor.” 27 –29,31 All five studies reported that auricular acupoints were assessed on both ears, satisfying the reporting for “laterality of assessed points.”
Summary of main findings by outcome
Body acupoints
Table 5 shows the summary of main findings for studies pertaining to body acupoints. This table is subdivided into the following three sections, by outcome type: (1) occurrence rate of tenderness; (2) VAS pain intensity score; and (3) PPT.
Summary of Main Findings by Outcome in Studies Evaluating Body Acupoints
HS, healthy subjects; n/a, not available; PPT, pressure pain threshold; PMS, premenstrual syndrome; VAS, visual analog scale.
Occurrence rate of tenderness
There were three studies that assessed the occurrence rate of tenderness at acupoints in healthy versus clinical populations. Ko et al. 21 found that subjects with functional dyspepsia compared with healthy controls exhibited a higher occurrence rate of tenderness at CV4, CV6, CV9, CV10, CV12, CV14, ST21, ST25, and KI16 (i.e., all assessed acupoints), using Pearson’s χ2 test or Fisher’s exact test. 21 Wu et al. 22 reported a higher occurrence of tenderness at acupoint LR5 in subjects with pelvic inflammatory disease compared with healthy controls, but not at SP6 and SP9. No description on statistical analysis was provided in this study. 22 Chen et al. 24 found that there is a higher occurrence of tenderness at SP8 in subjects with dysmenorrhea compared with healthy controls during both menstrual and nonmenstrual periods, based on a χ2 test. 24
VAS pain intensity score
There were two studies that compared the intensity of subject-reported pain in response to applied pressure at acupoints in healthy versus clinical populations. Wu et al. 22 reported higher VAS pain scores among subjects with pelvic inflammatory disease compared with healthy controls at SP6, SP9, and LR5. There was no information provided on statistical analysis. 22 Chen et al. 24 found that women with dysmenorrhea compared with healthy controls exhibited a significantly higher VAS score at SP8 during the menstrual period, but not during the nonmenstrual period. Wilcoxon test was used to compare the VAS scores in the two groups. 24
Pressure pain threshold
There were five studies that examined the PPT of acupoints in healthy versus clinical populations. Wu et al. 22 found that acupoints SP6, SP9, and LR5 exhibited higher PPT in subjects with pelvic inflammatory disease compared with healthy controls. They did not provide information on their statistical analysis. 22 In the other four studies, subjects in the clinical condition group compared with the healthy control group generally showed lower PPT at the assessed acupoints.
Chen et al. 24 found a significantly lower PPT at SP8 in women with dysmenorrhea compared with healthy subjects during the menstrual period, but not during nonmenstrual period based on a t-test. 24 Also using a t-test, Chae et al. 26 reported lower PPT at SP6 in adolescent girls with high premenstrual syndrome (PMS) compared with those with low PMS. SP6 was one of six acupoints assessed in this study. They also found no significant difference in PPT of nonacupoints among subjects with high versus low PMS. 26
Ben et al. 25 reported lower PPT in subjects with gastric ulcer compared with healthy controls at ST36, ST37, ST39, LI10, LI4, BL25 (6 of the 9 assessed acupoints). They also assessed adjacent nonacupoints and found no significant differences in PPT values between the two categories of points (i.e., acupoints vs. adjacent nonacupoints). No statistical analysis plan was provided for this study. 25
In Ko et al.’s 23 study, subjects with functional dyspepsia were first classified into two groups based on the presence or absence of tenderness, as diagnosed by an abdominal examination by Korean medicine doctors: (1) Simhabi (SH) refers to epigastric discomfort without tenderness, and (2) Simhabikyung (SHK) refers to epigastric discomfort with tenderness. In comparing these two groups with the healthy control group, they found lower PPT at CV14 in subjects with SHK-classified functional dyspepsia, but no significant difference in PPT between subjects with SH-classified functional dyspepsia and healthy subjects. 23
Auricular acupoints
Table 6 shows the summary of main findings for the five studies pertaining to auricular acupoints. Four studies were conducted by the same research team. 27 –30 In these studies, the investigators assessed the PPT of both acupoints and a reference point to determine the proportion of subjects or the occurrence rate of having lower PPT at acupoints relative to a reference point in healthy versus clinical groups. Shenmen was used as the reference point. Suen et al. 27 found that the proportion of subjects having lower PPT at acupoints relative to the reference point (Shenmen) was greater in the metabolic disease group compared with the healthy control group for the Heart and Endocrine AA zones, but not for the Pancreas and Gallbladder AA zones. 27 Higher occurrence rate of lower PPT relative to Shenmen was also found for subjects with type 2 diabetes mellitus compared with healthy subjects for the Pancreas and Gallbladder AA zones. 28 For men with urinary tract symptoms, there was a higher occurrence rate of lower PPT at most assessed auricular acupoints relative to Shenmen, including the Angle of Superior Concha, Urinary Bladder, Ureter, Kidney, Urethra, and Internal Genitalia AA zones. 29 Suen et al. 30 also found a higher occurrence rate of lower PPT at Heart AA zone relative to Shenmen in subjects with coronary heart disease compared with healthy controls. 30
Summary of Main Findings by Outcome in Studies Evaluating Auricular Acupoints
AA, auricular acupuncture; HS, healthy subjects; PPT, pressure pain threshold; VAS, visual analog scale.
In one study by Cheing et al., 31 the investigators assessed the PPT of a reference point and applied the same amount of pressure (i.e., PPT value of the reference point) to the acupoint of interest to determine the relative pain intensity on a 0–2 scale (i.e., 0 = less painful or having similar pain level as he/she felt on the reference zone; 1 = mildly more painful; 2 = significantly greater pain). Tooth AA zone was used as the reference point. This study found no significant difference between subjects with hepatic disorder and healthy controls in the pain intensity of the Liver AA zone relative to the Tooth AA zone. 31
Data Synthesis and Sources of Heterogeneity
There were many sources of heterogeneity across the included studies. First, there was substantial between-study difference in clinical populations. Among the six studies pertaining to body acupoints, there were two studies for functional dyspepsia and only one each for pelvic inflammatory disease, dysmenorrhea, gastric ulcer, and premenstrual syndrome. Among the five studies pertaining to auricular acupoints, there was only one study each for metabolic syndrome, type 2 diabetes, lower urinary tract symptoms, coronary heart disease, and hepatic disorders.
Second, the subjects in the clinical condition and healthy control groups were not comparable on age and sex in two 21,25 and four studies, 21 –23,31 respectively. Third, there was substantial heterogeneity in the selection of acupoints. Most acupoints were assessed in only one study, resulting in insufficient data to explore whether and how sensitivity of each point may vary or be associated with different clinical conditions.
Fourth, the studies also varied considerably in their outcomes. Among six studies pertaining to body acupoints, three studies reported on the occurrence rate of tenderness, two on VAS pain intensity score, and five on PPT. Among the five studies pertaining to auricular acupoints, four studies reported on the occurrence rate of lower PPT at acupoint(s) relative to a reference point and one on the occurrence rate of lower pain intensity rating relative to a reference point.
Fifth, there was also variability in the method or device used to apply pressure and evoke pain for acupoint sensitivity assessment. While most studies used a pressure algometer, two studies used manual palpation (i.e., investigator’s fingertip pressure) to assess the occurrence rate of tenderness, potentially resulting in inconsistent amount of pressure applied at acupoints across subjects. 21,24 Even in studies using a pressure algometer, there was insufficient information regarding the amount of pressure applied to acupoints for assessing the VAS pain intensity score, potentially introducing another source of heterogeneity. Moreover, there was also insufficient information for various specifications relevant to pressure algometry, including the algometer tip size, the angle of algometer application, and rate of application.
Discussion
In this systematic review, the authors identified 11 studies comparing acupoint sensitivity in individuals with and without visceral disorders. Overall, most studies included in this review supported the notion of acupoint sensitization, that is, corresponding acupoints are sensitized in pathologic conditions. However, they also found substantial heterogeneity and methodological quality issues across the included studies. Thus, no definitive conclusion can be drawn as to whether mechanical sensitivity of acupoints “reflects” or is associated with an individual’s health-disease status.
In recent years, the concept of acupoint sensitization has gained increasing attention to be a promising new paradigm for investigating the scientific basis of acupoints, especially with a growing body of preclinical animal research to support its premise. 8 –16 However, while findings from animal research have provided a valuable insight and perspective in the understanding of acupoints, data obtained from preclinical animal models may not extrapolate and apply to human subjects. 32 –34 Moreover, it is largely unclear how well the acupoints on the human body can be transposed onto acupoints in rodent models, especially given their small body sizes and limited spatial resolution. Thus, it will be essential to translate and validate preclinical findings in humans through clinical and translational research. To this end, this review was conducted to systematically examine the present status and quality of human studies on this topic. Below, we discuss existing evidence in the context of the included studies’ methodological quality as well as limitations of the present review and recommendations for improving the rigor of future research in this area.
Findings from studies included in this review suggest that both body and auricular acupoints may be mechanically sensitized in pathologic conditions. Among the six studies pertaining to body acupoints, there were two methods of applying pressure for mechanical sensitivity assessment: (1) manual palpation (i.e., investigator’s fingertip pressure) and (2) pressure algometry. While manual palpation is a commonly used approach in clinical settings, it does not provide a standardized measure of pain sensitivity. 35 Different amounts of force may have been applied by the investigators for subjects in healthy versus clinical condition groups, potentially leading to biased results. Thus, results obtained from the use of manual palpation in studies by Ko et al. 21 and Chen et al. 24 should be interpreted with caution.
Pressure algometry, on the contrary, is a widely used technique in pain research and has been shown to be valid, reliable, and reproducible in quantifying subject’s mechanical sensitivity for various clinical conditions, including neuropathic pain, musculoskeletal pain, and headache. 36 –42 A common outcome measure obtained from the use of pressure algometry is PPT, that is, the magnitude of applied pressure at which the subject starts to perceive pressure as painful. It also allows for a standardized amount of force to be applied against the body surface to assess the presence or absence of tenderness and the intensity of pain at that applied force. However, in studies using pressure algometry to assess the occurrence rate of tenderness and VAS pain intensity score, no information was provided in regard to the amount of force that was applied to obtain results for these two outcomes, raising questions about their validity and reliability.
Pressure algometry was also used for all five studies pertaining to auricular acupoints for outcome measures. In four studies, the PPT of acupoint(s) was compared with that of a reference point, and the acupoint in question was considered “positive” for tenderness if its PPT was lower or “negative” if not lower relative to that of the reference point. While dichotomizing continuous variable, such as PPT, may simplify statistical analysis and interpretation of the data, this is problematic as much information is lost, including the extent of variation in outcome. In one study by Cheing et al., 31 the amount of force applied to acupoint in determining the VAS pain intensity score was individualized for each participant to be his or her own PPT at a reference point (Tooth AA zone). 31 While this approach may take into account potential individual variability in pain sensitivity, it would be important to assess and confirm that the PPT of reference point is not affected by the given pathologic condition of interest in future studies.
There were also many potential sources of bias that were not adequately accounted for in the study design and analysis of the included studies. First, previous studies have shown that participant characteristics, such as age and sex, could affect one’s perceived level of pain sensitivity, and thus, there may a bias when comparing groups of different age and/or sex. 43 –47 While cases and controls were comparable on age in all five studies pertaining to auricular acupoints, sex was not comparable in the Cheing et al.’s 31 study. As for studies pertaining to body acupoints, cases and controls were not comparable on age and sex for two and three studies, respectively. Second, ambient temperature has also been shown to influence pain sensitivity measurements. 48 –50 Across all 11 studies, information on ambient temperature was clearly described in only one study. 23 While two studies did report that the data was collected in “room temperature,” there is insufficient information to ascertain whether the ambient temperature was well-controlled, and if so, within what ranges of temperature. 27,28 Third, only one study pertaining to body acupoints reported that the assessor was blinded to the participant status (cases vs. controls). 26 Fourth, many studies provided no or insufficient information relevant to algometer specifications, including its tip size and material as well as the angle and rate of its application. This is problematic as variability in these specifications may potentially affect outcomes. Having sufficient information on these parameters would be essential to ensure reproducibility and establish standard parameters and practices in future research. 41,42
The present review also has many limitations. First, a relatively limited number of databases were used to identify potentially eligible studies. Second, the search was limited to the English language. Thus, this review may have not included non-English studies meeting the other eligibility criteria. Third, a meta-analysis was not conducted and only a narrative summary of main findings from included studies is provided. Despite these limitations, to our knowledge, this review is the first to provide a comprehensive summary of presently available literature on pain sensitivity of acupoints in health and disease in humans. More reviews are needed to examine the present status of literature in regard to other physiological characteristics of acupoint sensitization. While we have previously conducted another systematic review addressing the question of whether acupoints are thermally distinct in healthy versus clinical populations, 51 it would be of interest to systematically synthesize evidence on other characteristics, including electrical properties of acupoints in health and disease.
In addition to the need for more systematic reviews, there is a need for more rigorous original clinical and translational studies investigating acupoint sensitization. Compared with other areas of acupuncture research, such as efficacy studies, which have grown substantially over the past few decades, relatively little work has been done to understand the scientific basis of acupoints. Given that the concept of acupoints is fundamental to the theory and practice of acupuncture, it will be important to address this research gap to move the field forward.
To improve the rigor of future research on this topic, it will be important to have a larger sample size and ensure that the cases and controls are comparable on participant characteristics, such as age and sex. It will also be important for future studies to report more complete information on their experimental designs and variables that could potentially influence pain sensitivity measurements. Thus, it may be of interest to the acupuncture research community todevelop and establish standardized methodological and reporting guidelines for acupoint sensitivity assessments through a Delphi process. In addition, in planning future research relating to acupoints, it will be important to recognize that there are substantial differences across acupuncturists in how they select and locate acupoints for treatment and that there are other methods (e.g., electrical properties) used in clinical practice for locating points that are independent of pain sensitivity. It is also important to recognize that sensitized points may not necessarily map onto the classical acupoint locations. These are important considerations for future research. Furthermore, it will be important to address a gap in the literature as to whether and how acupoint sensitivity is altered in response to acupuncture treatment and changes in the health-disease status within the same individuals over time.
In regard to clinical implications, findings suggest that pressure pain of acupoints may be associated with disorders of the internal organs, and as such, palpation may be an important diagnostic technique in acupuncture treatment. However, more rigorous research is needed to confirm these findings. Furthermore, it may be of great interest to investigate the therapeutic value of acupoint sensitization. In a recent 2021 randomized controlled trial, Huang et al. showed that acupressure at acupoints with the highest pain sensitivity was significantly more effective in reducing the frequency of angina attacks, compared with acupressure at acupoints with the lowest pain sensitivity. 52 This is an exciting finding, as the concept of acupoint sensitization may provide new insights and systematic approach to optimizing point selection for acupuncture treatment. However, without more rigorous research, it will be difficult to ascertain whether stimulation of sensitized acupoints is clinically more beneficial compared with that of nonsensitized points.
In conclusion, this is the first review to systematically collate and summarize previous studies addressing the question of whether acupoints are mechanically sensitized in pathologic conditions in humans. Based on this review, there is insufficient evidence to draw a definitive conclusion regarding acupoint pain sensitivity in relation to health and disease. However, provocative trends support the value of further research. Improving the rigor and quality of studies on this topic will be important to better understand the potential diagnostic and therapeutic values of acupoint sensitization in future research.
Author Contribution Statement
E.Y. and P.M.W. conceived of the study and planned the study design and search strategy. E.Y. and D.M.V. screened articles for eligibility and assessed the quality of included studies. E.Y. and E.G. conducted data extraction. E.Y. drafted the initial article. E.Y., W.L., T.J.K., V.N., A.C.A., and P.M.W. contributed to the interpretation of the results, and all authors read and contributed to the revisions of the article and approved the final version.
Registration Information
The present review was not registered. The protocol for the present review is available from the corresponding author on reasonable request.
Footnotes
Author Disclosure Statement
All authors declare that they have no conflict of interest.
Funding Statement
E.Y. was supported by NIH/NCCIH training grant (T32 AT000051). P.M.W. was supported by NIH/NCCIH mid-career investigator award (K24 AT009282). The funders had no role in the design, interpretation, and presentation of this manuscript.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.