
Abstract
Background:
In community and school settings, gardens and garden interventions have been shown to confer several psychosocial, physiological, and nutritional benefits. However, little is known about the implementation and impact of health care gardens on patients, visitors, and staff health and well-being. The primary aim of this review is to identify and describe the types of gardens and common design elements implemented in health care settings and the impact these gardens have on the health and well-being of patients, visitors, and staff. A secondary aim is to assess the quality of available evidence.
Methods:
PubMed, CINAHL, EMBASE, and PsycINFO were systematically searched on October 28, 2022. Primary qualitative and quantitative studies (excluding case reports and studies) were eligible for inclusion if they described the types of gardens and common design elements implemented in health care settings (hospitals, aged care, rehabilitation facilities, and medical centers) and/or assessed the impact of garden interventions on the health and well-being of patients, visitors, and staff. Review, selection, and data extraction were conducted by two independent researchers, with findings synthesized and presented in narrative form. Articles were critically appraised using the mixed methods appraisal tool (MMAT).
Results:
Eighteen articles were included. Eight studies provided detailed descriptions of the types of gardens implemented in health care settings (healing [n = 3], therapeutic [n = 2], sensory [n = 2], children's fairy gardens [n = 1], and enriched [n = 1] gardens). Studies examining the psychosocial impacts of gardens were most frequently reported (n = 16), followed by physical (n = 4) and nutritional (n = 2). A wide range of positive outcomes, predominantly relating to patients (n = 12), were reported, including improvements in stress, quality of life (QOL), cognitive function, physical activity, and fruit and vegetable intake. The evidence was heterogeneous and low-medium quality.
Conclusions:
The findings suggest that implementing gardens and garden interventions in health care settings may positively impact the health and well-being of patients, visitors, and staff. Most studies related to the impact of gardens on patients' mental health and QOL, indicating the need for further research to explore physical and nutritional outcomes, as well as health outcomes of staff and visitors. Findings also suggest the need for high-quality study designs (e.g., cluster control trials) and standardized measurement tools.
Introduction
Gardens and garden interventions have been associated with numerous health and well-being benefits for individuals, including psychosocial, physical, and nutritional. 1 –5 For example, community and school gardens have been shown to improve fruit and vegetable (F&V) intake, 6 –10 decrease body mass index (BMI) 11 and blood pressure, 12 and reduce stress, anxiety, and burnout. 3,5 These are important concepts of health as high F&V intake is known to reduce the risk of chronic diseases such as heart disease and type 2 diabetes, lower blood pressure, and prevent some types of cancer such as bowel cancer. 1,13,14 Furthermore, mental well-being is understood to be integral to good health as it is associated with positive health behaviors 15 and has been shown to improve recovery from illness. 16
Like schools and communities, health care settings such as hospitals, medical centers, aged care, and rehabilitation facilities can serve as valuable sites for gardens. They have the potential for short-term benefits for patients and visitors, such as reducing stress in family members of hospitalized patients, 17 and ongoing benefits for health care workers, such as reduced burnout in nursing staff. 18,19 This is important as health care workers commonly report poor diets, 20,21 inadequate physical activity, 22 and poor mental health as a result of burnout. 23 Some hospitals in the United States now offer on-site gardens or farms and locally sourced produce in patient and staff meals. 20,21 These projects have been shown to produce several beneficial outcomes, including access to healthy food, physical activity, nutrition education, and environmental sustainability. 20,21
Gardens located in hospitals, medical centers, aged care, and rehabilitation facilities are a business innovation 20 that may provide complementary therapy to facilitate health improvements for their patients, visitors, and staff. Despite this, collated information on how health care settings implement gardens on-site is difficult to find. Moreover, the effectiveness of implementing gardens in health care settings is relatively unknown, given the heterogeneity inherent in this research. Therefore, the primary aim of this systematic scoping review was to (1) identify and describe the types of gardens and common design elements implemented in health care settings and (2) identify and describe the impact these gardens have on the health and well-being of patients, visitors, and staff. A secondary aim was to (3) assess the quality of available evidence.
Methods
The systematic scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) checklist. 24 The protocol was registered with Open Sciences Framework (https://doi.org/10.17605/OSF.IO/T5JZK) on November 16, 2022.
Search strategy
Searches were conducted in Medline (PubMed), CINAHL, PsychINFO (EBSCOHost), and EMBASE databases on October 28, 2022. The search strategy was developed in consultation with the Bond University Health and Medical Sciences Faculty Librarian and included relevant MeSH (Medical Subject Headings) terms, subject headings, and keywords such as “horticulture” OR “garden” AND “healthcare setting” OR “hospital” OR “aged care” OR “rehabilitation” AND “psychosocial” OR “wellbeing” OR “nutrition” OR “health outcome” (Supplementary Material).
To ensure all relevant literature was included, no limit on time or language was set. Before exporting articles into Covidence for screening, retrieved articles were deduplicated using the systematic accelerator deduplication tool. 25 Screening by title and abstract was conducted in duplicate by two researchers. Non-English studies were translated with the assistance of bilingual researchers. The remaining full-text articles were assessed in Covidence for relevance against inclusion criteria. At both screening stages, conflicts were resolved through consensus or with a third research team member (an experienced academic researcher).
Study eligibility
Studies met the inclusion criteria if they described the implementation of health care gardens and/or assessed individual health benefits of horticulture or garden-based interventions. The term health care encompasses hospitals, medical centers, aged care, and rehabilitation facilities. There was no restriction on the types, design (e.g., randomized and nonrandomized control trials, cohort, qualitative), population, or sample size of included studies. To be included, studies had to describe primary research (excluding case reports and studies) and be peer reviewed. Thus, protocol articles, systematic reviews, and gray literature were excluded.
The primary outcome was related to the positive impact health care gardens had on patients, visitors, and staff health and well-being. The term “well-being” referred to the following: psychosocial (such as, but not limited to, anxiety, depression, burnout, mood, happiness, quality of life [QOL], connectedness to nature, socialization, and knowledge sharing), nutritional (dietary intake), and physiological components such as heart rate (HR), blood pressure, and cholesterol. Studies that reported on garden interventions outside of predefined health care settings and/or did not sufficiently describe health care gardens were excluded. In addition, to maintain a targeted scope of the implementation of health care gardens, studies assessing the benefits of nature views or pictures of nature were also excluded.
Quality appraisals
Eligible studies were assessed using the Mixed Methods Appraisal Tool (MMAT). 26 The MMAT is a validated critical appraisal tool designed to assess multiple study designs, including qualitative research, randomized control trials, nonrandomized control trials, quantitative descriptive studies, and mixed method studies. 26 Two researchers completed quality appraisals of all article, and discrepancies were resolved through consensus or consultation with a third researcher. The researchers critically appraised the quality of studies based on the adequacy of collected data and whether the data answered the research question.
Results
Study characteristics
From 5821 citations, a total of 18 full-text studies (n = 613) 17 –19,27 –42 were eligible for inclusion (Fig. 1). Of the 18 articles included, 9 were quantitative (n = 407), 17 –19,27,28,32 –34,42 6 were qualitative (n = 145), 31,35,36,38 –40 and 3 were mixed methods studies (n = 61). 29,30,41 Sixteen studies evaluated the impact of gardens on patients (n = 471), 27 –36,41,42 two studies on health care staff (n = 86), 18,19 and two studies (n = 56) on visitors. 17,39 Hence, overall findings are primarily related to patients.
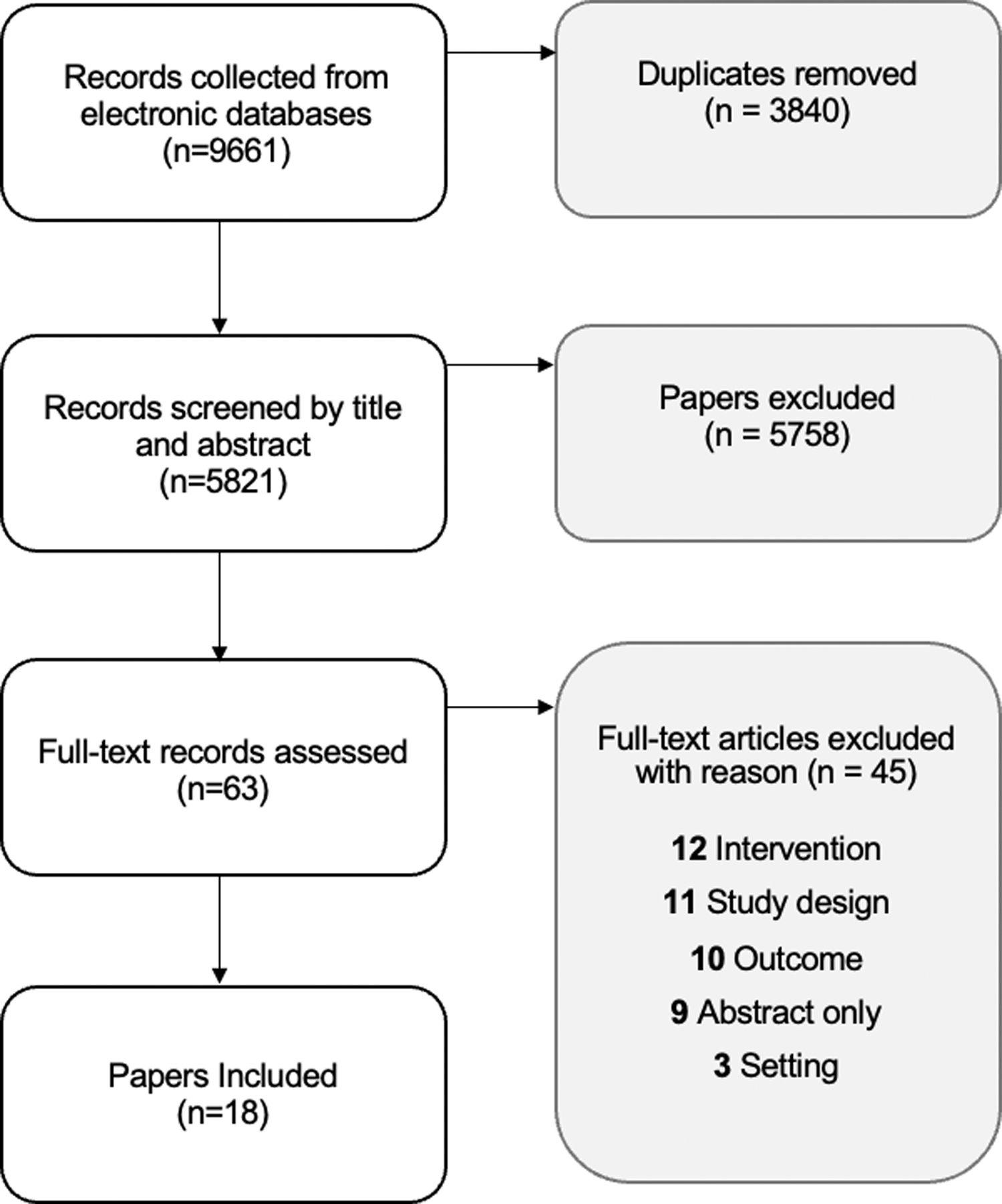
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Most studies (n = 16) assessed the impact of gardens on psychosocial outcomes, including cognitive function, mental health, social, burnout, and QOL. 17 –19,27 –32,34 –36,38 –40,42 Four studies reported specific physiological outcomes, 41,42 for example, HR and physical function, and two studies reported nutritional outcomes, 33,41 for example, dietary behavior and intake. The studies were conducted across 3 settings: 12 in a hospital setting, 17 –19,27,32 –34,36 –40,42 3 in an aged care facility, 28 –30 2 in a rehabilitation setting 31,35 and 1 in a medical center. 41 A detailed description of the implementation of gardens was provided in 8 17,18,27,28,30 –32,38 of the 18 studies. Sixteen studies were published in English, 17 –19,27 –33,35,36,38 –42 one in French, 19 and one in Korean. 34 Country of origin included the United States, 17,18,33,35,36,41,42 Thailand, 38 –40 France, 19,28,32 Australia, 29,30 Switzerland, 27,31 and South Korea. 34 Characteristics of the included studies are summarized in Table 1.
Quantitative, Mixed Methods, and Qualitative Study Characteristics
BMI, body mass index; CMD, cognitive motor dissociation; CSG, conventional sensory garden; CVD, cardiovascular disease; EG, enriched garden; FG, Fairy Garden; HT, horticultural therapy program; HR, heart rate; ICU, intensive care unit; PEC, patient education class; PTSD, post-traumatic stress disorder; QOL, quality of life; SARRTP, Substance Abuse Residential Rehabilitation Treatment Program; SD, standard deviation; TG, therapeutic garden.
Description of gardens
Eight studies 17,18,27,28,30 –32,38 provided detailed descriptions of the implementation of gardens, as seen in Table 1. The studies described a range of garden types, including two therapeutic gardens, 27,31 a children's fairy garden, 38 two sensory gardens, 28,30 an enriched garden, 28 and three healing gardens. 17,18,38 Of these eight studies, four were in a hospital setting, 17,18,27,38 three in an aged care facility, 28,30,32 and one in a rehabilitation facility. 31 All hospital healing gardens 17,18,38 were designed for patients, visitors, and staff, whereas the aged care 28,30,32 and rehabilitation 27,31 gardens were designed for use by patients and visitors.
Five of the eight studies 17,18,28,30,32 described incorporating evidence-based practice recommendations into the design process. Common design themes emerged from the studies, including easy accessibility, both in terms of direct access to the garden (24/7) and pathway for people with wheelchairs, crutches, and walkers; providing shade, acceptable hygiene, and safety standards (e.g., no stagnate water), views from indoor windows, portable seating, and running water, that is, fountains. In addition, there was the provision of an array of different textured flora and hard landscapes to illicit the senses. 17,18,27,28,30 –32,38
Of the 18 included studies, 12 studies 17 –19,27 –32,38 –40 examined the benefits of therapeutic garden-based interventions for various populations, which included physical therapy, cognitive behavioral therapy, socializing, sitting, walking, and viewing from within the garden. Four studies 34 –36,42 examined horticultural therapy interventions that included a range of activities for participants. Some of these activities focused on passive involvement, such as sitting, walking, and viewing from within the garden. Other interventions involved active participation, including gardening, education sessions, crafts, and meditation. Finally, two studies 33,41 focused on culinary nutrition interventions that involved a combination of activities related to nutrition education/promotion, vegetable and herb gardening, and cooking. These interventions aimed to improve participant's knowledge and skills in nutrition, promote healthy eating habits, and encourage the consumption of fresh, homegrown produce. 33,41
Health outcomes
Psychosocial outcomes
Twenty-one psychosocial outcomes were reported in 16 studies. 17 –19,27 –32,34 –36,38 –40,42 Twelve studies reported on the emotional well-being benefits of gardens for patients, visitors, and staff. 17,18,29 –32,35,36,38 –40,42 Six quantitative studies (including two mixed methods 29,30 ) assessed anxiety, depression, stress, and mood, using six different assessment tools, 17,18,29,30,32,42 detailed in Tables 2 and 3. Of the six studies, five reported significant improvement in emotional well-being. 17,29,30,32,42 These quantitative findings were supported by eight qualitative studies (including two mixed methods 29,30 ) that further emphasized the emotional well-being benefits of gardens. 29 –31,35,36,38 –40 Commonly reported themes from semistructured open-ended interviews with patients, visitors, and staff emerged, including a perceived reduction in stress, improvements in relaxation and happiness, and the healing properties of being surrounded by nature (e.g., escapism from illness). 29 –31,35,36,38 –40
Quantitative Study Outcomes
C, control; CMD, cognitive motor dissociation; CSG, conventional sensory garden; EG, enriched garden; HR, heart rate; ICU, intensive care unit; KATZ ADL, Katz Index of Independence in Activities of Daily Living; MBI, Maslach Burnout Inventory Human Services survey; MMSE, Mini mental status examination; POMS, profile of mood states; SCQ, Self-Consciousness Questionnaire; SMBQ, Shirom-Melamed Burnout Questionnaire; SMVM, Shirom-Melamed Vigor Measure; TG, therapeutic garden; TMD, total mood disturbance; TUG, timed up and go; VAS, Visual Analog Scale.
Mixed Method Study Outcomes
ARS, Affect Rating Scale; BMI, body mass index; CMAI, Cohen-Mansfield Agitation Inventory; CSDD, Cornell Scale for Depression in Dementia; CVD, cardiovascular disease; DEMQOL, Dementia Quality-of-Life Instrument; F&V, fruit and vegetable; PA, physical activity; QOL, quality of life.
Four studies cited positive social benefits of gardens. 31,36,39,40 Two nonrandomized controlled trials assessed the impact of taking daily work breaks in a garden on burnout in nurses. 18,19 Both studies reported significant improvements in symptoms of burnout. One measured by the Pediatric Quality-of-Life Present Functioning Visual Analog Scale and the Maslach Burnout Inventory Human Services Survey, 18 while the other study assessed burnout using a questionnaire adapted from the following validated assessment tools: The Demand-Control Support Questionnaire, Effort-Reward Imbalance Questionnaire, Shirom-Melamed Burnout Questionnaire, and Shirom-Melamed Vigor Measure. 19
Six qualitative studies (including two mixed methods 29,30 ), presented in Tables 3 and 4, evaluated the impact therapeutic gardens have on QOL by way of interviews that were recorded and transcribed, and interpretation given to arising patterns. 29,30,35,38 –40 The data obtained from focus groups and semistructured interviews highlighted the experiences of patients, visitors, and staff with the gardens. 29,30,35,38 –40 Overall, the nature-based environment was found to promote joy, calmness, engagement, movement, and socialization among the participants. 29,30,35,38 –40 Participants reported valuing the esthetics of the natural environment, particularly in contrast to the clinical setting, 29,30,35,38 –40 as well as appreciating different gardening activities and sensory experiences. 29,30,35,38 –40 The quantitative components of the two mixed methods studies 29,30 further supported these findings, citing significant improvements in aspects of QOL, measured by the Quality-of-life Assessment in Dementia 30 and the Affect Rating Scale. 29
Qualitative Study Outcomes
FG, Fairy Garden; QOL, quality of life; TG, therapeutic garden.
Three nonrandomized control trials assessed the impact of therapeutic gardens on cognitive function among participants with cognitive motor dissociation and dementia. 27,28,32 Each study used a different assessment tool—A Behavioral Grid, 27 Mini Mental Status Examination, 28 or Self-Consciousness Questionnaire—to measure varying aspects of cognitive function. All studies reported significant improvements in aspects of cognitive function after exposure to a garden. 27,28,32
Physical outcomes
Four studies examined the physical health outcomes of patients. 27,28,41,42 Of these four studies, two assessed the impacts of horticultural therapy or gardening on HR in patients with cardiovascular disease (CVD) 41,42 : One a nonrandomized control trial 42 and one study with pre- and post-measurements with no comparison group. 41 While one study reported a significant difference in HR, 42 the other did not. 41 One study assessed participants' blood pressure, BMI, and physical activity. 41 The study reported significant improvements in physical activity levels, but no significant difference in blood pressure or BMI. 41 Physical function was assessed in two studies among participants with dementia 28 and cognitive motor dissociation. 27 In both studies, participant's access to outdoor gardens appeared to result in significantly better physical functioning, 27,28 measured by unipodal stance, 28 timed up and go, 28 Katz Index of independence in Activities of Daily Living, 28 and Indicators of Purposeful Behavior. 27
Nutrition outcomes
Two studies reporting on the impact of vegetable gardens on patients' diets and health were identified. 33,41 Both used a prestudy-poststudy design and sought to measure the consumption of F&V. 33,41 One study also looked at the intake of total fiber and energy from fat, 41 while the other study looked at behaviors toward nutrition and healthy eating, home gardening practice, and food preparation. 33 Following the 12-week hospital-based garden intervention, participants reported an increase of 1.2 serves F&V and significantly more fiber intake, although no reduction in the percent of energy from fat. 41 In the hospital-based cooking and gardening program for children, there was a reported increase in gardening and cooking at home among participants who completed the program, although only 50% of the original participants completed the program. 33
Study quality
Assessment of studies using the MMAT 26 indicated that the overall quality of included studies was medium-low (Fig. 2). All included studies had a clear research question. Most studies' data addressed the research question, except for one study, which only reported baseline data. 33 The main reasons for the medium-low quality of studies related to the outcome measures, most of which were heterogeneous, low in reliability and validity, lacked controls, and had variable follow-up lengths. Seven studies were assessed under the quantitative nonrandomized controlled trial category in MMAT. 17,18,27,28,32,33,42
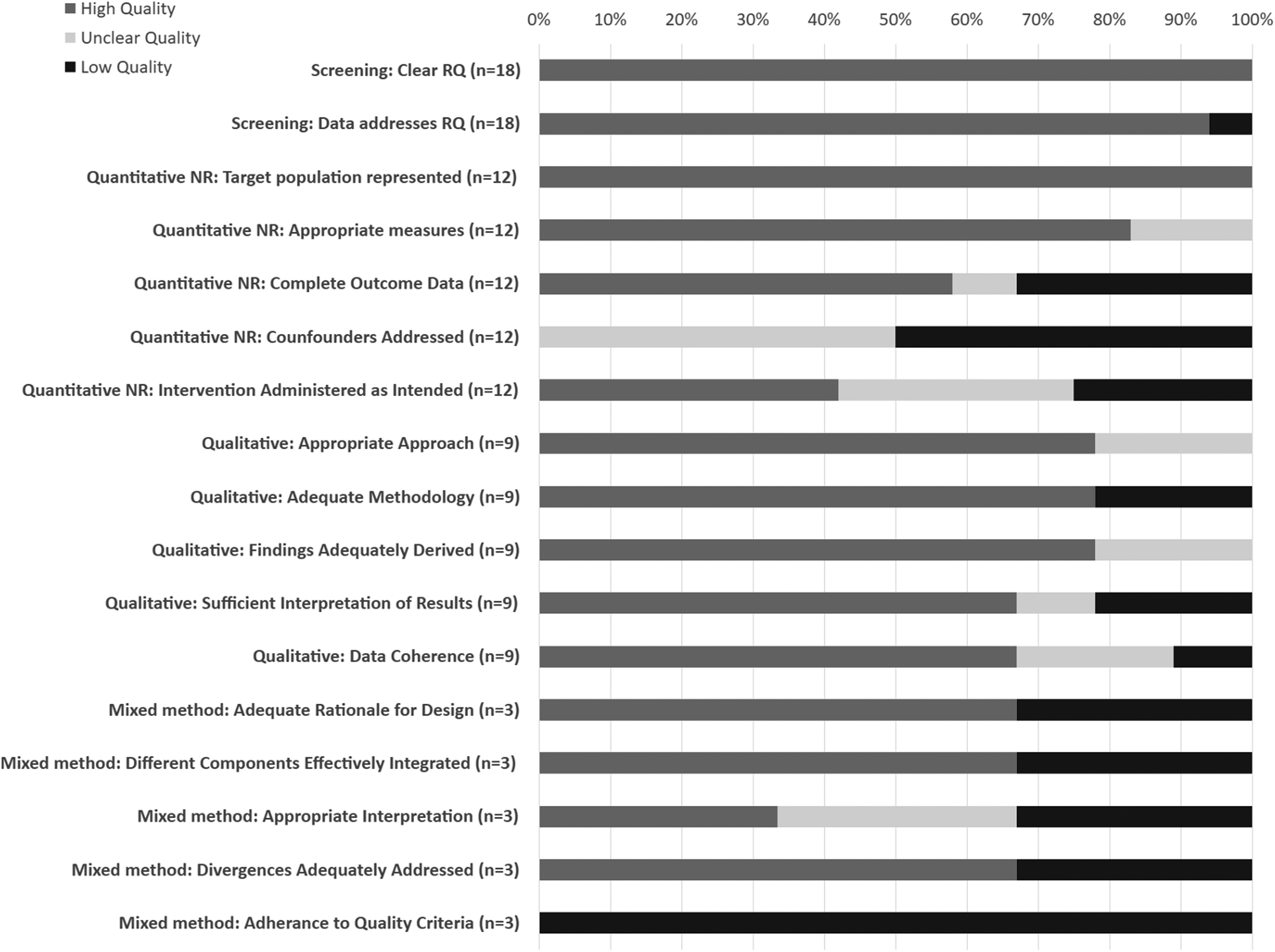
Quality assessment of included studies using the MMAT—version 2018. MMAT, Mixed Methods Appraisal Tool.
The majority did not meet quality questions, except for represented target population and utilizing appropriate measures. Six studies 31,35,36,38 –40 were assessed under the qualitative category where the majority met all quality questions, except for one study 35 that did not meet any. Finally, three studies were assessed using the mixed methods questions. 29,30,41 One study 30 performed poorly on all qualitative questions, and the other two studies 29,41 were of medium quality.
Discussion
This systematic scoping review synthesizes the available evidence for the implementation and impact of health care gardens on human health. The findings suggest that exposure to gardens in health care settings may positively impact the health and well-being of patients, visitors, and staff. Most research has measured psychosocial outcomes, but some gardens and garden interventions have been implemented to improve patients' physical health and nutritional outcomes. That said, the overall evidence was of medium-low quality and heterogeneous and may not be sufficient to draw strong conclusions.
Gardens implemented in health care settings appear to support the health and well-being of patients, visitors, and staff. Notably, the studies that provided descriptions of gardens described therapeutic, healing, or sensory-type gardens used for emotional well-being, QOL, and cognitive function in all three settings: hospital, aged care, and rehabilitation. Sensory or enriched gardens were often employed in aged care settings with easy access, an array of trees, plants and flowers, and other stimulating accessories.
This finding aligns with current literature on nature-based interventions in full-time care or rehabilitation settings, which indicates that sensory gardens may produce positive effects for improved well-being in aged care. 43 Furthermore, healing gardens were commonly implemented in a hospital setting to address the psychosocial outcomes of patients, visitors, and staff. Although results are limited by sample size and the quality design of studies, the implication is that gardens can provide respite for patients, visitors, and staff from the often stressful stimuli of clinical settings. Most described gardens also utilized evidence-based design recommendations for gardens that provide a sound basis for future implementation of gardens in health care settings.
Regarding psychosocial outcomes, gardens in health care settings appear to positively impact the QOL and emotional well-being of patients, visitors, and staff. Of studies included in this review that assessed psychosocial outcomes, each used a variety of different measures and study designs and the overall reliability and validity of evidence of studies were medium-low quality.
Nevertheless, most studies indicated improved emotional well-being and QOL from both reported outcome measures and the experiences and perceptions of participants taking part in health care-based garden interventions. These findings are consistent with current literature, which highlights community gardens and horticultural therapy as having an overall positive effect on psychosocial well-being. 5,44 Emotional well-being is considered an essential aspect of health because it is related to positive health behaviors. 45 It is worth highlighting two studies that explored the possible benefits of gardens for reducing burnout in health care staff, as both studies reported significant improvements in reducing burnout symptoms. 18,19 These findings are particularly relevant since health care workers experience high rates of burnout, 46 which have been exacerbated by the recent COVID-19 pandemic. 47
Physical health is considered the cornerstone of an individual's overall well-being and is affected by lifestyle choices such as physical activity, diet, smoking, and alcohol consumption. 48 The results for garden-associated physiological health outcomes were mixed. However, the included studies varied substantially concerning the outcomes assessed, assessment tools, sample size, population characteristics, and study quality and design. Similar to the result from this review, a recent systematic review and meta-analysis (2020) 49 assessing the impact of community gardens on physical health reported mixed results for HR, blood pressure, and physical activity. However, the meta-analysis for BMI showed a positive association between gardening and weight reduction, which contrasted with the findings from this study. 49 The authors of the systematic review and meta-analysis also reported significant heterogeneity in included studies and outcomes, 49 which is a common theme across the breadth of research in this area and may potentially explain the reported inconsistencies.
The impact of garden-based interventions on improving nutrition in health care settings remains inconclusive due to the low-quality studies, such as few randomized trials or evaluations without comparison groups. However, available findings suggest gardening interventions generally showed greater fruit, vegetable, and fiber intake in participants. These findings are consistent with community-based gardening interventions. For example, a horticultural therapy intervention for cancer survivors resulted in significant improvements in overall dietary patterns (increased consumption of F&V and a decrease in consumption of red/processed meat and sugar-sweetened beverages). 50 A recent systematic review and meta-analysis also reported that gardening was associated with higher consumption of F&V among gardeners compared to nongardeners. 49 Furthermore, the beneficial effects of garden interventions on behavior and self-efficacy toward nutrition among school children are also demonstrated in another, more recent systematic review. 51
A strength of this review was the systematic approach, which included conducting a comprehensive search in four databases, and multiple researchers screening, assessing, and conducting quality appraisal in duplicate. To strengthen the study's generalizability and ensure all relevant literature was included, the search was developed and executed in consultation with an experienced librarian and included no time or language limit. Publication bias, due to the exclusion of gray literature, is a limitation of this study. However, the main purpose of this review was to assess the available evidence in peer-reviewed journals.
The rationale is that, while many hospitals have implemented on-site gardens, 20 evaluations of these interventions are either difficult to find or they lack the study quality, design, and rigor standards required of a scholarly report. Given gardens and garden interventions are multifaceted health interventions, another strength of this study was that all study designs were included (quantitative, qualitative, and mixed methods), which lends to a richer evaluation of health outcomes. A major limitation of the review is that the research in this area is limited, is of low-medium quality, and has significant variability in the study designs, garden types, and outcomes measured, with very few studies reporting using the same measurement tool. However, randomized controlled trials to evaluate the health effects of garden interventions may not be feasible. For example, they may be unethical as it would require withholding access to a therapeutic garden to participants in a control group.
Similarly, a garden intervention to measure objective physical health benefits would require very long intervention and follow-up periods. Finally, despite best efforts, due to the significant heterogeneity in study design, it is possible that not all relevant studies were captured by the search strategy. In saying that, if relevant studies were missed, it is unlikely to change the overall findings, given they are consistent with the larger body of gardening research in other populations and settings.
Conclusion
The overall findings suggest that regardless of the type of garden or health care setting, the implementation of gardens may confer several psychosocial, physical, and nutritional benefits to its users. Health care gardens, be as extensive as rooftop or vegetable gardens or simply include a small collection of plants in an atrium, can offer respite for long-term patients, solace and fresh air for visitors, or a place to take breaks and unwind for staff. Health care providers can feel confident that any investment in on-site gardens may offer a benefit to patients, staff, and/or visitors without any significant risk.
This study also highlighted key gaps in the existing evidence base and quality of primary research, indicating the need for future research to explore the physical, nutritional, and health outcomes of staff and visitors. It is also recommended that researchers in this area use high-quality study designs (e.g., cluster control trials) and standardized measurement tools to determine the effects of health care garden interventions on individual health and well-being-related outcomes.
Footnotes
Acknowledgments
The authors thank the Bond University Nutrition and Dietetics Program (MNDP) team for contributing to the development of this article. This scoping review was partially published as a poster presentation for the Dietitians Australia Conference, July 23–25, 2023. 52
Authors' Contributions
C.C. and J.H. developed and executed the search strategy with an experienced librarian. C.C. and J.H. reviewed, selected, and extracted the data from eligible articles and equally contributed to writing the article. Through each stage of the systematic process, J.U. provided guidance and assistance with reviewing and editing the article. S.M. reviewed and edited the final article. All authors read and approved the final article.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.